
Early Monitoring Response to Therapy in Patients with Brain Lesions Using the Cumulative SUV Histogram

 ,
,  ,
, 
 ,
,
Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. [11C]-Methionine PET (MET)
2.3. PET/CT
2.4. PET Feature-Based Measures
2.5. Data Analysis
2.6. Statistical Analysis
3. Results
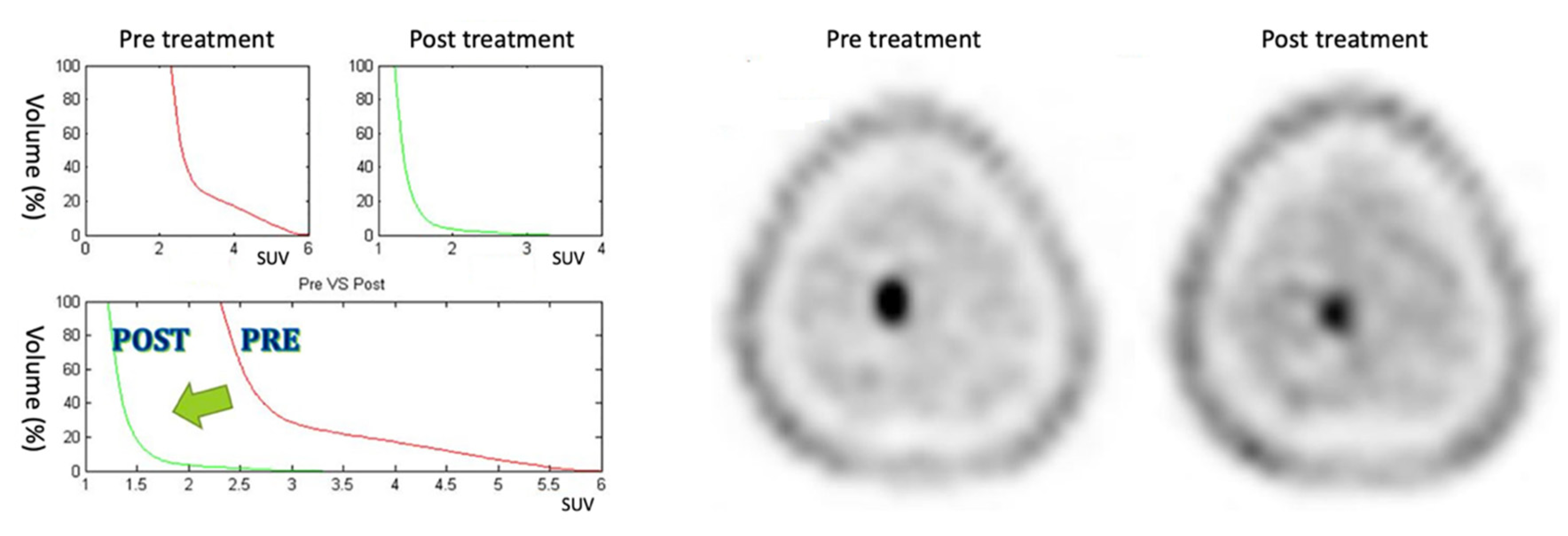
3.1. Positive Response
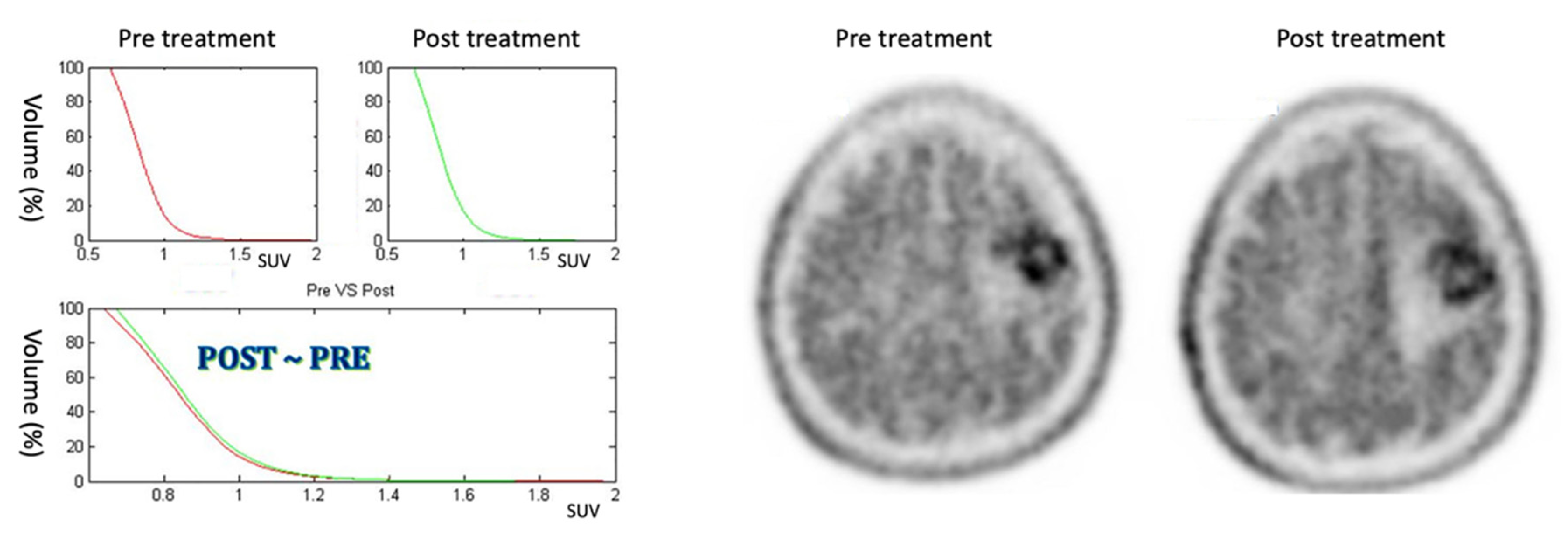
3.2. Stable Response
3.3. Negative Response
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Moskvin, V.; DesRosiers, C.; Papiez, L.; Timmerman, R.; Randall, M.; DesRosiers, P.; Dittmer, P. Monte Carlo simulation of the Leksell Gamma Knife: I. Source modelling and calculations in homogeneous media. Phys. Med. Biol. 2002, 47, 301. [Google Scholar] [CrossRef]
- Wu, A. Physics and dosimetry of the gamma knife. Neurosurg. Clin. N. Am. 1992, 3, 35–50. [Google Scholar] [CrossRef]
- Khoo, V.S.; Joon, D.L. New developments in MRI for target volume delineation in radiotherapy. Br. J. Radiol. 2006, 79, S2–S15. [Google Scholar] [CrossRef]
- Bol, G.H.; Kotte, A.N.T.J.; van der Heide, U.A.; Lagendijk, J.J.W. Simultaneous multi-modality ROI delineation in clinical practice. Comput. Methods Programs Biomed. 2009, 96, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Cuocolo, R.; Cipullo, M.B.; Stanzione, A.; Ugga, L.; Romeo, V.; Radice, L.; Brunetti, A.; Imbriaco, M. Machine learning applications in prostate cancer magnetic resonance imaging. Eur. Radiol. Exp. 2019, 3, 35. [Google Scholar] [CrossRef]
- Comelli, A.; Terranova, M.C.; Scopelliti, L.; Salerno, S.; Midiri, F.; Lo Re, G.; Petrucci, G.; Vitabile, S. A kernel support vector machine based technique for Crohn’s disease classification in human patients. In Advances in Intelligent Systems and Computing; Springer: Cham, Switzerland, 2018; Volume 611, pp. 262–273. ISBN 9783319615653. [Google Scholar]
- Comelli, A.; Stefano, A.; Russo, G.; Bignardi, S.; Sabini, M.G.; Petrucci, G.; Ippolito, M.; Yezzi, A. K-nearest neighbor driving active contours to delineate biological tumor volumes. Eng. Appl. Artif. Intell. 2019, 81, 133–144. [Google Scholar] [CrossRef]
- Comelli, A.; Stefano, A. A Fully Automated Segmentation System of Positron Emission Tomography Studies. In Medical Image Understanding and Analysis; Zheng, Y., Williams, B.M., Chen, K., Eds.; Communications in Computer and Information Science; Springer: Cham, Switzerland, 2020; Volume 1065, pp. 353–363. [Google Scholar]
- Comelli, A.; Stefano, A.; Bignardi, S.; Coronnello, C.; Russo, G.; Sabini, M.G.; Ippolito, M.; Yezzi, A. Tissue Classification to Support Local Active Delineation of Brain Tumors. In Medical Image Understanding and Analysis; Zheng, Y., Williams, B.M., Chen, K., Eds.; Communications in Computer and Information Science; Springer: Cham, Switzerland, 2020; Volume 1065, pp. 3–14. [Google Scholar]
- Gempt, J.; Bette, S.; Buchmann, N.; Ryang, Y.-M.; Förschler, A.; Pyka, T.; Wester, H.-J.; Förster, S.; Meyer, B.; Ringel, F. Volumetric Analysis of F-18-FET-PET Imaging for Brain Metastases. World Neurosurg. 2015, 84, 1790–1797. [Google Scholar] [CrossRef]
- Stefano, A.; Vitabile, S.; Russo, G.; Ippolito, M.; Marletta, F.; D’Arrigo, C.; D’Urso, D.; Sabini, M.G.; Gambino, O.; Pirrone, R.; et al. An automatic method for metabolic evaluation of gamma knife treatments. In Image Analysis and Processing—ICIAP 2015; Lecture Notes in Computer Science; Springer: Cham, Switzerland, 2015; Volume 9279, pp. 579–589. [Google Scholar]
- Weber, W.A.; Grosu, A.L.; Czernin, J. Technology Insight: Advances in molecular imaging and an appraisal of PET/CT scanning. Nat. Clin. Pract. Oncol. 2008, 5, 160–170. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, J.W.; Djulbegovic, B.; Soares, H.P.; Siegel, B.A.; Lowe, V.J.; Lyman, G.H.; Coleman, R.E.; Wahl, R.; Paschold, J.C.; Avril, N.; et al. Recommendations on the use of 18F-FDG PET in oncology. J. Nucl. Med. 2008, 49, 480–508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stefano, A.; Porcino, N.; Banna, G.; Russoa, G.; Mocciaro, V.; Anile, G.; Gieri, S.; Cosentino, S.; Murè, G.; Baldari, S.; et al. Metabolic response assessment in non-small cell lung cancer patients after platinum-based therapy: A preliminary analysis. Curr. Med. Imaging Rev. 2015, 11, 218–227. [Google Scholar] [CrossRef]
- Banna, G.L.; Anile, G.; Russo, G.; Vigneri, P.; Castaing, M.; Nicolosi, M.; Strano, S.; Gieri, S.; Spina, R.; Patanè, D.; et al. Predictive and Prognostic Value of Early Disease Progression by PET Evaluation in Advanced Non-Small Cell Lung Cancer. Oncology 2017, 92, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Cegla, P.; Kazmierska, J.; Gwozdz, S.; Czepczynski, R.; Malicki, J.; Cholewinski, W. Assessment of biological parameters in head and neck cancer based on in vivo distribution of 18F-FDG-FLT-FMISO-PET/CT images. Tumori 2019, 106, 33–38. [Google Scholar] [CrossRef]
- Wahl, R.L.; Jacene, H.; Kasamon, Y.; Lodge, M.A. From RECIST to PERCIST: Evolving Considerations for PET response criteria in solid tumors. J. Nucl. Med. 2009, 50 (Suppl. 1), 122S–150S. [Google Scholar] [CrossRef] [Green Version]
- Borasi, G.; Russo, G.; Alongi, F.; Nahum, A.; Candiano, G.; Stefano, A.; Gilardi, M.C.; Messa, C. Radiotherapy and High Intensity Focused Ultrasound in Oncology: Competition or integration? A future scenario. J. Ther. Ultrasound 2013, 1, 6. [Google Scholar] [CrossRef] [Green Version]
- Levivier, M.; Wikier, D.; Goldman, S.; David, P.; Metens, T.; Massager, N.; Gerosa, M.; Devriendt, D.; Desmedt, F.; Simon, S.; et al. Integration of the metabolic data of positron emission tomography in the dosimetry planning of radiosurgery with the gamma knife: Early experience with brain tumors. Technical note. J. Neurosurg. 2000, 93 (Suppl. 3), 233–238. [Google Scholar] [CrossRef]
- Stefano, A.L.; Gallivanone, F.; Messa, C.L.; Gilardi, M.C.L.; Castiglioni, I. Metabolic impact of Partial Volume Correction of [18F]FDG PET-CT oncological studies on the assessment of tumor response to treatment. Q. J. Nucl. Med. Mol. Imaging 2014, 58, 413–423. [Google Scholar] [PubMed]
- D`Urso, D.; Stefano, A.; Romano, A.; Russo, G.; Cosentino, S.; Fallanca, F.; Gioe, M.; Attanasio, M.; Sabini, M.G.; Di Raimondo, F.; et al. Analysis of Metabolic Parameters Coming from Basal and Interim PET in Hodgkin Lymphoma. Curr. Med. Imaging Rev. 2017, 14, 533–544. [Google Scholar] [CrossRef]
- van Velden, F.H.P.; Cheebsumon, P.; Yaqub, M.; Smit, E.F.; Hoekstra, O.S.; Lammertsma, A.A.; Boellaard, R. Evaluation of a cumulative SUV-volume histogram method for parameterizing heterogeneous intratumoural FDG uptake in non-small cell lung cancer PET studies. Eur. J. Nucl. Med. Mol. Imaging 2011, 38, 1636–1647. [Google Scholar] [CrossRef] [Green Version]
- Nariai, T.; Tanaka, Y.; Wakimoto, H.; Aoyagi, M.; Tamaki, M.; Ishiwata, K.; Senda, M.; Ishii, K.; Hirakawa, K.; Ohno, K. Usefulness of L-[methyl-11C] methionine—Positron emission tomography as a biological monitoring tool in the treatment of glioma. J. Neurosurg. 2005, 103, 498–507. [Google Scholar] [CrossRef] [PubMed]
- Stefano, A.; Vitabile, S.; Russo, G.; Ippolito, M.; Sardina, D.; Sabini, M.G.; Gallivanone, F.; Castiglioni, I.; Gilardi, M.C. A Graph-Based Method for PET Image Segmentation in Radiotherapy Planning: A Pilot Study. In Image Analysis and Processing—ICIAP 2013; Lecture Notes in Computer Science; Springer: Berlin/Heidelberg, Germany, 2013; pp. 711–720. [Google Scholar]
- Stefano, A.; Comelli, A.; Bravatà, V.; Barone, S.; Daskalovski, I.; Savoca, G.; Sabini, M.G.; Ippolito, M.; Russo, G. A preliminary PET radiomics study of brain metastases using a fully automatic segmentation method. BMC Bioinform. 2020, 21, 325. [Google Scholar] [CrossRef] [PubMed]
- Miwa, K.; Matsuo, M.; Shinoda, J.; Aki, T.; Yonezawa, S.; Ito, T.; Asano, Y.; Yamada, M.; Yokoyama, K.; Yamada, J.; et al. Clinical Value of [11C]Methionine PET for Stereotactic Radiation Therapy With Intensity Modulated Radiation Therapy to Metastatic Brain Tumors. Int. J. Radiat. Oncol. 2012, 84, 1139–1144. [Google Scholar] [CrossRef] [PubMed]
- Grosu, A.L.; Weber, W.a.; Riedel, E.; Jeremic, B.; Nieder, C.; Franz, M.; Gumprecht, H.; Jaeger, R.; Schwaiger, M.; Molls, M. L-(methyl-11C) methionine positron emission tomography for target delineation in resected high-grade gliomas before radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2005, 63, 64–74. [Google Scholar] [CrossRef] [PubMed]
- Grosu, A.L.; Weber, W.A.; Franz, M.; Stärk, S.; Piert, M.; Thamm, R.; Gumprecht, H.; Schwaiger, M.; Molls, M.; Nieder, C. Reirradiation of recurrent high-grade gliomas using amino acid PET (SPECT)/CT/MRI image fusion to determine gross tumor volume for stereotactic fractionated radiotherapy. Int. J. Radiat. Oncol. 2005, 63, 511–519. [Google Scholar] [CrossRef]
- Tu, Z.; Mach, R.H. C-11 Radiochemistry in Cancer Imaging Applications. Curr. Top. Med. Chem. 2010, 10, 1060–1095. [Google Scholar] [CrossRef] [PubMed]
- Drzymala, R.E.; Mohan, R.; Brewster, L.; Chu, J.; Goitein, M.; Harms, W.; Urie, M. Dose-volume histograms. Int. J. Radiat. Oncol. 1991, 21, 71–78. [Google Scholar] [CrossRef]
- Stefano, A.; Vitabile, S.; Russo, G.; Ippolito, M.; Marletta, F.; D’Arrigo, C.; D’Urso, D.; Gambino, O.; Pirrone, R.; Ardizzone, E.; et al. A fully automatic method for biological target volume segmentation of brain metastases. Int. J. Imaging Syst. Technol. 2016, 26, 29–37. [Google Scholar] [CrossRef]
- Soret, M.; Bacharach, S.L.; Buvat, I.I. Partial-volume effect in PET tumor imaging. J. Nucl. Med. 2007, 48, 932–945. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El Naqa, I.; Grigsby, P.; Apte, A.; Kidd, E.; Donnelly, E.; Khullar, D.; Chaudhari, S.; Yang, D.; Schmitt, M.; Laforest, R.; et al. Exploring feature-based approaches in PET images for predicting cancer treatment outcomes. Pattern Recognit. 2009, 42, 1162–1171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stefano, A.; Vitabile, S.; Russo, G.; D’Urso, D.; Ippolito, M.; Marletta, F.; Sabini, M.G.; Patti, I.V.; Pittera, S.; Sardina, D.; et al. Biological target volume segmentation for radiotherapy treatment planning. Phys. Medica 2016, 32, 64. [Google Scholar] [CrossRef]
- Comelli, A.; Bignardi, S.; Stefano, A.; Russo, G.; Sabini, M.G.; Ippolito, M.; Yezzi, A. Development of a new fully three-dimensional methodology for tumours delineation in functional images. Comput. Biol. Med. 2020, 120, 103701. [Google Scholar] [CrossRef] [PubMed]
- Comelli, A.; Stefano, A.; Russo, G.; Sabini, M.G.; Ippolito, M.; Bignardi, S.; Petrucci, G.; Yezzi, A. A smart and operator independent system to delineate tumours in Positron Emission Tomography scans. Comput. Biol. Med. 2018, 102, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Comelli, A.; Stefano, A.; Benfante, V.; Russo, G. Normal and Abnormal Tissue Classification in Positron Emission Tomography Oncological Studies. Pattern Recognit. Image Anal. 2018, 28, 106–113. [Google Scholar] [CrossRef]
- Kang, S.R.; Song, H.C.; Byun, B.H.; Oh, J.R.; Kim, H.S.; Hong, S.P.; Kwon, S.Y.; Chong, A.; Kim, J.; Cho, S.G.; et al. Intratumoral Metabolic Heterogeneity for Prediction of Disease Progression After Concurrent Chemoradiotherapy in Patients with Inoperable Stage III Non-Small-Cell Lung Cancer. Nucl. Med. Mol. Imaging (2010) 2014, 48, 16–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takeshita, T.; Morita, K.; Tsutsui, Y.; Kidera, D.; Mikasa, S.; Maebatake, A.; Akamatsu, G.; Miwa, K.; Baba, S.; Sasaki, M. The influence of respiratory motion on the cumulative SUV-volume histogram and fractal analyses of intratumoral heterogeneity in PET/CT imaging. Ann. Nucl. Med. 2016, 30, 393–399. [Google Scholar] [CrossRef] [PubMed]
- Stefano, A.; Gioè, M.; Russo, G.; Palmucci, S.; Torrisi, S.E.; Bignardi, S.; Basile, A.; Comelli, A.; Benfante, V.; Sambataro, G.; et al. Performance of Radiomics Features in the Quantification of Idiopathic Pulmonary Fibrosis from HRCT. Diagnostics 2020, 10, 306. [Google Scholar] [CrossRef] [PubMed]
- Comelli, A.; Stefano, A.; Coronnello, C.; Russo, G.; Vernuccio, F.; Cannella, R.; Salvaggio, G.; Lagalla, R.; Barone, S. Radiomics: A New Biomedical Workflow to Create a Predictive Model. In Medical Image Understanding and Analysis; Communications in Computer and Information Science; Springer: Cham, Switzerland, 2020; pp. 280–293. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
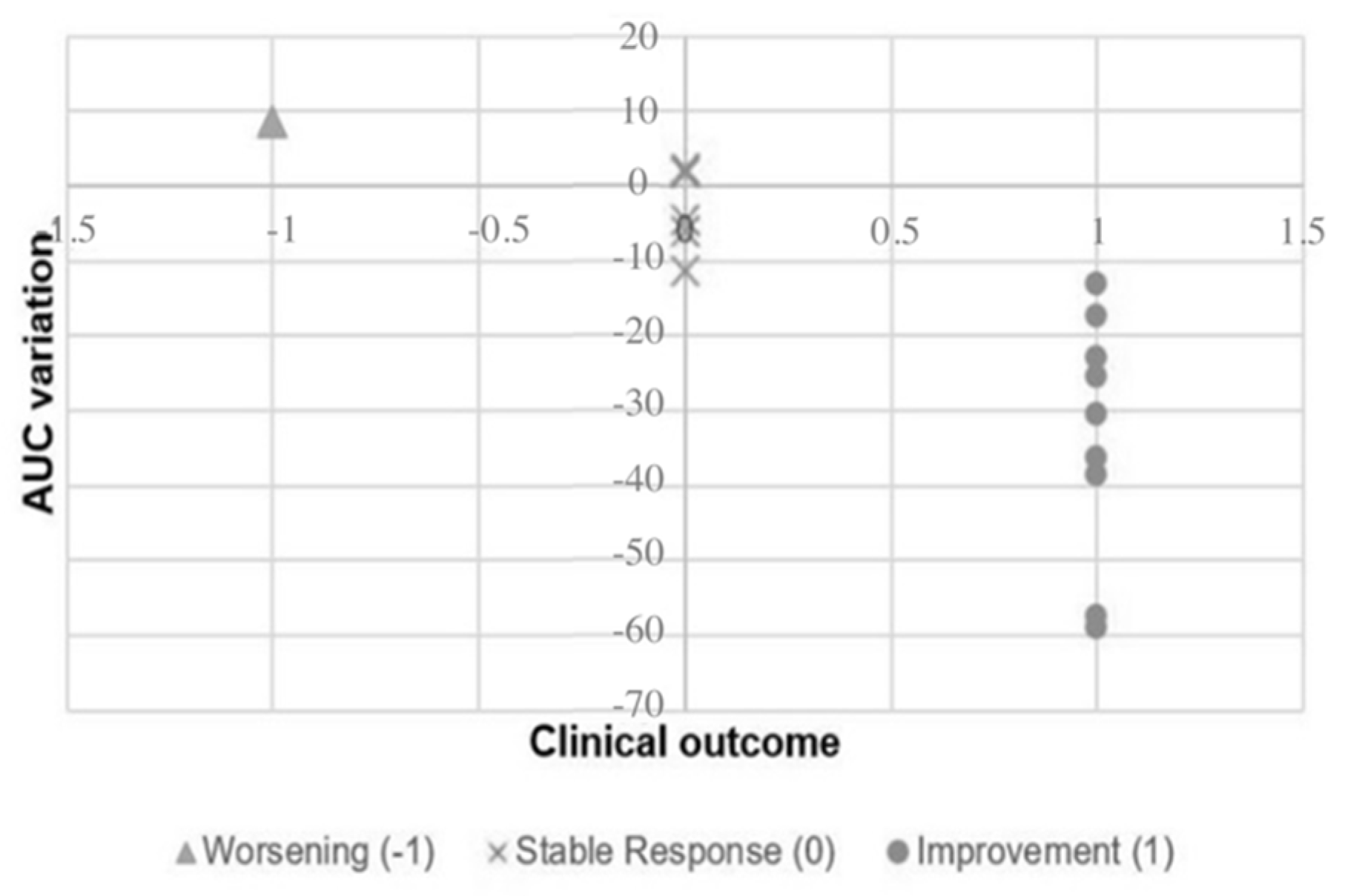
| Patient N. | ΔAUC | ΔMTV | ΔSUVmax | ΔSUVmean | ΔTLG | Physician Report |
|---|---|---|---|---|---|---|
| #1 | 2.33 | 13.87 | −12.63 | −12.18 | 0.05 | Stable |
| #2 | −38.62 | 18.80 | −32.72 | −25.73 | −11.77 | Improvement |
| #3 | −59.05 | 0.12 | −47.66 | −33.56 | −33.48 | Improvement |
| #4 | −17.43 | −62.72 | −20.23 | −5.91 | −64.93 | Improvement |
| #5 | −57.59 | −81.16 | −41.83 | −14.34 | −83.86 | Improvement |
| #6 | −36.42 | 24.85 | −44.36 | −40.85 | −26.15 | Improvement |
| #7 | 8.62 | −16.90 | 9.47 | 10.10 | −8.50 | Worsening |
| #8 | 16 | −100 | −100 | −100 | −100 | Complete Response |
| #9 | −11.22 | 7.73 | −2.29 | −5.56 | 1.73 | Stable |
| #10 | −4.61 | −13.27 | −11.28 | 3.08 | −10.60 | Stable |
| #11 | −30.37 | −31.53 | −26.21 | −17.96 | −43.83 | Improvement |
| #12 | −13.07 | 14.14 | −22.74 | −17.40 | −5.72 | Improvement |
| #13 | −23.03 | −94.29 | −34.64 | −10.65 | −94.90 | Improvement |
| #14 | −25.48 | −62.20 | −30.11 | −11.82 | −66.67 | Improvement |
| #15 | 1.88 | −61.12 | −1.00 | 4.34 | −59.43 | Stable |
| #16 | −6.11 | −5.06 | −33.55 | −13.41 | −17.80 | Stable |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stefano, A.; Pisciotta, P.; Pometti, M.; Comelli, A.; Cosentino, S.; Marletta, F.; Cicero, S.; Sabini, M.G.; Ippolito, M.; Russo, G. Early Monitoring Response to Therapy in Patients with Brain Lesions Using the Cumulative SUV Histogram. Appl. Sci. 2021, 11, 2999. https://0-doi-org.brum.beds.ac.uk/10.3390/app11072999
Stefano A, Pisciotta P, Pometti M, Comelli A, Cosentino S, Marletta F, Cicero S, Sabini MG, Ippolito M, Russo G. Early Monitoring Response to Therapy in Patients with Brain Lesions Using the Cumulative SUV Histogram. Applied Sciences. 2021; 11(7):2999. https://0-doi-org.brum.beds.ac.uk/10.3390/app11072999
Chicago/Turabian StyleStefano, Alessandro, Pietro Pisciotta, Marco Pometti, Albert Comelli, Sebastiano Cosentino, Francesco Marletta, Salvatore Cicero, Maria G. Sabini, Massimo Ippolito, and Giorgio Russo. 2021. "Early Monitoring Response to Therapy in Patients with Brain Lesions Using the Cumulative SUV Histogram" Applied Sciences 11, no. 7: 2999. https://0-doi-org.brum.beds.ac.uk/10.3390/app11072999