
Effect of Information about COVID-19 Vaccine Effectiveness and Side Effects on Behavioural Intentions: Two Online Experiments


Abstract
:1. Introduction
1.1. Transparent Communication of Vaccine Risks and Benefits
1.2. Beliefs about COVID Vaccines and Vaccine Hesitancy
1.3. The Effect of COVID-19 Vaccine Communications on Intentions
1.4. Post-Vaccination Protective Behaviour Messaging and Vaccine Confidence
2. Study 1
2.1. Methods
2.1.1. Participants
2.1.2. Materials and Procedure
2.2. Results
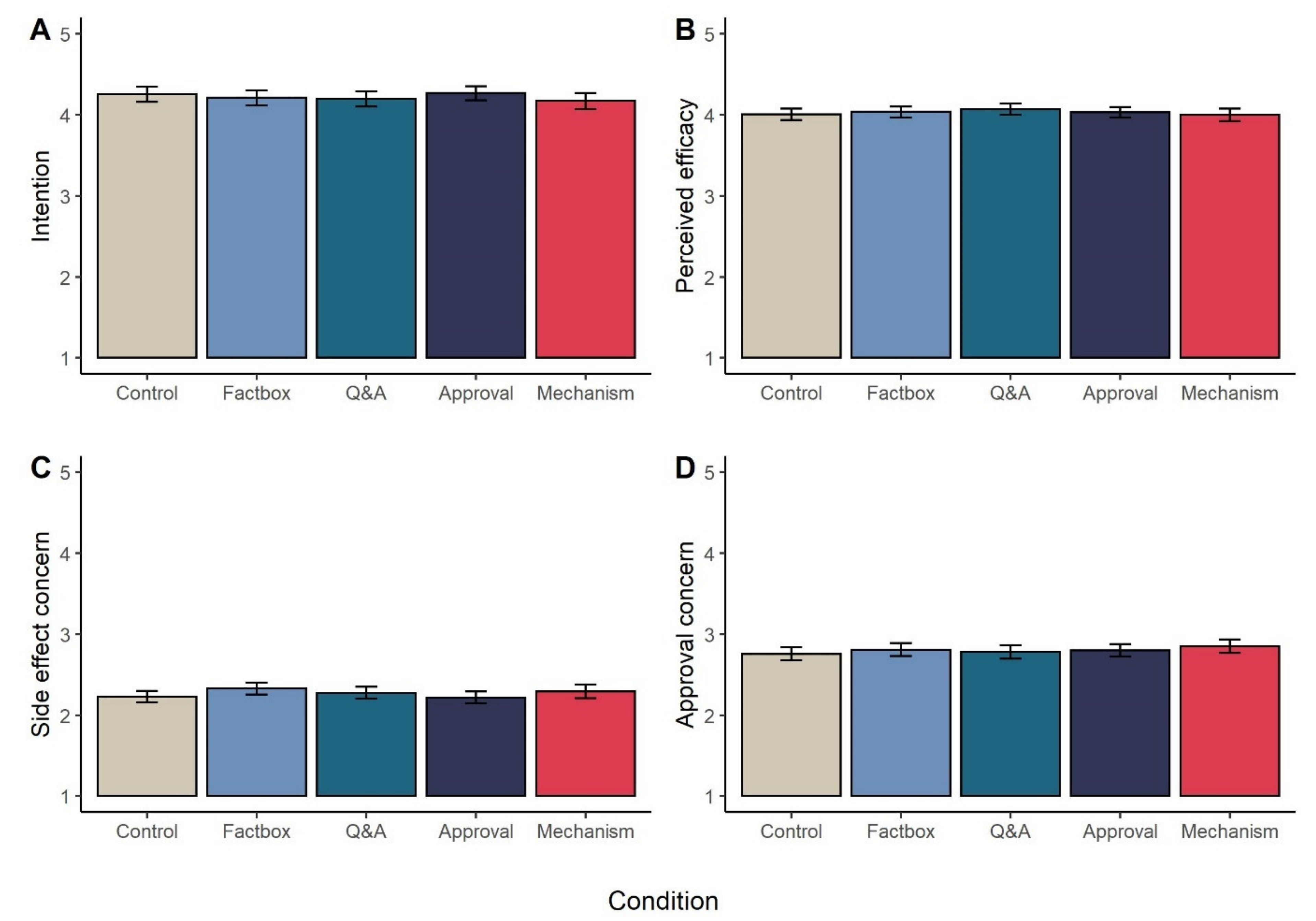
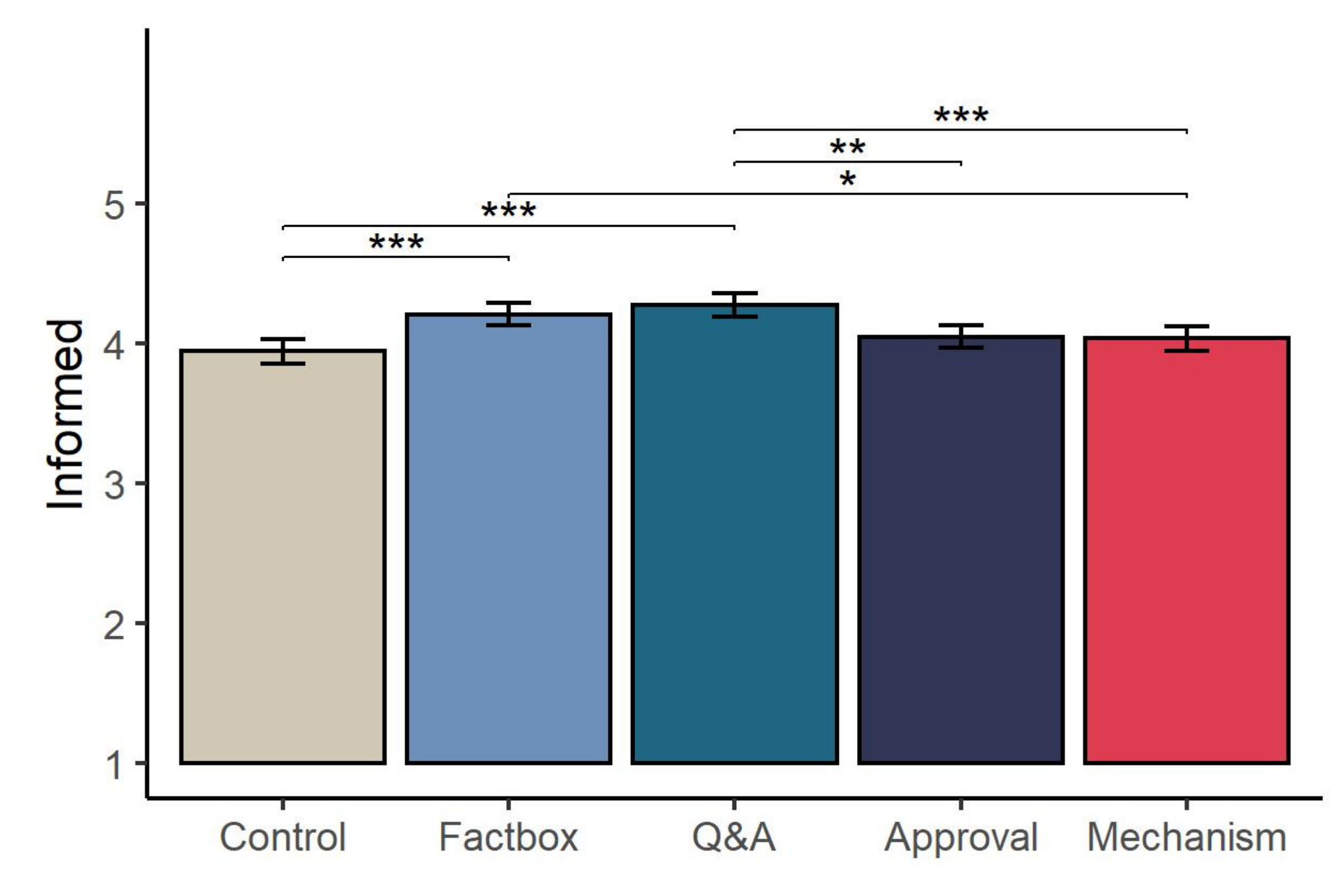
2.2.1. Primary Outcomes
2.2.2. Secondary Outcomes
2.3. Interim Discussion
3. Study 2
3.1. Methods
3.1.1. Participants
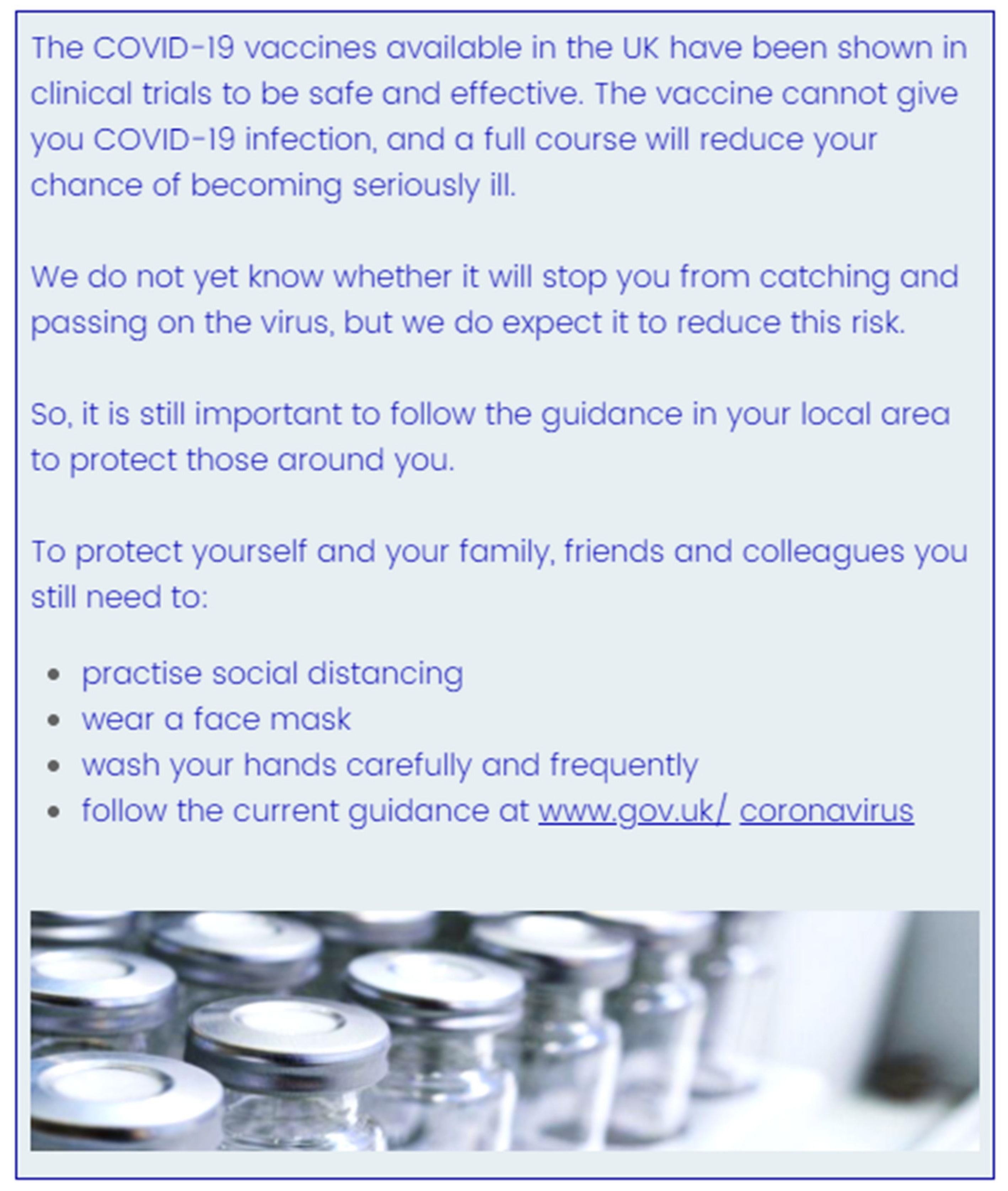
3.1.2. Materials and Procedure
3.1.3. Analysis
3.2. Results
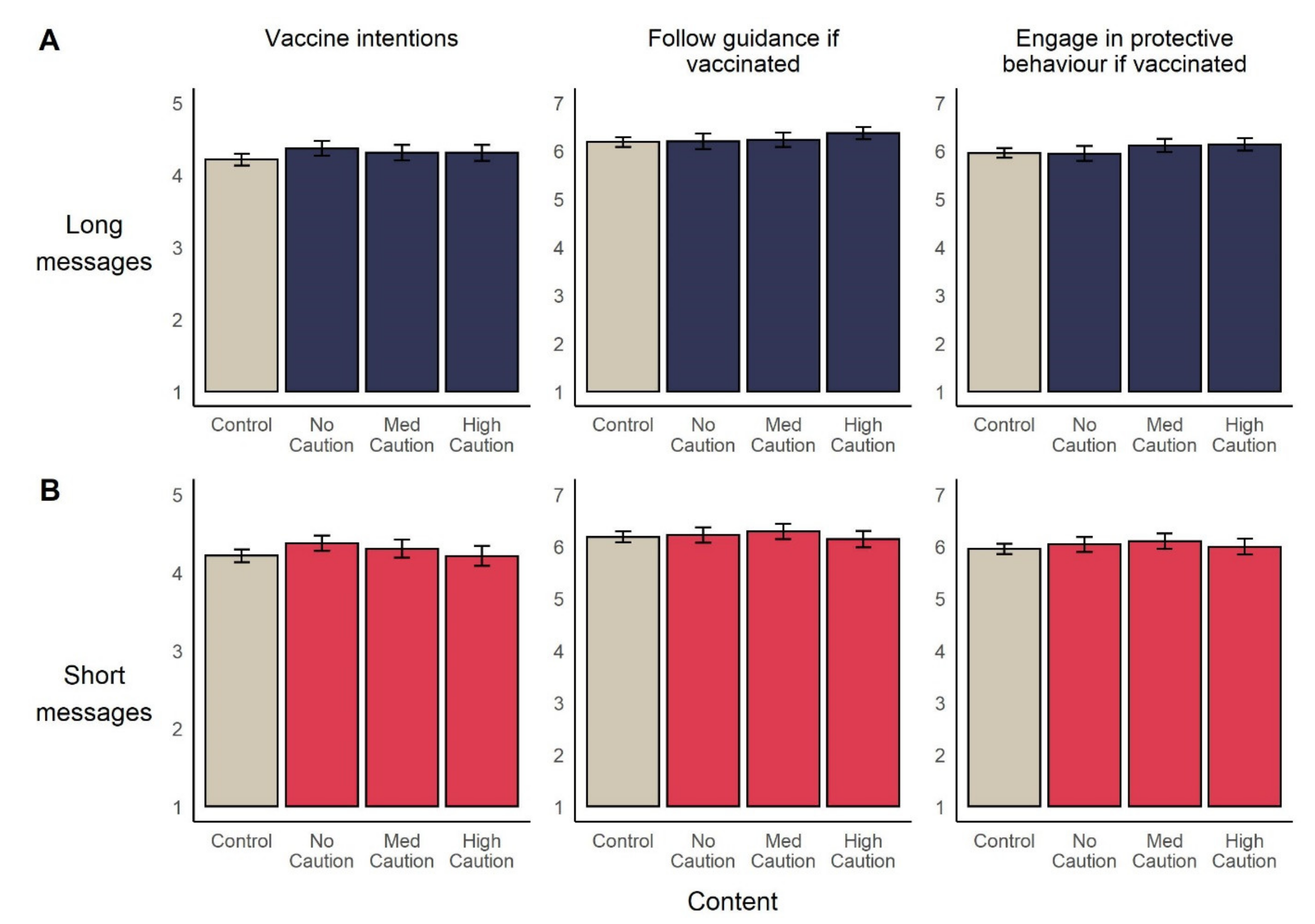
3.2.1. Primary Outcomes
3.2.2. Secondary Outcomes
3.3. Study 2 Discussion
4. General Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO Weekly Epidemiological Update-9 March 2021. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update---10-march-2021 (accessed on 12 March 2021).
- Saladino, V.; Algeri, D.; Auriemma, V. The Psychological and Social Impact of Covid-19: New Perspectives of Well-Being. Front. Psychol. 2020, 11, 2550. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, E.K.; Khan, I.I.; Dhar, B.K. Catastrophic impact of Covid-19 on the global stock markets and economic activities. Bus. Soc. Rev. 2021, 00, 1–24. [Google Scholar] [CrossRef]
- Pearl, R. The Queen’s Gambit and Covid-19: Why It’s All about the End Game Now. Available online: https://www.forbes.com/sites/robertpearl/2020/12/07/the-queens-gambit-and-covid-19-its-all-about-the-end-game-now/?sh=1cc0447d3f8a (accessed on 3 March 2021).
- Randolph, H.E.; Barreiro, L.B. Herd Immunity: Understanding COVID-19. Immunity 2020, 52, 737–741. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.M.; Vegvari, C.; Truscott, J.; Collyer, B.S. Challenges in creating herd immunity to SARS-CoV-2 infection by mass vaccination. Lancet 2020, 396, 1614–1616. [Google Scholar] [CrossRef]
- Kadkhoda, K. Herd Immunity to COVID-19. Am. J. Clin. Pathol. 2021, 155, 471–472. [Google Scholar] [CrossRef]
- Lin, C.; Tu, P.; Beitsch, L.M. Confidence and receptivity for covid-19 vaccines: A rapid systematic review. Vaccines 2021, 9, 16. [Google Scholar] [CrossRef]
- WHO. Report of the Sage Working Group on Vaccine Hesitancy; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- De Figueiredo, A.; Simas, C.; Karafillakis, E.; Paterson, P.; Larson, H.J. Mapping global trends in vaccine confidence and investigating barriers to vaccine uptake: A large-scale retrospective temporal modelling study. Lancet 2020, 396, 898–908. [Google Scholar] [CrossRef]
- Kerr, J.R.; Schneider, C.R.; Recchia, G.; Dryhurst, S.; Sahlin, U.; Dufouil, C.; Arwidson, P.; Freeman, A.L.J.; van der Linden, S. Predictors of COVID-19 vaccine acceptance across time and countries. medRxiv 2020. [Google Scholar] [CrossRef]
- Freeman, D.; Loe, B.S.; Chadwick, A.; Vaccari, C.; Waite, F.; Rosebrock, L.; Jenner, L.; Petit, A.; Lewandowsky, S.; Vanderslott, S.; et al. COVID-19 vaccine hesitancy in the UK: The Oxford coronavirus explanations, attitudes, and narratives survey (Oceans) II. Psychol. Med. 2021, 1–15. [Google Scholar] [CrossRef]
- Quinn, S.C.; Jamison, A.M.; Freimuth, V. Communicating Effectively About Emergency Use Authorization and Vaccines in the COVID-19 Pandemic. Am. J. Public Health 2021, 111, 355–358. [Google Scholar] [CrossRef]
- Cohen, A.F.; van Gerven, J.; Burgos, J.G.; de Boer, A.; Foucher, R.A.M.; Flore, H.; Teitelbaum, Z.; van Eden, W.; Webb, A.; Cremers, S. COVID-19 vaccines: The importance of transparency and fact-based education. Br. J. Clin. Pharmacol. 2020, 86, 2107–2110. [Google Scholar] [CrossRef]
- Nature COVID vaccine confidence requires radical transparency. Nature 2020, 586, 8. [CrossRef]
- Rzymski, P.; Borkowski, L.; Drąg, M.; Flisiak, R.; Jemielity, J.; Krajewski, J.; Mastalerz-Migas, A.; Matyja, A.; Pyrć, K.; Simon, K.; et al. The Strategies to Support the COVID-19 Vaccination with Evidence-Based Communication and Tackling Misinformation. Vaccines 2021, 9, 109. [Google Scholar] [CrossRef]
- Blastland, M.; Freeman, A.L.J.; van der Linden, S.; Marteau, T.M.; Spiegelhalter, D. Five rules for evidence communication. Nature 2020, 587, 362–364. [Google Scholar] [CrossRef]
- Cousins, S.; Blencowe, N.S.; Blazeby, J.M. What is an invasive procedure? A definition to inform study design, evidence synthesis and research tracking. BMJ Open 2019, 9, 2018–2020. [Google Scholar] [CrossRef] [Green Version]
- Reiss, D.R.; Karako-Eyal, N. Informed Consent to Vaccination: Theoretical, Legal, and Empirical Insights. Am. J. Law Med. 2019, 45, 357–419. [Google Scholar] [CrossRef]
- O’Neill, O. Some limits of informed consent. Elder. Leg. Ethical Issues Healthc. Policy 2017, 103–106. [Google Scholar] [CrossRef] [Green Version]
- Parmet, W.E. Informed consent and public health: Are they compatible when it comes to vaccines? J. Health Care Law Policy 2005, 8, 71–110. [Google Scholar]
- O’Neill, J. Case for persuasion in parental informed consent to promote rational vaccine choices. J. Med. Ethics 2020, 1–6. [Google Scholar] [CrossRef]
- GMC Coronavirus: Your Frequently Asked Questions. Available online: https://www.gmc-uk.org/ethical-guidance/ethical-hub/covid-19-questions-and-answers (accessed on 12 April 2021).
- Marco-Franco, J.E.; Pita-Barros, P.; Vivas-Orts, D.; González-de-Julián, S.; Vivas-Consuelo, D. COVID-19, Fake News, and Vaccines: Should Regulation Be Implemented? Int. J. Environ. Res. Public Health 2021, 18, 744. [Google Scholar] [CrossRef]
- Petersen, M.B.; Bor, A.; Jørgensen, F.J.; Lindholt, M.F. Transparency Is Necessary but Not Sufficient to Reduce Skepticism About a COVID-19 Vaccine. PsyArXiv 2020. [Google Scholar] [CrossRef]
- Rossen, I.; Hurlstone, M.J.; Lawrence, C. Going with the Grain of Cognition: Applying Insights from Psychology to Build Support for Childhood Vaccination. Front. Psychol. 2016, 7, 1483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simis, M.J.; Madden, H.; Cacciatore, M.A.; Yeo, S.K. The lure of rationality: Why does the deficit model persist in science communication? Public Underst. Sci. 2016, 25, 400–414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kitta, A.; Goldberg, D.S. The significance of folklore for vaccine policy: Discarding the deficit model. Crit. Public Health 2017, 27, 506–514. [Google Scholar] [CrossRef]
- Opel, D.J.; Salmon, D.A.; Marcuse, E.K. Building Trust to Achieve Confidence in COVID-19 Vaccines. JAMA Netw. Open 2020, 3, e2025672. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Hu, Z.; Zhao, Q.; Alias, H.; Danaee, M.; Wong, L.P. Understanding COVID-19 vaccine demand and hesitancy: A nationwide online survey in China. PLoS Negl. Trop. Dis. 2020, 12, e0008961. [Google Scholar] [CrossRef]
- Karlsson, L.C.; Soveri, A.; Lewandowsky, S.; Karlsson, L.; Karlsson, H.; Nolvi, S.; Karukivi, M.; Lindfelt, M.; Antfolk, J. Fearing the disease or the vaccine: The case of COVID-19. Pers. Individ. Dif. 2021, 172, 110590. [Google Scholar] [CrossRef]
- Wang, K.; Wong, E.L.Y.; Ho, K.F.; Cheung, A.W.L.; Yau, P.S.Y.; Dong, D.; Wong, S.Y.S.; Yeoh, E.K. Change of willingness to accept covid-19 vaccine and reasons of vaccine hesitancy of working people at different waves of local epidemic in hong kong, china: Repeated cross-sectional surveys. Vaccines 2021, 9, 62. [Google Scholar] [CrossRef]
- Callaghan, T.; Moghtaderi, A.; Lueck, J.A.; Hotez, P.; Strych, U.; Dor, A.; Fowler, E.F.; Motta, M. Correlates and disparities of intention to vaccinate against COVID-19. Soc. Sci. Med. 2021, 272, 113638. [Google Scholar] [CrossRef]
- Paul, E.; Steptoe, A.; Fancourt, D. Attitudes towards vaccines and intention to vaccinate against COVID-19: Implications for public health communications. Lancet Reg. Health Eur. 2021, 1, 100012. [Google Scholar] [CrossRef]
- Wong, L.P.; Alias, H.; Wong, P.-F.; Lee, H.Y.; AbuBakar, S. The use of the health belief model to assess predictors of intent to receive the COVID-19 vaccine and willingness to pay. Hum. Vaccin. Immunother. 2020, 16, 2204–2214. [Google Scholar] [CrossRef]
- Fisher, K.A.; Bloomstone, S.J.; Walder, J.; Crawford, S.; Fouayzi, H.; Mazor, K.M. Attitudes Toward a Potential SARS-CoV-2 Vaccine: A Survey of U.S. Adults. Ann. Intern. Med. 2020, 173, 964–973. [Google Scholar] [CrossRef] [PubMed]
- Frank, K.; Arim, R. Canadians’ Willingness to Get a COVID-19 Vaccine When One Becomes Available: What Role Does Trust Play? Available online: https://www150.statcan.gc.ca/n1/pub/45-28-0001/2020001/article/00043-eng.htm (accessed on 22 November 2020).
- Yoda, T.; Katsuyama, H. Willingness to receive covid-19 vaccination in Japan. Vaccines 2021, 9, 48. [Google Scholar] [CrossRef]
- Ruiz, J.B.; Bell, R.A. Predictors of intention to vaccinate against COVID-19: Results of a nationwide survey. Vaccine 2021, 7, 1080–1086. [Google Scholar] [CrossRef]
- Yigit, M.; Ozkaya-Parlakay, A.; Senel, E. Evaluation of COVID-19 Vaccine Refusal in Parents. Pediatr. Infect. Dis. J. 2021, 40, e134–e136. [Google Scholar] [CrossRef]
- Momplaisir, F.; Haynes, N.; Nkwihoreze, H.; Nelson, M.; Werner, R.M.; Jemmott, J. Understanding Drivers of COVID-19 Vaccine Hesitancy Among Blacks. Clin. Infect. Dis. 2021. [Google Scholar] [CrossRef]
- Lockyer, B.; Islam, S.; Rahman, A.; Dickerson, J.; Pickett, K.; Sheldon, T.; Wright, J.; McEachan, R.; Sheard, L. Understanding Covid-19 misinformation and vaccine hesitancy in context: Findings from a qualitative study involving citizens in Bradford, UK. medRxiv 2020. [Google Scholar] [CrossRef]
- Williams, L.; Gallant, A.J.; Rasmussen, S.; Brown Nicholls, L.A.; Cogan, N.; Deakin, K.; Young, D.; Flowers, P. Towards intervention development to increase the uptake of COVID-19 vaccination among those at high risk: Outlining evidence-based and theoretically informed future intervention content. Br. J. Health Psychol. 2020, 25, 1039–1054. [Google Scholar] [CrossRef] [PubMed]
- Hotez, P.J. COVID19 meets the antivaccine movement. Microbes Infect. 2020, 22, 162–164. [Google Scholar] [CrossRef]
- Roozenbeek, J.; Schneider, C.R.; Dryhurst, S.; Kerr, J.; Freeman, A.L.J.; Recchia, G.; van der Bles, A.M.; van der Linden, S. Susceptibility to misinformation about COVID-19 around the world. R. Soc. Open Sci. 2020, 7, 201199. [Google Scholar] [CrossRef]
- Carpenter, C.J. A Meta-Analysis of the Effectiveness of Health Belief Model Variables in Predicting Behavior. Health Commun. 2010, 25, 661–669. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maiman, L.A.; Becker, M.H. The Health Belief Model: Origins and Correlates in Psychological Theory. Health Educ. Monogr. 1974, 2, 336–353. [Google Scholar] [CrossRef]
- Jones, C.L.; Jensen, J.D.; Scherr, C.L.; Brown, N.R.; Christy, K.; Weaver, J. The Health Belief Model as an Explanatory Framework in Communication Research: Exploring Parallel, Serial, and Moderated Mediation. Health Commun. 2015, 30, 566–576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Motta, M. Can a COVID-19 vaccine live up to Americans’ expectations? A conjoint analysis of how vaccine characteristics influence vaccination intentions. Soc. Sci. Med. 2021, 272, 113642. [Google Scholar] [CrossRef]
- Borriello, A.; Master, D.; Pellegrini, A.; Rose, J.M. Preferences for a COVID-19 vaccine in Australia. Vaccine 2021, 39, 473–479. [Google Scholar] [CrossRef]
- Kreps, S.; Prasad, S.; Brownstein, J.S.; Hswen, Y.; Garibaldi, B.T.; Zhang, B.; Kriner, D.L. Factors Associated With US Adults’ Likelihood of Accepting COVID-19 Vaccination. JAMA Netw. Open 2020, 3, e2025594. [Google Scholar] [CrossRef]
- Schwarzinger, M.; Watson, V.; Arwidson, P.; Alla, F.; Luchini, S. COVID-19 vaccine hesitancy in a representative working-age population in France: A survey experiment based on vaccine characteristics. Lancet Public Health 2021, 6, e210–e221. [Google Scholar] [CrossRef]
- Kaplan, R.M.; Milstein, A. Influence of a COVID-19 vaccine’s effectiveness and safety profile on vaccination acceptance. Proc. Natl. Acad. Sci. USA 2021, 118, 2021726118. [Google Scholar] [CrossRef]
- Motta, M.; Sylvester, S.; Callaghan, T.; Lunz-Trujillo, K. Encouraging COVID-19 Vaccine Uptake Through Effective Health Communication. Front. Polit. Sci. 2021, 3, 1. [Google Scholar] [CrossRef]
- Palm, R.; Bolsen, T.; Kingsland, J.; Alakaloko, F.M.; Akase, I.E.; Otrofanowei, E.; Salu, O.B.; Adeyemo, W.L.; Ademuyiwa, A.O.; Omilabu, S.A.; et al. The Effect of Frames on COVID-19 Vaccine Hesitancy. medRxiv 2021. [Google Scholar] [CrossRef]
- Loomba, S.; de Figueiredo, A.; Piatek, S.J.; de Graaf, K.; Larson, H.J. Measuring the impact of COVID-19 vaccine misinformation on vaccination intent in the UK and USA. Nat. Hum. Behav. 2021, 1–12. [Google Scholar] [CrossRef]
- Duquette, N. Heard Immunity: Effective Persuasion for a Future COVID-19 Vaccine. SSRN Electron. J. 2020. [Google Scholar] [CrossRef]
- Altay, S.; Hacquin, A.-S.; Chevallier, C.; Mercier, H. Information Delivered by a Chatbot Has a Positive Impact on COVID-19 Vaccines Attitudes and Intentions. PsyArXiv 2021. [Google Scholar] [CrossRef]
- Ranney, M.A.; Clark, D. Climate change conceptual change: Scientific information can transform attitudes. Top. Cogn. Sci. 2016, 8, 49–75. [Google Scholar] [CrossRef] [Green Version]
- McPhetres, J.; Rutjens, B.T.; Weinstein, N.; Brisson, J.A. Modifying attitudes about modified foods: Increased knowledge leads to more positive attitudes. J. Environ. Psychol. 2019, 64, 21–29. [Google Scholar] [CrossRef] [Green Version]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Torjesen, I. Covid-19: AstraZeneca vaccine is approved in EU with no upper age limit. BMJ 2021, 372, n295. [Google Scholar] [CrossRef]
- The Lancet Microbe COVID-19 vaccines: The pandemic will not end overnight. Lancet Microbe 2021, 2, e1. [CrossRef]
- Su, Z.; Wen, J.; McDonnell, D.; Goh, E.; Li, X.; Šegalo, S.; Ahmad, J.; Cheshmehzangi, A.; Xiang, Y.-T. Vaccines are not yet a silver bullet: The imperative of continued communication about the importance of COVID-19 safety measures. Brain Behav. Immun. Health 2021, 12, 100204. [Google Scholar] [CrossRef]
- NHS. If You’ve Had the COVID-19 Vaccine, It’s Vital That You Continue to Follow Social Distancing Guidance. Read the Latest Guidance Here. Available online: https://twitter.com/NHSuk/status/1351861597157912576 (accessed on 12 April 2021).
- CDC. What to Expect after Getting a COVID-19 Vaccine [Archived Webpage]. Available online: https://web.archive.org/web/20210228020728/https://www.cdc.gov/coronavirus/2019-ncov/vaccines/expect/after.html (accessed on 2 March 2021).
- Pennings, S.; Symons, X. Persuasion, not coercion or incentivisation, is the best means of promoting COVID-19 vaccination. J. Med. Ethics 2021. [Google Scholar] [CrossRef]
- Prasad, V. Op-Ed: Throw Away Your Mask After COVID Vaccination? Available online: https://www.medpagetoday.com/blogs/vinay-prasad/90764 (accessed on 17 March 2021).
- Krupnikov, Y.; Findley, B. Survey experiments: Managing the methodological costs and benefits. In The Oxford Handbook of Polling and Polling Methods; Oxford University Press: Oxford, UK, 2015; pp. 483–504. ISBN 9780190213299. [Google Scholar]
- Nyhan, B.; Reifler, J. Does correcting myths about the flu vaccine work? An experimental evaluation of the effects of corrective information. Vaccine 2015, 33, 459–464. [Google Scholar] [CrossRef] [Green Version]
- Godinho, C.A.; Yardley, L.; Marcu, A.; Mowbray, F.; Beard, E.; Michie, S. Increasing the intent to receive a pandemic influenza vaccination: Testing the impact of theory-based messages. Prev. Med. (Baltim) 2016, 89, 104–111. [Google Scholar] [CrossRef] [Green Version]
- Erdfelder, E.; Faul, F.; Buchner, A. GPOWER: A general power analysis program. Behav. Res. Methods Instrum. Comput. 1996, 28, 1–11. [Google Scholar] [CrossRef]
- Göritz, A.S. Using Online Panels in Psychological Research. In Oxford Handbook of Internet Psychology; Oxford University Press: Oxford, UK, 2012; ISBN 9780191743771. [Google Scholar]
- Prolific Representative Samples on Prolific. Available online: https://researcher-help.prolific.co/hc/en-gb/articles/360019236753-Representative-Samples-on-Prolific (accessed on 19 October 2020).
- Brick, C.; McDowell, M.; Freeman, A.L.J. Risk communication in tables versus text: A registered report randomized trial on “fact boxes”. R. Soc. Open Sci. 2020, 7. [Google Scholar] [CrossRef] [Green Version]
- McDowell, M.; Rebitschek, F.G.; Gigerenzer, G.; Wegwarth, O. A Simple Tool for Communicating the Benefits and Harms of Health Interventions. MDM Policy Pract. 2016, 1, 238146831666536. [Google Scholar] [CrossRef]
- Schwartz, L.M.; Woloshin, S. The drug facts box: Improving the communication of prescription drug information. Proc. Natl. Acad. Sci. USA 2013, 110, 14069–14074. [Google Scholar] [CrossRef] [Green Version]
- Schneider, C.R.; Freeman, A.L.J.; Spiegelhalter, D.; van der Linden, S. The Effects of Quality of Evidence Communication on Perception of Public Health Information about COVID-19: Two Randomised Controlled Trials. 2021; (Manuscript submitted for publication). [Google Scholar]
- FDA. FDA Briefing Document: Moderna COVID-19 Vaccine. Available online: https://www.fda.gov/media/144434/download (accessed on 12 April 2021).
- European Medicines Agency. COVID-19 Vaccine Moderna. Available online: https://www.ema.europa.eu/en/documents/overview/covid-19-vaccine-moderna-epar-medicine-overview_en.pdf (accessed on 12 April 2021).
- European Medicines Agency. COVID-19 Vaccines: Development, Evaluation, Approval and Monitoring [Archived]. Available online: https://web.archive.org/web/20210101021942/https:/www.ema.europa.eu/en/human-regulatory/overview/public-health-threats/coronavirus-disease-covid-19/treatments-vaccines/covid-19-vaccines-development-evaluation-approval-monitoring (accessed on 26 February 2021).
- CDC. Understanding and Explaining mRNA COVID-19 Vaccines [Archived]. Available online: https://web.archive.org/web/20210106092135/https://www.cdc.gov/vaccines/covid-19/hcp/mrna-vaccine-basics.html (accessed on 26 February 2021).
- British Society for Immunology How Vaccines Work. Available online: https://www.immunology.org/celebrate-vaccines/public-engagement/guide-childhood-vaccinations/how-vaccines-work (accessed on 26 February 2021).
- O’Connor, A.M. Validation of a Decisional Conflict Scale. Med. Decis. Mak. 1995, 15, 25–30. [Google Scholar] [CrossRef]
- Quintana, D.S.; Williams, D.R. Bayesian alternatives for common null-hypothesis significance tests in psychiatry: A non-technical guide using JASP. BMC Psychiatry 2018, 18, 178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jarosz, A.F.; Wiley, J. What are the odds? A practical guide to computing and reporting bayes factors. J. Probl. Solving 2014, 7, 2–9. [Google Scholar] [CrossRef] [Green Version]
- Public Health England. What to Expect after Your COVID-19 Vaccination [Archived]. Available online: https://web.archive.org/web/20210224172559/https://www.gov.uk/government/publications/covid-19-vaccination-what-to-expect-after-vaccination/what-to-expect-after-your-covid-19-vaccination#can-you-give-covid-19-to-anyone-if-you-have-had-the-vaccine (accessed on 26 February 2021).
- Public Health England. Even if You’ve Had Your #COVID19 #Vaccine, It’s Important That You Continue to Follow National Restrictions. Available online: https://twitter.com/phe_uk/status/1348991695971643393 (accessed on 12 April 2021).
- Marcus, G.E.; Neuman, W.R.; MacKuen, M.B. Measuring Emotional Response: Comparing Alternative Approaches to Measurement. Polit. Sci. Res. Methods 2017, 5, 733–754. [Google Scholar] [CrossRef]
- Wood, T.; Porter, E. The Elusive Backfire Effect: Mass Attitudes’ Steadfast Factual Adherence. Polit. Behav. 2019, 41, 135–163. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention. Catalogue of Interventions Addressing Vaccine Hesitancy; European Centre for Disease Prevention: Stockholm, Sweden, 2017. [Google Scholar]
- Penţa, M.A.; Băban, A. Message Framing in Vaccine Communication: A Systematic Review of Published Literature. Health Commun. 2018, 33, 299–314. [Google Scholar] [CrossRef]
- O’Neill, J. The COVID-19 Vaccine, Informed Consent and the Recruitment of Volunteers. Available online: https://0-blogs-bmj-com.brum.beds.ac.uk/medical-ethics/2020/11/23/the-covid-19-vaccine-informed-consent-and-the-recruitment-of-volunteers (accessed on 12 April 2020).
- Larson, H.J.; Heymann, D.L. Public health response to influenza A(H1N1) as an opportunity to build public trust. JAMA J. Am. Med. Assoc. 2010, 303, 271–272. [Google Scholar] [CrossRef]
- Balog-Way, D.H.P.; McComas, K.A. COVID-19: Reflections on trust, tradeoffs, and preparedness. J. Risk Res. 2020, 23, 1–11. [Google Scholar] [CrossRef]
- Betsch, C.; Böhm, R.; Korn, L.; Holtmann, C. On the benefits of explaining herd immunity in vaccine advocacy. Nat. Hum. Behav. 2017, 1, 0056. [Google Scholar] [CrossRef]
- Betsch, C.; Böhm, R. Moral values do not affect prosocial vaccination. Nat. Hum. Behav. 2018, 2, 881–882. [Google Scholar] [CrossRef]
- Troiano, G.; Nardi, A. Vaccine hesitancy in the era of COVID-19. Public Health 2021. [Google Scholar] [CrossRef]
- Paterson, P.; Meurice, F.; Stanberry, L.R.; Glismann, S.; Rosenthal, S.L.; Larson, H.J. Vaccine hesitancy and healthcare providers. Vaccine 2016, 34, 6700–6706. [Google Scholar] [CrossRef] [Green Version]
- Ansell, B.; Bauer, M.W.; Gingrich, J.; Stilgoe, J. Coping with Covid: Two-Wave Survey. Available online: https://rpubs.com/benwansell/729135 (accessed on 10 March 2021).
- Nuki, P. Oxford’s Vaccine is a Positive British Success Story, Projecting Our Soft Power around the World. Available online: https://www.telegraph.co.uk/global-health/science-and-disease/oxfords-vaccine-positive-british-success-story-projecting-soft/ (accessed on 12 April 2021).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Condition | n | Content | Source | Length in Words (Incl. Tables) |
|---|---|---|---|---|
| Control | 412 | None | - | - |
| Factbox | 409 | Tables detailing incidence of COVID-19 and side effects in the vaccine and placebo arms of a large clinical trial, both as absolute numbers and percentages. Data was presented separately for trial participants aged 18–65 and aged 65+. A separate table reported rare side effects. | Adapted from US FDA [79] briefing document | 541 |
| Q&A | 417 | A Q&A format outlining the results of a clinical trial, including the absolute numbers of symptomatic COVID- 19 cases and vaccine efficacy. The text also noted several recommendations around the vaccine and known side effects with approximate frequencies, ranging from mild (e.g., pain at injection site, 1 in 10) to severe (facial swelling and facial paralysis, 1 in 1000). | European Medicines Agency [80] webpage | 708 |
| Approval | 443 | An overview of the standard and expedited COVID-19 vaccine review processes, highlighting the point that regulatory assessments of COVID-19 vaccine data were undertaken during the research and development process, as opposed after. A figure depicted this visually. | European Medicines Agency [81] webpage | 624 |
| Mechanism | 416 | A description of how vaccines induce immunity and in particular the mechanism by which mRNA vaccines produce antigens, noting the benefits of using mRNA, such scaling up vaccine production quickly. Two figures were included. | Extracts from US CDC [82] and British Society for Immunology [83] and a figure from Pfizer | 686 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kerr, J.R.; Freeman, A.L.J.; Marteau, T.M.; van der Linden, S. Effect of Information about COVID-19 Vaccine Effectiveness and Side Effects on Behavioural Intentions: Two Online Experiments. Vaccines 2021, 9, 379. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9040379
Kerr JR, Freeman ALJ, Marteau TM, van der Linden S. Effect of Information about COVID-19 Vaccine Effectiveness and Side Effects on Behavioural Intentions: Two Online Experiments. Vaccines. 2021; 9(4):379. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9040379
Chicago/Turabian StyleKerr, John R., Alexandra L. J. Freeman, Theresa M. Marteau, and Sander van der Linden. 2021. "Effect of Information about COVID-19 Vaccine Effectiveness and Side Effects on Behavioural Intentions: Two Online Experiments" Vaccines 9, no. 4: 379. https://0-doi-org.brum.beds.ac.uk/10.3390/vaccines9040379