
Apparent Diffusion Coefficient Value as a Biomarker for Detecting Muscle-Invasive and High-Grade Bladder Cancer: A Systematic Review


Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Study Selection
2.3. Data Extraction
2.4. Quality Assessment
3. Results
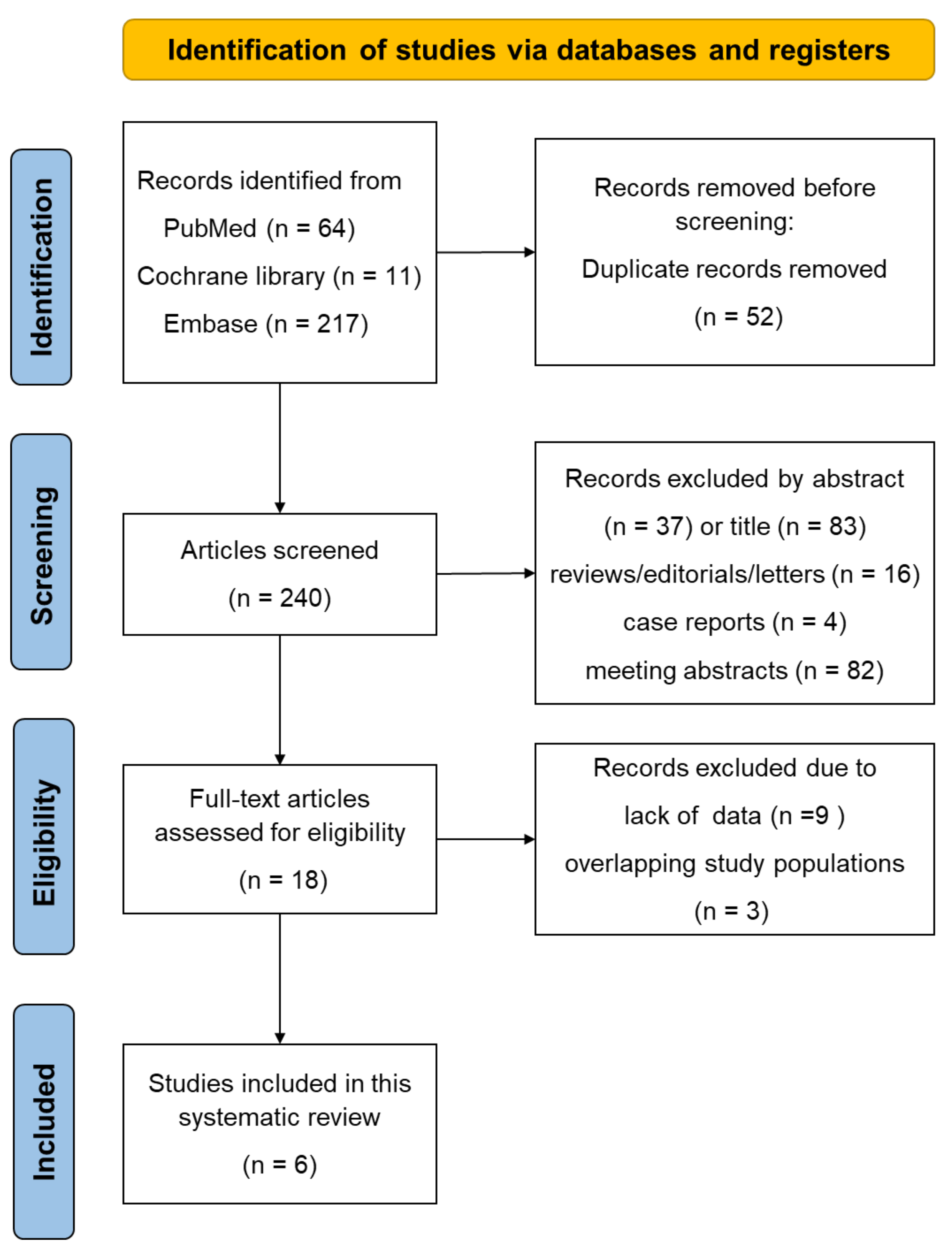
3.1. Literature Search
3.2. Study Characteristics
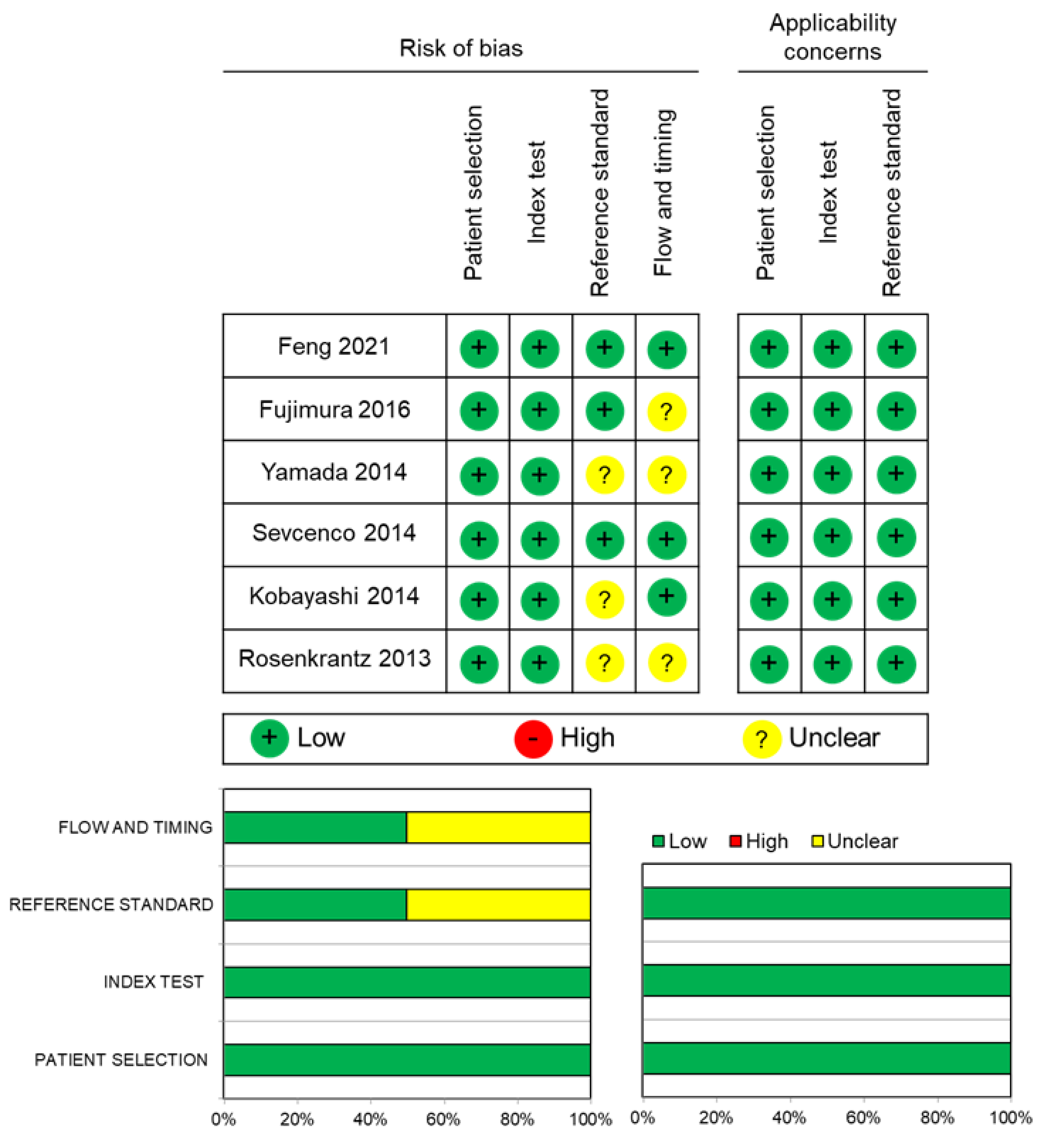
3.3. Quality Assessment
3.4. Data Analysis
3.4.1. Diagnostic Performance of ADC Values to Differentiate MIBC from NMIBC
3.4.2. Diagnostic Performance of ADC Values to Differentiate High-Grade Disease from Low-Grade Disease
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Sylvester, R.J.; van der Meijden, A.P.; Oosterlinck, W.; Witjes, J.A.; Bouffioux, C.; Denis, L.; Newling, D.W.; Kurth, K. Predicting recurrence and progression in individual patients with stage Ta T1 bladder cancer using EORTC risk tables: A combined analysis of 2596 patients from seven EORTC trials. Eur. Urol. 2006, 49, 466–475, discussion 475–477. [Google Scholar] [CrossRef] [PubMed]
- Babjuk, M.; Burger, M.; Capoun, O.; Cohen, D.; Compérat, E.M.; Dominguez Escrig, J.L.; Gontero, P.; Liedberg, F.; Masson-Lecomte, A.; Mostafid, A.H.; et al. European Association of Urology Guidelines on Non-muscle-invasive Bladder Cancer (Ta, T1, and Carcinoma in Situ). Eur. Urol. 2022, 81, 75–94. [Google Scholar] [CrossRef]
- Witjes, J.A.; Bruins, H.M.; Cathomas, R.; Compérat, E.M.; Cowan, N.C.; Gakis, G.; Hernández, V.; Linares Espinós, E.; Lorch, A.; Neuzillet, Y.; et al. European Association of Urology Guidelines on Muscle-invasive and Metastatic Bladder Cancer: Summary of the 2020 Guidelines. Eur. Urol. 2021, 79, 82–104. [Google Scholar] [CrossRef] [PubMed]
- Stein, J.P.; Lieskovsky, G.; Cote, R.; Groshen, S.; Feng, A.C.; Boyd, S.; Skinner, E.; Bochner, B.; Thangathurai, D.; Mikhail, M.; et al. Radical cystectomy in the treatment of invasive bladder cancer: Long-term results in 1054 patients. J. Clin. Oncol. 2001, 19, 666–675. [Google Scholar] [CrossRef] [PubMed]
- Giacalone, N.J.; Shipley, W.U.; Clayman, R.H.; Niemierko, A.; Drumm, M.; Heney, N.M.; Michaelson, M.D.; Lee, R.J.; Saylor, P.J.; Wszolek, M.F.; et al. Long-term Outcomes After Bladder-preserving Tri-modality Therapy for Patients with Muscle-invasive Bladder Cancer: An Updated Analysis of the Massachusetts General Hospital Experience. Eur. Urol. 2017, 71, 952–960. [Google Scholar] [CrossRef] [PubMed]
- Ark, J.T.; Keegan, K.A.; Barocas, D.A.; Morgan, T.M.; Resnick, M.J.; You, C.; Cookson, M.S.; Penson, D.F.; Davis, R.; Clark, P.E.; et al. Incidence and predictors of understaging in patients with clinical T1 urothelial carcinoma undergoing radical cystectomy. BJU Int. 2014, 113, 894–899. [Google Scholar] [CrossRef] [PubMed]
- Woo, S.; Suh, C.H.; Kim, S.Y.; Cho, J.Y.; Kim, S.H. Diagnostic performance of MRI for prediction of muscle-invasiveness of bladder cancer: A systematic review and meta-analysis. Eur. J. Radiol. 2017, 95, 46–55. [Google Scholar] [CrossRef]
- Huang, L.; Kong, Q.; Liu, Z.; Wang, J.; Kang, Z.; Zhu, Y. The Diagnostic Value of MR Imaging in Differentiating T Staging of Bladder Cancer: A Meta-Analysis. Radiology 2018, 286, 502–511. [Google Scholar] [CrossRef] [Green Version]
- Panebianco, V.; Narumi, Y.; Altun, E.; Bochner, B.H.; Efstathiou, J.A.; Hafeez, S.; Huddart, R.; Kennish, S.; Lerner, S.; Montironi, R.; et al. Multiparametric Magnetic Resonance Imaging for Bladder Cancer: Development of VI-RADS (Vesical Imaging-Reporting And Data System). Eur. Urol. 2018, 74, 294–306. [Google Scholar] [CrossRef] [Green Version]
- Woo, S.; Panebianco, V.; Narumi, Y.; Del Giudice, F.; Muglia, V.F.; Takeuchi, M.; Ghafoor, S.; Bochner, B.H.; Goh, A.C.; Hricak, H.; et al. Diagnostic Performance of Vesical Imaging Reporting and Data System for the Prediction of Muscle-invasive Bladder Cancer: A Systematic Review and Meta-analysis. Eur. Urol. Oncol. 2020, 3, 306–315. [Google Scholar] [CrossRef] [Green Version]
- Del Giudice, F.; Pecoraro, M.; Vargas, H.A.; Cipollari, S.; De Berardinis, E.; Bicchetti, M.; Chung, B.I.; Catalano, C.; Narumi, Y.; Catto, J.W.F.; et al. Systematic Review and Meta-Analysis of Vesical Imaging-Reporting and Data System (VI-RADS) Inter-Observer Reliability: An Added Value for Muscle Invasive Bladder Cancer Detection. Cancers 2020, 12, 2994. [Google Scholar] [CrossRef] [PubMed]
- Bammer, R. Basic principles of diffusion-weighted imaging. Eur. J. Radiol. 2003, 45, 169–184. [Google Scholar] [CrossRef]
- Kobayashi, S.; Koga, F.; Yoshida, S.; Masuda, H.; Ishii, C.; Tanaka, H.; Komai, Y.; Yokoyama, M.; Saito, K.; Fujii, Y.; et al. Diagnostic performance of diffusion-weighted magnetic resonance imaging in bladder cancer: Potential utility of apparent diffusion coefficient values as a biomarker to predict clinical aggressiveness. Eur. Radiol. 2011, 21, 2178–2186. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, S.; Koga, F.; Kajino, K.; Yoshita, S.; Ishii, C.; Tanaka, H.; Saito, K.; Masuda, H.; Fujii, Y.; Yamada, T.; et al. Apparent diffusion coefficient value reflects invasive and proliferative potential of bladder cancer. J. Magn. Reson. Imaging 2014, 39, 172–178. [Google Scholar] [CrossRef]
- Rosenkrantz, A.B.; Mussi, T.C.; Spieler, B.; Melamed, J.; Taneja, S.S.; Huang, W.C. High-grade bladder cancer: Association of the apparent diffusion coefficient with metastatic disease: Preliminary results. J. Magn. Reson. Imaging 2012, 35, 1478–1483. [Google Scholar] [CrossRef]
- Rosenkrantz, A.B.; Haghighi, M.; Horn, J.; Naik, M.; Hardie, A.D.; Somberg, M.B.; Melamed, J.; Xiao, G.Q.; Huang, W.C.; Taouli, B. Utility of quantitative MRI metrics for assessment of stage and grade of urothelial carcinoma of the bladder: Preliminary results. Am. J. Roentgenol. 2013, 201, 1254–1259. [Google Scholar] [CrossRef]
- Sevcenco, S.; Ponhold, L.; Heinz-Peer, G.; Fajkovic, H.; Haitel, A.; Susani, M.; Shariat, S.F.; Szarvas, T.; Baltzer, P.A. Prospective evaluation of diffusion-weighted MRI of the bladder as a biomarker for prediction of bladder cancer aggressiveness. Urol. Oncol. 2014, 32, 1166–1171. [Google Scholar] [CrossRef]
- Yamada, Y.; Kobayashi, S.; Isoshima, S.; Arima, K.; Sakuma, H.; Sugimura, Y. The usefulness of diffusion-weighted magnetic resonance imaging in bladder cancer staging and functional analysis. J. Cancer Res. Ther. 2014, 10, 878–882. [Google Scholar] [CrossRef]
- Wang, H.J.; Pui, M.H.; Guo, Y.; Li, S.R.; Guan, J.; Zhang, X.L.; Cai, H.S. Multiparametric 3-T MRI for differentiating low-versus high-grade and category T1 versus T2 bladder urothelial carcinoma. Am. J. Roentgenol. 2015, 204, 330–334. [Google Scholar] [CrossRef]
- Fujimura, M.; Sakamoto, S.; Sekita, N.; Takeuchi, N.; Nishikawa, R.; Suzuki, H.; Mikami, K.; Ichikawa, T. Apparent diffusion coefficient value for estimating clinicohistological factors in bladder cancer including infiltration style and lymphatic invasion. Springerplus 2016, 5, 848. [Google Scholar] [CrossRef] [Green Version]
- Al Johi, R.S.; Seifeldein, G.S.; Moeen, A.M.; Aboulhagag, N.A.; Moussa, E.M.; Hameed, D.A.; Imam, H.M. Diffusion weighted magnetic resonance imaging in bladder cancer, is it time to replace biopsy? Cent. Eur. J. Urol. 2018, 71, 31–37. [Google Scholar]
- Wang, Y.; Hu, D.; Yu, H.; Shen, Y.; Tang, H.; Kamel, I.R.; Li, Z. Comparison of the Diagnostic Value of Monoexponential, Biexponential, and Stretched Exponential Diffusion-weighted MRI in Differentiating Tumor Stage and Histological Grade of Bladder Cancer. Acad. Radiol. 2019, 26, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Liu, L.; Ding, L.; Zhang, Z.; Zhang, M. Quantitative Assessment of Bladder Cancer Reflects Grade and Recurrence: Comparing of Three Methods of Positioning Region of Interest for ADC Measurements at Diffusion-weighted MR Imaging. Acad. Radiol. 2019, 26, 1148–1153. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Shen, Y.; Hu, X.; Li, Z.; Feng, C.; Hu, D.; Kamel, I.R. Application of R2* and Apparent Diffusion Coefficient in Estimating Tumor Grade and T Category of Bladder Cancer. Am. J. Roentgenol. 2020, 214, 383–389. [Google Scholar] [CrossRef]
- Yuan, L.; Li, D.; Mu, D.; Zhang, X.; Kong, W.; Cheng, L.; Shu, X.; Zhang, B.; Wang, Z. Combined T2 SPAIR, Dynamic Enhancement and DW Imaging Reliably Detect T Staging and Grading of Bladder Cancer With 3.0T MRI. Front. Oncol. 2020, 10, 582532. [Google Scholar] [CrossRef]
- Feng, C.; Wang, Y.; Dan, G.; Zhong, Z.; Karaman, M.M.; Li, Z.; Hu, D.; Zhou, X.J. Evaluation of a fractional-order calculus diffusion model and bi-parametric VI-RADS for staging and grading bladder urothelial carcinoma. Eur. Radiol. 2021. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Knoll, T.; Omar, M.I.; Maclennan, S.; Hernández, V.; Canfield, S.; Yuan, Y.; Bruins, M.; Marconi, L.; Van Poppel, H.; N’Dow, J.; et al. Key Steps in Conducting Systematic Reviews for Underpinning Clinical Practice Guidelines: Methodology of the European Association of Urology. Eur. Urol. 2018, 73, 290–300. [Google Scholar] [CrossRef]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Padhani, A.R.; Liu, G.; Koh, D.M.; Chenevert, T.L.; Thoeny, H.C.; Takahara, T.; Dzik-Jurasz, A.; Ross, B.D.; Van Cauteren, M.; Collins, D.; et al. Diffusion-weighted magnetic resonance imaging as a cancer biomarker: Consensus and recommendations. Neoplasia 2009, 11, 102–125. [Google Scholar] [CrossRef] [Green Version]
- Klaassen, Z.; Kamat, A.M.; Kassouf, W.; Gontero, P.; Villavicencio, H.; Bellmunt, J.; van Rhijn, B.W.G.; Hartmann, A.; Catto, J.W.F.; Kulkarni, G.S. Treatment Strategy for Newly Diagnosed T1 High-grade Bladder Urothelial Carcinoma: New Insights and Updated Recommendations. Eur. Urol. 2018, 74, 597–608. [Google Scholar] [CrossRef] [PubMed]
- Jeh, S.K.; Kim, S.H.; Kim, H.S.; Kang, B.J.; Jeong, S.H.; Yim, H.W.; Song, B.J. Correlation of the apparent diffusion coefficient value and dynamic magnetic resonance imaging findings with prognostic factors in invasive ductal carcinoma. J. Magn. Reson. Imaging 2011, 33, 102–109. [Google Scholar] [CrossRef]
- Giganti, F.; Orsenigo, E.; Esposito, A.; Chiari, D.; Salerno, A.; Ambrosi, A.; Albarello, L.; Mazza, E.; Staudacher, C.; Del Maschio, A.; et al. Prognostic Role of Diffusion-weighted MR Imaging for Resectable Gastric Cancer. Radiology 2015, 276, 444–452. [Google Scholar] [CrossRef] [PubMed]
- Rosenkrantz, A.B.; Obele, C.; Rusinek, H.; Balar, A.V.; Huang, W.C.; Deng, F.M.; Ream, J.M. Whole-lesion diffusion metrics for assessment of bladder cancer aggressiveness. Abdom. Imaging 2015, 40, 327–332. [Google Scholar] [CrossRef]
- Sevcenco, S.; Maj-Hes, A.B.; Hruby, S.; Ponhold, L.; Heinz-Peer, G.; Rauchenwald, M.; Marszalek, M.; Klingler, H.C.; Polanec, S.; Baltzer, P.A.T. Apparent diffusion coefficient values obtained by unenhanced MRI predicts disease-specific survival in bladder cancer. Clin. Radiol. 2018, 73, 881–885. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, S.; Koga, F.; Kobayashi, S.; Ishii, C.; Tanaka, H.; Tanaka, H.; Komai, Y.; Saito, K.; Masuda, H.; Fujii, Y.; et al. Role of diffusion-weighted magnetic resonance imaging in predicting sensitivity to chemoradiotherapy in muscle-invasive bladder cancer. Int. J. Radiat. Oncol. Biol. Phys. 2012, 83, e21–e27. [Google Scholar] [CrossRef]
- Le Bihan, D.; Breton, E.; Lallemand, D.; Grenier, P.; Cabanis, E.; Laval-Jeantet, M. MR imaging of intravoxel incoherent motions: Application to diffusion and perfusion in neurologic disorders. Radiology 1986, 161, 401–407. [Google Scholar] [CrossRef] [Green Version]
- Magin, R.L.; Abdullah, O.; Baleanu, D.; Zhou, X.J. Anomalous diffusion expressed through fractional order differential operators in the Bloch-Torrey equation. J. Magn. Reson. 2008, 190, 255–270. [Google Scholar] [CrossRef]
- Dixon, W.T. Separation of diffusion and perfusion in intravoxel incoherent motion MR imaging: A modest proposal with tremendous potential. Radiology 1988, 168, 566–567. [Google Scholar] [CrossRef]
- Zhang, M.; Chen, Y.; Cong, X.; Zhao, X. Utility of intravoxel incoherent motion MRI derived parameters for prediction of aggressiveness in urothelial bladder carcinoma. J. Magn. Reson. Imaging 2018, 48, 1648–1656. [Google Scholar] [CrossRef]
- Carando, R.; Afferi, L.; Marra, G.; Krajewski, W.; Pagliarulo, V.; Abufaraj, M.; Xylinas, E.; Cathelineau, X.; Sanchez-Salas, R.; Moschini, M. The effectiveness of multiparametric magnetic resonance imaging in bladder cancer (Vesical Imaging-Reporting and Data System): A systematic review. Arab. J. Urol. 2020, 18, 67–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, J.; Yin, J.; Cui, L.; Gu, X.; Cai, R.; Gong, S.; Xu, Y.; Ma, H.; Mao, J. Lung Cancer: Short-Term Reproducibility of Intravoxel Incoherent Motion Parameters and Apparent Diffusion Coefficient at 3T. J. Magn. Reson. Imaging 2018, 47, 1003–1012. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Zhao, M.; Liu, J.; Yang, H.; Zhou, X.; Wen, C.; Li, G.; Duan, Y. Mean apparent diffusion coefficient in a single slice may predict tumor response to whole-brain radiation therapy in non-small-cell lung cancer patients with brain metastases. Eur. Radiol. 2021, 31, 5565–5575. [Google Scholar] [CrossRef] [PubMed]
- Priola, A.M.; Priola, S.M.; Parlatano, D.; Gned, D.; Giraudo, M.T.; Giardino, R.; Ferrero, B.; Ardissone, F.; Veltri, A. Apparent diffusion coefficient measurements in diffusion-weighted magnetic resonance imaging of the anterior mediastinum: Inter-observer reproducibility of five different methods of region-of-interest positioning. Eur. Radiol. 2017, 27, 1386–1394. [Google Scholar] [CrossRef]
- Sakamoto, K.; Ito, M.; Ikuta, S.; Nakanishi, Y.; Kataoka, M.; Takemura, K.; Suzuki, H.; Tobisu, K.-I.; Kamai, T.; Koga, F. Detection of Muscle-Invasive Bladder Cancer on Biparametric MRI Using Vesical Imaging-Reporting and Data System and Apparent Diffusion Coefficient Values (VI-RADS/ADC). Bladder Cancer 2020, 6, 161–169. [Google Scholar] [CrossRef]
- Sasaki, M.; Yamada, K.; Watanabe, Y.; Matsui, M.; Ida, M.; Fujiwara, S.; Shibata, E. Variability in absolute apparent diffusion coefficient values across different platforms may be substantial: A multivendor, multi-institutional comparison study. Radiology 2008, 249, 624–630. [Google Scholar] [CrossRef]
- Donati, O.F.; Chong, D.; Nanz, D.; Boss, A.; Froehlich, J.M.; Andres, E.; Seifert, B.; Thoeny, H.C. Diffusion-weighted MR imaging of upper abdominal organs: Field strength and intervendor variability of apparent diffusion coefficients. Radiology 2014, 270, 454–463. [Google Scholar] [CrossRef]
- Nishizawa, T.; Yoshida, S.; Koga, F.; Tanaka, H.; Kaga, M.; Watanabe, K.; Fukushima, H.; Nakanishi, Y.; Yokoyama, M.; Ishioka, J.; et al. Standardization of the apparent diffusion coefficient value of bladder cancer across different centers: Applicability in predicting aggressive pathologic phenotypes. Clin. Imaging 2017, 44, 121–126. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author [Reference No.] | Year | Country | Study Period | Study Design | Age, Mean (Range) | No. Patients (%, Female) | No. BT | Magnet Strength | b Value (Number) | Pathological Findings (No. Patients) | Surgical Modalities to Obtain Specimens | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Grade | pT Category | |||||||||||
| Feng [26] | 2021 | China | 2014–2019 | Prospective | 60 (37–79) | 58 (12) | 58 | 3.0 T | 0–3600 (16) | Low (21) High (37) | NMIBC (33) MIBC (25) | TUR (30) PC (4) RC (24) |
| Fujimura [20] | 2016 | Japan | 2009–2013 | Retrospective | 73 (42–95) | 114 (24) | NA | 1.5 T | 0, 1000 (2) | G1 (9) G2 (48) G3 (57) | NMIBC (83) MIBC (31) | TUR (114) |
| Yamada [18] | 2014 | Japan | 2006–2013 | Retrospective | 72 (38–90) | 160 (38) | 99 | 1.5 T | 0, 1000 (2) | Low (31) High (129) | NMIBC (125) MIBC (35) | TUR (129) RC (31) |
| Sevcenco [17] | 2014 | Austria | 2012–2013 | Prospective | NA | 49 (20) | 43 | 3.0 T | 50–1000 (3) | Low (24) High (19) | NMIBC (33) MIBC (10) | TUR (51) |
| Kobayashi [14] | 2014 | Japan | 2007–2011 | Prospective | 68 (38–88) | 132 (23) | 132 | 1.5 T | 0–2000 (4) | G1 (2) G2 (67) G3 (63) | NMIBC (81) MIBC (51) | TUR (132) |
| Rosenkrantz [16] | 2013 | USA | NA | Retrospective | NA | 37 (NA) | 37 | 1.5 T | 0–800 (3) | NA | NMIBC (21) MIBC (16) | TUR (29) RC (8) |
| Author [Reference No.] | NMIBC (Mean ± SD) | MIBC (Mean ± SD) | p Value | Cutoff | Sensitivity (%) | Specificity (%) | AUC | |
|---|---|---|---|---|---|---|---|---|
| Feng [26] | 1.30 ± 0.31 | 1.06 ± 0.24 | 0.003 | NA | 72.0 | 66.7 | 0.730 | |
| Rosenkrantz [16] | 1.04 ± 0.25 | 0.85 ± 0.24 | 0.006 | 0.87 | 75.0 | 81.0 | 0.765 | |
| Fujimura [20] | 1.08 (0.16–2.18) | 0.72 (0.35–1.82) | <0.001 | 0.89 | 68.8 | 84.4 | 0.758 | |
| Sevcenco [17] | 1.12 (1.02–1.22) * | 0.76 (0.65–0.87) * | <0.001 | 0.92 | 90.0 | 78.8 | 0.884 | |
| Yamada [18] | 1.31 ± 0.27 | 1.00 ± 0.21 | <0.001 | NA | NA | NA | NA | |
| Ta | T1 | ≥T2 | ||||||
| Kobayashi [14] | 1.00 (0.92–1.14) † | 0.83 (0.75–0.92) † | 0.74 (0.62–0.85) | <0.001 | NA | NA | NA | NA |
| Author [Reference No.] | Grade (Mean ± SD) | p Value | Cutoff | Sensitivity (%) | Specificity (%) | AUC | ||
|---|---|---|---|---|---|---|---|---|
| Low-grade | High-grade | |||||||
| Feng [26] | 1.40 ± 0.26 | 1.08 ± 0.27 | <0.001 | NA | 73.0 | 76.2 | 0.804 | |
| Rosenkrantz [16] | 1.35 ± 0.28 | 0.92 ± 0.24 | 0.023 | 1.03 | 76.5 | 100.0 | 0.902 | |
| Yamada [18] | 1.58 ± 0.21 | 1.20 ± 0.27 | <0.001 | NA | NA | NA | NA | |
| Sevcenco [17] | 1.23 (1.15–1.32) * | 0.79 (0.69–0.88) * | <0.001 | 0.92 | 75.0 | 95.8 | 0.906 | |
| Grade 1 | Grade 2 | Grade 3 | ||||||
| Fujimura [20] | 1.41 (0.68–2.00) † | 1.15 (0.16–2.10) † | 0.74 (0.17–2.18) † | <0.001 | NA | NA | NA | NA |
| Kobayashi [14] | 1.00 (0.92–1.14) † | 0.83 (0.75–0.92) † | 0.74 (0.62–0.85) † | <0.001 | NA | NA | NA | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kobayashi, S.; Takemura, K.; Koga, F. Apparent Diffusion Coefficient Value as a Biomarker for Detecting Muscle-Invasive and High-Grade Bladder Cancer: A Systematic Review. Appl. Sci. 2022, 12, 1278. https://0-doi-org.brum.beds.ac.uk/10.3390/app12031278
Kobayashi S, Takemura K, Koga F. Apparent Diffusion Coefficient Value as a Biomarker for Detecting Muscle-Invasive and High-Grade Bladder Cancer: A Systematic Review. Applied Sciences. 2022; 12(3):1278. https://0-doi-org.brum.beds.ac.uk/10.3390/app12031278
Chicago/Turabian StyleKobayashi, Shuichiro, Kosuke Takemura, and Fumitaka Koga. 2022. "Apparent Diffusion Coefficient Value as a Biomarker for Detecting Muscle-Invasive and High-Grade Bladder Cancer: A Systematic Review" Applied Sciences 12, no. 3: 1278. https://0-doi-org.brum.beds.ac.uk/10.3390/app12031278