1. Introduction
Periodontal disease (PD) consists of a chronic inflammatory destruction of tooth-supporting tissues caused by the action of specific anaerobic pathogens contained in dental plaque [
1]. If not treated, PD can lead to tooth loss, as well as impaired quality of life, and important systemic inflammation [
2].
A strict correlation between diabetes and periodontal disease was assessed [
3,
4]. In fact, periodontal disease is considered the sixth complication of diabetes [
5]. Diabetic patients with concomitant periodontal disease generally have a worse glycemic control and a higher prevalence of diabetes-related complications [
6]. It was also demonstrated that the glycemic control is strictly correlated with incidence and gravity of periodontal disease [
7,
8], as well as that the treatment of PD is able to improve the metabolic control [
9].
Different pathogenetic mechanisms to explain how hyperglycemia could affect the periodontal status have been proposed, e.g., an excessive inflammatory response to infection, a decreased reparative reaction, and the action of advanced glycation end products. In addition, periodontal disease could affect glycemic control in diabetic patients through chronic inflammation [
1]. On the basis of these considerations, PD should be carefully regarded as an important aspect of the clinical care of diabetic patients.
Diabetes mellitus (DM) is mainly classified into two different types, type 1 and type 2 DM. Type 1 DM (T1DM) is associated with the autoimmune destruction of pancreatic β-cells, resulting in the failure of insulin production, whereas type 2 DM (T2DM) is characterized by PD. Hyperglycemia was mainly found in T2DM patients [
10], as it can be deduced considering previous literature [
3]. Anyway, according to a recent systematic review [
1], even T1DM is related to the onset of PD, as the number of patients affected was twice as those of non-diabetic ones. Moreover, among T1DM patients, PD seems to be more severe, with significant differences between subjects under glycemic control.
Probiotics are living microorganisms that are able to exert a beneficial action on human health and are being used in recent years for the prevention and treatment of oral diseases like periodontitis. The strains generally used are
Bifidobacterium and
Lactobacillus. According to the recent systematic review by Hardan et al., the use of probiotics seems to be beneficial for the improvement of some clinical periodontal parameters [
11]. Notwithstanding their positive effects, several shortcomings on probiotics should be taken into consideration; specifically, the safety of live microorganisms should be carefully evaluated in cases of older and immunocompromised patients making use of them. Accordingly, the novel non-viable probiotics are named paraprobiotics (tyndallized probiotics). Their beneficial role is explained by the fact that they are inactivated microbial cells that do not present risks to the host thanks to their anti-inflammatory, antiproliferative, and antioxidant actions, with a regulation of adaptive and innate immune systems, and an antagonistic role against pathogens [
12].
The objective of the present report is to evaluate the effect of two domiciliary oral hygiene protocols on the periodontal clinical status as well as on the amount of glycosylated hemoglobin (HbA1c) in patients affected by T1DM. In particular, a natural extracts-based toothpaste and probiotics-based agents have been chosen due to their wide diffusion among products for oral care.
The first null hypothesis of the study is that no significant differences occur between the two groups considering the periodontal evaluation. The second null hypothesis is that no significant differences neither occur for the amount of HbA1c.
2. Materials and Methods
2.1. Materials
The composition of the products tested in the present report is shown in
Table 1 [
12,
13]. In order to reduce the bias, products by the same manufacturer (Coswell S.p.A., Funo di Argelato, BO, Italy) differing for the active ingredients but not for the excipients have been chosen.
2.2. Trial Design
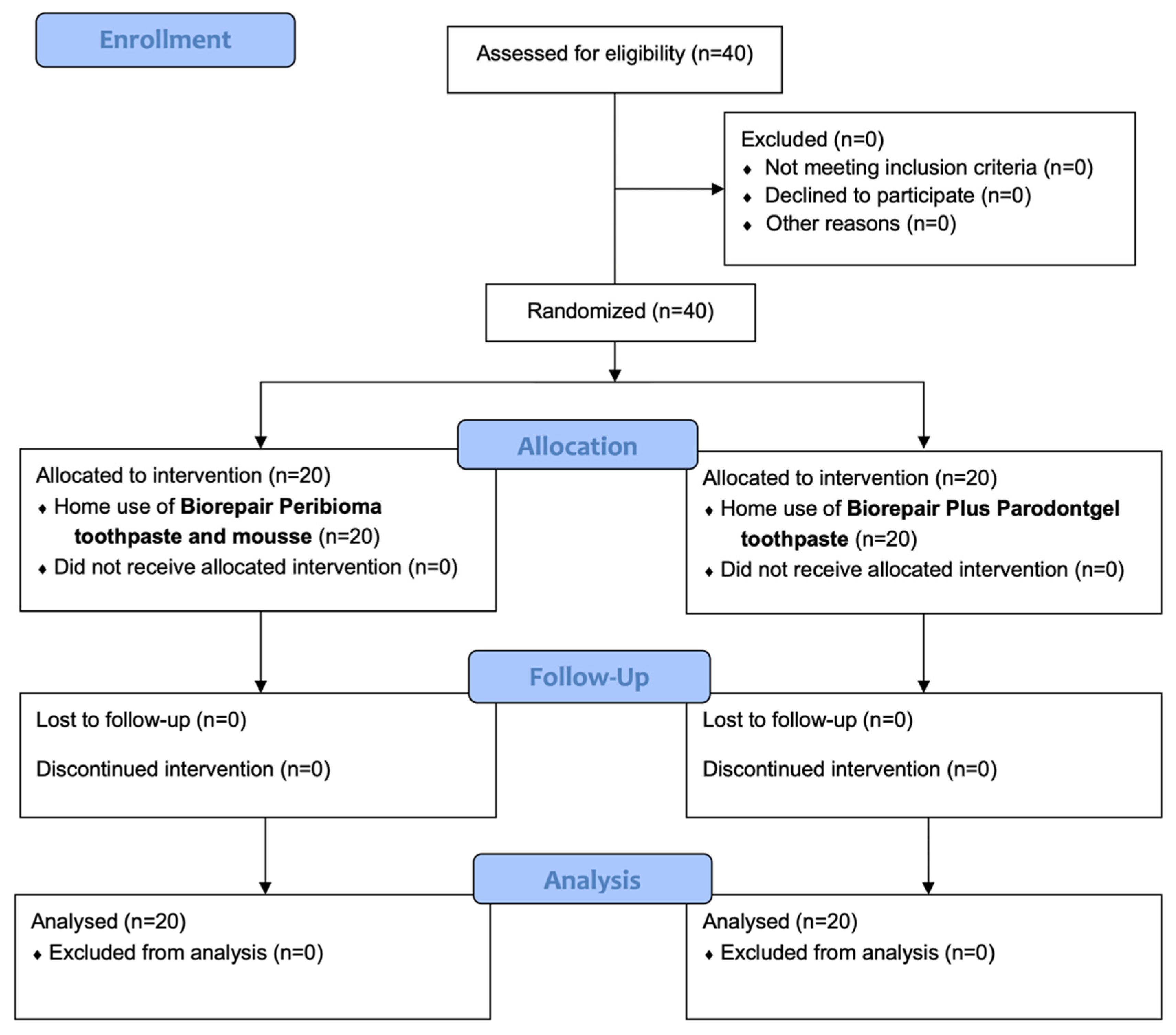
This was a single center, parallel group, randomized clinical trial with a 1:1 allocation ratio, approved by the Unit Internal Review Board (registration number: 2021-0224) and registered on Clinicaltrials.gov (NCT number: NCT04865809).
2.3. Participants
Patients diagnosed with diabetes type 1 at the Department of Internal Medicine, Geriatric and Diabetology Unit, University of Pavia, Italy were referred to the Unit of Dental Hygiene, Section of Dentistry, Department of Clinical, Surgical, Diagnostic and Pediatric Sciences of the University of Pavia (Pavia, Italy) for periodontal evaluation. The objectives of the study were explained to patients fulfilling the inclusion criteria, and they asked to participate. After signing the informed consent, they were enrolled from May 2021 to July 2021.
The inclusion criteria adopted are presented in
Table 2.
2.4. Interventions and Outcomes
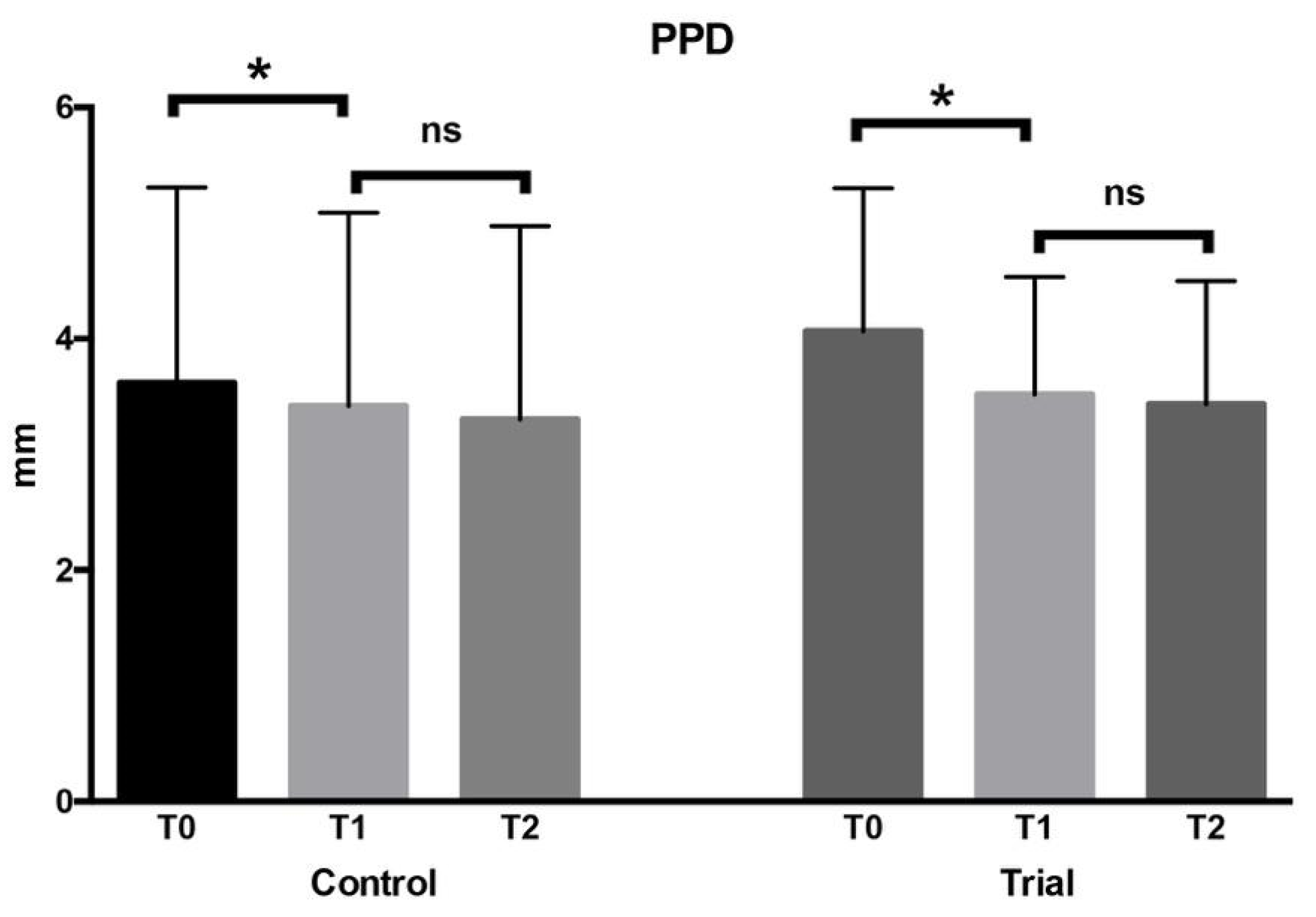
At the first appointment (T0), patients signed the informed consent. Glycosylated hemoglobin (HbA1c) was measured with a blood sample before each dental procedure. After that, an instructed operator collected the following periodontal indexes by means of a probe (UNC probe 15; Hu-Friedy, Chicago, IL, USA): Probing Pocket Depth (PPD) (measured on six sites per element) [
15], Bleeding on Probing (BOP) [
13], Bleeding Score (BS) [
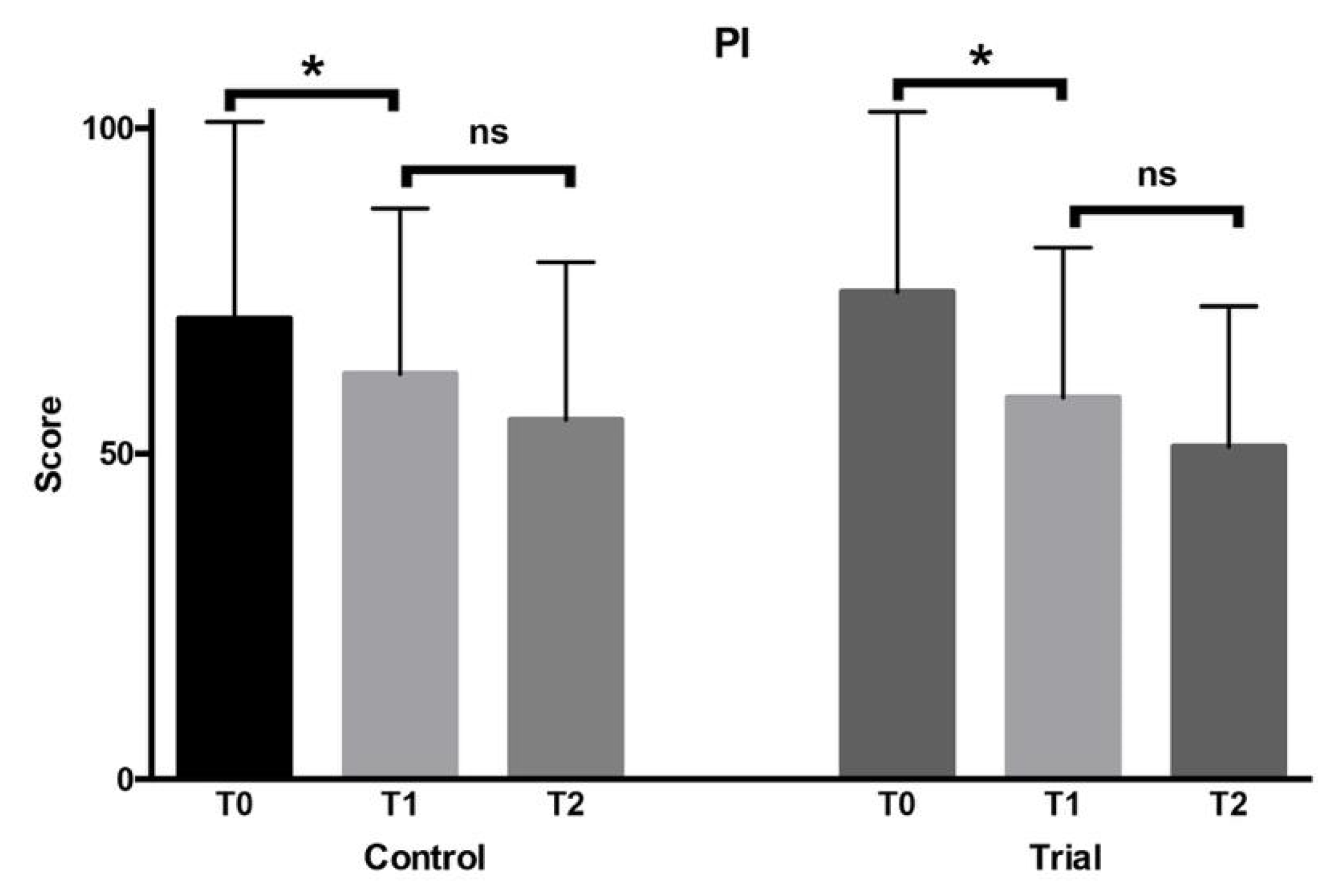
16], and Plaque Index (PI) [
15]. Then, professional oral hygiene was performed with a piezoelectric instrument (Multipiezo, Mectron S.p.a, Carasco, Italy) and Gracey curettes (Hu-Friedy, Chicago, IL, USA). Ozonized water was administered with the Aquolab
® professional device (Aquolab s.r.l. EB2C S.r.l., Milano, Italy) using the following parameters: 45° angulation of the nozzle, 60 s time per site, 12 V tension, and ozone level 3 [
16].
Participants received verbal instructions on domiciliary oral hygiene with a soft-bristled electric toothbrush to be used twice a day for 2 min. They were asked to perform a supervised brushing session in front of a mirror under the supervision of the dental hygienist to check if a correct brushing technique was used. At this stage, they were randomly assigned into two groups according to the different home treatment: in the trial group, Biorepair Toothpaste and Mousse were used; in the control group, Biorepair Plus Parodontgel toothpaste was used. The planned follow-ups were after 3 months from baseline (T1) and after 6 months (T2). At each appointment, the periodontal examination with the collection of clinical indexes and the blood sample for HbA1c assessment were performed.
2.5. Sample Size
The sample size calculation (Alpha = 0.05; Power = 80%) for two independent study groups and a continuous primary endpoint was calculated considering the “glycosylated hemoglobin (HbA1c)” variable. The expected mean was supposed to be 7.35 with a standard deviation of 1.82, and the expected difference between the means was supposed to be 1.62; therefore, 20 patients per group were required for the study [
16]. No dropout rate was calculated for the present study [
17,
18,
19].
2.6. Randomization and Blinding
A block randomization table was used to allocate patients. The data analyst provided a randomization sequence, considering a permuted block of 40 total participants. An operator enrolled the participants and executed the professional oral procedures, collecting all the above mentioned indexes. On the basis of previously prepared sequentially numbered, opaque, sealed envelopes (SNOSE), an assistant assigned each participant to the respective group, concealing the products for home use. The data analyst was blinded for the allocation and outcomes.
2.7. Statistical Methods
Data underwent statistical analysis with R Software (R version 3.1.3, R Development Core Team, R Foundation for Statistical Computing, Wien, Austria). For each group and variable, descriptive statistics (mean, standard deviation, minimum, median, and maximum) were calculated. PPD and CAL were calculated in millimeters; BOP, PI, and HbA1c were calculated in percentage. Data normality was confirmed by the Kolmogorov–Smirnov test. Then, an ANOVA test followed by post hoc Tukey tests were performed for inferential comparisons. Significance was predetermined for p < 0.05 for all the statistical tests.
4. Discussion
According to current studies, the most significant evidence regarding the link between periodontitis and systemic conditions encompasses the biunivocal relationship between periodontal inflammation and DM [
21,
22]. Periodontitis consists of a plaque-induced inflammation of the periodontium. The pathogenic importance of periodontal inflammation in T2DM has been extensively demonstrated, whereas the link between T1DM and periodontitis has not been extensively investigated. Paraprobiotics are non-viable microorganisms that may provide benefits to the host thanks to their anti-inflammatory, immunomodulatory, anti-proliferative, antioxidant, and antimicrobial activity. Even the influence of paraprobiotics on patients with T1DM represents an unexplored field.
Accordingly, the objective of the present report was to compare the effect of two domiciliary oral hygiene protocols (the experimental one based on paraprobiotics) on the periodontal clinical status as well as on the amount of glycosylated hemoglobin (HbA1c) in patients affected by type 1 diabetes mellitus.
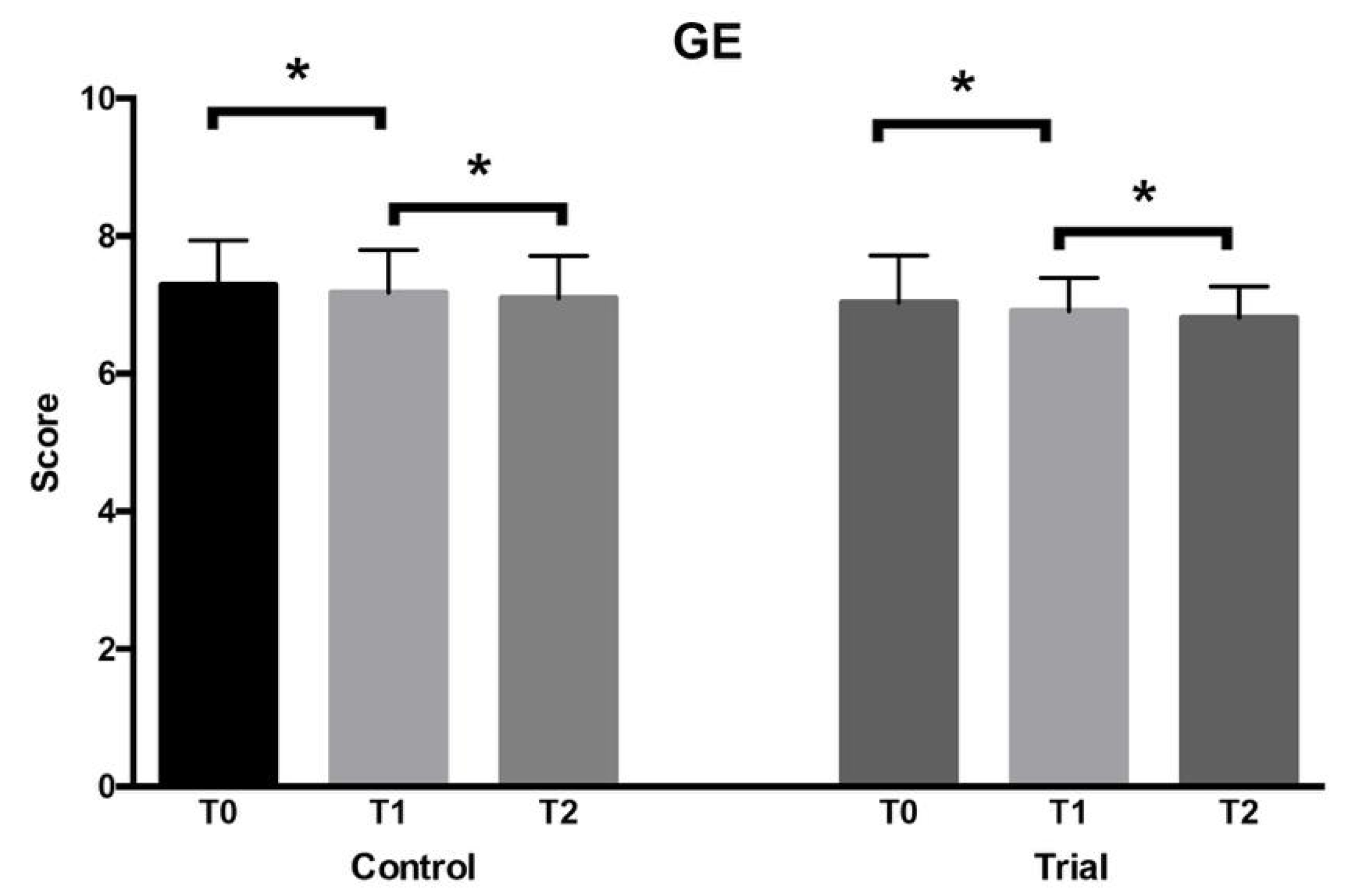
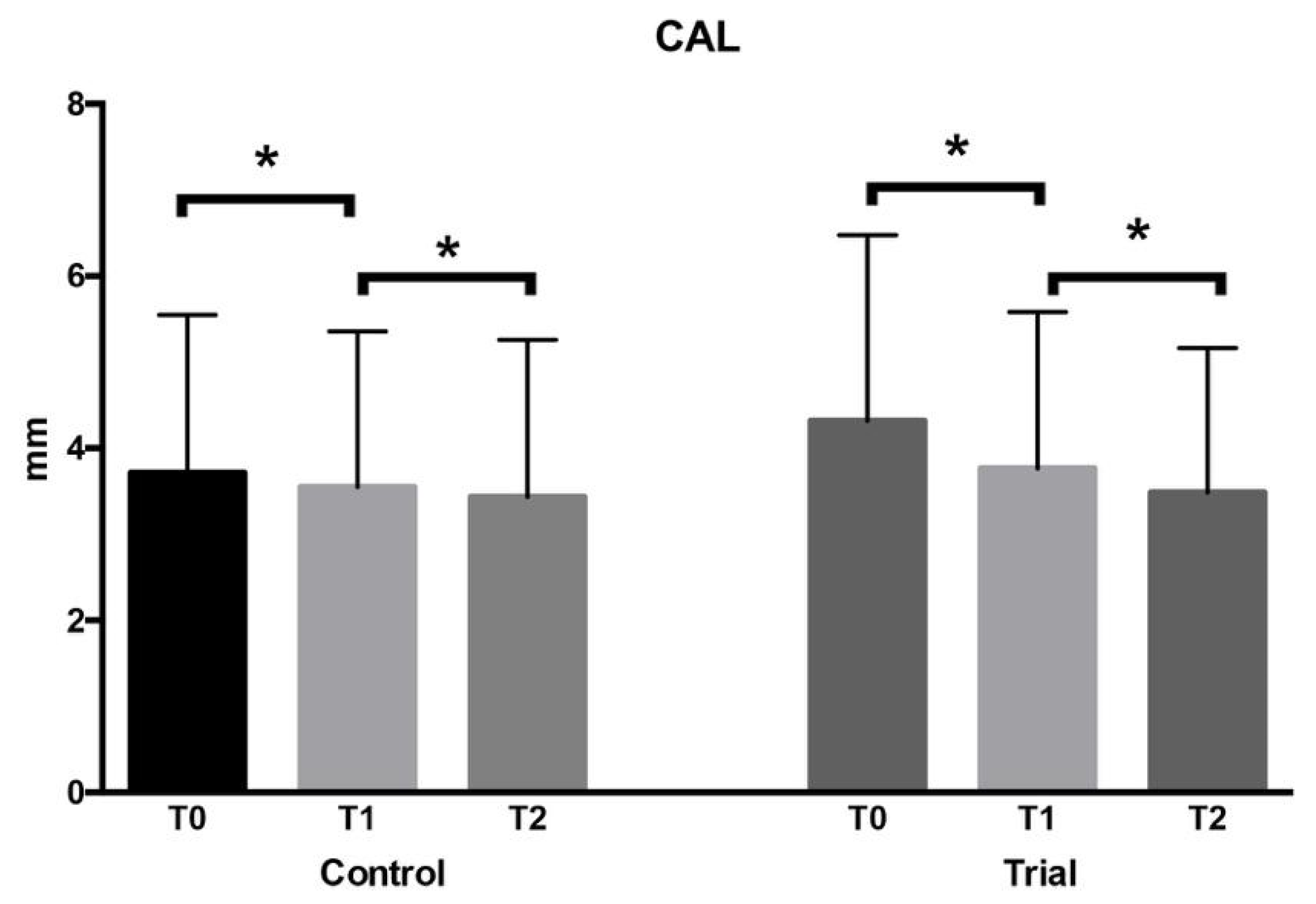
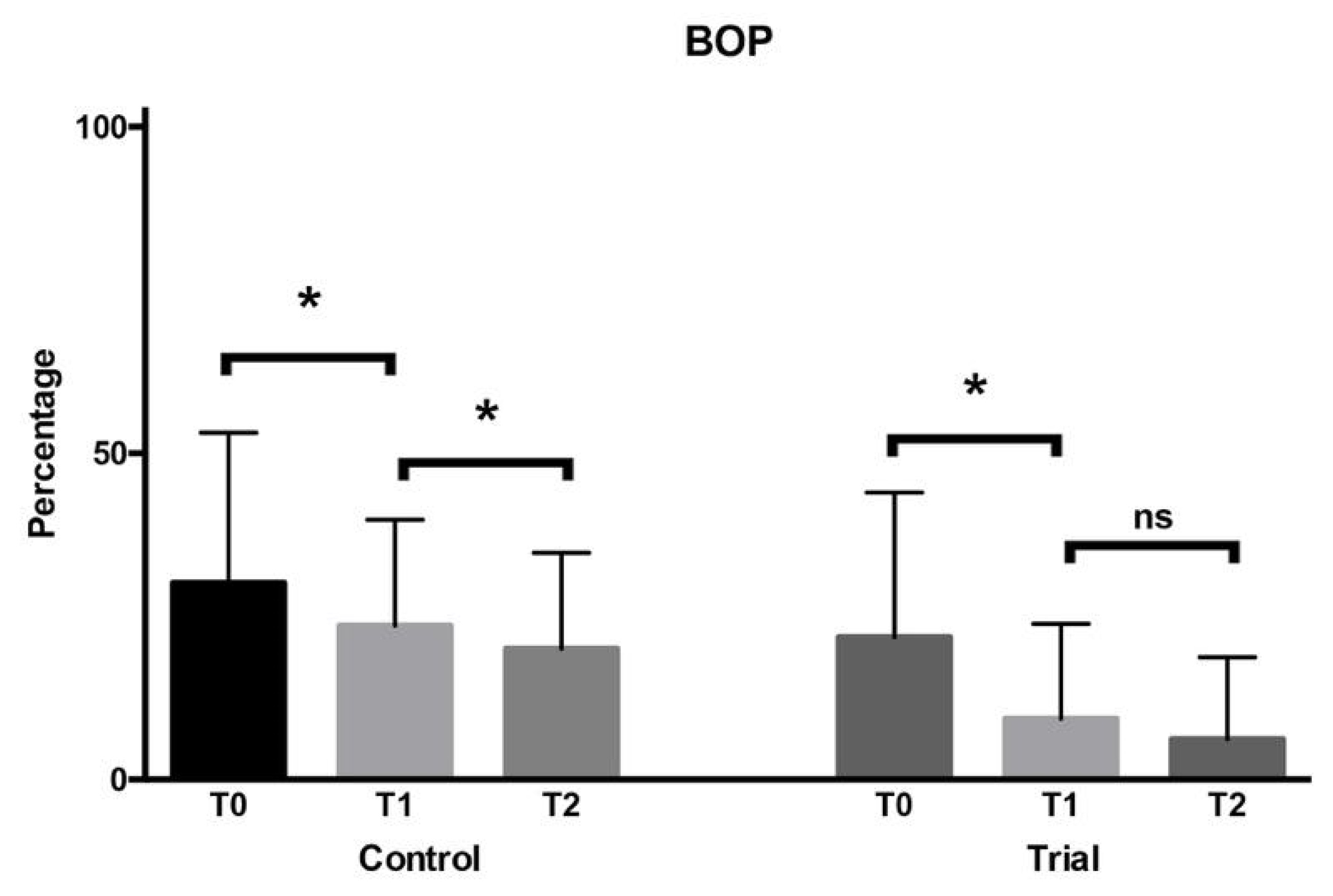
The first null hypothesis of the study has been rejected. In fact, significant differences were found for the clinical periodontal parameters considered in the study. In particular, PPD significantly decreased from baseline to the subsequent 3 months, with no further significant reductions at 6 months. No significant intergroup differences have been assessed comparing the control and trial group. Additionally, the same intergroup and intragroup differences have been found for PI. Therefore, both the use of probiotics-based toothpaste and mouthwash, as well as the use of a natural extracts-based toothpaste, resulted in a similar improvement of PPD and PI, as expected, with a reduction in the pathological values starting from the first endpoint. Conversely, CAL significantly decreased in both groups only after 6 months from the baseline, with no significant intergroup differences even in this case. The different pattern of variation of CAL, if compared to PPD and PI, could be explained by the fact that the reconstitution of the attachment level requires a longer time to occur. Finally, as regards BoP, a significant progressive reduction occurred at every endpoint starting from the baseline in the trial group, whereas in the group treated with the natural extracts-toothpaste the reduction at 3 months from the baseline was more significant, and no further significant reductions were assessed at 6 months.
On the basis of these considerations, both the combination of the probiotics-based toothpaste and mouthwash and the use of the natural extracts-based toothpaste similarly led to an improvement of PPD, PI, and CAL. Probiotics are defined as ”live microorganisms which when administered in adequate amounts confer a health benefit on the host” (FAO/WHO) [
23]. Their positive action is still an object of study, and possible explanations can be found in the exclusion of pathogenetic bacteria and the competition with pathogenetic bacteria for nutrients and epithelial cell adhesion, the production of antimicrobial molecules towards these harmful microorganisms, the enhancement of the mucosal barrier function, and the reestablishment of the physiological immunomodulatory function of the host [
24]. According to a recent study, probiotics provide valid support to non-surgical periodontal treatment, with a positive improvement on periodontal indexes and a decrease in specific periodontal bacteria; additionally, it has been suggested that probiotics not only reduce microbic counts but also exert an immunomodulatory action, thus switching from a pro-inflammatory towards an anti-inflammatory response [
16].
The improvement of BoP occurred in both groups, but was more evident for the trial one: the more evident influence of Biorepair Parodontgel Plus toothpaste on the BoP could be explained by the effect of its content, which includes soothing extracts like Lactoferrin, hamamelis virginiana leaf extract, Spirulina platensis extract, Calendula officinalis flower extract, and tocopheryl acetate. This outcome confirms previous findings demonstrating the high influence of hyaluronic acid and lactoferrin-based toothpaste on periodontal bleeding indexes [
14]. In particular, the effect of Biorepair Parodontgel Plus toothpaste on BoP could be ascribed to its content of lactoferrin. The anti-inflammatory action of this element has been studied both by means of in vitro periodontitis models as well as through observational clinical studies: in vitro lactoferrin has shown strong anti-inflammatory properties against gingival fibroblasts infected with the periodontopathogen
Prevotella intermedia, whereas in vivo the topical administration to periodontal patients leads to the decrease of cytokines levels in crevicular fluid and other inflammatory periodontal indexes [
25]. Furthermore, Biorepair Plus Parodontgel contains tocopheryl acetate (vitamin E), an antioxidant agent whose positive role in periodontitis has been suggested [
26].
Considering oral hygiene and the periodontal status, previous research has demonstrated the relationship between these two factors. For example, Vidya et al. [
27] have found among children with T1DM that caries prevalence and gingival health in permanent dentition are affected by metabolic control: with lower levels of glycemia, the caries prevalence and gingival inflammation increased. Interestingly, the association between oral hygiene and diabetes has been shown to be bidirectional: on one hand, periodontitis could be a potential complication of diabetes, but, on the other hand, the increased levels of periodontal inflammatory markers, such as C-reactive protein and interleukin-6, are found to be significant risk factors for T2DM [
28]. According to a recent systematic review with meta-analysis, scaling and root planing exert a positive effect on metabolic control (i.e., reduction of HbA1c) and reduction in systemic inflammation (decrease of C-reactive protein, CRP) in patients with T2DM [
29].
According to the findings of the study, only the natural extracts-based toothpaste caused a significant decrease of HbA1c, whereas the probiotics-based agents had no influence. This could be due to a more anti-inflammatory power of the natural extracts exerting not only a local effect but also a systemic one. This outcome appears to be particular interesting from a clinical point of view. According to Ismail et al. [
30], the literature highlights that worse periodontal parameters are found among children with T1DM. Accordingly, every effort should be made by clinicians to ensure proper oral hygiene protocols to these patients, considering their systemic condition.
The main limitations of the present report relate to the recruitment of participants without stratification based on metabolic control (patients under control and patients not under control) as well as to the relatively short follow-up. Moreover, patients might not have correctly performed the oral hygiene procedures verbally given, and their dietary habits have also not been taken into account, which might have influenced the results of the study. Future evaluations should be conducted to verify whether the effect of the oral hygiene products tested might be different in patients depending on their metabolic control, and to assess the effect even at a long term. Moreover, besides clinical indexes, additional parameters like inflammatory and microbiological ones should be assessed. Finally, the frequency, quantity, and kind of food income throughout the day should be evaluated.


 ,
, 








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}