
Acute and Chronic Effects of Static Stretching on Neuromuscular Properties: A Meta-Analytical Review



Department of Biomedical Engineering, Newark College of Engineering, New Jersey Institute of Technology, Newark, NJ 07102, USA
*
Author to whom correspondence should be addressed.
†
These authors contributed equally to this work.
Appl. Sci. 2023, 13(21), 11979; https://0-doi-org.brum.beds.ac.uk/10.3390/app132111979
Submission received: 6 September 2023
/
Revised: 24 October 2023
/
Accepted: 30 October 2023
/
Published: 2 November 2023
(This article belongs to the Special Issue Sports and Exercise Rehabilitation)
Abstract
:The aim of this review was to provide an overview of the recent findings on the acute and chronic effects of static stretching on joint behaviors and neuromuscular responses and to discuss the overall effects of acute and chronic static stretching on selected outcomes via meta-analyses, using a total of 50 recent studies. The results of our meta-analyses demonstrated that acute static stretching results in increased range of motion (ROM), decreased passive resistive torque (PRT), increased maximum tolerable PRT (PRTmax), decreased maximum voluntary isometric torque, decreased muscle–tendon unit stiffness, decreased muscle stiffness, decreased tendon stiffness, and decreased shear elastic modulus. Moreover, the chronic effects of static stretching included increased ROM, increased PRTmax, decreased muscle stiffness, and decreased shear elastic modulus (or shear wave speed). These results suggest that static stretching interventions have the potential to increase ROM and reduce the mechanical properties of muscle–tendon tissue, but they may not change corticospinal excitability and spinal reflex excitability or muscle architecture parameters.
1. Introduction
Static stretching is commonly used in athletic environments with the specific aims of increasing joint range of motion (ROM) and reducing injury risk [1]. Briefly, static stretching involves keeping a target muscle for a prescribed period of time in a lengthened position at where a stretch sensation or the point of discomfort is reached [2]. Considering that static stretching is relatively easy to implement even for professionally untrained people, static stretching may have potential in many clinical applications, especially for individuals with increased muscle tightness or severe weakness, preventing them from developing undesired disuse-induced motor impairments. Indeed, static stretching has widely been applied to treat and prevent spasticity and contracture in individuals with neurologic diseases (for review see [3,4,5]). However, its underlying mechanisms and thus stretching protocols remain unclear, probably because functional outcome measures (e.g., joint mobility, walking performance) have mainly been discussed.
Understanding how static stretching affects the neuromuscular system may help clinicians develop more effective, subject-specific protocols that can maximize functional outcomes. Specifically, the excitability of spinal motor neurons (i.e., their ability to fire action potentials) is closely associated with motor behavior and performance. It has been shown that after neurological diseases, there are significant changes in the excitability of the corticospinal pathway (as measured by motor evoked potential [MEP]) [6,7,8] and in spinal excitability (as measured by Hoffman reflex [H-reflex] and tendon reflex [T-reflex]) [9,10]. In addition, muscle contractile properties (i.e., the ability of muscles to generate force and movement) are linked to motoneuron excitability as well as motor performance. For instance, muscle architectural parameters (e.g., fascicle length, pennation angle, muscle thickness) are important determinants of muscle function (such as force-generating capacity and shortening velocity) [11,12,13]. It has also been suggested that muscular contraction performance appears to be influenced by an interaction between contractile and passive connective tissues (e.g., stiffness of muscle/tendon tissues) in a pennate muscle [14,15,16,17,18]. Additionally, muscle bulging condition (e.g., the material properties of extracellular connective tissues, transverse loading) can also change muscle performance [19,20,21,22,23]. Therefore, it is essential to understand whether and to what extent the neuromuscular factors could respond to static stretching.
Although a large body of studies have been carried out to understand the effects of stretching, most of the review articles in the literature have primarily focused on mechanical outputs (e.g., one-repetition maximum, maximum muscle strength, muscle power) or performance measures (e.g., vertical jump height, sprint running time, rate of force/torque development, electromechanical delay) [2,24,25,26,27]. Several review studies have addressed the effects of static stretching on neural or muscular responses, but these studies only focused on either the neural or mechanical responses or acute or chronic effects of static stretching [28,29,30,31]. In addition, few review studies have considered outcome measures using shear wave ultrasound elastography (e.g., shear wave velocity, shear elastic modulus), although it has been applied to quantify the effects of static stretching on muscle stiffness over the past decade [32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47].
The aim of this review was to provide an overview of the recent findings on the acute and chronic effects of static stretching on joint behaviors (e.g., range of motion, joint torque) and neuromuscular responses (e.g., motor evoked potentials, reflex responses, muscle architecture, muscle stiffness, tendon stiffness, shear elastic modulus) and to discuss the overall effects of acute and chronic static stretching on the aforementioned outcomes across the studied articles via meta-analyses. The findings of this review could help clinicians obtain a more complete picture of the effects of acute and chronic static stretching on neuromuscular properties, potentially providing the foundation for designing a more subject-specific, effective protocol that might improve neuromuscular responses.
2. Materials and Methods
For this study, we utilized the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines [48]. Using the PubMed, Scopus, and ProQuest databases, all authors independently performed a literature search using the following keyword combinations: static stretching, passive stretching, neural response, motor evoked potential, H-reflex, tendon reflex, stretch reflex, excitability, muscle architecture, fascicle length, pennation angle, muscle thickness, muscle stiffness, tendon stiffness, shear elastic modulus, shear wave speed, and shear wave elastography; for example, “(“static stretch” OR “passive stretch” OR “static stretching” OR “passive stretching”) AND (“neural response” OR “motor evoked potential” OR “H-reflex” OR “tendon reflex” OR “stretch reflex” OR excitability OR “muscle architecture” OR “fascicle length” OR “pennation angle” OR “muscle thickness” OR “ultrasound” OR “muscle stiffness” OR “tendon stiffness” OR “shear elastic modulus” OR “shear wave speed”).” We also found some relevant studies from the references of the selected articles and from a personal library. The PRISMA flow diagram is shown in Figure 1.
The inclusion criteria were as follows: (1) peer-reviewed research articles published in English between January 2012 and December 2022; (2) adults aged 18–50 with no history of serious injury or an ongoing injury (non-athletic and athlete population); (3) static/passive stretching in a single session (acute) or multiple sessions (chronic), targeted lower extremity joints, not combined with other interventions (e.g., voluntary contraction, electrical stimulation); (4) each intervention session dedicated to only one muscle group, not multiple joints or different muscle groups; (5) pre–post comparison of at least one of the aforementioned outcome variables. The exclusion criteria were as follows: (1) participants with neurologic or musculoskeletal injuries; (2) any of the aforementioned outcome measures not available; and (3) other types of publications (e.g., reviews, book chapters, conference proceedings/abstracts, theses, dissertations).
By extracting the necessary information from the reviewed studies (e.g., the number of participants, mean and standard deviation of available outcomes), meta-analyses were conducted to provide more precise estimates of the acute and chronic effects of static stretching on neuromuscular properties. Considering that many studies also reported joint behaviors such as range of motion (ROM), passive resistance torque (PRT), maximum tolerable PRT (PRTmax), maximum voluntary isometric torque (MVIT), and muscle–tendon unit (MTU) stiffness, these parameters were also considered in the meta-analyses.
All the statistical analyses were performed using IBM SPSS Statistics (Version 28, IBM SPSS Inc., Chicago, IL, USA) [49]. Briefly, a random effects model with restricted maximal likelihood estimation was chosen to account for the heterogeneity between the studies. The effect size was calculated using Cohen’s d, and d values of 0.2, 0.5, and 0.8 are considered to indicate small, moderate, and large effect sizes, respectively [50]. The I2 statistic was used to assess the degree of heterogeneity, and I2 values of 25%, 50%, and 75% are considered to indicate low, moderate, and high heterogeneity, respectively [51]. If an outcome measure was not available from at least two studies, a meta-analysis for the outcome measure was not performed.
3. Results
The literature search identified 564 studies, and 7 studies from other sources (i.e., the references of the studies and a personal library) were added (Figure 1). After the removal of duplicates and the screening process, a total of 50 studies (i.e., 31 studies for acute static stretching and 19 studies for chronic static stretching) were eligible for inclusion.
3.1. Acute Effects of Static Stretching
This section reviews the acute (a single session of intervention) effects of static stretching on neuromuscular properties from 31 studies [32,33,34,35,36,37,38,39,40,41,42,43,44,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69]. The total number of participants across the 31 studies was 550 (median: 16; range: 10–30). Of the 31 studies, six studies assessed neural responses (n = 106) [52,53,54,55,56,57], and 25 studies investigated muscular responses [32,33,34,35,36,37,38,39,40,41,42,43,44,58,59,60,61,62,63,64,65,66,67,68,69]. The main findings are summarized in Table 1.
Joint behavior responses were reported in 25 studies [32,34,35,36,37,38,40,41,42,43,44,54,56,57,58,59,60,61,62,63,65,66,67,68,69]. ROM was reported in 24 studies [32,34,35,36,37,38,40,41,42,43,54,56,57,58,59,60,61,62,63,65,66,67,68,69], and all the studies showed a significant increase. Of these studies, one study examined two stretching methods (i.e., constant angle and constant torque) [67], two studies examined two [66] or three [43] different intensities, and one study examined three different rest intervals [41], and the raw values from one study were not available [54]. This led to the attainment of a total of 29 data points from 23 studies. A meta-analysis revealed a significant overall large effect with moderate heterogeneity (d = 0.91; 95% CI = 0.71 to 1.10; p < 0.001; I2 = 53%; Figure 2A).
PRT was reported in 13 studies [35,36,37,42,58,59,60,61,62,63,65,67,68], and all the studies showed a significant decrease. Of these studies, one study examined two stretching methods (i.e., constant angle and constant torque) [67], and the raw values from one study were not available [60]. This led to the attainment of a total of 13 data points from 12 studies. A meta-analysis revealed a significant overall moderate to large effect with low heterogeneity (d = −0.59; 95% CI = −0.81 to −0.38; p < 0.001; I2 = 13%; Figure 2B).
PRTmax was reported in five studies [37,41,58,59,60], showing a significant increase in all but one study [37]. Of these five studies, one study examined three different rest intervals [41], and the raw values from two studies were not available [59,60], which led to a total of five data points being available. A meta-analysis revealed a significant overall moderate to large effect with low heterogeneity (d = 0.78; 95% CI = 0.41 to 1.16; p < 0.001; I2 = 18%; Figure 2C).
MVIT was reported in 12 studies [32,44,54,56,57,59,60,61,62,65,67,69], and nine studies showed a significant decrease [44,54,56,57,59,60,62,65,69], whereas three studies did not show a significant change [32,61,67]. Of these studies, one study examined two stretching methods [67], one study examined two protocols [54], and the raw values from one study were not available [60], leading to a total of 13 data points from eleven studies. A meta-analysis revealed a significant small to moderate effect with moderate to high heterogeneity (d = −0.48; 95% CI = −0.82 to −0.15; p = 0.01; I2 = 68%; Figure 2D).
MTU stiffness was reported in 11 studies [32,58,59,60,61,62,63,65,66,67,68], and 10 studies showed a significant decrease [32,58,59,60,61,62,63,65,67,68], while one study did not show a significant change [66]. Of these studies, one study examined two stretching methods [67], one study examined two different intensities [66], and the raw values from one study were not available [58], leading to a total of 12 data points from 10 studies. A meta-analysis revealed a significant low to moderate effect with no heterogeneity (d = −0.33; 95% CI = −0.54 to −0.13; p < 0.001; I2 = 0%; Figure 2E).
Neural responses were reported in six studies [52,53,54,55,56,57]. Two studies examined only the soleus [52,53], two studies examined two muscles (i.e., soleus and medial gastrocnemius [54,56]), and two studies examined three muscles (i.e., soleus and medial/lateral gastrocnemius [55,57]). Regarding the MEP amplitude [52,53,54,55,56], four studies showed no significant change in the soleus [52,53,54,56], and one study showed no significant change in the medial gastrocnemius [55], while one study showed a significant increase in the soleus and lateral gastrocnemius [55]. Of these studies, one study examined two protocols [54], and the raw values from one study were not available [53], leading to a total of seven datapoints from four studies. A meta-analysis revealed no significant overall small effect with no heterogeneity (d = 0.24; 95% CI = −0.03 to 0.51; p = 0.08; I2 = 0%; Figure 3A).
Regarding the H-reflex amplitude [52,53,55,56,57], three studies showed no significant change in both the soleus and medial gastrocnemius [55,56,57], and two studies showed no significant change in the lateral gastrocnemius [55,57], whereas two studies showed a significant increase in the soleus [52,53]. Of these studies, the raw values from one study were not available [53]; thus, eight data points were available from four studies. A meta-analysis revealed no significant overall small effect with no heterogeneity (d = −0.02; 95% CI = −0.24 to 0.20; p = 0.85; I2 = 0%; Figure 3B).
Regarding the T-reflex amplitude, two studies showed a significant decrease in the soleus [52,53], but a meta-analysis was not conducted because raw values were only available from one study [52].
Regarding the M-wave amplitude [54,55,56,57], all the studies did not show a significant change in the soleus [54,55,56,57], medial gastrocnemius [54,55,56,57], and lateral gastrocnemius [55,57]. A meta-analysis revealed no significant overall small effect with no heterogeneity (d = 0.05; 95% CI = −0.14 to 0.25; p = 0.58; I2 = 0%; Figure 3C).
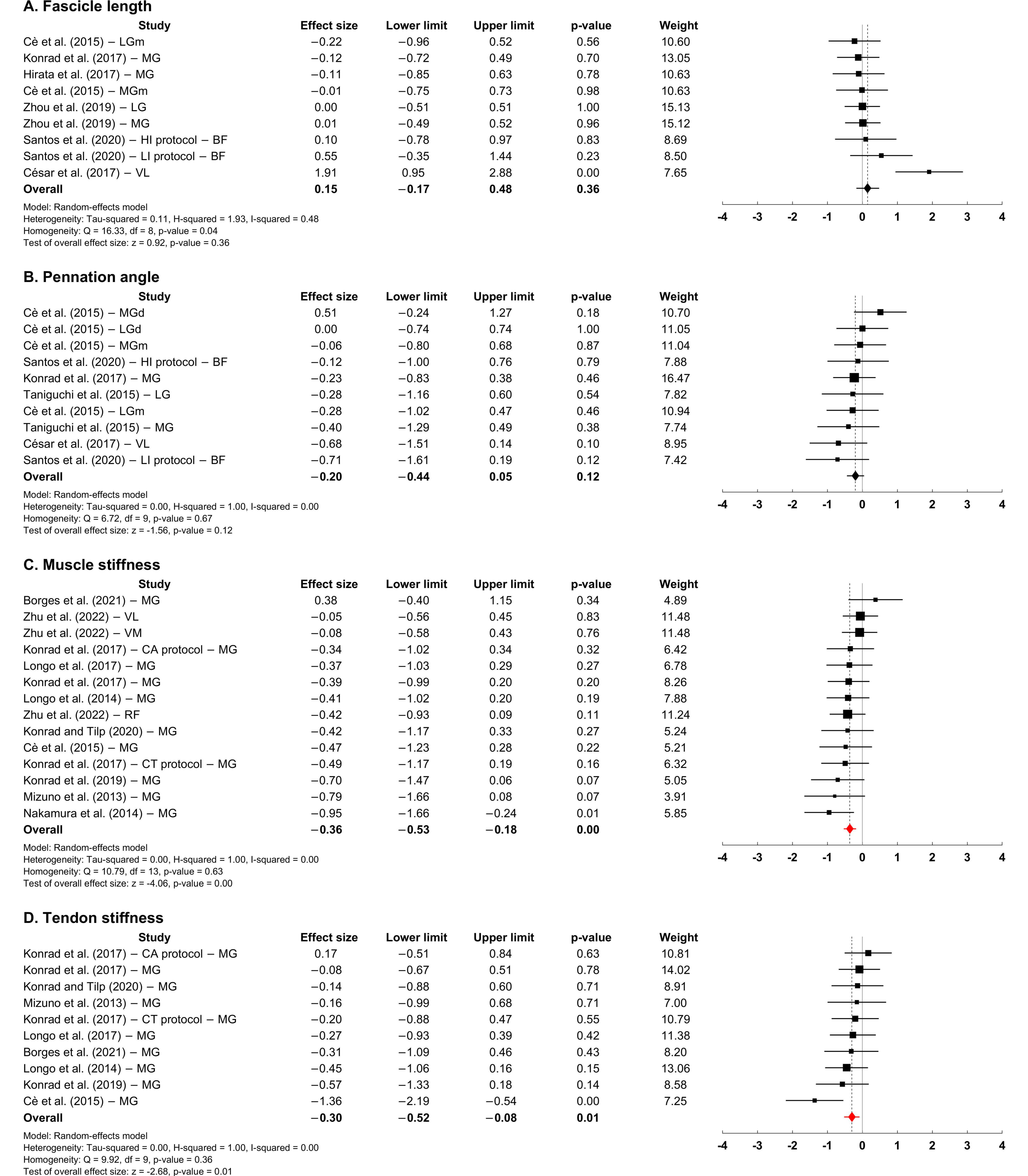
Muscular responses were reported in 25 studies [32,33,34,35,36,37,38,39,40,41,42,43,44,58,59,60,61,62,63,64,65,66,67,68,69]. Six studies reported the resting fascicle length [37,40,60,61,64,66]; three studies examined one muscle (i.e., medial gastrocnemius [37,61], vastus lateralis [64]), two studies examined two muscles (i.e., medial/lateral gastrocnemius [40,60]), and one study examined one muscle but two protocols (i.e., biceps femoris [66]), leading to a total of nine available data points, and only one study showed a significant increase [64]. A meta-analysis revealed no significant overall small effect with low to moderate heterogeneity (d = 0.15; 95% CI = −0.17 to 0.48; p = 0.36; I2 = 48%; Figure 4A).
The resting pennation angle was reported in five studies [34,60,61,64,66]; two studies examined one muscle (i.e., medial gastrocnemius [61], vastus lateralis [64]), two studies examined two muscles (i.e., medial/lateral gastrocnemius [34,60]), and one study examined one muscle but two protocols (i.e., biceps femoris [66]). This led to a total of 10 available data points, and only one data point showed a significant decrease [64]. A meta-analysis revealed no significant overall small effect with no heterogeneity (d = −0.20; 95% CI = −0.44 to 0.05; p = 0.12; I2 = 0%; Figure 4B).
Muscle stiffness was reported in 11 studies [33,58,59,60,61,62,63,65,67,68,69]; nine studies examined one muscle (i.e., medial gastrocnemius [33,58,59,60,61,62,65,67,68]), one study examined three muscles (i.e., rectus femoris and vastus medialis/lateralis [69]), and one study examined one muscle but two protocols (i.e., medial gastrocnemius [63]). This led to a total of 14 data points available from the 11 studies. Eleven data points showed a significant decrease, whereas three showed no significant change from two studies [68,69]. A meta-analysis revealed a significant overall small to moderate effect with no heterogeneity (d = −0.36; 95% CI = −0.53 to −0.18; p < 0.001; I2 = 0%; Figure 4C).
Tendon stiffness was reported in nine studies [58,59,60,61,62,63,65,67,68]; eight studies examined one muscle (i.e., medial gastrocnemius [58,59,60,61,62,65,67,68]), and one study examined one muscle but two protocols (i.e., medial gastrocnemius [63]), leading to a total of 10 data points. Three data points showed a significant decrease from three studies [59,60,62], whereas seven showed no significant changes from six studies [58,61,63,65,67,68]. A meta-analysis revealed a significant overall small to moderate effect with no heterogeneity (d = −0.30; 95% CI = −0.52 to −0.08; p = 0.01; I2 = 0%; Figure 4D).
Thirteen studies reported the shear elastic modulus [32,33,34,35,36,37,38,39,40,41,42,43,44]; three studies examined one muscle (i.e., medial gastrocnemius [33,37,41]), three studies examined two muscles (i.e., medial/lateral gastrocnemius [32,34,38]), two studies examined three muscles (i.e., soleus and medial/lateral gastrocnemius [36], or biceps femoris, semitendinosus, and semimembranosus [35]), two studies examined medial gastrocnemius with a different protocol (i.e., 10-/30-/90-s interval [44], or 0-/30-s interval [39]), one study examined three different regions (i.e., proximal/middle/distal parts) of two muscles (i.e., medial/lateral gastrocnemius) [40], one study examined three muscles (i.e., rectus femoris and vastus medialis/lateralis) with three different intensities (i.e., 120%/100%/80% intensity [43]), and one study examined three muscles but with more measurement sites (i.e., soleus, lateral gastrocnemius, central/distal medial gastrocnemius) [42], and the raw values for the soleus reported in one study [42] were not available. This led to the attainment of a total of 38 shear elastic modulus data points from the 13 studies, and the shear elastic modulus significantly decreased in 27 out of the 38 data points. A meta-analysis revealed a significant overall moderate to large effect with low to moderate heterogeneity (d = −0.59; 95% CI = −0.74 to −0.44; p < 0.001; I2 = 46%; Figure 4E).
3.2. Chronic Effects of Static Stretching
This section reviews the chronic (multiple sessions of intervention over several weeks) effects of static stretching on neuromuscular properties from 19 recent studies [45,46,47,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86]. The total number of participants across the 19 studies was 327 (median: 15; range: 5–28). Of the 19 studies, one study assessed both neural and muscular responses (n = 12) [72], one study investigated neural responses [71], and 17 studies investigated muscular responses [45,46,47,73,74,75,76,77,78,79,80,81,82,83,84,85,86]. The main findings are summarized in Table 2.
Joint behavior responses were reported in 18 studies [45,47,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86]. ROM was reported in 16 studies [45,47,71,72,73,74,75,76,77,78,79,82,83,84,85,86]; four studies examined two stretching methods in terms of stretching intensity [78,84,86] and the total number of sessions [79], and the raw values from one study [73] were not available. This led to the attainment of a total of 19 data points from 16 studies, and 17 of the 19 data points showed a significant increase. A meta-analysis revealed a significant overall large effect with low heterogeneity (d = 0.94; 95% CI = 0.73 to 1.15; p < 0.001; I2 = 18%; Figure 5A).
PRT was reported in seven studies [47,71,72,73,74,78,83], showing no significant change in all but three studies [47,73,83]. Of these studies, one study examined two stretching methods in terms of stretching intensity [78], and the raw values from one study [73] were not available, leading to a total of seven data points being available from six studies. A meta-analysis revealed no significant overall small effect with low to moderate heterogeneity (d = −0.19; 95% CI = −0.57 to 0.18; p = 0.31; I2 = 43%; Figure 5B).
PRTmax was reported in eight studies [72,76,78,82,83,84,85,86], and three studies examined two stretching methods in terms of stretching intensity [78,84,86]. This led to the attainment of a total of 11 data points from the studies, and seven out of the 11 data points showed a significant increase. A meta-analysis revealed a significant overall moderate to large effect with low to moderate heterogeneity (d = 0.71; 95% CI = 0.39 to 1.02; p < 0.001; I2 = 40%; Figure 5C).
MVIT was reported in nine studies [45,71,72,74,80,81,82,83,84], showing no significant change in all but one study [81]. Of these studies, two studies examined two stretching methods in terms of stretching intensity [84] and the total number of sessions [80], leading to a total of 11 data points. A meta-analysis revealed no significant small effect with no heterogeneity (d = 0.08; 95% CI = −0.13 to 0.30; p = 0.44; I2 = 0%; Figure 5D).
MTU stiffness was reported in five studies [45,72,74,78,82], showing no significance in all but one study [82]. Of these studies, one study examined two stretching methods in terms of stretching intensity [78], leading to a total of six data points. A meta-analysis revealed no significant low effect with no heterogeneity (d = −0.12; 95% CI = −0.43 to 0.20; p = 0.47; I2 = 0%; Figure 5E).
Neural responses were reported in two studies [71,72] and demonstrated a significant decrease in the H-reflex amplitude in both the soleus and medial gastrocnemius. However, the raw values from one study [71] were not available; thus, a meta-analysis was not conducted.
Muscular responses were reported in 18 studies [45,46,47,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86]. Twelve studies reported the resting fascicle length [47,72,73,74,75,78,81,82,83,84,85,86]; six studies examined one muscle (i.e., medial gastrocnemius [72,73,74,83,85], biceps femoris [75]), two studies examined two muscles (i.e., medial/lateral gastrocnemius [47,81]), one study examined one muscle but two protocols (i.e., biceps femoris [78]), one study examined two different regions (i.e., middle/distal parts) of three muscles (i.e., soleus and medial/lateral gastrocnemius) [82], two studies examined two muscles (i.e., medial/lateral gastrocnemius) with two protocols [84,86], and the raw values from one study [73] were not available. This led to the attainment of a total of 25 data points from 11 studies, and only two out of the 25 data points showed a significant increase. A meta-analysis revealed no significant overall small effect with no heterogeneity (d = 0.04; 95% CI = −0.11 to 0.19; p = 0.60; I2 = 0%; Figure 6A).
Eleven studies reported the resting pennation angle [74,75,77,78,80,81,82,83,84,85,86]; five studies examined one muscle (i.e., medial gastrocnemius [74,77,83,85], biceps femoris [75]), one study examined two muscles (i.e., medial/lateral gastrocnemius [81]), two studies examined one muscle but two protocols (i.e., biceps femoris [78], medial gastrocnemius [80]), one study examined two different regions (i.e., middle/distal parts) of three muscles (i.e., soleus and medial/lateral gastrocnemius) [82], and two studies examined two muscles (i.e., medial/lateral gastrocnemius) with two protocols [84,86]. This led to a total of 25 data points being available, and only one out of the 25 data points showed a significant increase. A meta-analysis revealed no significant overall small effect with no heterogeneity (d = 0.06; 95% CI = −0.09 to 0.21; p = 0.45; I2 = 0%; Figure 6B.
Muscle thickness was reported in nine studies [47,75,77,80,81,82,83,84,86]; three studies examined one muscle (i.e., medial gastrocnemius [77,83], biceps femoris [75]), two studies examined three muscles (i.e., soleus and medial/lateral gastrocnemius [81,82]), two studies examined one muscle but two protocols (i.e., medial gastrocnemius [47,80]), and two studies examined three muscles (i.e., soleus and medial/lateral gastrocnemius) with two protocols [84,86]. This led to a total of 25 available data points from the nine studies, and only two out of the 25 data points showed a significant increase. A meta-analysis revealed no significant overall small effect with no heterogeneity (d = 0.05; 95% CI = −0.09 to 0.20; p = 0.49; I2 = 0%; Figure 6C).
Muscle stiffness was reported in seven studies [72,74,76,79,82,84,86]; four studies examined one muscle (i.e., medial gastrocnemius [72,74,76,82]), and three studies examined one muscle but two protocols [79,84,86]. This led to a total of 10 available data points, and five out of the 10 data points showed a significant decrease. A meta-analysis revealed a significant overall small to moderate effect with low to moderate heterogeneity (d = −0.35; 95% CI = −0.67 to −0.02; p = 0.04; I2 = 48%; Figure 6D).
Four studies reported tendon stiffness [72,74,85] or tangent modulus [83], and all the studies did not show a significant change. Of these studies, two studies reported two values that were obtained from two different sites (i.e., free/whole Achilles tendon [83]) or from the middle and final third parts of the stress–strain curve [85], leading to a total of six data points from the four studies. A meta-analysis revealed no significant overall small effect with no heterogeneity (d = 0.05; 95% CI = −0.22 to 0.33; p = 0.70; I2 = 0%; Figure 6E).
Three studies reported shear elastic modulus [45,46] or shear wave speed [47]; one study examined two muscles (i.e., medial/lateral gastrocnemius [45]), one study examined three muscles (i.e., semitendinosus, semimembranosus, and biceps femoris [46]), and one study measured the shear wave speed from two different regions (i.e., proximal/distal parts) for soleus and from three different regions (i.e., proximal/intermediate/distal parts) for medial/lateral gastrocnemius [47]. This led to a total of 13 data points being available from the three studies, and 12 out of the 13 data points showed a significant decrease. A meta-analysis revealed a significant overall moderate to large effect with no heterogeneity (d = −0.58; 95% CI = −0.76 to −0.40; p < 0.001; I2 = 0%; Figure 6F).
4. Discussion and Conclusions
The purpose of this review was to evaluate the acute and chronic effects of static stretching on neuromuscular properties by summarizing the selected joint behaviors and neuromuscular responses based on data from the recent literature. The results of our meta-analyses based on the reviewed studies suggested that (1) acute static stretching may change joint behaviors (e.g., increased ROM, decreased PRT, increased PRTmax, decreased MVIT, decreased MTU stiffness) and muscular responses (e.g., decreased muscle stiffness, decreased tendon stiffness, decreased shear elastic modulus), and that (2) chronic static stretching may change joint behaviors (e.g., increased ROM, increased PRTmax) and muscular responses (e.g., decreased muscle stiffness, decreased shear elastic modulus or shear wave speed).
It has been suggested that a stretching-induced increase in ROM may be a result of an increase in stretch tolerance (i.e., the ability to tolerate the discomfort at the end of ROM) [87] and/or changes in MTU mechanical properties (e.g., reduced stiffness of muscle and connective tissues) [88]. The results from our meta-analyses support the findings that both acute and chronic static stretching appear to be effective in increasing ROM and PRTmax (a measure of an increase in stretch tolerance), suggesting that the increased ROM may be explained, in part, by an increase in stretch tolerance, as reflected in the increased PRTmax. Moreover, considering the significant overall effect for the MTU stiffness and muscle/tendon stiffness after acute static stretching, increased ROM in response to acute static stretching may also be associated with reduced MTU mechanical properties. However, as the results of our meta-analyses showed no significant overall effect for the MTU stiffness and tendon stiffness after chronic static stretching, the potential associations between the increased ROM and changes in MTU mechanical properties in response to chronic static stretching are unclear. Interestingly, despite no significant changes in MTU stiffness and tendon stiffness, muscle stiffness and shear elastic modulus or shear wave speed (i.e., muscle-specific variables) were significantly reduced in response to chronic static stretching. These results may imply that in the reviewed studies, changes in the mechanical properties of muscle tissue did not lead to changes in mechanical behavior at joint levels, especially for chronic static stretching.
Indeed, based on the presumption that non-muscular structures (e.g., fasciae, nerves, vessels, skin) sitting in/around/across muscles can also contribute to the mechanical properties measured at joint levels, the non-muscular structures have been considered a possible contributor to changes in joint behavior in response to static stretching. For example, it has been evidenced that ankle joint ROM is substantially influenced by different hip and knee joint positions [89], and such notable hip joint position-dependent ankle ROM was observed even without significant changes in ankle joint torque and MG shear elastic modulus for a given ankle angle [90]. These findings have emphasized the possible role of fasciae which connect inter-muscles from ankle to hip/spine joints, also referred to myofascial tissue connectivity (for review see [91]). Acute static stretching protocols aiming to load the sciatic nerve also led to a significant increase in ankle ROM and a significant decrease in the sciatic nerve shear wave velocity (an index of stiffness) without significant changes in MG and BF shear wave velocity, indicating that changes in the mechanical properties of nerves only can directly affect a joint’s ROM without changes in the mechanical properties of the muscles across the joint [92]. Together with the fact that the increased ROM was strongly correlated with age-related increased fascia thickness [93] and with decreased sciatic nerve shear wave velocity [92], it seems possible that static stretching-induced changes in passive joint behavior is attributable, in part, to changes in the mechanical properties of the non-muscular structures (for review see [91,94]). In addition to the possible mechanical contribution of the non-muscular structures, given that fasciae are densely innervated with sensory nerves, including proprioceptors and nociceptors [95,96], the sensitivity of the sensory neurons responsible for the sensation of pain (e.g., nociceptors) may be altered in response to static stretching and thus may contribute to an increase in stretch tolerance.
It is also plausible that an increase in stretch tolerance might result from some neural adaptations, which could be reflected in altered neural responses to static stretching. However, the results of our meta-analyses demonstrated no significant change in neural responses. Although a meta-analysis for the effects of chronic static stretching on neural responses was not conducted due to the limited data available from the reviewed studies, neural responses to chronic static stretching are seemingly not associated with increased stretch tolerance, which was evaluated at a stretched position. For example, the spinal reflex excitability (e.g., Hmax/Mmax ratio) was significantly reduced in the resting lengths but not in the stretched lengths of both the SOL and MG after 3 weeks static of stretching training [72], and the maximum voluntary activation (e.g., RMS EMG) of the triceps surae did not change after a 12-week static stretch intervention [82]. Collectively, it appears that acute and chronic static stretching may not lead to a significant change in neural responses, and an increase in stretch tolerance may be possible without significant changes in reflex and voluntary responses.
Decreases in maximum isometric force generation after acute static stretching, so called stretch-induced force loss, have received consistent attention, probably because reduced muscle performance after static stretching as a means of a warm-up before competitive exercise is undesirable. Two primary hypotheses have been developed to explain such stretching-induced force deficits: (1) mechanical factors such as altered MTU mechanical properties and (2) neural factors such as a reduced efferent neural drive and altered motor control strategies (for review see [97]). First, the results of our meta-analyses appear to support the mechanical hypothesis that more compliant tendons can lead to stretching-induced force loss, presumably shifting the fiber/fascicle operating range toward the ascending limb of the active force–length curve [98,99]. In addition, the fact that the overall effect size was significant for the MTU mechanical properties and shear elastic modulus but not for muscle fascicle length suggests the possibility of stretching-induced changes in the mechanical properties of the intramuscular connective tissue (e.g., endomysium, perimysium, epimysium) [73,100]. As these connective tissues connect adjacent fibers, fascicles, and muscles directly and indirectly, they are known to provide a route by which active contractile forces can be transmitted to the adjacent fibers/fascicles/muscles, also referred to as myofascial force transmission (for review see [101,102,103]). In this regard, more compliant connective tissues, as a result of static stretching if any, could compromise the efficiency of the force transmission, potentially resulting in decreased MVIT.
The results of our meta-analyses did not support the possible contribution of corticospinal excitability and spinal reflex excitability to the stretching-induced force loss, as also suggested by previous studies [54,56,104]. However, based on the fact that the EMG amplitude normalized to Mmax and the relative voluntary muscle activation (estimated using the interpolated twitch technique) significantly reduced after stretching [104,105], there seem to be other potential neurophysiological mechanisms that may influence the effective, voluntary neural drive. For example, afferent signals from some peripheral proprioceptive structures, such as muscle spindles, Golgi tendon organs, and free nerve endings, are likely integrated in the process of muscle force control (for review see [106]). In particular, the amplification of the motor command provided by persistent inward currents in motor neurons seems to be reduced after static stretching, which might prevent the motoneurons from discharging at higher firing rates (for review see [31]). Indeed, Mazzo et al. [107] reported that the magnitude of neural drive (estimated from the cumulative spike train) to the plantar flexors significantly increased after static stretching, albeit during low isometric contraction at 10% of MVIT. Future studies are required to study the effects of static stretching on spinal motoneuron firing behaviors and the association between motoneuron excitability and stretch-induced force loss.
The present review has several limitations. First, this review does not include all the relevant studies, probably due to the limitations in the keyword searches and search engine algorithms used. This may have biased the results of the current meta-analyses. Second, the static stretching protocols in each of the studies varied in terms of dosage, intensity, and target joint and muscle, and this was not considered in the meta-analyses. Third, the participants in the studies were mostly young healthy male individuals, so the current results may not be generalizable to other populations, such as older adults, female individuals, and patients with neurologic diseases or musculoskeletal injuries. Lastly, many data points in the meta-analyses came from the same articles or research teams, which may lead to an overestimation of the effect size.
In conclusion, static stretching may be effective for increasing range of motion and reducing muscle, tendon, and muscle–tendon unit stiffness. However, the reduced stiffness of tendons and the muscle–tendon units is likely an acute response, suggesting that long-term (chronic) static stretching may be beneficial for improving the flexibility of joint and muscle tissue than the flexibility of tendons and the muscle–tendon units. Moreover, static stretching alone may not significantly change neural excitability and muscle architecture. Given that long-term disuse (e.g., due to neurological diseases) likely leads to measurable changes in neural excitability and muscle contractile properties, further studies are required to explore the impact of various aspects of static stretching protocols, such as intensity, duration, and dosage. Furthermore, it is essential to investigate how the integration of static stretching with various sensorimotor stimuli can reshape the neuromuscular systems.
Author Contributions
Conceptualization, J.S.; methodology, R.S., M.W.S. and J.S.; software, J.S.; validation, R.S., M.W.S. and J.S.; formal analysis, J.S.; investigation, R.S., M.W.S. and J.S.; resources, J.S.; data curation, R.S., M.W.S. and J.S.; writing—original draft preparation, R.S., M.W.S. and J.S.; writing—review and editing, J.S.; visualization, J.S.; supervision, J.S.; project administration, J.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- McHugh, M.P.; Cosgrave, C.H. To stretch or not to stretch: The role of stretching in injury prevention and performance. Scand. J. Med. Sci. Sports 2010, 20, 169–181. [Google Scholar] [CrossRef] [PubMed]
- Behm, D.G.; Blazevich, A.J.; Kay, A.D.; McHugh, M. Acute effects of muscle stretching on physical performance, range of motion, and injury incidence in healthy active individuals: A systematic review. Appl. Physiol. Nutr. Metab. 2015, 41, 1–11. [Google Scholar] [CrossRef]
- Harvey, L.A.; Herbert, R.D. Muscle stretching for treatment and prevention of contracture in people with spinal cord injury. Spinal Cord 2002, 40, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Bovend’Eerdt, T.J.; Newman, M.; Barker, K.; Dawes, H.; Minelli, C.; Wade, D.T. The Effects of Stretching in Spasticity: A Systematic Review. Arch. Phys. Med. Rehabil. 2008, 89, 1395–1406. [Google Scholar] [CrossRef] [PubMed]
- Salazar, A.P.; Pinto, C.; Ruschel Mossi, J.V.; Figueiro, B.; Lukrafka, J.L.; Pagnussat, A.S. Effectiveness of static stretching positioning on post-stroke upper-limb spasticity and mobility: Systematic review with meta-analysis. Ann. Phys. Rehabil. Med. 2019, 62, 274–282. [Google Scholar] [CrossRef]
- Rapisarda, G.; Bastings, E.; Noordhout, A.M.d.; Pennisi, G.; Delwaide, P.J. Can Motor Recovery in Stroke Patients Be Predicted by Early Transcranial Magnetic Stimulation? Stroke 1996, 27, 2191–2196. [Google Scholar] [CrossRef]
- Brum, M.; Cabib, C.; Valls-Solé, J. Clinical Value of the Assessment of Changes in MEP Duration with Voluntary Contraction. Front. Neurosci. 2016, 9, 505. [Google Scholar] [CrossRef]
- Cleland, B.T.; Sisel, E.; Madhavan, S. Motor evoked potential latency and duration from tibialis anterior in individuals with chronic stroke. Exp. Brain Res. 2021, 239, 2251–2260. [Google Scholar] [CrossRef]
- Phadke, C.P.; Robertson, C.T.; Condliffe, E.G.; Patten, C. Upper-extremity H-reflex measurement post-stroke: Reliability and inter-limb differences. Clin. Neurophysiol. 2012, 123, 1606–1615. [Google Scholar] [CrossRef]
- Afzal, T.; Chardon, M.K.; Rymer, W.Z.; Suresh, N.L. Stretch reflex excitability in contralateral limbs of stroke survivors is higher than in matched controls. J. Neuroeng. Rehabil. 2019, 16, 154. [Google Scholar] [CrossRef]
- Gans, C.; Gaunt, A.S. Muscle architecture in relation to function. J. Biomech. 1991, 24 (Suppl. S1), 53–65. [Google Scholar] [CrossRef] [PubMed]
- Fukunaga, T.; Kawakami, Y.; Kuno, S.; Funato, K.; Fukashiro, S. Muscle architecture and function in humans. J. Biomech. 1997, 30, 457–463. [Google Scholar] [CrossRef]
- Lieber, R.L.; Fridén, J. Functional and Clinical Significance of Skeletal Muscle Architecture. Muscle Nerve 2000, 23, 1647–1666. [Google Scholar] [CrossRef] [PubMed]
- Azizi, E.; Brainerd, E.L.; Roberts, T.J. Variable gearing in pennate muscles. Proc. Natl. Acad. Sci. USA 2008, 105, 1745–1750. [Google Scholar] [CrossRef]
- Randhawa, A.; Wakeling, J.M. Associations between muscle structure and contractile performance in seniors. Clin. Biomech. 2013, 28, 705–711. [Google Scholar] [CrossRef]
- Holt, N.C.; Danos, N.; Roberts, T.J.; Azizi, E. Stuck in gear: Age-related loss of variable gearing in skeletal muscle. J. Exp. Biol. 2016, 219, 998–1003. [Google Scholar] [CrossRef] [PubMed]
- Son, J.; Rymer, W.Z. Loss of variable fascicle gearing during voluntary isometric contractions of paretic medial gastrocnemius muscles in male chronic stroke survivors. J. Physiol. 2020, 598, 5183–5194. [Google Scholar] [CrossRef]
- Monte, A.; Zignoli, A. Muscle and tendon stiffness and belly gearing positively correlate with rate of torque development during explosive fixed end contractions. J. Biomech. 2021, 114, 110110. [Google Scholar] [CrossRef]
- Wakeling, J.M.; Jackman, M.; Namburete, A.I. The Effect of External Compression on the Mechanics of Muscle Contraction. J. Appl. Biomech. 2013, 29, 360–364. [Google Scholar] [CrossRef]
- Siebert, T.; Till, O.; Stutzig, N.; Günther, M.; Blickhan, R. Muscle force depends on the amount of transversal muscle loading. J. Biomech. 2014, 47, 1822–1828. [Google Scholar] [CrossRef]
- Rahemi, H.; Nigam, N.; Wakeling, J.M. The effect of intramuscular fat on skeletal muscle mechanics: Implications for the elderly and obese. J. R. Soc. Interface 2015, 12, 20150365. [Google Scholar] [CrossRef] [PubMed]
- Siebert, T.; Eb, M.; Ryan, D.S.; Wakeling, J.M.; Stutzig, N. Impact of Multidirectional Transverse Calf Muscle Loading on Calf Muscle Force in Young Adults. Front. Physiol. 2018, 9, 1148. [Google Scholar] [CrossRef] [PubMed]
- Stutzig, N.; Ryan, D.; Wakeling, J.M.; Siebert, T. Impact of transversal calf muscle loading on plantarflexion. J. Biomech. 2019, 85, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Behm, D.G.; Chaouachi, A. A review of the acute effects of static and dynamic stretching on performance. Eur. J. Appl. Physiol. 2011, 111, 2633–2651. [Google Scholar] [CrossRef]
- Chaabene, H.; Behm, D.G.; Negra, Y.; Granacher, U. Acute Effects of Static Stretching on Muscle Strength and Power: An Attempt to Clarify Previous Caveats. Front. Physiol. 2019, 10, 1468. [Google Scholar] [CrossRef]
- Kay, A.D.; Blazevich, A.J. Effect of Acute Static Stretch on Maximal Muscle Performance: A Systematic Review. Med. Sci. Sports Exerc. 2012, 44, 154–164. [Google Scholar] [CrossRef]
- Simic, L.; Sarabon, N.; Markovic, G. Does pre-exercise static stretching inhibit maximal muscular performance? A meta-analytical review. Scand. J. Med. Sci. Sports 2013, 23, 131–148. [Google Scholar] [CrossRef]
- Guissard, N.; Duchateau, J. Neural Aspects of Muscle Stretching. Exerc. Sport Sci. Rev. 2006, 34, 154–158. [Google Scholar] [CrossRef]
- Freitas, S.R.; Mendes, B.; Le Sant, G.; Andrade, R.J.; Nordez, A.; Milanovic, Z. Can chronic stretching change the muscle-tendon mechanical properties? A review. Scand. J. Med. Sci. Sports 2018, 28, 794–806. [Google Scholar] [CrossRef]
- Nunes, J.P.; Schoenfeld, B.J.; Nakamura, M.; Ribeiro, A.S.; Cunha, P.M.; Cyrino, E.S. Does stretch training induce muscle hypertrophy in humans? A review of the literature. Clin. Physiol. Funct. Imaging 2020, 40, 148–156. [Google Scholar] [CrossRef]
- Trajano, G.S.; Blazevich, A.J. Static Stretching Reduces Motoneuron Excitability: The Potential Role of Neuromodulation. Exerc. Sport Sci. Rev. 2021, 49, 126–132. [Google Scholar] [CrossRef] [PubMed]
- Akagi, R.; Takahashi, H. Acute Effect of Static Stretching on Hardness of the Gastrocnemius Muscle. Med. Sci. Sports Exerc. 2013, 45, 1348–1354. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, M.; Ikezoe, T.; Kobayashi, T.; Umegaki, H.; Takeno, Y.; Nishishita, S.; Ichihashi, N. Acute Effects of Static Stretching on Muscle Hardness of the Medial Gastrocnemius Muscle Belly in Humans: An Ultrasonic Shear-Wave Elastography Study. Ultrasound Med. Biol. 2014, 40, 1991–1997. [Google Scholar] [CrossRef] [PubMed]
- Taniguchi, K.; Shinohara, M.; Nozaki, S.; Katayose, M. Acute decrease in the stiffness of resting muscle belly due to static stretching. Scand. J. Med. Sci. Sports 2015, 25, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Umegaki, H.; Ikezoe, T.; Nakamura, M.; Nishishita, S.; Kobayashi, T.; Fujita, K.; Tanaka, H.; Ichihashi, N. Acute effects of static stretching on the hamstrings using shear elastic modulus determined by ultrasound shear wave elastography: Differences in flexibility between hamstring muscle components. Man. Ther. 2015, 20, 610–613. [Google Scholar] [CrossRef]
- Hirata, K.; Miyamoto-Mikami, E.; Kanehisa, H.; Miyamoto, N. Muscle-specific acute changes in passive stiffness of human triceps surae after stretching. Eur. J. Appl. Physiol. 2016, 116, 911–918. [Google Scholar] [CrossRef] [PubMed]
- Hirata, K.; Kanehisa, H.; Miyamoto, N. Acute effect of static stretching on passive stiffness of the human gastrocnemius fascicle measured by ultrasound shear wave elastography. Eur. J. Appl. Physiol. 2017, 117, 493–499. [Google Scholar] [CrossRef]
- Nakamura, M.; Ikezoe, T.; Nishishita, S.; Umehara, J.; Kimura, M.; Ichihashi, N. Acute effects of static stretching on the shear elastic moduli of the medial and lateral gastrocnemius muscles in young and elderly women. Musculoskelet. Sci. Pract. 2017, 32, 98–103. [Google Scholar] [CrossRef]
- Nojiri, S.; Ikezoe, T.; Nakao, S.; Umehara, J.; Motomura, Y.; Yagi, M.; Hirono, T.; Ichihashi, N. Effect of static stretching with different rest intervals on muscle stiffness. J. Biomech. 2019, 90, 128–132. [Google Scholar] [CrossRef]
- Zhou, J.; Liu, C.; Zhang, Z. Non-uniform Stiffness within Gastrocnemius-Achilles tendon Complex Observed after Static Stretching. J. Sports Sci. Med. 2019, 18, 454–461. [Google Scholar]
- Nakamura, M.; Sato, S.; Kiyono, R.; Takahashi, N.; Yoshida, T. Effect of Rest Duration Between Static Stretching on Passive Stiffness of Medial Gastrocnemius Muscle In Vivo. J. Sport Rehabil. 2020, 29, 578–582. [Google Scholar] [CrossRef] [PubMed]
- Hirata, K.; Yamadera, R.; Akagi, R. Can Static Stretching Reduce Stiffness of the Triceps Surae in Older Men? Med. Sci. Sports Exerc. 2020, 52, 673–679. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, M.; Sato, S.; Murakami, Y.; Kiyono, R.; Yahata, K.; Sanuki, F.; Yoshida, R.; Fukaya, T.; Takeuchi, K. The Comparison of Different Stretching Intensities on the Range of Motion and Muscle Stiffness of the Quadriceps Muscles. Front. Physiol. 2021, 11, 628870. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, M.; Sato, S.; Kiyono, R.; Yahata, K.; Yoshida, R.; Fukaya, T.; Nishishita, S.; Knorad, A. Relationship between changes in passive properties and muscle strength after static stretching. J. Bodyw. Mov. Ther. 2021, 28, 535–539. [Google Scholar] [CrossRef]
- Akagi, R.; Takahashi, H. Effect of a 5-week static stretching program on hardness of the gastrocnemius muscle. Scand. J. Med. Sci. Sports 2014, 24, 950–957. [Google Scholar] [CrossRef]
- Ichihashi, N.; Umegaki, H.; Ikezoe, T.; Nakamura, M.; Nishishita, S.; Fujita, K.; Umehara, J.; Nakao, S.; Ibuki, S. The effects of a 4-week static stretching programme on the individual muscles comprising the hamstrings. J. Sports Sci. 2016, 34, 2155–2159. [Google Scholar] [CrossRef]
- Andrade, R.J.; Freitas, S.R.; Hug, F.; Sant, G.L.; Lacourpaille, L.; Gross, R.; Quillard, J.-B.; McNair, P.J.; Nordez, A. Chronic effects of muscle and nerve-directed stretching on tissue mechanics. J. Appl. Physiol. 2020, 129, 1011–1023. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Sen, S.; Yildirim, I. A Tutorial on How to Conduct Meta-Analysis with IBM SPSS Statistics. Psych 2022, 4, 640–667. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge Academic: New York, NY, USA, 1988. [Google Scholar]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Budini, F.; Gallasch, E.; Christova, M.; Rafolt, D.; Rauscher, A.B.; Tilp, M. One minute static stretch of plantar flexors transiently increases H reflex excitability and exerts no effect on corticospinal pathways. Exp. Physiol. 2017, 102, 901–910. [Google Scholar] [CrossRef] [PubMed]
- Budini, F.; Kemper, D.; Christova, M.; Gallasch, E.; Rafolt, D.; Tilp, M. Five minutes static stretching influences neural responses at spinal level in the background of unchanged corticospinal excitability. J. Musculoskelet. Neuronal Interact. 2019, 19, 30–37. [Google Scholar] [PubMed]
- Pulverenti, T.S.; Trajano, G.S.; Kirk, B.J.C.; Blazevich, A.J. The loss of muscle force production after muscle stretching is not accompanied by altered corticospinal excitability. Eur. J. Appl. Physiol. 2019, 119, 2287–2299. [Google Scholar] [CrossRef]
- Opplert, J.; Paizis, C.; Papitsa, A.; Blazevich, A.J.; Cometti, C.; Babault, N. Static stretch and dynamic muscle activity induce acute similar increase in corticospinal excitability. PLoS ONE 2020, 15, e0230388. [Google Scholar] [CrossRef] [PubMed]
- Pulverenti, T.S.; Trajano, G.S.; Walsh, A.; Kirk, B.J.C.; Blazevich, A.J. Lack of cortical or Ia-afferent spinal pathway involvement in muscle force loss after passive static stretching. J. Neurophysiol. 2020, 123, 1896–1906. [Google Scholar] [CrossRef]
- Coratella, G.; CÈ, E.; Doria, C.; Borrelli, M.; Longo, S.; Esposito, F. Neuromuscular Correlates of the Contralateral Stretch-induced Strength Loss. Med. Sci. Sports Exerc. 2021, 53, 2066–2075. [Google Scholar] [CrossRef]
- Mizuno, T.; Matsumoto, M.; Umemura, Y. Viscoelasticity of the muscle–tendon unit is returned more rapidly than range of motion after stretching. Scand. J. Med. Sci. Sports 2013, 23, 23–30. [Google Scholar] [CrossRef]
- Longo, S.; Cè, E.; Rampichini, S.; Devoto, M.; Limonta, E.; Esposito, F. Mechanomyogram amplitude correlates with human gastrocnemius medialis muscle and tendon stiffness both before and after acute passive stretching. Exp. Physiol. 2014, 99, 1359–1369. [Google Scholar] [CrossRef]
- Cè, E.; Longo, S.; Rampichini, S.; Devoto, M.; Limonta, E.; Venturelli, M.; Esposito, F. Stretch-induced changes in tension generation process and stiffness are not accompanied by alterations in muscle architecture of the middle and distal portions of the two gastrocnemii. J. Electromyogr. Kinesiol. 2015, 25, 469–478. [Google Scholar] [CrossRef]
- Konrad, A.; Stafilidis, S.; Tilp, M. Effects of acute static, ballistic, and PNF stretching exercise on the muscle and tendon tissue properties. Scand. J. Med. Sci. Sports 2017, 27, 1070–1080. [Google Scholar] [CrossRef]
- Longo, S.; Cè, E.; Rampichini, S.; Devoto, M.; Venturelli, M.; Limonta, E.; Esposito, F. Correlation between stiffness and electromechanical delay components during muscle contraction and relaxation before and after static stretching. J. Electromyogr. Kinesiol. 2017, 33, 83–93. [Google Scholar] [CrossRef] [PubMed]
- Konrad, A.; Budini, F.; Tilp, M. Acute effects of constant torque and constant angle stretching on the muscle and tendon tissue properties. Eur. J. Appl. Physiol. 2017, 117, 1649–1656. [Google Scholar] [CrossRef] [PubMed]
- César, E.P.; de Oliveira Teixeira, L.; de Souza, D.V.B.C.; Gomes, P.S.C. Acute effects of passive static stretching on the vastus lateralis muscle architecture of healthy young men. Rev. Bras. Cineantropometria Desempenho Hum. 2017, 19, 585–595. [Google Scholar] [CrossRef]
- Konrad, A.; Reiner, M.M.; Thaller, S.; Tilp, M. The time course of muscle-tendon properties and function responses of a five-minute static stretching exercise. Eur. J. Sport Sci. 2019, 19, 1195–1203. [Google Scholar] [CrossRef]
- Santos, C.X.; Beltrão, N.B.; Pirauá, A.L.T.; Durigan, J.L.Q.; Behm, D.; de Araújo, R.C. Static Stretching Intensity Does Not Influence Acute Range of Motion, Passive Torque, and Muscle Architecture. J. Sport Rehabil. 2020, 29, 1–6. [Google Scholar] [CrossRef]
- Konrad, A.; Tilp, M. The Time Course of Muscle-Tendon Unit Function and Structure Following Three Minutes of Static Stretching. J. Sports Sci. Med. 2020, 19, 52–58. [Google Scholar]
- Borges, M.; Cini, A.; Sonda, F.C.; Souza da Rocha, E.; Felappi, C.J.; Vaz, M.A.; Lima, C.S. Triceps surae muscle-tendon unit mechanical property changes during 10 minutes of streching. J. Bodyw. Mov. Ther. 2021, 27, 591–596. [Google Scholar] [CrossRef]
- Zhu, Y.; Feng, Y.; Huang, F.; Li, Y.; Wang, W.; Wang, X.; Cao, X.; Zhang, Z. Changes in stiffness of the specific regions of knee extensor mechanism after static stretching. Front. Bioeng. Biotechnol. 2022, 10, 958242. [Google Scholar] [CrossRef]
- Ferreira-Valente, M.A.; Pais-Ribeiro, J.L.; Jensen, M.P. Validity of four pain intensity rating scales. PAIN® 2011, 152, 2399–2404. [Google Scholar] [CrossRef]
- Blazevich, A.J.; Kay, A.D.; Waugh, C.; Fath, F.; Miller, S.; Cannavan, D. Plantarflexor stretch training increases reciprocal inhibition measured during voluntary dorsiflexion. J. Neurophysiol. 2012, 107, 250–256. [Google Scholar] [CrossRef]
- Blazevich, A.J.; Cannavan, D.; Waugh, C.M.; Miller, S.C.; Thorlund, J.B.; Aagaard, P.; Kay, A.D. Range of motion, neuromechanical, and architectural adaptations to plantar flexor stretch training in humans. J. Appl. Physiol. 2014, 117, 452–462. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, M.; Ikezoe, T.; Takeno, Y.; Ichihashi, N. Effects of a 4-week static stretch training program on passive stiffness of human gastrocnemius muscle-tendon unit in vivo. Eur. J. Appl. Physiol. 2012, 112, 2749–2755. [Google Scholar] [CrossRef]
- Konrad, A.; Tilp, M. Increased range of motion after static stretching is not due to changes in muscle and tendon structures. Clin. Biomech. 2014, 29, 636–642. [Google Scholar] [CrossRef]
- Freitas, S.R.; Mil-Homens, P. Effect of 8-Week High-Intensity Stretching Training on Biceps Femoris Architecture. J. Strength Cond. Res. 2015, 29, 1737–1740. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, M.; Ikezoe, T.; Umegaki, H.; Kobayashi, T.; Nishishita, S.; Ichihashi, N. Changes in Passive Properties of the Gastrocnemius Muscle–Tendon Unit During a 4-Week Routine Static-Stretching Program. J. Sport Rehabil. 2017, 26, 263–268. [Google Scholar] [CrossRef] [PubMed]
- Mizuno, T. Combined Effects of Static Stretching and Electrical Stimulation on Joint Range of Motion and Muscle Strength. J. Strength Cond. Res. 2019, 33, 2694–2703. [Google Scholar] [CrossRef]
- Beltrão, N.B.; Ximenes Santos, C.; de Oliveira, V.M.A.; Pirauá, A.L.T.; Behm, D.; Pitangui, A.C.R.; de Araújo, R.C. Effects of a 12-Week Chronic Stretch Training Program at Different Intensities on Joint and Muscle Mechanical Responses: A Randomized Clinical Trial. J. Sport Rehabil. 2020, 29, 904–912. [Google Scholar] [CrossRef]
- Nakamura, M.; Sato, S.; Hiraizumi, K.; Kiyono, R.; Fukaya, T.; Nishishita, S. Effects of static stretching programs performed at different volume-equated weekly frequencies on passive properties of muscle–tendon unit. J. Biomech. 2020, 103, 109670. [Google Scholar] [CrossRef]
- Sato, S.; Hiraizumi, K.; Kiyono, R.; Fukaya, T.; Nishishita, S.; Nunes, J.P.; Nakamura, M. The effects of static stretching programs on muscle strength and muscle architecture of the medial gastrocnemius. PLoS ONE 2020, 15, e0235679. [Google Scholar] [CrossRef]
- Yahata, K.; Konrad, A.; Sato, S.; Kiyono, R.; Yoshida, R.; Fukaya, T.; Nunes, J.P.; Nakamura, M. Effects of a high-volume static stretching programme on plantar-flexor muscle strength and architecture. Eur. J. Appl. Physiol. 2021, 121, 1159–1166. [Google Scholar] [CrossRef]
- Longo, S.; Cè, E.; Bisconti, A.V.; Rampichini, S.; Doria, C.; Borrelli, M.; Limonta, E.; Coratella, G.; Esposito, F. The effects of 12 weeks of static stretch training on the functional, mechanical, and architectural characteristics of the triceps surae muscle–tendon complex. Eur. J. Appl. Physiol. 2021, 121, 1743–1758. [Google Scholar] [CrossRef] [PubMed]
- Moltubakk, M.M.; Villars, F.O.; Magulas, M.M.; Magnusson, S.P.; Seynnes, O.R.; Bojsen-MØLler, J. Altered Triceps Surae Muscle–Tendon Unit Properties after 6 Months of Static Stretching. Med. Sci. Sports Exerc. 2021, 53, 1975–1986. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, M.; Yoshida, R.; Sato, S.; Yahata, K.; Murakami, Y.; Kasahara, K.; Fukaya, T.; Takeuchi, K.; Nunes, J.P.; Konrad, A. Comparison Between High- and Low-Intensity Static Stretching Training Program on Active and Passive Properties of Plantar Flexors. Front. Physiol. 2021, 12, 796497. [Google Scholar] [CrossRef] [PubMed]
- Peixinho, C.C.; Silva, G.A.; Brandão, M.C.A.; Menegaldo, L.L.; de Oliveira, L.F. Effect of a 10-Week Stretching Program of the Triceps Surae Muscle Architecture and Tendon Mechanical Properties. J. Sci. Sport Exerc. 2021, 3, 107–114. [Google Scholar] [CrossRef]
- Nakamura, M.; Yoshida, R.; Sato, S.; Yahata, K.; Murakami, Y.; Kasahara, K.; Fukaya, T.; Takeuchi, K.; Nunes, J.P.; Konrad, A. Cross-education effect of 4-week high- or low-intensity static stretching intervention programs on passive properties of plantar flexors. J. Biomech. 2022, 133, 110958. [Google Scholar] [CrossRef]
- Magnusson, S.P.; Simonsen, E.B.; Aagaard, P.; Sørensen, H.; Kjaer, M. A mechanism for altered flexibility in human skeletal muscle. J. Physiol. 1996, 497, 291–298. [Google Scholar] [CrossRef]
- Morse, C.I.; Degens, H.; Seynnes, O.R.; Maganaris, C.N.; Jones, D.A. The acute effect of stretching on the passive stiffness of the human gastrocnemius muscle tendon unit. J. Physiol. 2008, 586, 97–106. [Google Scholar] [CrossRef]
- Mitchell, B.; Bressel, E.; McNair, P.J.; Bressel, M.E. Effect of pelvic, hip, and knee position on ankle joint range of motion. Phys. Ther. Sport 2008, 9, 202–208. [Google Scholar] [CrossRef]
- Andrade, R.J.; Lacourpaille, L.; Freitas, S.R.; McNair, P.J.; Nordez, A. Effects of hip and head position on ankle range of motion, ankle passive torque, and passive gastrocnemius tension. Scand. J. Med. Sci. Sports 2016, 26, 41–47. [Google Scholar] [CrossRef]
- Stecco, C.; Pirri, C.; Fede, C.; Yucesoy, C.A.; De Caro, R.; Stecco, A. Fascial or Muscle Stretching? A Narrative Review. Appl. Sci. 2021, 11, 307. [Google Scholar] [CrossRef]
- Andrade, R.J.; Freitas, S.R.; Hug, F.; Le Sant, G.; Lacourpaille, L.; Gross, R.; McNair, P.; Nordez, A. The potential role of sciatic nerve stiffness in the limitation of maximal ankle range of motion. Sci. Rep. 2018, 8, 14532. [Google Scholar] [CrossRef] [PubMed]
- Wilke, J.; Macchi, V.; De Caro, R.; Stecco, C. Fascia thickness, aging and flexibility: Is there an association? J. Anat. 2019, 234, 43–49. [Google Scholar] [CrossRef]
- Nordez, A.; Gross, R.; Andrade, R.; Le Sant, G.; Freitas, S.; Ellis, R.; McNair, P.J.; Hug, F. Non-Muscular Structures Can Limit the Maximal Joint Range of Motion during Stretching. Sports Med. 2017, 47, 1925–1929. [Google Scholar] [CrossRef] [PubMed]
- Tesarz, J.; Hoheisel, U.; Wiedenhöfer, B.; Mense, S. Sensory innervation of the thoracolumbar fascia in rats and humans. Neuroscience 2011, 194, 302–308. [Google Scholar] [CrossRef]
- Fede, C.; Petrelli, L.; Pirri, C.; Neuhuber, W.; Tiengo, C.; Biz, C.; De Caro, R.; Schleip, R.; Stecco, C. Innervation of human superficial fascia. Front. Neuroanat. 2022, 16, 981426. [Google Scholar] [CrossRef]
- Trajano, G.S.; Nosaka, K.; Blazevich, A.J. Neurophysiological Mechanisms Underpinning Stretch-Induced Force Loss. Sports Med. 2017, 47, 1531–1541. [Google Scholar] [CrossRef] [PubMed]
- Fowles, J.R.; Sale, D.G.; MacDougall, J.D. Reduced strength after passive stretch of the human plantarflexors. J. Appl. Physiol. 2000, 89, 1179–1188. [Google Scholar] [CrossRef]
- Cramer, J.T.; Beck, T.W.; Housh, T.J.; Massey, L.L.; Marek, S.M.; Danglemeier, S.; Purkayastha, S.; Culbertson, J.Y.; Fitz, K.A.; Egan, A.D. Acute effects of static stretching on characteristics of the isokinetic angle–torque relationship, surface electromyography, and mechanomyography. J. Sports Sci. 2007, 25, 687–698. [Google Scholar] [CrossRef]
- Nakamura, M.; Ikezoe, T.; Takeno, Y.; Ichihashi, N. Acute and prolonged effect of static stretching on the passive stiffness of the human gastrocnemius muscle tendon unit in vivo. J. Orthop. Res. 2011, 29, 1759–1763. [Google Scholar] [CrossRef]
- Huijing, P.A. Epimuscular myofascial force transmission: A historical review and implications for new research. International society of biomechanics Muybridge award lecture, Taipei, 2007. J. Biomech. 2009, 42, 9–21. [Google Scholar] [CrossRef]
- Yucesoy, C.A. Epimuscular Myofascial Force Transmission Implies Novel Principles for Muscular Mechanics. Exerc. Sport Sci. Rev. 2010, 38, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Maas, H.; Sandercock, T.G. Force Transmission between Synergistic Skeletal Muscles through Connective Tissue Linkages. J. Biomed. Biotechnol. 2010, 2010, 575672. [Google Scholar] [CrossRef] [PubMed]
- Behm, D.G.; Button, D.C.; Butt, J.C. Factors Affecting Force Loss With Prolonged Stretching. Can. J. Appl. Physiol. 2001, 26, 262–272. [Google Scholar] [CrossRef]
- Trajano, G.S.; Nosaka, K.; Seitz, L.B.; Blazevich, A.J. Intermittent Stretch Reduces Force and Central Drive more than Continuous Stretch. Med. Sci. Sports Exerc. 2014, 46, 902–910. [Google Scholar] [CrossRef] [PubMed]
- Veldman, M.P.; Maffiuletti, N.A.; Hallett, M.; Zijdewind, I.; Hortobágyi, T. Direct and crossed effects of somatosensory stimulation on neuronal excitability and motor performance in humans. Neurosci. Biobehav. Rev. 2014, 47, 22–35. [Google Scholar] [CrossRef]
- Mazzo, M.R.; Weinman, L.E.; Giustino, V.; McLagan, B.; Maldonado, J.; Enoka, R.M. Changes in neural drive to calf muscles during steady submaximal contractions after repeated static stretches. J. Physiol. 2021, 599, 4321–4336. [Google Scholar] [CrossRef]
Figure 1.
The systematic process for including studies relevant to the scope of this review.

Figure 2.
Forest plots of the effect sizes and 95% confidence intervals of acute static stretching-induced changes in range of motion (A), passive resistance torque (B), maximum tolerable passive resistance torque (C), maximum voluntary isometric torque (D), and muscle–tendon unit stiffness (E). Note that the red diamond marker indicates a significant overall effect size. Abbreviations: ankle (A); knee (K); low-intensity (LI); high-intensity (HI); constant angle (CA); constant torque (CT) [32,34,35,36,37,38,40,41,42,43,44,56,57,58,59,60,61,62,65,66,67,68,69].
Figure 2.
Forest plots of the effect sizes and 95% confidence intervals of acute static stretching-induced changes in range of motion (A), passive resistance torque (B), maximum tolerable passive resistance torque (C), maximum voluntary isometric torque (D), and muscle–tendon unit stiffness (E). Note that the red diamond marker indicates a significant overall effect size. Abbreviations: ankle (A); knee (K); low-intensity (LI); high-intensity (HI); constant angle (CA); constant torque (CT) [32,34,35,36,37,38,40,41,42,43,44,56,57,58,59,60,61,62,65,66,67,68,69].


Figure 3.
Forest plots of the effect sizes and 95% confidence intervals of acute static stretching-induced changes in motor evoked potential amplitude (A), H-reflex amplitude (B), and maximum M-wave amplitude (C). Abbreviations: soleus (SOL); medial gastrocnemius (MG); lateral gastrocnemius (LG) [52,54,55,56,57].
Figure 3.
Forest plots of the effect sizes and 95% confidence intervals of acute static stretching-induced changes in motor evoked potential amplitude (A), H-reflex amplitude (B), and maximum M-wave amplitude (C). Abbreviations: soleus (SOL); medial gastrocnemius (MG); lateral gastrocnemius (LG) [52,54,55,56,57].

Figure 4.
Forest plots of the effect sizes and 95% confidence intervals of acute static stretching-induced changes in fascicle length (A), pennation angle (B), muscle stiffness (C), tendon stiffness (D), and shear elastic modulus (E). Note that the red diamond marker indicates a significant overall effect size. Abbreviations: low-intensity (LI); high-intensity (HI); constant angle (CA); constant torque (CT); middle/distal/central region of muscle (m/l/c); soleus (SOL); medial gastrocnemius (MG); lateral gastrocnemius (LG); rectus femoris (RF); vastus medialis (VM); vastus lateralis (VL); semitendinosus (ST); semimembranosus (SM); biceps femoris (BF) [32,33,34,35,36,37,38,39,40,41,42,43,44,58,59,60,61,62,64,65,66,67,68,69].
Figure 4.
Forest plots of the effect sizes and 95% confidence intervals of acute static stretching-induced changes in fascicle length (A), pennation angle (B), muscle stiffness (C), tendon stiffness (D), and shear elastic modulus (E). Note that the red diamond marker indicates a significant overall effect size. Abbreviations: low-intensity (LI); high-intensity (HI); constant angle (CA); constant torque (CT); middle/distal/central region of muscle (m/l/c); soleus (SOL); medial gastrocnemius (MG); lateral gastrocnemius (LG); rectus femoris (RF); vastus medialis (VM); vastus lateralis (VL); semitendinosus (ST); semimembranosus (SM); biceps femoris (BF) [32,33,34,35,36,37,38,39,40,41,42,43,44,58,59,60,61,62,64,65,66,67,68,69].


Figure 5.
Forest plots of the effect sizes and 95% confidence intervals of chronic static stretching-induced changes in range of motion (A), passive resistance torque (B), maximum tolerable passive resistance torque (C), maximum voluntary isometric torque (D), and muscle–tendon unit stiffness (E). Note that the red diamond marker indicates a significant overall effect size. Abbreviations: ankle (A); knee (K); muscle-directed (MD); hip-neutral (HN); low-intensity (LI); high-intensity (HI); constant angle (CA); constant torque (CT) [45,47,71,72,74,75,76,77,78,79,80,81,82,83,84,85,86].
Figure 5.
Forest plots of the effect sizes and 95% confidence intervals of chronic static stretching-induced changes in range of motion (A), passive resistance torque (B), maximum tolerable passive resistance torque (C), maximum voluntary isometric torque (D), and muscle–tendon unit stiffness (E). Note that the red diamond marker indicates a significant overall effect size. Abbreviations: ankle (A); knee (K); muscle-directed (MD); hip-neutral (HN); low-intensity (LI); high-intensity (HI); constant angle (CA); constant torque (CT) [45,47,71,72,74,75,76,77,78,79,80,81,82,83,84,85,86].


Figure 6.
Forest plots of the effect sizes and 95% confidence intervals of chronic static stretching-induced changes in fascicle length (A), pennation angle (B), muscle thickness (C), muscle stiffness (D), tendon stiffness (E), and shear elastic modulus or shear wave speed (F). Note that the red diamond markers indicate a significant overall effect size. Abbreviations: low-intensity (LI); high-intensity (HI); muscle-directed (MD); hip-neutral (HN); low-intensity group (GLow); high-intensity group (GHigh); soleus (SOL); proximal region of SOL (SOLp); distal region of SOL (SOLd); medial gastrocnemius (MG); proximal region of MG (MGp); intermediate region of MG (MGi); distal region of MG (MGd); lateral gastrocnemius (LG); proximal region of LG (LGp); intermediate region of LG (LGi); distal region of LG (LGd); Achilles tendon tangent modulus considering the middle (ATm) and end (ATe) third parts of curves; whole Achilles tendon stiffness (ATw); free Achilles tendon stiffness (ATf); semitendinosus (ST); semimembranosus (SM); biceps femoris (BF) [45,46,47,72,74,75,76,77,78,79,80,81,82,83,84,85,86].
Figure 6.
Forest plots of the effect sizes and 95% confidence intervals of chronic static stretching-induced changes in fascicle length (A), pennation angle (B), muscle thickness (C), muscle stiffness (D), tendon stiffness (E), and shear elastic modulus or shear wave speed (F). Note that the red diamond markers indicate a significant overall effect size. Abbreviations: low-intensity (LI); high-intensity (HI); muscle-directed (MD); hip-neutral (HN); low-intensity group (GLow); high-intensity group (GHigh); soleus (SOL); proximal region of SOL (SOLp); distal region of SOL (SOLd); medial gastrocnemius (MG); proximal region of MG (MGp); intermediate region of MG (MGi); distal region of MG (MGd); lateral gastrocnemius (LG); proximal region of LG (LGp); intermediate region of LG (LGi); distal region of LG (LGd); Achilles tendon tangent modulus considering the middle (ATm) and end (ATe) third parts of curves; whole Achilles tendon stiffness (ATw); free Achilles tendon stiffness (ATf); semitendinosus (ST); semimembranosus (SM); biceps femoris (BF) [45,46,47,72,74,75,76,77,78,79,80,81,82,83,84,85,86].



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Summary of acute effects of static stretching.
| Study | Stretch Protocol | Target Joint/Muscle (n) | Test Muscle | Static Stretching Effect | ||
|---|---|---|---|---|---|---|
| Joint/ Functional | Neural | Muscular | ||||
| Budini et al. [52] | 60 s (2 × 30 s), maximum dorsiflexion | Ankle/Plantar flexors (19) | SOL | N/A | MEP ↔, H ↑, T ↓ | N/A |
| Budini et al. [53] | 300 s (5 × 60 s), 0-s interval, maximum dorsiflexion | Ankle/Plantar flexors (17) | SOL | N/A | MEP ↔, H/M ↑, T ↓ | N/A |
| Pulverenti et al. [54] | 300 s (5 × 60 s), 15-s interval, two protocols (A and B), constant torque 1 | Ankle/Plantar flexors (14) | SOL | ROM ↓, MVIT ↓ | MEP/Mmax ↔, Mmax ↔, EMG/Mmax ↓ | N/A |
| MG | Mmax ↔, EMG/Mmax ↓ (Protocol B) | |||||
| Opplert et al. [55] | 100 s (5 × 20 s), 20-s interval, maximum dorsiflexion | Ankle/Plantar flexors (15) | SOL | N/A | MEP ↑, MEP/Mmax ↑, Hmax ↔, Hmax/Mmax ↔, Mmax ↔, EMG/Mmax ↔ | N/A |
| MG | MEP ↔, MEP/Mmax ↔, Hmax ↔, Hmax/Mmax ↔, Mmax ↔, EMG/Mmax ↔ | |||||
| LG | MEP ↑, MEP/Mmax ↑, Hmax ↔, Hmax/Mmax ↔, Mmax ↔, EMG/Mmax ↔ | |||||
| Pulverenti et al. [56] | 300 s (5 × 60 s), 15-s interval, constant torque 1 | Ankle/Plantar flexors (15) | SOL | ROM ↑, MVIT ↓ | MEP/Mmax ↔, H/Mmax ↔, Mmax ↔, EMG/Mmax ↓ | N/A |
| MG | Mmax ↔, EMG/Mmax ↓ | |||||
| Coratella et al. [57] | 225 s (5 × 45 s), 15-s interval, constant torque 2 | Ankle/Plantar flexors (26) | SOL | ROM ↑, MVIT ↓ | Hmax ↔, Hsup ↔, Mmax ↔, Msup ↔, EMG/Msup ↓ | N/A |
| MG | Hmax ↔, Hsup ↔, Mmax ↔, Msup ↔, EMG/Msup ↓ | |||||
| LG | Hmax ↔, Hsup ↔, Mmax ↔, Msup ↔, EMG/Msup ↓ | |||||
| Mizuno et al. [58] | 300 s (5 × 60 s), maximum dorsiflexion | Ankle/Plantar flexors (11) | MG | ROM ↑, PRT ↓, PRTmax ↑, MTU stiffness ↓ | N/A | MTJ displacement ↔, Tendon displacement ↔, Muscle stiffness ↓, Tendon stiffness ↔ |
| Akagi and Takahashi [32] | 360 s (3 × 120 s), 60-s interval, maximum dorsiflexion | Ankle/Plantar flexors (20) | MG | ROM ↑, MVIT ↔, MTU stiffness ↓ | N/A | Shear elastic modulus ↓ |
| LG | Shear elastic modulus ↓ | |||||
| Longo et al. [59] | 270 s (6 × 45 s), 15-s interval, maximum dorsiflexion | Ankle/Plantar flexors (21) | MG | ROM ↑, PRT ↓, PRTmax ↑, MVIT ↓, MTU stiffness ↓ | EMG ↓ | Muscle stiffness ↓, Tendon stiffness ↓ |
| Nakamura et al. [33] | 120 s (4 × 30 s), maximum dorsiflexion | Ankle/Plantar flexors (17) | MG | N/A | N/A | Muscle stiffness ↓, Shear elastic modulus ↓ |
| Taniguchi et al. [34] | 300 s (5 × 60 s), 20-s interval, maximum dorsiflexion | Ankle/Plantar flexors (10) | MG | ROM ↑ | N/A | Pennation angle ↔, Shear elastic modulus ↓ |
| LG | Pennation angle ↔, Shear elastic modulus ↓ | |||||
| Umegaki et al. [35] | 300 s (5 × 60 s), 30-s interval, maximum dorsiflexion | Knee/Flexors (20) | BF | ROM ↑, PRT ↓ | N/A | Shear elastic modulus ↓ |
| ST | Shear elastic modulus ↓ | |||||
| SM | Shear elastic modulus ↓ | |||||
| Cè et al. [60] | 270 s (6 × 45 s), 15-s interval, maximum dorsiflexion | Ankle/Plantar flexors (14) | MG | ROM ↑, PRT ↓, PRTmax ↑, MVIT ↓, MTU stiffness ↓ | N/A | Fascicle length ↔, Pennation angle ↔, Muscle stiffness ↓, Tendon stiffness ↓ |
| LG | Fascicle length ↔, Pennation angle ↔ | |||||
| Hirata et al. [36] | 300 s, maximum dorsiflexion | Ankle/Plantar flexors (12) | SOL | ROM ↑, PRT ↓ | N/A | Shear modulus ↔ |
| MG | Shear modulus ↓ | |||||
| LG | Shear modulus ↔ | |||||
| Konrad et al. [61] | 30 s, maximum dorsiflexion | Ankle/Plantar flexors (25) | MG | ROM ↑, PRT ↓, MVIT ↔, MTU stiffness ↓ | N/A | Fascicle length ↔, Pennation angle ↔, Muscle stiffness ↓, Tendon stiffness ↔ |
| Hirata et al. [37] | 300 s, maximum dorsiflexion | Ankle/Plantar flexors (14) | MG | ROM ↑, PRT ↓, PRTmax ↔ | N/A | Fascicle length ↔, Shear modulus ↓ |
| Longo et al. [62] | 270 s (6 × 45 s), 15-s interval, maximum dorsiflexion | Ankle/Plantar flexors (18) | MG | PRT ↓, MVIT ↓, MTU stiffness ↓, EMD ↑ | N/A | Muscle stiffness ↓, Tendon stiffness ↓ |
| Konrad et al. [63] | 120 s (4 × 30 s), 20-s interval, constant angle/torque 3 | Ankle/Plantar flexors (17) | MG | ROM ↑, PRT ↓, MVIT ↔, MTU stiffness ↓ | N/A | Muscle stiffness ↓, Tendon stiffness ↔ |
| Nakamura et al. [38] | 300 s, maximum dorsiflexion | Ankle/Plantar flexors (15) | MG | ROM ↑ | N/A | Shear modulus ↓ |
| LG | Shear modulus ↓ | |||||
| César et al. [64] | 30 s, maximum knee flexion | Knee/Extensors (12) | VL | N/A | N/A | Fascicle length ↑, Pennation angle ↓ |
| Konrad et al. [65] | 300 s (5 × 60 s), 20-s interval, maximum dorsiflexion | Ankle/Plantar flexors (14) | MG | ROM ↑, PRT ↓, MVIT ↓, MTU stiffness ↓ | N/A | Muscle elongation ↑, Tendon elongation ↔, Muscle stiffness ↓, Tendon stiffness ↔ |
| Nojiri et al. [39] | 120 s (4 × 30 s), 0-/30-s interval, maximum dorsiflexion | Ankle/Plantar flexors (15) | MG | N/A | N/A | Shear modulus ↓ |
| Zhou et al. [40] | 300 s, maximum dorsiflexion | Ankle/Plantar flexors (30) | MG | ROM ↑ | N/A | Fascicle length ↔, Shear modulus ↓ |
| LG | Fascicle length ↔, Shear modulus ↓ | |||||
| Santos et al. [66] | 180 s (3 × 60 s), 30-s interval, low intensity 4 | Knee/Flexors (10) | BF | ROM ↑, MTU stiffness ↔ | N/A | Fascicle length ↔, Pennation angle ↔ |
| 180 s (3 × 60 s), 30-s interval, high intensity 4 | Knee/Flexors (10) | BF | ROM ↑, MTU stiffness ↔ | N/A | Fascicle length ↔, Pennation angle ↔ | |
| Nakamura et al. [41] | 300 s (10 × 30 s), 10-/30-/90-s interval, maximum dorsiflexion | Ankle/Plantar flexors (16) | MG | ROM ↑, PRTmax ↑ | N/A | Shear modulus ↓ |
| Hirata et al. [42] | 450 s (5 × 90 s), 0-s interval, maximum dorsiflexion | Ankle/Plantar flexors (20) | SOL | ROM ↑, PRT ↓ | N/A | Shear modulus ↔ |
| MG | Shear modulus ↓ | |||||
| LG | Shear modulus ↓ | |||||
| Konrad and Tilp [67] | 180 s (3 × 60 s), 20-s interval, maximum dorsiflexion | Ankle/Plantar flexors (14) | MG | ROM ↑, PRT ↓, MVIT ↔, MTU stiffness ↓ | N/A | Muscle stiffness ↓, Tendon stiffness ↔, Active tendon stiffness ↔ |
| Nakamura et al. [43] | 180 s (3 × 60 s), 30-s interval, 120%/100%/80% intensity 5 | Knee/Extensors (18) | RF | ROM ↑ (120% and 100%) | N/A | Shear modulus ↓ (100%) |
| VM | Shear modulus ↔ | |||||
| VL | Shear modulus ↔ | |||||
| Borges et al. [68] | 600 s, maximum dorsiflexion | Ankle/Plantar flexors (13) | MG | ROM ↑, PRT ↓, MTU stiffness ↓ | N/A | MTJ displacement ↔ Muscle stiffness ↔ Tendon stiffness ↔ |
| Nakamura et al. [44] | 600 s, maximum dorsiflexion | Ankle/Plantar flexors (16) | MG | MVIT ↓, RFD ↓ | N/A | Shear modulus ↓ |
| Zhu et al. [69] | 180 s (3 × 60 s), 30-s interval, maximum knee flexion | Knee/Extensors (30) | RF | ROM ↑ | N/A | Muscle stiffness ↓ |
| VM | Muscle stiffness ↔ | |||||
| VL | Muscle stiffness ↔ | |||||
1 85–90% of maximal tolerable stretch torque; 2 90% of maximal tolerable stretch torque; 3 constant angle (dorsiflexion corresponding to 95% of maximum dorsiflexion) and constant torque (passive resistance torque corresponding to 95% of maximum dorsiflexion); 4 based on the numerical rating scale [70], low (between 1 and 2) and high (between 9 and 10); 5 based on the knee flexion range of motion (ROM) in the pre-intervention, 120% (1.2 times of the ROM). ↑: significant increase (p < 0.05); ↓: significant decrease (p < 0.05); ↔: non-significant change (p > 0.05). Stretching effects in boldface indicate significant change. SOL: soleus; MG: medial gastrocnemius; LG: lateral gastrocnemius; BF: biceps femoris; ST: semitendinosus; SM: semimembranosus; RF: rectus femoris; VM: vastus medialis; VL: vastus lateralis; ROM: range of motion; PRT: passive resistance torque; PRTmax: maximum tolerable passive resistance torque; MVIT: maximum voluntary isometric torque; MTU: muscle–tendon unit; VA: voluntary activation; EMD: electromechanical delay; RFD: rate of force development; MEP: motor evoked potential amplitude; H: H-reflex amplitude; Hmax: maximum H-reflex amplitude; Hsup: superimposed H-reflex amplitude; T: tendon reflex amplitude; M: M-wave amplitude; Mmax: maximum M-wave amplitude; Msup: superimposed M-wave amplitude; EMG: electromyography amplitude; MTJ: muscle–tendon junction.
Table 2.
Summary of chronic effects of static stretching.
| Study | Stretch Protocol | Target Joint/Muscle (n) | Test Muscle | Static Stretching Effect | ||
|---|---|---|---|---|---|---|
| Joint/ Functional | Neural | Muscular | ||||
| Blazevich et al. [71] | 120 s (4 × 30 s), 15-s interval, twice a day, maximum dorsiflexion, 44 sessions over 4 weeks (average sessions = 40) | Ankle/Plantar flexors (11) | SOL | ROM ↑, PRT ↔, MVIT ↔ | Hmax/Mmax ↓ (plantarflexed and neutral at 2% MVIT, all positions at 20% MVIT) | N/A |
| MG | Hmax/Mmax ↓ (plantarflexed at 2% MVIT, dorsiflexed at 20% MVIT) | |||||
| Blazevich et al. [72] | 120 s (4 × 30 s), 15-s interval, maximum dorsiflexion, 42 sessions over 3 weeks (average sessions = 41) | Ankle/Plantar flexors (12) | SOL | ROM ↑, PRT ↔, PRTmax ↑, MVIT ↔, MTU stiffness ↔ | Hmax/Mmax ↓ | N/A |
| MG | Hmax/Mmax ↓ | Fascicle length ↔, Muscle/fascicle strain ↑, Fascicle rotation ↔, Tendon elongation ↔, Muscle stiffness ↓, Tendon stiffness ↔ | ||||
| Nakamura et al. [73] | 120 s (2 × 60 s), maximum dorsiflexion, 28 sessions over 4 weeks | Ankle/Plantar flexors (9) | MG | ROM ↑, PRT ↓ | N/A | Fascicle length ↔, Fascicle rotation ↔, MTJ displacement ↑ |
| Akagi and Takahashi [45] | 360 s (3 × 120 s), 60-s interval, maximum dorsiflexion, 30 sessions over 5 weeks | Ankle/Plantar flexors (19) | MG | ROM ↑, MVIT ↔, MTU stiffness ↔ | N/A | Shear modulus ↓ |
| LG | Shear modulus ↓ | |||||
| Konrad and Tilp [74] | 120 s (4 × 30 s), 0-s interval, maximum dorsiflexion, 30 sessions over 6 weeks | Ankle/Plantar flexors (15) | MG | ROM ↑, PRT ↔, MVIT ↔, MTU stiffness ↔ | N/A | Fascicle length ↔, Pennation angle ↔, Muscle stiffness ↔, Tendon stiffness ↔ |
| Freitas and Mil-Homens [75] | 450 s, 0-s interval, maximum knee extension (adjusted every 90 s), 40 sessions over 8 weeks (average sessions = 25) | Knee/Flexors (5) | BF | ROM ↑ | N/A | Fascicle length ↑, Pennation angle ↔, Muscle thickness ↔ |
| Ichihashi et al. [46] | 300 s, maximum knee extension, 12 sessions over 4 weeks | Knee/Flexors (15) | ST | N/A | N/A | Shear modulus ↓ |
| SM | Shear modulus ↓ | |||||
| BF | Shear modulus ↓ | |||||
| Nakamura et al. [76] | 120 s (4 × 30 s), maximum dorsiflexion, 12 sessions over 4 weeks | Ankle/Plantar flexors (12) | MG | ROM ↑, PRTmax ↑ | N/A | Muscle stiffness ↓ |
| Mizuno [77] | 120 s (4 × 30 s), 30-s interval, maximum dorsiflexion, 24 sessions over 8 weeks | Ankle/Plantar flexors (11) | MG | ROM ↑, 1RM ↔ | N/A | Pennation angle ↔, Muscle thickness ↑ |
| Beltrão et al. [78] | 180 s (3 × 60 s), 30-s interval, low constant torque 1, 36 sessions over 12 weeks | Knee/Flexors (7) | BF | ROM ↑, PRT ↔, PRTmax ↔, MTU stiffness ↔ | N/A | Fascicle length ↔, Pennation angle ↔ |
| 180 s (3 × 60 s), 30-s interval, high constant torque 1, 36 sessions over 12 weeks | Knee/Flexors (8) | |||||
| Nakamura et al. [79] | 360 s, maximum dorsiflexion, 6 sessions over 6 weeks | Ankle/Plantar flexors (12) | MG | ROM ↔ | N/A | Muscle stiffness ↔ |
| 120 s, maximum dorsiflexion, 18 sessions over 6 weeks | Ankle/Plantar flexors (12) | ROM ↑ | N/A | Muscle stiffness ↓ | ||
| Sato et al. [80] | 360 s, maximum dorsiflexion, 6 sessions over 6 weeks | Ankle/Plantar flexors (12) | MG | MVIT ↔ | N/A | Pennation angle ↔, Muscle thickness ↔ |
| 120 s, maximum dorsiflexion, 18 sessions over 6 weeks | Ankle/Plantar flexors (12) | |||||
| Andrade et al. [47] | 450 s (5 × 45 s × 2 maneuvers), <5-s interval, maximum dorsiflexion, 60 sessions over 12 weeks | Ankle/Plantar flexors (21) | SOL | ROM↑ (HN), PRT↓ (HN) | RMS EMG ↔ | Shear wave speed (p) ↔, Shear wave speed (d) ↓ |
| MG | RMS EMG ↔ | Fascicle length ↑, Muscle thickness ↔, Shear wave speed (p/i/d) ↓ | ||||
| LG | N/A | Fascicle length ↔, Muscle thickness ↔, Shear wave speed (p/i/d) ↓ | ||||
| Nerve shear wave speed | Sciatic (p/d) ↔, Tibial (p) ↔ | |||||
| Yahata et al. [81] | 1800 s (6 × 300 s), 60-s interval, maximum dorsiflexion, 30 sessions over 5 weeks | Ankle/Plantar flexors (16) | SOL | MVIT ↑, RFD ↔ | N/A | Muscle thickness ↔ |
| MG | Fascicle length ↔, Pennation angle ↔, Muscle thickness ↔ | |||||
| LG | Fascicle length ↔, Pennation angle ↔, Muscle thickness ↔ | |||||
| Longo et al. [82] | 450 s (5 × 45 s × 2 maneuvers), 15-s interval, maximum dorsiflexion, 60 sessions over 12 weeks (average sessions = 54) | Ankle/Plantar flexors (15) | SOL | ROM ↑, PRTmax ↑, MVIT ↔, MTU stiffness ↓, RTD ↔, EMD ↔ | RMS EMG ↔ | Fascicle length (m/d) ↔, Pennation angle (m/d) ↔, Muscle thickness (m) ↔ |
| MG | RMS EMG ↔ | Fascicle length (m/d) ↔, Pennation angle (m/d) ↔, Muscle thickness (m) ↔, MTJ displacement ↑, Muscle stiffness ↓ | ||||
| LG | RMS EMG ↔ | Fascicle length (m/d) ↔, Pennation angle (m/d) ↔, Muscle thickness (m) ↔ | ||||
| Moltubakk et al. [83] | 240 s (4 × 60 s) for the first eight weeks, 240 s (2 × 60 s × 2 maneuvers) for the remaining weeks, maximum dorsiflexion, 168 sessions over 24 weeks (average sessions = 150) | Ankle/Plantar flexors (25 for passive dorsiflexion, 24 for passive ultrasound, 21 and 23 for free and whole Achilles tendon stiffness, respectively, and 19 for isometric strength measurements) | SOL | ROM ↑, PRT ↓, PRTmax ↑, MVIT ↔ | N/A | Muscle elongation ↔, Free Achilles tendon stiffness↔ |
| MG | Fascicle length ↔, Pennation angle ↑, Muscle thickness ↑, Muscle elongation ↔, Fascicle rotation ↔, Whole Achilles tendon elongation ↔, Whole Achilles tendon stiffness ↔ | |||||
| Nakamura et al. [84] | 180 s (3 × 60 s), 30-s interval, low constant torque 2, 12 sessions over 4 weeks | Ankle/Plantar flexors (13) | SOL | ROM ↑, PRTmax ↔, MVIT ↔ | N/A | Muscle thickness ↔ |
| MG | Fascicle length ↔, Pennation angle ↔, Muscle thickness ↔, Muscle stiffness ↓ | |||||
| LG | Fascicle length ↔, Pennation angle ↔, Muscle thickness ↔ | |||||
| 180 s (3 × 60 s), 30-s interval, high constant torque 2, 12 sessions over 4 weeks | Ankle/Plantar flexors (14) | SOL | ROM ↑, PRTmax ↑, MVIT ↔ | N/A | Muscle thickness ↔ | |
| MG | Fascicle length ↔, Pennation angle ↔, Muscle thickness ↔, Muscle stiffness ↓ | |||||
| LG | Fascicle length ↔, Pennation angle ↔, Muscle thickness ↔ | |||||
| Peixinho et al. [85] | 120 s (2 × 30 s × 2 maneuvers), 0-s interval, maximum dorsiflexion, approximately 45 sessions over 10 weeks | Ankle/Plantar flexors (12) | MG | ROM ↑, PRTmax ↑ | N/A | Fascicle length ↔, Pennation angle ↔, Tendon tangent modulus ↔ (middle and end parts of the stress–strain curve), Tendon tension ↔, Tendon deformation ↔ |
| Nakamura et al. [86] | 180 s (3 × 60 s), 30-s interval, low constant torque 2, 12 sessions over 4 weeks | Ankle/Plantar flexors (14) | SOL | ROM ↔, PRTmax ↔ | N/A | Muscle thickness ↔ |
| MG | Fascicle length ↔, Pennation angle ↔, Muscle thickness ↔, Muscle stiffness ↔ | |||||
| LG | Fascicle length ↔, Pennation angle ↔, Muscle thickness ↔ | |||||
| 180 s (3 × 60 s), 30-s interval, high constant torque 2, 12 sessions over 4 weeks | Ankle/Plantar flexors (14) | SOL | ROM ↑, PRTmax ↑ | N/A | Muscle thickness ↔ | |
| MG | Fascicle length ↔, Pennation angle ↔ Muscle thickness ↔ Muscle stiffness ↔ | |||||
| LG | Fascicle length ↔ Pennation angle ↔ Muscle thickness ↔ | |||||
1 based on the verbal numerical scale [70], low (between 1 and 2) and high (between 9 and 10); 2 based on the verbal numerical scale [70], low (between 0 and 1) and high (between 6 and 7). ↑: significant increase (p < 0.05); ↓: significant decrease (p < 0.05); ↔: non-significant change (p > 0.05). Stretching effects in boldface indicate significant change. p/i/m/d: proximal/intermediate/middle/distal region of muscle; SOL: soleus; MG: medial gastrocnemius; LG: lateral gastrocnemius; BF: biceps femoris; ST: semitendinosus; SM: semimembranosus; RF: rectus femoris; VM: vastus medialis; VL: vastus lateralis; ROM: range of motion; PRT: passive resistance torque; PRTmax: maximum tolerable passive resistance torque; MVIT: maximum voluntary isometric torque; MTU: muscle–tendon unit; VA: voluntary activation; EMD: electromechanical delay; RFD: rate of force development; MEP: motor evoked potential amplitude; H: H-reflex amplitude; Hmax: maximum H-reflex amplitude; Hsup: superimposed H-reflex amplitude; T: tendon reflex amplitude; M: M-wave amplitude; Mmax: maximum M-wave amplitude; Msup: superimposed M-wave amplitude; RMS EMG: root square mean electromyogram amplitude; MTJ: muscle–tendon junction.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Shah, R.; Samuel, M.W.; Son, J. Acute and Chronic Effects of Static Stretching on Neuromuscular Properties: A Meta-Analytical Review. Appl. Sci. 2023, 13, 11979. https://0-doi-org.brum.beds.ac.uk/10.3390/app132111979
AMA Style
Shah R, Samuel MW, Son J. Acute and Chronic Effects of Static Stretching on Neuromuscular Properties: A Meta-Analytical Review. Applied Sciences. 2023; 13(21):11979. https://0-doi-org.brum.beds.ac.uk/10.3390/app132111979
Chicago/Turabian StyleShah, Ruchi, Marina W. Samuel, and Jongsang Son. 2023. "Acute and Chronic Effects of Static Stretching on Neuromuscular Properties: A Meta-Analytical Review" Applied Sciences 13, no. 21: 11979. https://0-doi-org.brum.beds.ac.uk/10.3390/app132111979
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.