
Uptake of COVID-19 Vaccines among Pregnant Women: A Systematic Review and Meta-Analysis

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Strategy
2.2. Selection and Eligibility Criteria
2.3. Data Extraction and Risk of Bias Assessment
2.4. Statistical Analysis
3. Results
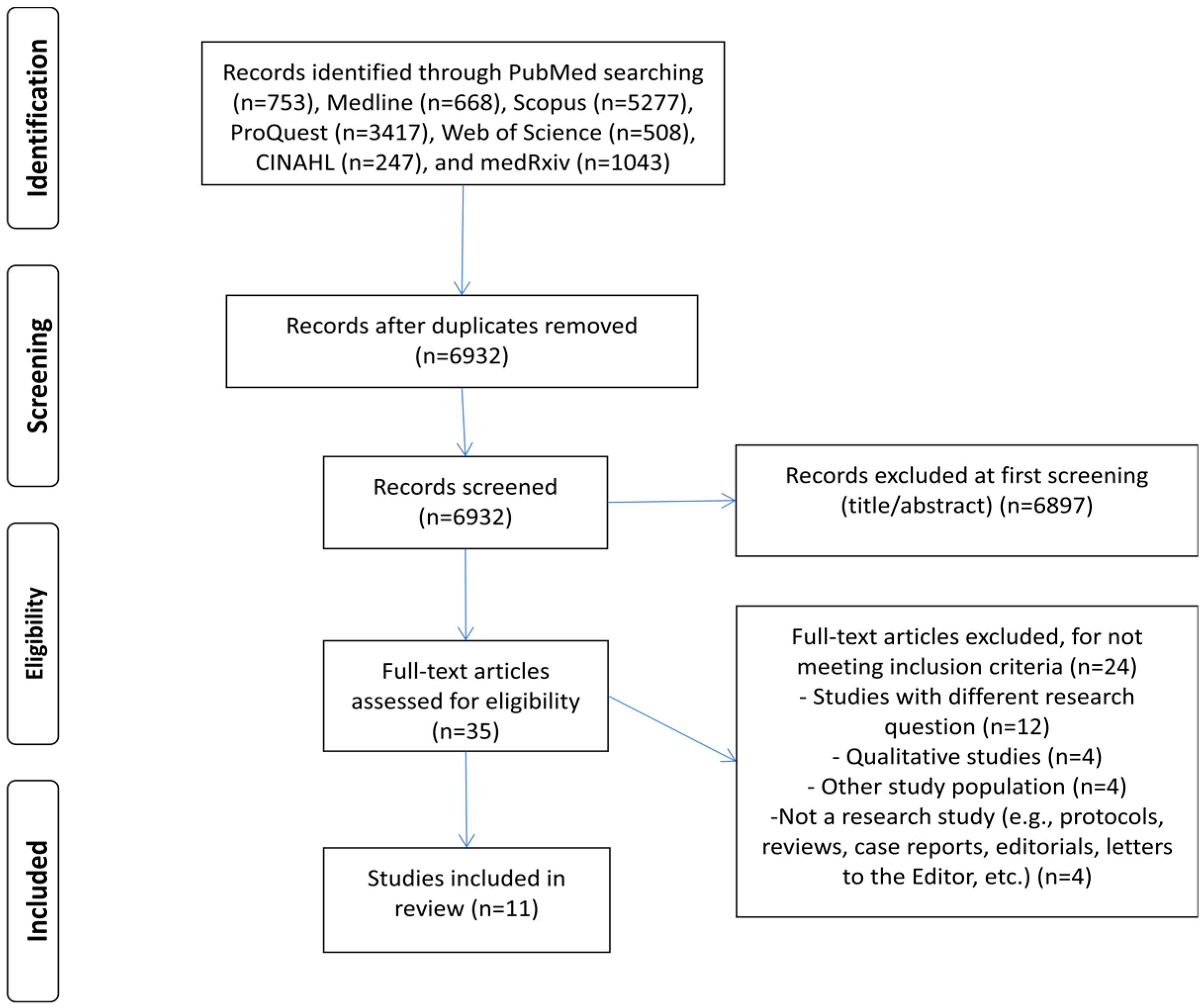
3.1. Identification and Selection of Studies
3.2. Characteristics of the Studies
3.3. Risk of Bias Assessment
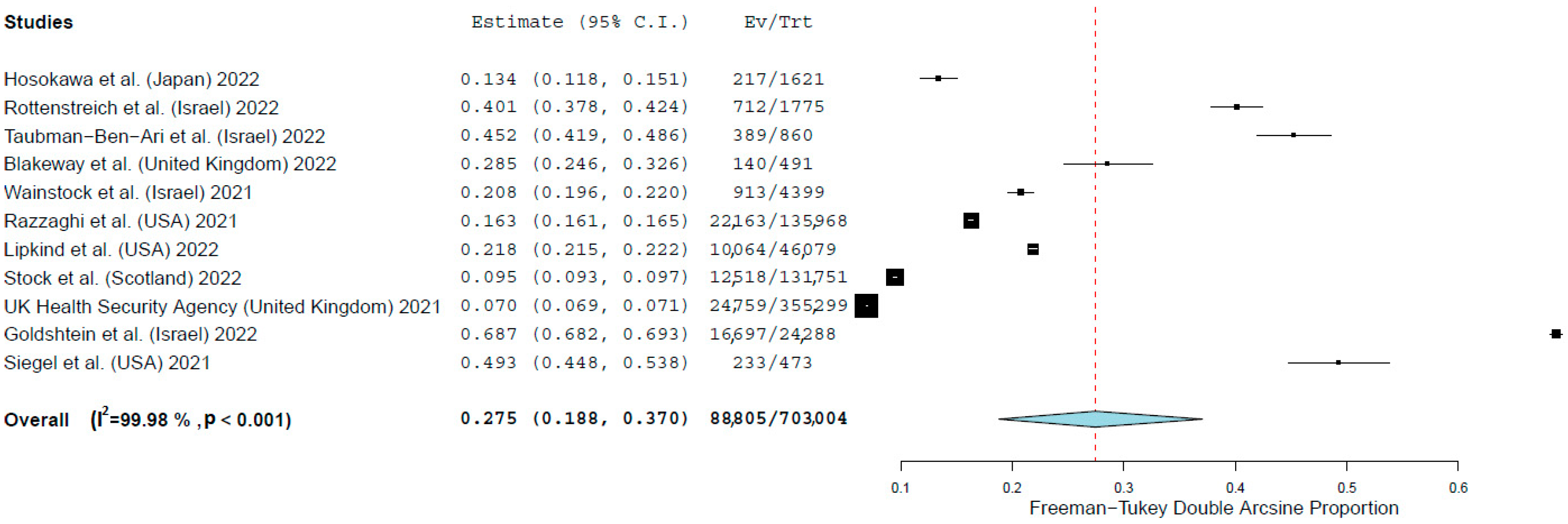
3.4. COVID-19 Vaccination Uptake
3.5. Factors Related to COVID-19 Vaccination Uptake
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Khalil, A.; von Dadelszen, P.; Draycott, T.; Ugwumadu, A.; O’Brien, P.; Magee, L. Change in the Incidence of Stillbirth and Preterm Delivery during the COVID-19 Pandemic. JAMA 2020, 324, 705. [Google Scholar] [CrossRef]
- Lokken, E.M.; Huebner, E.M.; Taylor, G.G.; Hendrickson, S.; Vanderhoeven, J.; Kachikis, A.; Coler, B.; Walker, C.L.; Sheng, J.S.; Al-Haddad, B.J.S.; et al. Disease Severity, Pregnancy Outcomes, and Maternal Deaths among Pregnant Patients with Severe Acute Respiratory Syndrome Coronavirus 2 Infection in Washington State. Am. J. Obstet. Gynecol. 2021, 225, 77.e1–77.e14. [Google Scholar] [CrossRef]
- Vousden, N.; Bunch, K.; Morris, E.; Simpson, N.; Gale, C.; O’Brien, P.; Quigley, M.; Brocklehurst, P.; Kurinczuk, J.J.; Knight, M. The Incidence, Characteristics and Outcomes of Pregnant Women Hospitalized with Symptomatic and Asymptomatic SARS-CoV-2 Infection in the UK from March to September 2020: A National Cohort Study Using the UK Obstetric Surveillance System (UKOSS). PLoS ONE 2021, 16, e0251123. [Google Scholar] [CrossRef]
- Woodworth, K.R.; Olsen, E.O.; Neelam, V.; Lewis, E.L.; Galang, R.R.; Oduyebo, T.; Aveni, K.; Yazdy, M.M.; Harvey, E.; Longcore, N.D.; et al. Birth and Infant Outcomes Following Laboratory-Confirmed SARS-CoV-2 Infection in Pregnancy-SET-NET, 16 Jurisdictions, March 29-October 14, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1635–1640. [Google Scholar] [CrossRef]
- Zambrano, L.D.; Ellington, S.; Strid, P.; Galang, R.R.; Oduyebo, T.; Tong, V.T.; Woodworth, K.R.; Nahabedian, J.F.; Azziz-Baumgartner, E.; Gilboa, S.M.; et al. Update: Characteristics of Symptomatic Women of Reproductive Age with Laboratory-Confirmed SARS-CoV-2 Infection by Pregnancy Status-United States, January 22–October 3, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1641–1647. [Google Scholar] [CrossRef]
- Iacobucci, G. COVID-19 and Pregnancy: Vaccine Hesitancy and How to Overcome It. BMJ 2021, 375, n2862. [Google Scholar] [CrossRef]
- UK Health Security Agency. COVID-19 Vaccine Surveillance Report Week 47; UK Health Security Agency: London, UK, 2021. [Google Scholar]
- Tognon, M.; Tagliapietra, A.; Magagnoli, F.; Mazziotta, C.; Oton-Gonzalez, L.; Lanzillotti, C.; Vesce, F.; Contini, C.; Rotondo, J.C.; Martini, F. Investigation on Spontaneous Abortion and Human Papillomavirus Infection. Vaccines 2020, 8, 473. [Google Scholar] [CrossRef]
- Giakoumelou, S.; Wheelhouse, N.; Cuschieri, K.; Entrican, G.; Howie, S.; Horne, A. The role of infection in miscarriage. Hum. Reprod. Updat. 2016, 22, 116–133. [Google Scholar] [CrossRef] [Green Version]
- Pogue, K.; Jensen, J.L.; Stancil, C.K.; Ferguson, D.G.; Hughes, S.J.; Mello, E.J.; Burgess, R.; Berges, B.K.; Quaye, A.; Poole, B.D. Influences on Attitudes Regarding Potential COVID-19 Vaccination in the United States. Vaccines 2020, 8, 582. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 MRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Falsaperla, R.; Leone, G.; Familiari, M.; Ruggieri, M. COVID-19 Vaccination in Pregnant and Lactating Women: A Systematic Review. Expert Rev. Vaccines 2021, 20, 1619–1628. [Google Scholar] [CrossRef]
- Fu, W.; Sivajohan, B.; McClymont, E.; Albert, A.; Elwood, C.; Ogilvie, G.; Money, D. Systematic Review of the Safety, Immunogenicity, and Effectiveness of COVID-19 Vaccines in Pregnant and Lactating Individuals and Their Infants. Int. J. Gynaecol. Obstet. 2022, 156, 406–417. [Google Scholar] [CrossRef]
- Rawal, S.; Tackett, R.L.; Stone, R.H.; Young, H.N. COVID-19 Vaccination among Pregnant People in the U.S.: A Systematic Review. Am. J. Obstet. Gynecol. 2022, 4, 100616. [Google Scholar] [CrossRef]
- Garg, I.; Shekhar, R.; Sheikh, A.B.; Pal, S. COVID-19 Vaccine in Pregnant and Lactating Women: A Review of Existing Evidence and Practice Guidelines. Infect. Dis. Rep. 2021, 13, 685–699. [Google Scholar] [CrossRef]
- Mendoza, M.; Garcia-Ruiz, I.; Maiz, N.; Rodo, C.; Garcia-Manau, P.; Serrano, B.; Lopez-Martinez, R.; Balcells, J.; Fernandez-Hidalgo, N.; Carreras, E.; et al. Pre-eclampsia-like Syndrome Induced by Severe COVID-19: A Prospective Observational Study. BJOG: Int. J. Obstet. Gy. 2020, 127, 1374–1380. [Google Scholar] [CrossRef]
- American College of Obstetricians and Gynecologist. ACOG and SMFM Recommend COVID-19 Vaccination for Pregnant Individuals; American College of Obstetricians and Gynecologist: Washington, DC, USA, 2021. [Google Scholar]
- Centers for Disease Control and Prevention. COVID-19 Vaccines While Pregnant or Breastfeeding; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2021; pp. 1–6. [Google Scholar]
- Rasmussen, S.A.; Jamieson, D.J. Pregnancy, Postpartum Care, and COVID-19 Vaccination in 2021. JAMA 2021, 325, 1099–1100. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The PRISMA Group Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Dos Santos, W.M.; Secoli, S.R.; Püschel, V.A.D.A. The Joanna Briggs Institute Approach for Systematic Reviews. Rev. Latino-Am. Enfermagem. 2018, 26, e3074. [Google Scholar] [CrossRef] [Green Version]
- Barendregt, J.J.; Doi, S.A.; Lee, Y.Y.; Norman, R.E.; Vos, T. Meta-Analysis of Prevalence. J. Epidemiol. Community Health 2013, 67, 974–978. [Google Scholar] [CrossRef]
- Higgins, J.P.T. Measuring Inconsistency in Meta-Analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in Meta-Analysis Detected by a Simple, Graphical Test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wallace, B.C.; Schmid, C.H.; Lau, J.; Trikalinos, T.A. Meta-Analyst: Software for Meta-Analysis of Binary, Continuous and Diagnostic Data. BMC Med. Res. Methodol. 2009, 9, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldshtein, I.; Steinberg, D.M.; Kuint, J.; Chodick, G.; Segal, Y.; Shapiro Ben David, S.; Ben-Tov, A. Association of BNT162b2 COVID-19 Vaccination during Pregnancy with Neonatal and Early Infant Outcomes. JAMA Pediatr. 2022, 176, 470. [Google Scholar] [CrossRef]
- Rottenstreich, M.; Sela, H.; Rotem, R.; Kadish, E.; Wiener-Well, Y.; Grisaru-Granovsky, S. COVID-19 Vaccination during the Third Trimester of Pregnancy: Rate of Vaccination and Maternal and Neonatal Outcomes, a Multicentre Retrospective Cohort Study. BJOG 2022, 129, 248–255. [Google Scholar] [CrossRef]
- Taubman-Ben-Ari, O.; Weiss, E.; Abu-Sharkia, S.; Khalaf, E. A Comparison of COVID-19 Vaccination Status among Pregnant Israeli Jewish and Arab Women and Psychological Distress among the Arab Women. Nurs. Health Sci. 2022, 1–8. [Google Scholar] [CrossRef]
- Wainstock, T.; Yoles, I.; Sergienko, R.; Sheiner, E. Prenatal Maternal COVID-19 Vaccination and Pregnancy Outcomes. Vaccine 2021, 39, 6037–6040. [Google Scholar] [CrossRef]
- Lipkind, H.S.; Vazquez-Benitez, G.; DeSilva, M.; Vesco, K.K.; Ackerman-Banks, C.; Zhu, J.; Boyce, T.G.; Daley, M.F.; Fuller, C.C.; Getahun, D.; et al. Receipt of COVID-19 Vaccine during Pregnancy and Preterm or Small-for-Gestational-Age at Birth—Eight Integrated Health Care Organizations, United States, 15 December 2020–22 July 2021. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 26–30. [Google Scholar] [CrossRef]
- Razzaghi, H.; Meghani, M.; Pingali, C.; Crane, B.; Naleway, A.; Weintraub, E.; Kenigsberg, T.A.; Lamias, M.J.; Irving, S.A.; Kauffman, T.L.; et al. COVID-19 Vaccination Coverage among Pregnant Women during Pregnancy—Eight Integrated Health Care Organizations, United States, December 14, 2020–May 8, 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 895–899. [Google Scholar] [CrossRef]
- Siegel, M.R.; Lumbreras-Marquez, M.I.; James, K.; McBay, B.R.; Gray, K.J.; Schantz-Dunn, J.; Diouf, K.; Goldfarb, I.T. Perceptions and Attitudes towards COVID-19 Vaccination Amongst Pregnant and Postpartum Individuals. MedRxiv 2021. [Google Scholar] [CrossRef]
- Blakeway, H.; Prasad, S.; Kalafat, E.; Heath, P.T.; Ladhani, S.N.; Le Doare, K.; Magee, L.A.; O’Brien, P.; Rezvani, A.; von Dadelszen, P.; et al. COVID-19 Vaccination during Pregnancy: Coverage and Safety. Am. J. Obstet. Gynecol. 2022, 226, 236.e1–236.e14. [Google Scholar] [CrossRef]
- Hosokawa, Y.; Okawa, S.; Hori, A.; Morisaki, N.; Takahashi, Y.; Fujiwara, T.; Nakayama, S.F.; Hamada, H.; Satoh, T.; Tabuchi, T. The Prevalence of COVID-19 Vaccination and Vaccine Hesitancy in Pregnant Women: An Internet-Based Cross-Sectional Study in Japan. J. Epidemiol. 2022, 32, 188–194. [Google Scholar] [CrossRef] [PubMed]
- Stock, S.J.; Carruthers, J.; Calvert, C.; Denny, C.; Donaghy, J.; Goulding, A.; Hopcroft, L.E.M.; Hopkins, L.; McLaughlin, T.; Pan, J.; et al. SARS-CoV-2 Infection and COVID-19 Vaccination Rates in Pregnant Women in Scotland. Nat. Med. 2022, 28, 504–512. [Google Scholar] [CrossRef] [PubMed]
- Carbone, L.; Di Girolamo, R.; Mappa, I.; Saccone, G.; Raffone, A.; Di Mascio, D.; De Vivo, V.; D’Antonio, F.; Guida, M.; Rizzo, G.; et al. Worldwide Beliefs among Pregnant Women on SARS-CoV-2 Vaccine: A Systematic Review. Eur. J. Obstet. Gynecol. Reprod. Biol. 2022, 268, 144–164. [Google Scholar] [CrossRef]
- Nikpour, M.; Sepidarkish, M.; Omidvar, S.; Firouzbakht, M. Global Prevalence of Acceptance of COVID-19 Vaccines and Associated Factors in Pregnant Women: A Systematic Review and Meta-Analysis. Expert Rev. Vaccines 2022, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Skjefte, M.; Ngirbabul, M.; Akeju, O.; Escudero, D.; Hernandez-Diaz, S.; Wyszynski, D.F.; Wu, J.W. COVID-19 Vaccine Acceptance among Pregnant Women and Mothers of Young Children: Results of a Survey in 16 Countries. Eur. J. Epidemiol. 2021, 36, 197–211. [Google Scholar] [CrossRef]
- The Israeli Health Ministry. Recommendation That Pregnant Women Get Vaccinated with Frequent Exposure to People or with Chronic Medical Conditions; The Israeli Health Ministry: Jerusalem, Israel, 2021. [Google Scholar]
- Shimabukuro, T.T.; Kim, S.Y.; Myers, T.R.; Moro, P.L.; Oduyebo, T.; Panagiotakopoulos, L.; Marquez, P.L.; Olson, C.K.; Liu, R.; Chang, K.T.; et al. Preliminary Findings of MRNA COVID-19 Vaccine Safety in Pregnant Persons. N. Engl. J. Med. 2021, 384, 2273–2282. [Google Scholar] [CrossRef]
- Trostle, M.E.; Limaye, M.A.; Avtushka, V.; Lighter, J.L.; Penfield, C.A.; Roman, A.S. COVID-19 Vaccination in Pregnancy: Early Experience from a Single Institution. Am. J. Obstet. Gynecol. 2021, 3, 100464. [Google Scholar] [CrossRef]
- Levy, A.T.; Singh, S.; Riley, L.E.; Prabhu, M. Acceptance of COVID-19 Vaccination in Pregnancy: A Survey Study. Am. J. Obstet. Gynecol. 2021, 3, 100399. [Google Scholar] [CrossRef]
- Stuckelberger, S.; Favre, G.; Ceulemans, M.; Nordeng, H.; Gerbier, E.; Lambelet, V.; Stojanov, M.; Winterfeld, U.; Baud, D.; Panchaud, A.; et al. SARS-CoV-2 Vaccine Willingness among Pregnant and Breastfeeding Women during the First Pandemic Wave: A Cross-Sectional Study in Switzerland. Viruses 2021, 13, 1199. [Google Scholar] [CrossRef]
- Glick, I.; Kadish, E.; Rottenstreich, M. Management of Pregnancy in Women of Advanced Maternal Age: Improving Outcomes for Mother and Baby. IJWH 2021, 13, 751–759. [Google Scholar] [CrossRef]
- Pinheiro, R.L.; Areia, A.L.; Mota Pinto, A.; Donato, H. Advanced Maternal Age: Adverse Outcomes of Pregnancy, A Meta-Analysis. Acta. Med. Port. 2019, 32, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Mehraeen, E.; Karimi, A.; Barzegary, A.; Vahedi, F.; Afsahi, A.M.; Dadras, O.; Moradmand-Badie, B.; Seyed Alinaghi, S.A.; Jahanfar, S. Predictors of Mortality in Patients with COVID-19—A Systematic Review. Eur. J. Integr. Med. 2020, 40, 101226. [Google Scholar] [CrossRef] [PubMed]
- Sepandi, M.; Taghdir, M.; Alimohamadi, Y.; Afrashteh, S.; Hosamirudsari, H. Factors Associated with Mortality in COVID-19 Patients: A Systematic Review and Meta-Analysis. IJPH 2020, 49, 1211–1221. [Google Scholar] [CrossRef] [PubMed]
- Yanez, N.D.; Weiss, N.S.; Romand, J.-A.; Treggiari, M.M. COVID-19 Mortality Risk for Older Men and Women. BMC Public Health 2020, 20, 1742. [Google Scholar] [CrossRef] [PubMed]
- Tao, L.; Wang, R.; Han, N.; Liu, J.; Yuan, C.; Deng, L.; Han, C.; Sun, F.; Liu, M.; Liu, J. Acceptance of a COVID-19 Vaccine and Associated Factors among Pregnant Women in China: A Multi-Center Cross-Sectional Study Based on Health Belief Model. Hum. Vaccin. Immunother. 2021, 17, 2378–2388. [Google Scholar] [CrossRef]
- Battarbee, A.N.; Stockwell, M.S.; Varner, M.; Newes-Adeyi, G.; Daugherty, M.; Gyamfi-Bannerman, C.; Tita, A.T.; Vorwaller, K.; Vargas, C.; Subramaniam, A.; et al. Attitudes toward COVID-19 Illness and COVID-19 Vaccination among Pregnant Women: A Cross-Sectional Multicenter Study during August–December 2020. Am. J. Perinatol. 2022, 39, 075–083. [Google Scholar] [CrossRef]
- Huddleston, H.G.; Jaswa, E.G.; Lindquist, K.J.; Kaing, A.; Morris, J.R.; Hariton, E.; Corley, J.; Hoskin, E.; Gaw, S.L.; Cedars, M.I. COVID-19 Vaccination Patterns and Attitudes among American Pregnant Individuals. Am. J. Obstet. Gynecol. 2022, 4, 100507. [Google Scholar] [CrossRef]
- Townsel, C.; Moniz, M.H.; Wagner, A.L.; Zikmund-Fisher, B.J.; Hawley, S.; Jiang, L.; Stout, M.J. COVID-19 Vaccine Hesitancy among Reproductive-Aged Female Tier 1A Healthcare Workers in a United States Medical Center. J. Perinatol. 2021, 41, 2549–2551. [Google Scholar] [CrossRef]
- Galanis, P.; Vraka, I.; Siskou, O.; Konstantakopoulou, O.; Katsiroumpa, A.; Kaitelidou, D. Predictors of COVID-19 Vaccination Uptake and Reasons for Decline of Vaccination: A Systematic Review. MedRxiv 2021. [Google Scholar] [CrossRef]
- Razzaghi, H.; Kahn, K.E.; Black, C.L.; Lindley, M.C.; Jatlaoui, T.C.; Fiebelkorn, A.P.; Havers, F.P.; D’Angelo, D.V.; Cheung, A.; Ruther, N.A.; et al. Influenza and Tdap Vaccination Coverage among Pregnant Women—United States, April 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1391–1397. [Google Scholar] [CrossRef]
- Ceulemans, M.; Foulon, V.; Panchaud, A.; Winterfeld, U.; Pomar, L.; Lambelet, V.; Cleary, B.; O’Shaughnessy, F.; Passier, A.; Richardson, J.L.; et al. Vaccine Willingness and Impact of the COVID-19 Pandemic on Women’s Perinatal Experiences and Practices—A Multinational, Cross-Sectional Study Covering the First Wave of the Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 3367. [Google Scholar] [CrossRef] [PubMed]
- Gencer, H.; Özkan, S.; Vardar, O.; Serçekuş, P. The Effects of the COVID 19 Pandemic on Vaccine Decisions in Pregnant Women. Women Birth 2021, 35, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Geoghegan, S.; Stephens, L.C.; Feemster, K.A.; Drew, R.J.; Eogan, M.; Butler, K.M. “This Choice Does Not Just Affect Me.” Attitudes of Pregnant Women toward COVID-19 Vaccines: A Mixed-Methods Study. Hum. Vaccin. Immunother. 2021, 17, 3371–3376. [Google Scholar] [CrossRef]
- Mappa, I.; Luviso, M.; Distefano, F.A.; Carbone, L.; Maruotti, G.M.; Rizzo, G. Women Perception of SARS-CoV-2 Vaccination during Pregnancy and Subsequent Maternal Anxiety: A Prospective Observational Study. J. Matern-Fetal Neonatal Med. 2021, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Deng, J.; Liu, Q.; Du, M.; Liu, M.; Liu, J. Effectiveness and Safety of COVID-19 Vaccine among Pregnant Women in Real-World Studies: A Systematic Review and Meta-Analysis. Vaccines 2022, 10, 246. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Reference | Country | Data Collection Time | Sample Size (N) | Age, Mean (Standard Deviation) | Study Design | Sampling Method | Response Rate (%) | COVID-19 Vaccination Uptake, % (n/N) | Publication |
|---|---|---|---|---|---|---|---|---|---|
| Hosokawa et al. [34] | Japan | 28 July to 30 August 2021 | 1621 | <29 years, 35.6%; ≥29 years, 64.4% | Cross-sectional | Convenience sampling | 73.9 | 13.4 (217/1621) | Journal |
| Rottenstreich et al. [27] | Israel | 19 January to 27 April 2021 | 1775 | 30.6 (5.8) for vaccinated and 29.5 (6) for unvaccinated | Cohort | NR | NR | 40.2 (712/1775) | Journal |
| Taubman et al. [28] | Israel | March to April, 2021 | 860 | 28.3 (4.4) | Cross-sectional | Convenience sampling | 65 | 45.2 (389/860) | Journal |
| Blakeway et al. [33] | United Kingdom | March to July, 2021 | 491 | 35 (NR) for vaccinated and 33 (NR) for unvaccinated | Cohort | NR | NR | 28.5 (140/491) | Journal |
| Wainstock et al. [29] | Israel | January to June, 2021 | 4399 | 30.6 (5.3) for vaccinated and 28.2 (5.7) for unvaccinated | Cohort | NR | NR | 20.8 (913/4399) | Journal |
| Razzaghi et al. [31] | USA | 14 December 2020 to 8 May 2021 | 135,968 | 18–24 years, 13.9%; 25–34 years, 61.3%; 35–49 years, 24.8% | Cohort | NR | NR | 16.3 (22,163/135,968) | Journal |
| Lipkind et al. [30] | USA | 15 December 2020 to 22 July 2021 | 46,079 | 32.3 (4.5) for vaccinated and 29.8 (5.3) for unvaccinated | Cohort | NR | NR | 21.8 (10,064/46,079) | Journal |
| Stock et al. [35] | Scotland | 1 December 2020 to 31 October 2021 | 131,751 | NR | Cohort | National data | NA | 9.5 (12,518/131,751) | Journal |
| UK Health Security Agency [7] | United Kingdom | January to August 2021 | 355,299 | NR | Cohort | National data | NA | 7 (24,759/355,299) | Journal |
| Goldshtein et al. [26] | Israel | March to September 2021 | 24,288 | 31.6 (5.2) for vaccinated and 30.5 (5.7) for unvaccinated | Cohort | NR | NR | 68.7 (16,697/24,288) | Journal |
| Siegel et al. [32] | USA | June to August 2021 | 473 | 33 (4.5) for vaccinated and 31.4 (5.6) for unvaccinated | Cross-sectional | Convenience sampling | 69.7 | 49.3 (233/473) | Pre-print service |
| Reference | Predictors of COVID-19 Vaccination Uptake | Reasons for Declining COVID-19 Vaccination |
|---|---|---|
| Blakeway et al. [33] |
| |
| Hosokawa et al. [34] |
| |
| Razzaghi et al. [31] |
| |
| UK Health Security [7] |
| |
| Siegel et al. [32] |
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Galanis, P.; Vraka, I.; Siskou, O.; Konstantakopoulou, O.; Katsiroumpa, A.; Kaitelidou, D. Uptake of COVID-19 Vaccines among Pregnant Women: A Systematic Review and Meta-Analysis. Vaccines 2022, 10, 766. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10050766
Galanis P, Vraka I, Siskou O, Konstantakopoulou O, Katsiroumpa A, Kaitelidou D. Uptake of COVID-19 Vaccines among Pregnant Women: A Systematic Review and Meta-Analysis. Vaccines. 2022; 10(5):766. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10050766
Chicago/Turabian StyleGalanis, Petros, Irene Vraka, Olga Siskou, Olympia Konstantakopoulou, Aglaia Katsiroumpa, and Daphne Kaitelidou. 2022. "Uptake of COVID-19 Vaccines among Pregnant Women: A Systematic Review and Meta-Analysis" Vaccines 10, no. 5: 766. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines10050766