
Effectiveness of Rehabilitation through Kinematic Analysis of Upper Limb Functioning in Wheelchair Basketball Athletes: A Pilot Study

 ,
,  , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
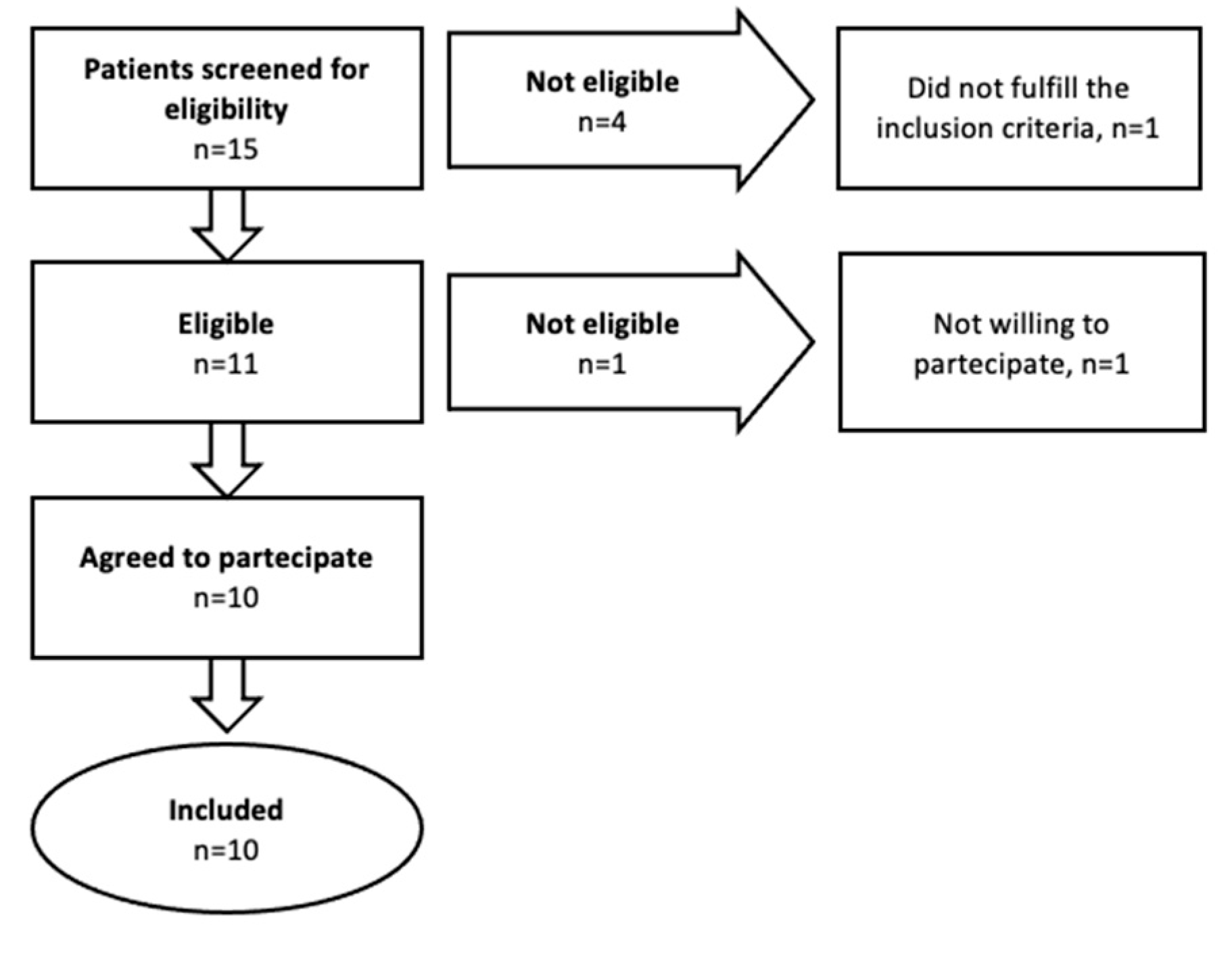
2.1. Participants
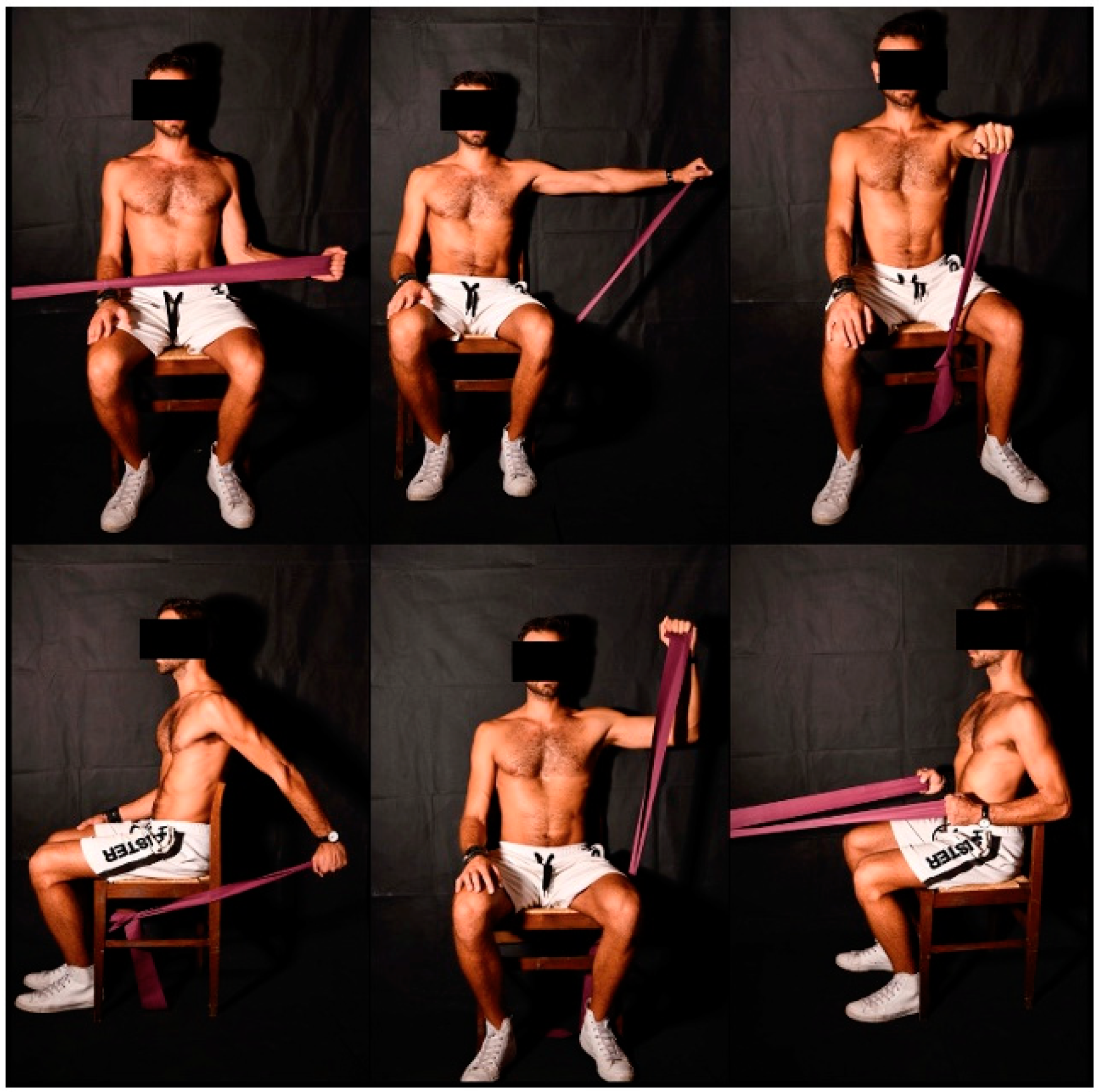
2.2. Intervention
2.3. Functional Outcome Measures
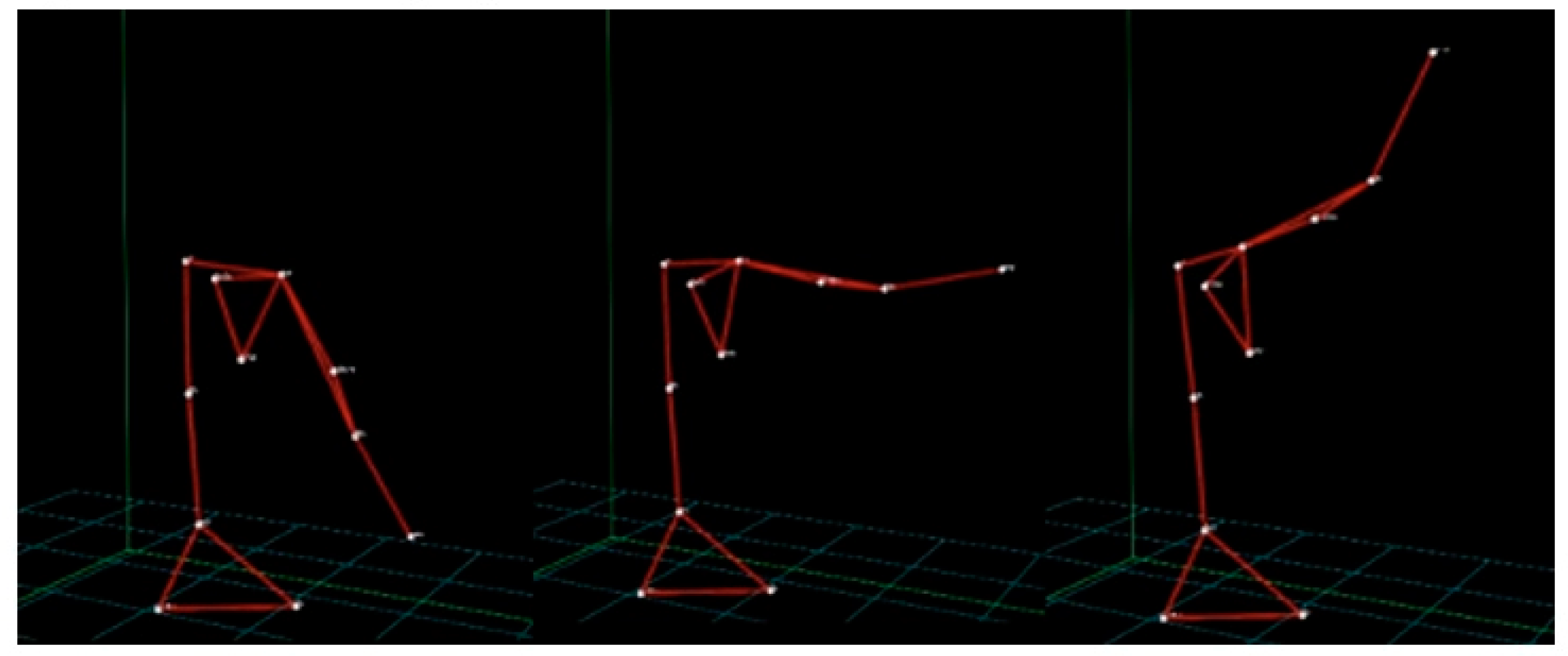
2.4. Kinematic Analysis
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tuakli-Wosornu, Y.A.; Mashkovskiy, E.; Ottesen, T.; Gentry, M.; Jensen, D.; Webborn, N. Acute and Chronic Musculoskeletal Injury in Para Sport: A Critical Review. Phys. Med. Rehabil. Clin. N. Am. 2018, 29, 205–243. [Google Scholar] [CrossRef] [PubMed]
- Fagher, K.; Lexell, J. Sports-Related Injuries in Athletes with Disabilities. Scand. J. Med. Sci. Sports 2014, 24, e320–e331. [Google Scholar] [CrossRef] [PubMed]
- Fagher, K.; Dahlström, Ö.; Jacobsson, J.; Timpka, T.; Lexell, J. Prevalence of Sports-Related Injuries and Illnesses in Paralympic Athletes. PM R 2020, 12, 271–280. [Google Scholar] [CrossRef] [PubMed]
- Heyward, O.W.; Vegter, R.J.K.; de Groot, S.; van der Woude, L.H.V. Shoulder Complaints in Wheelchair Athletes: A Systematic Review. PLoS ONE 2017, 12, e0188410. [Google Scholar] [CrossRef] [Green Version]
- Murgia, M.; Bernetti, A.; Delicata, M.; Massetti, C.; Achilli, E.M.; Mangone, M.; Ioppolo, F.; Di Sante, L.; Santilli, V.; Galeoto, G.; et al. Inter- and Intra-Interviewer Reliability of Italian Version of Pediatric Evaluation of Disability Inventory (I-PEDI). Ann. Ig 2018, 30, 153–161. [Google Scholar] [CrossRef] [PubMed]
- Paralyzed Veterans of America Consortium for Spinal Cord Medicine Preservation of Upper Limb Function Following Spinal Cord Injury: A Clinical Practice Guideline for Health-Care Professionals. J. Spinal Cord Med. 2005, 28, 434–470. [CrossRef] [PubMed] [Green Version]
- Mason, B.S.; van der Woude, L.H.V.; Goosey-Tolfrey, V.L. The Ergonomics of Wheelchair Configuration for Optimal Performance in the Wheelchair Court Sports. Sports Med. 2013, 43, 23–38. [Google Scholar] [CrossRef] [Green Version]
- Requejo, P.; Mulroy, S.; Haubert, L.; Newsam, C.; Gronley, J.; Perry, J. Evidence-Based Strategies to Preserve Shoulder Function in Manual Wheelchair Users with Spinal Cord Injury. Top. Spinal Cord Inj. Rehabil. 2008, 13, 86–119. [Google Scholar] [CrossRef]
- Ferrara, P.E.; Ferriero, G.; Palmieri, V.; Codazza, S.; Gatto, D.M.; Zordan, P.; Stefinlongo, G.; de Sire, A.; Ronconi, G. Effects of a training protocol for the prevention of shoulder overuse syndrome in wheelchair rugby athletes: A pilot study. J. Biol. Regul. Homeost. Agents 2021, 35, 1783–1787. [Google Scholar] [CrossRef]
- Invernizzi, M.; de Sire, A.; Fusco, N. Rethinking the Clinical Management of Volumetric Muscle Loss in Patients with Spinal Cord Injury: Synergy among Nutritional Supplementation, Pharmacotherapy, and Rehabilitation. Curr. Opin. Pharmacol. 2021, 57, 132–139. [Google Scholar] [CrossRef]
- Wilroy, J.; Hibberd, E. Evaluation of a Shoulder Injury Prevention Program in Wheelchair Basketball. J. Sport Rehabil. 2018, 27, 554–559. [Google Scholar] [CrossRef]
- Riccio, I.; de Sire, A.; Latte, C.; Pascarella, F.; Gimigliano, F. Conservative treatment of traumatic shoulder instability: A case series study. Musculoskelet Surg. 2015, 99, 133–137. [Google Scholar] [CrossRef]
- Lefèvre-Colau, M.-M.; Nguyen, C.; Palazzo, C.; Srour, F.; Paris, G.; Vuillemin, V.; Poiraudeau, S.; Roby-Brami, A.; Roren, A. Kinematic Patterns in Normal and Degenerative Shoulders. Part II: Review of 3-D Scapular Kinematic Patterns in Patients with Shoulder Pain, and Clinical Implications. Ann. Phys. Rehabil. Med. 2018, 61, 46–53. [Google Scholar] [CrossRef] [PubMed]
- de Sire, A.; Marotta, N.; Lippi, L.; Scaturro, D.; Farì, G.; Liccardi, A.; Moggio, L.; Letizia Mauro, G.; Ammendolia, A.; Invernizzi, M. Pharmacological Treatment for Acute Traumatic Musculoskeletal Pain in Athletes. Medicina 2021, 57, 1208. [Google Scholar] [CrossRef] [PubMed]
- Warner, M.B.; Wilson, D.; Heller, M.O.; Wood, D.; Worsley, P.; Mottram, S.; Webborn, N.; Veeger, D.; Batt, M. Scapular Kinematics in Professional Wheelchair Tennis Players. Clin. Biomech. 2018, 53, 7–13. [Google Scholar] [CrossRef] [PubMed]
- de Sire, A.; Mauro, A.; Priano, L.; Baudo, S.; Bigoni, M.; Solaro, C. Effects of Constraint-Induced Movement Therapy on Upper Limb Activity According to a Bi-Dimensional Kinematic Analysis in Progressive Multiple Sclerosis Patients: A Randomized Single-Blind Pilot Study. Funct. Neurol. 2019, 34, 151–157. [Google Scholar]
- Vigotsky, A.D.; Halperin, I.; Lehman, G.J.; Trajano, G.S.; Vieira, T.M. Interpreting Signal Amplitudes in Surface Electromyography Studies in Sport and Rehabilitation Sciences. Front. Physiol. 2017, 8, 985. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kraeutler, M.J.; Ciccotti, M.G.; Dodson, C.C.; Frederick, R.W.; Cammarota, B.; Cohen, S.B. Kerlan-Jobe Orthopaedic Clinic Overhead Athlete Scores in Asymptomatic Professional Baseball Pitchers. J. Shoulder Elb. Surg. 2013, 22, 329–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warner, M.B.; Chappell, P.H.; Stokes, M.J. Measuring Scapular Kinematics during Arm Lowering Using the Acromion Marker Cluster. Hum. Mov. Sci. 2012, 31, 386–396. [Google Scholar] [CrossRef]
- Wu, G.; Cavanagh, P.R. ISB Recommendations for Standardization in the Reporting of Kinematic Data. J. Biomech. 1995, 28, 1257–1261. [Google Scholar] [CrossRef]
- Bakshi, N.; Freehill, M.T. The Overhead Athletes Shoulder. Sports Med. Arthrosc. Rev. 2018, 26, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Weber, A.E.; Kontaxis, A.; O’Brien, S.J.; Bedi, A. The Biomechanics of Throwing: Simplified and Cogent. Sports Med. Arthrosc. Rev. 2014, 22, 72–79. [Google Scholar] [CrossRef] [PubMed]
- de Araújo, R.C.; Pirauá, A.L.T.; Beltrão, N.B.; Pitangui, A.C.R. Activity of Periscapular Muscles and Its Correlation with External Oblique during Push-up: Does Scapular Dyskinesis Change the Electromyographic Response? J. Sports Sci. 2018, 36, 571–577. [Google Scholar] [CrossRef] [PubMed]
- Hermens, H.J.; Freriks, B.; Disselhorst-Klug, C.; Rau, G. Development of Recommendations for SEMG Sensors and Sensor Placement Procedures. J. Electromyogr. Kinesiol. 2000, 10, 361–374. [Google Scholar] [CrossRef]
- Lewis, A.R.; Phillips, E.J.; Robertson, W.S.P.; Grimshaw, P.N.; Portus, M.; Winter, J. A Practical Assessment of Wheelchair Racing Performance Kinetics Using Accelerometers. Sports Biomech. 2019, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Rupf, R.; Tsai, M.C.; Thomas, S.G.; Klimstra, M. Original Article: Validity of Measuring Wheelchair Kinematics Using One Inertial Measurement Unit during Commonly Used Testing Protocols in Elite Wheelchair Court Sports. J. Biomech. 2021, 127, 110654. [Google Scholar] [CrossRef] [PubMed]
- Bergamini, E.; Morelli, F.; Marchetti, F.; Vannozzi, G.; Polidori, L.; Paradisi, F.; Traballesi, M.; Cappozzo, A.; Delussu, A.S. Wheelchair Propulsion Biomechanics in Junior Basketball Players: A Method for the Evaluation of the Efficacy of a Specific Training Program. BioMed Res. Int. 2015, 2015, 27596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Curtis, K.A.; Roach, K.E.; Applegate, E.B.; Amar, T.; Benbow, C.S.; Genecco, T.D.; Gualano, J. Development of the Wheelchair User’s Shoulder Pain Index (WUSPI). Paraplegia 1995, 33, 290–293. [Google Scholar] [CrossRef] [PubMed]
- Hicks, A.L.; Martin Ginis, K.A.; Pelletier, C.A.; Ditor, D.S.; Foulon, B.; Wolfe, D.L. The Effects of Exercise Training on Physical Capacity, Strength, Body Composition and Functional Performance among Adults with Spinal Cord Injury: A Systematic Review. Spinal Cord 2011, 49, 1103–1127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sciascia, A.; Haegele, L.E.; Lucas, J.; Uhl, T.L. Preseason Perceived Physical Capability and Previous Injury. J. Athl. Train. 2015, 50, 937–943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, R.M.; Gelber, J.D.; Schickendantz, M.S. The Weight-Bearing Shoulder. J. Am. Acad. Orthop. Surg. 2018, 26, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Kaźmierczak, K.; Lisiński, P. Leisure Time Physical Activity of People with Chronic Spinal Cord Injuries. Clin. Neurol. Neurosurg. 2018, 170, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Ludewig, P.M.; Reynolds, J.F. The Association of Scapular Kinematics and Glenohumeral Joint Pathologies. J. Orthop. Sports Phys. Ther. 2009, 39, 90–104. [Google Scholar] [CrossRef] [Green Version]
- de Witte, P.B.; Nagels, J.; van Arkel, E.R.; Visser, C.P.; Nelissen, R.G.; de Groot, J.H. Study Protocol Subacromial Impingement Syndrome: The Identification of Pathophysiologic Mechanisms (SISTIM). BMC Musculoskelet. Disord. 2011, 12, 282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooper, R.A.; Tuakli-Wosornu, Y.A.; Henderson, G.V.; Quinby, E.; Dicianno, B.E.; Tsang, K.; Ding, D.; Cooper, R.; Crytzer, T.M.; Koontz, A.M.; et al. Engineering and Technology in Wheelchair Sport. Phys. Med. Rehabil. Clin. N. Am. 2018, 29, 347–369. [Google Scholar] [CrossRef]
- Invernizzi, M.; de Sire, A.; Carda, S.; Venetis, K.; Renò, F.; Cisari, C.; Fusco, N. Bone Muscle Crosstalk in Spinal Cord Injuries: Pathophysiology and Implications for Patients’ Quality of Life. Curr. Osteoporos. Rep. 2020, 18, 422–431. [Google Scholar] [CrossRef] [PubMed]
- Kwarciak, A.M.; Sisto, S.A.; Yarossi, M.; Price, R.; Komaroff, E.; Boninger, M.L. Redefining the Manual Wheelchair Stroke Cycle: Identification and Impact of Nonpropulsive Pushrim Contact. Arch. Phys. Med. Rehabil. 2009, 90, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Han, D.-S.; Wu, W.-T.; Hsu, P.-C.; Chang, H.-C.; Huang, K.-C.; Chang, K.-V. Sarcopenia Is Associated With Increased Risks of Rotator Cuff Tendon Diseases Among Community-Dwelling Elders: A Cross-Sectional Quantitative Ultrasound Study. Front. Med. 2021, 8, 630009. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| T0 | T1 | p-Values | ||
|---|---|---|---|---|
| Scapulothoracic joint | ||||
| Abduction | Dominant | 33.30 ± 7.57 | 36.00 ± 7.77 | 0.018 * |
| Non-dominant | 39.20 ± 4.78 | 42.01 ± 8.56 | 0.031 * | |
| Extension | Dominant | 30.20 ± 11.14 | 33.30 ± 9.32 | 0.023 * |
| Non-dominant | 29.20 ± 14.49 | 32.40 ± 18.16 | 0.015 * | |
| Glenohumeral joint | ||||
| Abduction | Dominant | 123.60 ± 33.35 | 147.50 ± 16.20 | 0.007 * |
| Non-dominant | 110.20 ± 32.14 | 132.00 ± 23.12 | 0.019 * | |
| Extension | Dominant | 72.70 ± 11.08 | 80.60 ± 9.99 | 0.093 |
| Non-dominant | 75.10 ± 9.45 | 78.50 ± 3.03 | 0.402 | |
| Flexion | Dominant | 133.00 ± 20.58 | 131.30 ± 22.24 | 0.901 |
| Non-dominant | 147.00 ± 22.14 | 156.00 ± 5.16 | 0.335 | |
| External rotation | Dominant | 70.40 ± 11.39 | 80.20 ± 12.04 | 0.007 * |
| Non-dominant | 54.40 ± 14.21 | 77.10 ± 20.72 | 0.021 * | |
| Internal rotation | Dominant | 78.30 ± 14.91 | 82.20 ± 13.10 | 0.564 |
| Non-dominant | 77.30 ± 14.23 | 86.70 ± 14.85 | 0.191 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Demeco, A.; de Sire, A.; Marotta, N.; Palumbo, A.; Fragomeni, G.; Gramigna, V.; Pellegrino, R.; Moggio, L.; Petraroli, A.; Iona, T.; et al. Effectiveness of Rehabilitation through Kinematic Analysis of Upper Limb Functioning in Wheelchair Basketball Athletes: A Pilot Study. Appl. Sci. 2022, 12, 2929. https://0-doi-org.brum.beds.ac.uk/10.3390/app12062929
Demeco A, de Sire A, Marotta N, Palumbo A, Fragomeni G, Gramigna V, Pellegrino R, Moggio L, Petraroli A, Iona T, et al. Effectiveness of Rehabilitation through Kinematic Analysis of Upper Limb Functioning in Wheelchair Basketball Athletes: A Pilot Study. Applied Sciences. 2022; 12(6):2929. https://0-doi-org.brum.beds.ac.uk/10.3390/app12062929
Chicago/Turabian StyleDemeco, Andrea, Alessandro de Sire, Nicola Marotta, Arrigo Palumbo, Gionata Fragomeni, Vera Gramigna, Raffaello Pellegrino, Lucrezia Moggio, Annalisa Petraroli, Teresa Iona, and et al. 2022. "Effectiveness of Rehabilitation through Kinematic Analysis of Upper Limb Functioning in Wheelchair Basketball Athletes: A Pilot Study" Applied Sciences 12, no. 6: 2929. https://0-doi-org.brum.beds.ac.uk/10.3390/app12062929