
Periodontal Disease Diagnosis in the Context of Oral Rehabilitation Approaches

 ,
,  ,
,
Abstract
:1. Introduction
2. Aim of the Study
3. Materials and Methods
3.1. Paraclinical Section
3.2. Clinical Section
3.3. Statistical Analysis
4. Results
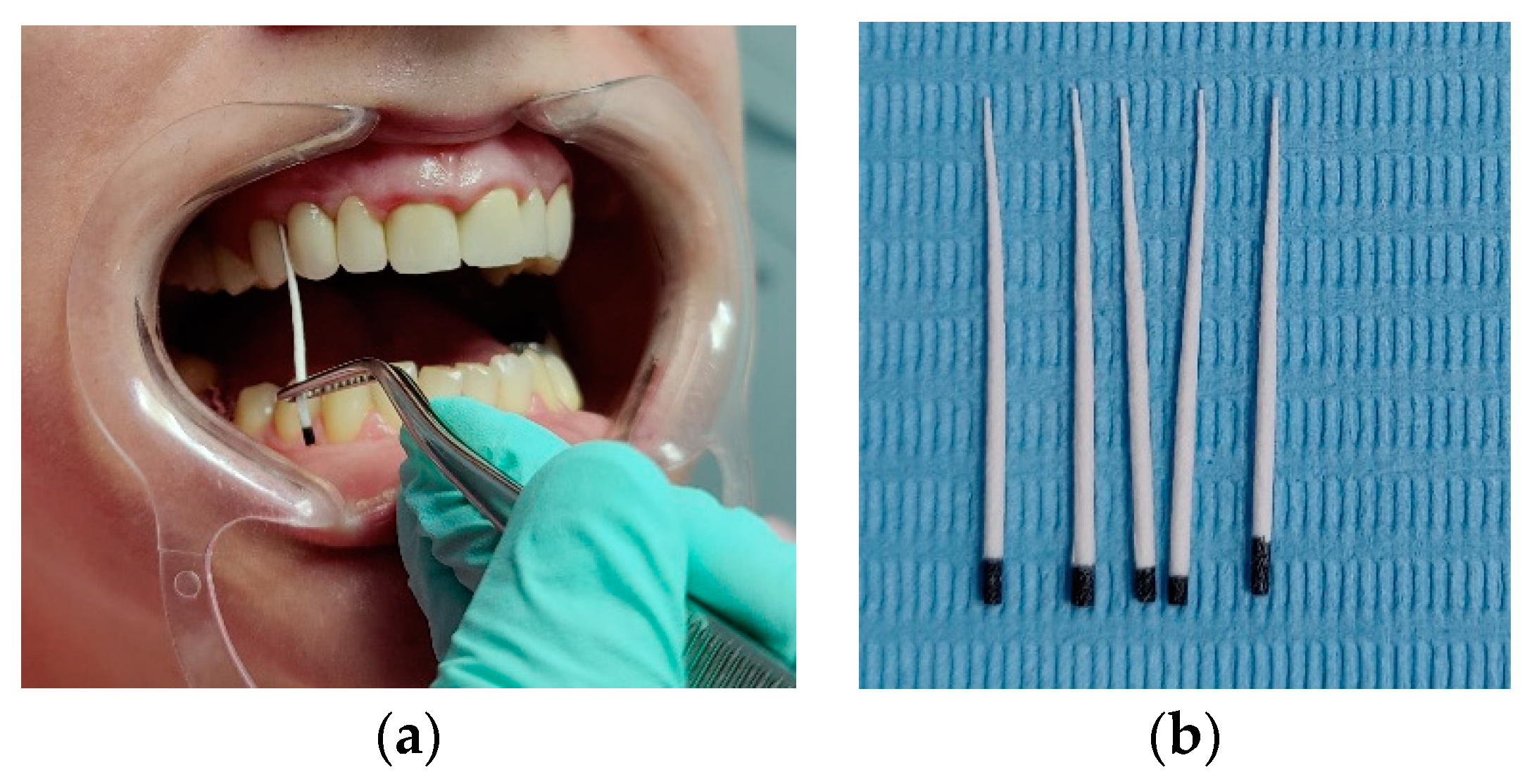
- 2% methyl blue,
- 1% fuchsia solution,
- fluorescent substances (Figure 2)
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| PD | periodontal disease |
| SS | stomatognathic system |
| TMJ | temporomandibular joint |
| PCR | polymerase chain reaction |
| DSSS | dysfunctional syndrome of stomatognathic system |
| PET | pozitron emission test |
| GCF | gingival crevicularfFluid |
| qPCR | quantitative PCR (qPCR) test is used to detect, characterize, and quantify nucleic acids |
References
- Raitapuro-Murray, T.; Molleson, T.I.; Hughes, F.J. The prevalence of periodontal disease in a Romano-British population c 200-400 AD. Br. Dent. J. 2014, 217, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Irani, S. Periodontitis and oral cancer-current concepts of the etiopathogenesis. Oncol. Rev. 2020, 14, 465. [Google Scholar] [CrossRef] [PubMed]
- Casanova, L.; Hughes, F.J.; Preshaw, P.M. Diabetes and periodontal disease: A two-way relationship. Br. Dent. J. 2014, 217, 433–437. [Google Scholar] [CrossRef]
- World Health Organization. WHO Global Oral Health Data. 2020. Available online: http://www.who.int/oral_health/databases/niigata/en (accessed on 15 June 2022).
- Lang, N.P.; Berglundh, T.; Giannobile, W.V.; Sanz, M. (Eds.) Lindhe’s Clinical Periodontology and Implant Dentistry, 7th ed.; 2 Volume Set; John Wiley and Sons Ltd.: Hoboken, NJ, USA, 2021. [Google Scholar]
- Carranza, F.A.; Newman, M.G.; Takei, H.H.; Klokkevold, P. Carranza’s Clinical Periodontology; Saunders Elsevier: St. Louis, MO, USA, 2006; pp. 1039–1049. [Google Scholar]
- Eke, P.I.; Dye, B.A.; Wei, L.; Slade, G.D.; Thornton-Evans, G.O.; Borgnakke, W.S.; Taylor, G.W.; Page, R.C.; Beck, J.D.; Genco, R.J. Update on Prevalence of Periodontitis in Adults in the United States: NHANES 2009 to 2012. J. Periodontol. 2015, 86, 611–622. [Google Scholar] [CrossRef] [PubMed]
- Song, L.; Dong, G.; Guo, L.; Graves, D.T. The function of dendritic cells in modulating the host response. Mol. Oral Microbiol. 2018, 33, 13–21. [Google Scholar] [CrossRef]
- Damgaard, C.; Holmstrup, P.; Van Dyke, T.E.; Nielsen, C.H. The complement system and its role in the pathogenesis of periodontitis: Current concepts. J. Periodontal. Res. 2015, 50, 283–293. [Google Scholar] [CrossRef]
- Rebelo Vieira, J.M.; Rebelo, M.A.; Martins, N.M.; Gomes, J.F.; Vettore, M.V. Contextual and individual determinants of non-utilization of dental services among Brazilian adults. J. Public Health Dent. 2019, 79, 60–70. [Google Scholar] [CrossRef]
- Meyle, J.; Dommisch, H.; Groeger, S.; Giacaman, R.A.; Costalonga, M.; Herzberg, M. The innate host response in caries and periodontitis. J. Clin. Periodontol. 2017, 44, 1215–1225. [Google Scholar] [CrossRef]
- Hajishengallis, G.; Sahingur, S.E. Novel inflammatory pathways in periodontitis. Adv. Dent. Res. 2014, 26, 23–29. [Google Scholar] [CrossRef]
- Khurshid, Z.; Naseem, M.; Sheikh, Z.; Najeeb, S.; Shahab, S.; Zafar, M.S. Oral antimicrobial peptides: Types and role in the oral cavity. Saudi Pharm. J. 2016, 24, 515–524. [Google Scholar] [CrossRef] [Green Version]
- Livingstone, D.; Murthy, V.; Reddy, V.K.; Pillai, A. Prosthodontic rehabilitation of a patient with aggressive periodontitis. BMJ Case Rep. 2015, 2015, bcr2014204588. [Google Scholar] [CrossRef]
- Herrera, D.; Alonso, B.; de Arriba, L.; Santa Cruz, I.; Serrano, C.; Sanz, M. Acute periodontal lesions. Periodontology 2000 2014, 65, 149–177. [Google Scholar] [CrossRef]
- Almeida, M.L.; Tôrres, A.C.; Oliveira, K.C.; Calderon, P.D.; Carreiro, A.D.; Gurgel, B.C. Longitudinal improvement in periodontal parameters between RPD abutment teeth with direct and indirect retainers, after periodontal therapy. J. Prosthodont. 2019, 28, e440–e444. [Google Scholar] [CrossRef]
- Pjetursson, B.E.; Sailer, I.; Makarov, N.A.; Zwahlen, M.; Thoma, D.S. All-ceramic or metal-ceramic tooth-supported fixed dental prostheses (FDPs)? A systematic review of the survival and complication rates. Part II: Multiple-unit FDPs. Dent. Mater. 2015, 31, 624–639. [Google Scholar] [CrossRef]
- Müller, S.; Eickholz, P.; Reitmeir, P.; Eger, T. Long-term tooth loss in periodontally compromised but treated patients according to the type of prosthodontic treatment. A retrospective study. J. Oral Rehabil. 2013, 40, 358–367. [Google Scholar] [CrossRef] [PubMed]
- Anner, R.; Grossmann, Y.; Anner, Y.; Levin, L. Smoking, diabetes mellitus, periodontitis, and supportive periodontal treatment as factors associated with dental implant survival: A long-term retrospective evaluation of patients followed for up to 10 years. Implant. Dent. 2010, 19, 57–64. [Google Scholar] [CrossRef]
- Ercoli, C.; Caton, J.G. Dental prostheses and tooth-related factors. J. Clin. Periodontol. 2018, 45 (Suppl. S20), S207–S218. [Google Scholar] [CrossRef]
- Marya, C.M. (Ed.) Dental Indices. In A Textbook of Public Health Dentistry; JP Medical Ltd.: New Delhi, India, 2014; p. 203. [Google Scholar]
- Azodo, C.C.; Erhabor, P. Management of tooth mobility in the periodontology clinic: An overview and experience from a tertiary healthcare setting. Afr. J. Med. Health Sci. 2016, 15, 50, ISSN 2384-5589. S2CID 77435443. [Google Scholar] [CrossRef]
- Sindhuja, S.; Balaji, A. Tooth Mobility. Eur. J. Molecul. Clinic. Med. 2020, 7, 671–673. [Google Scholar]
- Martu, M.-A.; Surlin, P.; Lazar, L.; Maftei, G.A.; Luchian, I.; Gheorghe, D.-N.; Rezus, E.; Toma, V.; Foia, L.-G. Evaluation of Oxidative Stress before and after Using Laser and Photoactivation Therapy as Adjuvant of Non-Surgical Periodontal Treatment in Patients with Rheumatoid Arthritis. Antioxidants 2021, 10, 226. [Google Scholar] [CrossRef]
- Teodorescu, A.C.; Martu, I.; Teslaru, S.; Kappenberg-Nitescu, D.C.; Goriuc, A.; Luchian, I.; Martu, M.A.; Solomon, S.M.; Mârțu, S. Assessment of salivary levels of RANKL and OPG in aggressive versus chronic periodontitis. J. Immunol. Res. 2019, 28, 2019. [Google Scholar] [CrossRef] [Green Version]
- Solomon, S.M.; Timpu, D.; Forna, D.A.; Stefanache, M.A.M.; Martu, S.; Stoleriu, S. AFM comparative study of root surface morphology after three methods of scaling. Mater. Plast. 2016, 53, 546–549. [Google Scholar]
- Popa, C.G.; Luchian, I.; Ioanid, N.; Goriuc, A.; Martu, I.; Bosinceanu, D.; Martu, M.A.; Tirca, T.; Martu, S. ELISA Evaluation of RANKL Levels in Gingival Fluid in Patients with Periodontitis and Occlusal Trauma. Rev. Chim. 2018, 69, 1578–1580. [Google Scholar] [CrossRef]
- Nicolae, V.; Neamtu, B.; Picu, O.; Stefanache, M.A.M.; Cioranu, V.S.I. The comparitive evaluation of salivary biomarkers (calcium, phosphate, salivary pH) in the cario-resistance versus cario-activity. Rev. Chim. 2016, 68, 821–824. [Google Scholar]
- Taraboanta, I.; Stoleriu, S.; Nica, I.; Georgescu, A.; Gamen, A.C.; Maftei, G.A.; Andrian, S. Roughness variation of a nonhybrid composite resin submitted to acid and abrasive challenges. Int. J. Med. Dent. 2020, 24, 182–187. [Google Scholar]
- Martu, M.A.; Maftei, G.A.; Luchian, I.; Popa, C.; Filioreanu, A.M.; Tatarciuc, D.; Nichitean, G.; Hurjui, L.-L.; Foia, L.-G. Wound healing of periodontal and oral tissues: Part II—Patho-phisiological conditions and metabolic diseases. Rom. J. Oral Rehabil. 2020, 12, 30–40. [Google Scholar]
- Periodontitis and cardiovascular diseases: Consensus report. J. Clin. Periodontol. 2020, 47, 268–288. [CrossRef]
- Periodontal disease and cancer: Epidemiologic studies and possible mechanisms. Periodontology 2000 2020, 83, 213–233. [CrossRef]
- Periodontal Disease and Vitamin D Deficiency in Pregnant Women: Which Correlation with Preterm and Low-Weight Birth? J. Clin. Med. 2021, 2, 4578. [CrossRef]
- Functional status and oral health in patients with amyotrophic lateral sclerosis: A cross-sectional study. NeuroRehabilitation 2021, 48, 49–57. [CrossRef]
- Martu, M.A.; Solomon, S.M.; Toma, V.; Maftei, G.A.; Iovan, A.; Gamen, A.; Hurjui, L.; Rezus, E.; Foia, L.; Forna, N.C. The importance of cytokines in periodontal disease and rheumatoid arthritis. Review. Rom. J. Oral Rehabil. 2019, 11, 220–240. [Google Scholar]
- Luchian, I.; Goriuc, A.; Martu, M.A.; Covasa, M. Clindamycin as an Alternative Option in Optimizing Periodontal Therapy. Antibiotics 2021, 10, 814. [Google Scholar] [CrossRef]
- Maftei, G.-A.; Martu, M.-A.; Martu, M.-C.; Popescu, D.; Surlin, P.; Tatarciuc, D.; Popa, C.; Foia, L.-G. Correlations between Salivary Immuno-Biochemical Markers and HbA1c in Type 2 Diabetes Subjects before and after Dental Extraction. Antioxidants 2021, 10, 1741. [Google Scholar] [CrossRef]
- Maftei, G.A.; Martu, C.M.; Popa, C.; Geletu, G.; Danila, V.; Jelihovschi, I.; Foia, L. The biomechanical properties of suture materials and their relationship to bacterial adherence. Mater. Plast. 2019, 56, 980–985. [Google Scholar] [CrossRef]
- Cioloca, D.P.; Foia, L.; Holban, C.; Trandafirescu, M.; Poroch, V.; Maxim, D.; Jipu, R.; Costuleanu, M.; Toma, V. Systemic diabetic context-induced biochemical periodontal alterations in children. Rev. Chim. 2016, 67, 2409–2412. [Google Scholar]
- Surlin, P.; Gheorhe, D.N.; Popescu, D.M.; Martu, A.; Solomon, S.; Roman, A.; Lazar, L.; Stratul, I.; Rusu, D.; Foia, L.; et al. Interleukin-1α and -1β assessment in the gingival crevicular fluid of periodontal patients with chronic hepatitis C. Exp. Ther. Med. 2020, 20, 2381–2386. [Google Scholar] [CrossRef]
- Vlad, C.E.; Foia, L.; Popescu, R.; Ivanov, I.; Luca, C.M.; Delianu, C.; Toma, V.; Statescu, C.; Rezus, C.; Florea, L. Apolipoproteins A and B and PCSK9: Non-Traditional Cardiovascular Risk Factors in Chronic Kidney Disease and in End-Stage Renal Disease. J. Diabet. Res. 2019, 2, 238–242. [Google Scholar] [CrossRef] [Green Version]
- Pontes Espíndola, L.C.; Picão, R.C.; Casas Novas Mançano, S.M.; Martins do Souto, R.; Vieira Colombo, A.P. Prevalence and antimicrobial susceptibility of Gram-negative bacilli in subgingival biofilm associated with periodontal diseases. J. Periodontol. 2022, 93, 69–79. [Google Scholar] [CrossRef]
- Murariu, A.; Hanganu, C.; Vasluianu, R. Oral impact on quality of life among young adults in Iasi. Rom. J. Oral Rehab. 2012, 4, 18–22. [Google Scholar]
- Vasluianu, R.I.; Ungureanu, D.; Jitaru, D.; Ioanid, A.D.; Forna, N.C. Crevicular C-telopeptide and C-propeptide of type I collagen are markers of parodontal disease evolution in diabetic and non-diabetic patients. Rev. Română Med. Lab. 2012, 20, 173–180. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Total (n = 390) | Study Sample (n = 195) | Control Sample (n = 195) | p-Value | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Gender | 1.000 † | ||||||
| M | 140 | 3.9 | 70 | 35.9% | 70 | 35.9% | |
| F | 250 | 64.1 | 125 | 64.1% | 125 | 64.1% | |
| Age group | 0.919 † | ||||||
| 20–29 yrs | 43 | 11.0% | 21 | 10.8% | 22 | 11.3% | |
| 30–39 yrs | 45 | 11.5% | 20 | 10.3% | 25 | 12.8% | |
| 40–49 yrs | 63 | 16.2% | 33 | 16.9% | 30 | 15.4% | |
| 50–59 yrs | 94 | 2.1% | 46 | 23.6% | 48 | 24.6% | |
| 60–69 yrs | 145 | 37.2% | 75 | 38.5% | 70 | 35.9% | |
| Subgingival tartar | 0.919 † | ||||||
| absent | 221 | 56.7% | 110 | 56.4% | 111 | 56.9% | |
| present | 169 | 43.3% | 85 | 43.6% | 84 | 43.1% | |
| Gingival recession | 0.463 † | ||||||
| absent | 245 | 62.8% | 119 | 61.0% | 126 | 64.6% | |
| present | 145 | 37.2% | 76 | 39.0% | 69 | 35.4% | |
| Periodontal pockets | 0.059 † | ||||||
| absent | 144 | 36.9% | 81 | 41.5% | 63 | 32.3% | |
| present | 246 | 63.1% | 114 | 58.5% | 132 | 67.7% | |
| Dental mobility | <0.001 **,† | ||||||
| 0 | 179 | 45.9% | 106 | 54.4% | 73 | 37.4% | |
| 1 | 123 | 31.5% | 63 | 32.3% | 60 | 30.8% | |
| 2 | 66 | 16.9% | 23 | 11.8% | 43 | 22.1% | |
| 3 | 22 | 5.6% | 3 | 1.5% | 19 | 9.7% | |
| Plaque index PI (m ± SD) | 0.354 ± 0.252 | 0.376 ± 0.248 | 0.333 ± 0.255 | 0.085 ‡ | |||
| Bleeding index BI (m ± SD) | 0.361 ± 0.247 | 0.479 ± 0.228 | 0.244 ± 0.206 | <0.001 **,‡ | |||
| Gingival index GI (m ± SD) | 0.370 ± 0.243 | 0.466 ± 0.208 | 0.275 ± 0.239 | <0.001 **,‡ | |||
| PDP index (m ± SD) | 2.630 ± 0.191 | 2.522 ± 0.212 | 2.722 ± 0.102 | <0.001 **,‡ | |||
| Subgingival Tartar | ||||||
|---|---|---|---|---|---|---|
| Parameter | Total (n = 390) | Study Sample (n = 195) | Control Sample (n = 195) | |||
| Absent n (%) | Present n (%) | Absent n (%) | Present n (%) | Absent n (%) | Present n (%) | |
| Gender | p = 0.776 † | p = 0.294 † | p = 0.516 † | |||
| M | 78 (35.3%) | 62 (36.7%) | 36 (32.7%) | 34 (40.0%) | 42 (37.8%) | 28 (33.3%) |
| F | 143 (64.7%) | 107 (63.3%) | 74 (67.3%) | 51 (60.0%) | 69 (62.2%) | 56 (66.7%) |
| Age group | p < 0.001 **,† | p = 0.003 **,† | p = 0.003 **,† | |||
| 20–29 yrs | 41 (18.6%) | 2 (1.2%) | 20 (18.2%) | 1(1.2%) | 21 (18.9%) | 1 (1.2%) |
| 30–39 yrs | 27 (12.2%) | 18 (10.7%) | 12 (10.9%) | 8 (9.4%) | 15 (13.5%) | 10 (11.9%) |
| 40–49 yrs | 36 (16.3%) | 27 (16.0%) | 19 (17.3%) | 14 (16.5%) | 17 (15.3%) | 13 (15.5%) |
| 50–59 yrs | 47 (21.3%) | 47 (27.8%) | 23 (20.9%) | 23 (27.1%) | 24 (21.6%) | 24 (28.6%) |
| 60–69 yrs | 70 (31.7%) | 75 (44.4%) | 36 (32.7%) | 39 (45.9%) | 34 (30.6%) | 36 (42.9%) |
| Gingival recession | p < 0.001 **,† | p < 0.001 **,† | p < 0.001 **,† | |||
| absent | 181 (81.9%) | 64 (37.9%) | 87 (79.1%) | 32 (37.6%) | 94 (84.7%) | 32 (38.1%) |
| present | 40 (18.1%) | 105 (62.1%) | 23 (20.9%) | 53 (62.4%) | 17 (15.3%) | 52 (61.9%) |
| Periodontal pockets | p < 0.001 **,† | p < 0.001 **,† | p = 0.012 *,† | |||
| absent | 114 (51.6%) | 30 (17.8%) | 70 (63.6%) | 11 (12.9%) | 44 (39.6%) | 19 (22.6%) |
| present | 107 (48.4%) | 139 (82.2%) | 40 (36.4%) | 74 (87.1%) | 67 (60.4%) | 65 (77.4%) |
| Dental mobility | p < 0.001 **,† | p < 0.001 **,† | p < 0.001 **,† | |||
| 0 | 140 (63.3%) | 39 (23.1%) | 86 (78.2%) | 20 (23.5%) | 54 (48.6%) | 19 (22.6%) |
| 1 | 56 (25.3%) | 67 (39.6%) | 18 (16.4%) | 45 (52.9%) | 38 (34.2%) | 22 (26.2%) |
| 2 | 24 (10.9%) | 42 (24.9%) | 5 (4.5%) | 18 (21.2%) | 19 (17.1%) | 24 (28.6%) |
| 3 | 1 (0.5%) | 21 (12.4%) | 1 (0.9%) | 2 (2.4%) | 0 (0.0%) | 19 (22.6%) |
| Plaque index PI (m ± SD) | p = 0.001 **,‡ | p = 0.602 ‡ | p < 0.001 **,‡ | |||
| 0.307 ± 0.204 | 0.416 ± 0.293 | 0.368 ±0.244 | 0.386 ± 0.253 | 0.248 ± 0.130 | 0.446 ± 0.328 | |
| Bleeding index BI (m ± SD) | p = 0.001 **,‡ | p = 0.328 ‡ | p < 0.001 **,‡ | |||
| 0.323 ± 0.230 | 0.411 ± 0.260 | 0.464 ± 0.225 | 0.497 ± 0.232 | 0.184 ± 0.128 | 0.324 ± 0.258 | |
| Gingival index GI (m ± SD) | p < 0.001 **,‡ | p = 0.207 ‡ | p < 0.001 **,‡ | |||
| 0.330 ± 0.234 | 0.422 ± 0.246 | 0.452 ± 0.208 | 0.484 ± 0.207 | 0.210 ± 0.193 | 0.360 ± 0.267 | |
| PDP index (m ± SD) | p = 0.754 ‡ | p = 0.766 ‡ | p = 00.029 *,‡ | |||
| 2.638 ± 0.177 | 2.623 ± 0.201 | 2.529 ± 0.226 | 2.520 ± 0.212 | 2.704± 0.091 | 2. 741 ± 0.110 | |
| Study Sample—With Bacteria Counting (n = 35) | ||
|---|---|---|
| n (%) | m ± SD | |
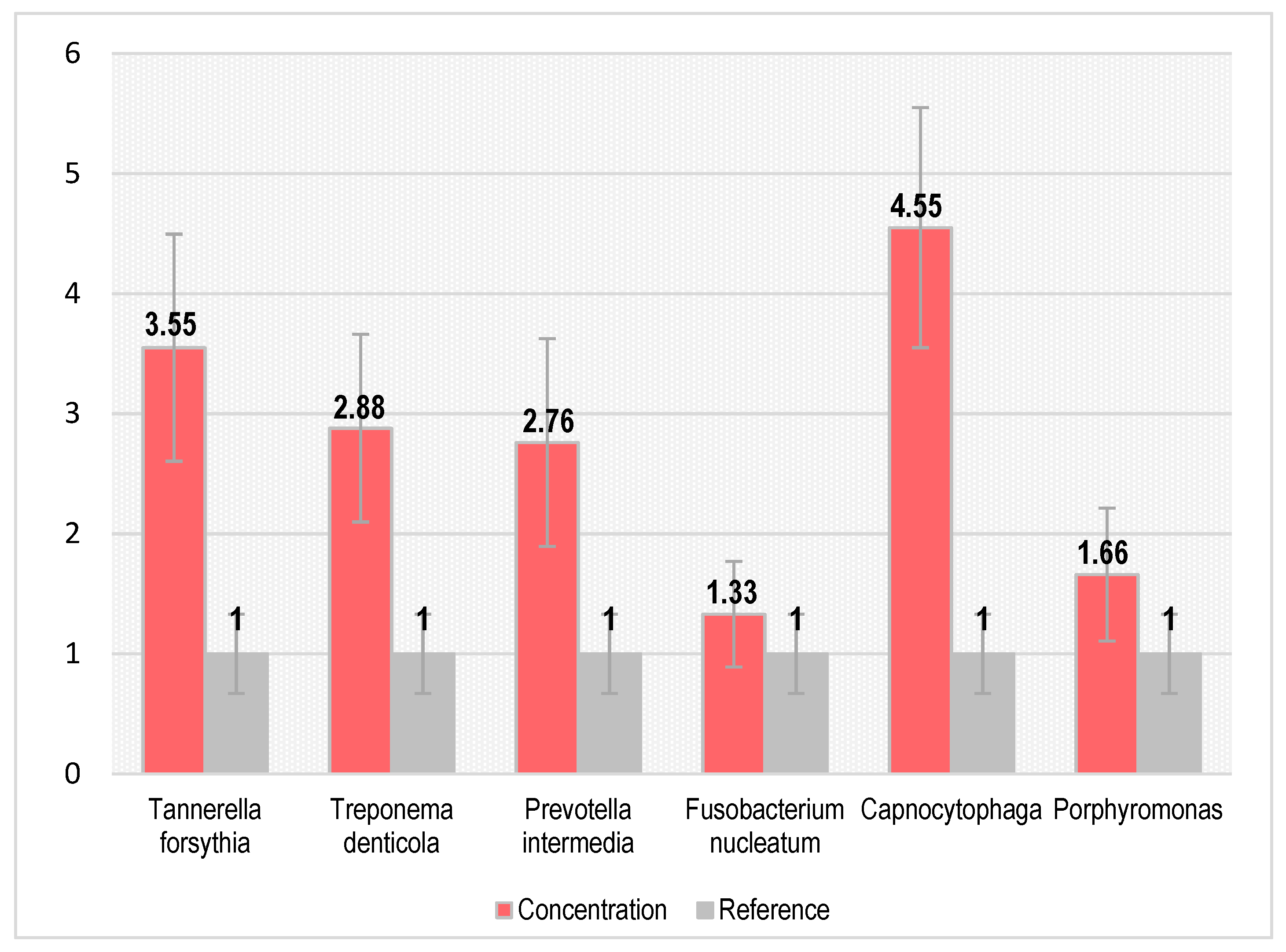
| Tannerella forsythia | 27 (77.1%) | 3.554 ± 0.946 |
| Treponema denticola | 32 (91.4%) | 2.883 ± 0.782 |
| Prevotella intermedia | 22 (62.9%) | 2.763 ± 0.865 |
| Fusobacterium nucleatum | 30 (85.7%) | 1.328 ± 0.439 |
| Capnocytophaga | 12 (34.3%) | 4.547 ± 1.068 |
| Porphyromonas | 28 (80.0%) | 1.658 ± 0.554 |
| Index (m ± SD) | Time | p-Value † | ||||
|---|---|---|---|---|---|---|
| Initially | 3 Months | 6 Months | 0 vs. 3 m | 3 m vs. 6 m | 0 vs. 6 m | |
| Control sample (n = 195) | ||||||
| Plaque index PI | 0.333 ± 0255 | 0.473 ± 0.504 | 0.685 ± 0.668 | p < 0.001 **,† | p < 0.001 **,† | p < 0.001 **,† |
| Bleeding index BI | 0.244 ± 0206 | 0.530 ± 0.101 | 0.550 ± 0.100 | p < 0.001 **,† | p < 0.001 **,† | p < 0.001 **,† |
| Gingival index GI | 0.275 ± 0239 | 0.415 ± 0.200 | 0.522 ± 0.317 | p < 0.001 **,† | p < 0.001 **,† | p < 0.001 **,† |
| PDP index | 2.722 ± 0102 | 3.210 ± 0.201 | 3.640 ± 0.803 | p < 0.001 **,† | p < 0.001 **,† | p < 0.001 **,† |
| Study sample—without bacteria counting (n = 160) | ||||||
| Plaque index PI | 0.381 ± 0247 | 0.360 ± 0.206 | 0.354 ± 0.202 | p < 0.001 **,† | p < 0.001 **,† | p < 0.001 **,† |
| Bleeding index BI | 0.481 ± 0219 | 0.471 ±0.260 | 0.463 ± 0.247 | p = 0.006 ** | p < 0.001 **,† | p < 0.001 **,† |
| Gingival index GI | 0.465 ± 0195 | 0.433 ± 0.203 | 0.434 ± 0.220 | p < 0.001 **,† | p = 0.868 | p < 0.001 **,† |
| PDP index | 2.538 ± 0179 | 2.382 ± 0.260 | 2.420 ±0.187 | p < 0.001 **,† | p = 0.004 ** | p < 0.001 **,† |
| Study sample—with bacteria counting (n = 35) | ||||||
| Plaque index PI | 0.352 ± 0252 | 0.334 ± 0.214 | 0.327 ± 0.214 | p = 0.015 * | p = 0.005 ** | p = 0.006 ** |
| Bleeding index BI | 0.467 ± 0269 | 0.454 ± 0.306 | 0.451 ± 0.288 | p = 0.097 | p = 0.853 | p = 0.005 ** |
| Gingival index GI | 0.467 ± 0260 | 0.440 ± 0.270 | 0.450 ±0.284 | p < 0.001 **,† | p = 0.025 * | p = 0.021 * |
| PDP index | 2.489 ± 0273 | 2.359 ± 0.334 | 2.269 ± 0.375 | p < 0.001 **,† | p < 0.001 **,† | p < 0.001 **,† |
| Plaque Index PI | Bleeding Index BI | Gingival Index GI | PDP Index | |||||
|---|---|---|---|---|---|---|---|---|
| r | p | r | p | r | p | r | p | |
| Tannerella forsythia | 0.354 | 0.070 | 0.274 | 0.167 | 0.126 | 0.532 | 0.194 | 0.332 |
| Treponema denticola | 0.393 | 0.026 * | 0.322 | 0.072 | 0.329 | 0.066 | 0.381 | 0.031 * |
| Prevotella intermedia | 0.388 | 0.075 | 0.427 | 0.048 * | 0.465 | 0.029 * | 0.446 | 0.038 * |
| Fusobacterium nucleatum | 0.362 | 0.049 * | 0.277 | 0.138 | 0.130 | 0.495 | 0.081 | 0.670 |
| Capnocytophaga | 0.776 | 0.003 * | 0.662 | 0.019 * | 0.605 | 0.037 * | 0.431 | 0.162 |
| Porphyromonas | 0.381 | 0.045 * | 0.335 | 0.081 | 0.293 | 0.131 | 0.254 | 0.191 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Checherita, L.E.; Antohe, M.E.; Stamatin, O.; Rudnic, I.; Lupu, I.C.; Croitoru, I.; Surdu, A.; Cioloca, D.; Gradinaru, I.; Francu, L.; et al. Periodontal Disease Diagnosis in the Context of Oral Rehabilitation Approaches. Appl. Sci. 2022, 12, 9067. https://0-doi-org.brum.beds.ac.uk/10.3390/app12189067
Checherita LE, Antohe ME, Stamatin O, Rudnic I, Lupu IC, Croitoru I, Surdu A, Cioloca D, Gradinaru I, Francu L, et al. Periodontal Disease Diagnosis in the Context of Oral Rehabilitation Approaches. Applied Sciences. 2022; 12(18):9067. https://0-doi-org.brum.beds.ac.uk/10.3390/app12189067
Chicago/Turabian StyleChecherita, Laura Elisabeta, Magda Ecaterina Antohe, Ovidiu Stamatin, Ioana Rudnic, Iulian Costin Lupu, Irina Croitoru, Amelia Surdu, Daniel Cioloca, Irina Gradinaru, Laurian Francu, and et al. 2022. "Periodontal Disease Diagnosis in the Context of Oral Rehabilitation Approaches" Applied Sciences 12, no. 18: 9067. https://0-doi-org.brum.beds.ac.uk/10.3390/app12189067