
Radiographic Evaluation of Bone Remodeling after Additively Manufactured Subperiosteal Jaw Implantation (AMSJI) in the Maxilla: A One-Year Follow-Up Study

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dahl, C. If the opportunity for implantation in the jaw of metal skeletons as the base or retention for fixed or removable dentures. Odontol. Tidskr. 1943, 51, 440–449. [Google Scholar]
- Linkow, L.I.; Ghalili, R. Critical design errors in maxillary subperiosteal implants. J. Oral Implant. 1998, 24, 198–205. [Google Scholar] [CrossRef]
- Fretwurst, T.; Nack, C.; Al-Ghrairi, M.; Raguse, J.; Stricker, A.; Schmelzeisen, R.; Nelson, K.; Nahles, S. Long-term retrospective evaluation of the peri-implant bone level in onlay grafted patients with iliac bone from the anterior superior iliac crest. J. Cranio-Maxillofac. Surg. 2015, 43, 956–960. [Google Scholar] [CrossRef] [PubMed]
- Duttenhoefer, F.; Nack, C.; Doll, C.; Raguse, J.-D.; Hell, B.; Stricker, A.; Nelson, K.; Nahles, S. Long-term peri-implant bone level changes of non-vascularized fibula bone grafted edentulous patients. J. Cranio-Maxillofac. Surg. 2015, 43, 611–615. [Google Scholar] [CrossRef] [PubMed]
- Rosén, A.; Gynther, G. Implant Treatment without Bone Grafting in Edentulous Severely Resorbed Maxillas: A Long-Term Follow-Up Study. J. Oral Maxillofac. Surg. 2007, 65, 1010–1016. [Google Scholar] [CrossRef]
- Kim, Y.-K.; Kim, S.-G.; Kim, B.-S.; Jeong, K.-I. Resorption of bone graft after maxillary sinus grafting and simultaneous implant placement. J. Korean Assoc. Oral Maxillofac. Surg. 2014, 40, 117–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mommaerts, M. Additively manufactured sub-periosteal jaw implants. Int. J. Oral Maxillofac. Surg. 2017, 46, 938–940. [Google Scholar] [CrossRef]
- Mommaerts, M. Evolutionary steps in the design and biofunctionalization of the additively manufactured sub-periosteal jaw implant ‘AMSJI’ for the maxilla. Int. J. Oral Maxillofac. Surg. 2018, 48, 108–114. [Google Scholar] [CrossRef] [Green Version]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Bodine, R.L. Evaluation of 27 mandibular subperiosteal implant dentures after 15 to 22 years. J. Prosthet. Dent. 1974, 32, 188–197. [Google Scholar] [CrossRef]
- Young, L.; Michel, J.D.; Moore, D.J. A twenty-year evaluation of subperiosteal implants. J. Prosthet. Dent. 1983, 49, 690–694. [Google Scholar] [CrossRef]
- Yanase, R.; Bodine, R.; Tom, J.; White, S. The mandibular subperiosteal implant denture: A prospective survival study. J. Prosthet. Dent. 1994, 71, 369–374. [Google Scholar] [CrossRef]
- Albrektsson, T.; Sennerby, L. State of the art in oral implants. J. Clin. Periodontol. 1991, 18, 474–481. [Google Scholar] [CrossRef] [PubMed]
- Bodine, R.L.; Yanase, R.T.; Bodine, A. Forty years of experience with subperiosteal implant dentures in 41 edentulous patients. J. Prosthet. Dent. 1996, 75, 33–44. [Google Scholar] [CrossRef]
- Schou, S.; Pallesen, L.; Pedersen, C.S.; Fibæk, B.; Hjørting-Hansen, E. A 41-year history of a mandibular subperiosteal implant. Clin. Oral Implant. Res. 2000, 11, 171–178. [Google Scholar] [CrossRef]
- Van Steenberghe, D.; Branemark, P.-I.; Quirynen, M.; De Mars, G.; Naert, I. The rehabilitation of oral defects by osseointegrated implants. J. Clin. Periodontol. 1991, 18, 488–493. [Google Scholar] [CrossRef]
- Esposito, M.; Grusovin, M.G.; Felice, P.; Karatzopoulos, G.; Worthington, H.V.; Coulthard, P. The efficacy of horizontal and vertical bone augmentation procedures for dental implants—A Cochrane systematic review. Eur. J. Oral Implantol. 2009, 2, 167–184. [Google Scholar] [CrossRef]
- Clark, D.; Barbu, H.; Lorean, A.; Mijiritsky, E.; Levin, L. Incidental findings of implant complications on postimplantation CBCTs: A cross-sectional study. Clin. Implant. Dent. Relat. Res. 2017, 19, 776–782. [Google Scholar] [CrossRef]
- Van Doorne, L.; Fonteyne, E.; Matthys, C.; Bronkhorst, E.; Meijer, G.; De Bruyn, H. Longitudinal Oral Health-Related Quality of Life in maxillary mini dental implant overdentures after 3 years in function. Clin. Oral Implant. Res. 2020, 32, 23–36. [Google Scholar] [CrossRef]
- Chiapasco, M.; Zaniboni, M.; Boisco, M. Augmentation procedures for the rehabilitation of deficient edentulous ridges with oral implants. Clin. Oral Implant. Res. 2006, 17, 136–159. [Google Scholar] [CrossRef]
- Gonzalez-Garcia, R.; Naval-Gias, L.; MunozGuerra, M.F.; Sastre-Perez, J.; Rodriguez-Campo, F.J.; Gil-Diez-Usandizaga, J.L. Preprosthetic and implantological surgery in patients with severe maxillary atrophy. Med. Oral Patol. Oral Cir. Bucal. 2005, 10, 343–354. [Google Scholar]
- Aghaloo, T.L.; Misch, C.; Lin, G.-H.; Iacono, V.J.; Wang, H.-L. Bone Augmentation of the Edentulous Maxilla for Implant Placement: A Systematic Review. Int. J. Oral Maxillofac. Implant. 2017, 31, s19–s30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simon, B.I.; Chiang, T.F.; Drew, H.J. Alternative to the gold standard for alveolar ridge augmentation: Tenting screw technology. Quintessence Int. 2010, 41, 379–386. [Google Scholar] [PubMed]
- Alérico, F.A.; Bernardes, S.R.; Fontao, F.G.K.; Diez, G.F.; Alérico, J.H.S.; Claudino, M. Prospective Tomographic Evaluation of Autogenous Bone Resorption Harvested From Mandibular Ramus in Atrophic Maxilla. J. Craniofacial Surg. 2014, 25, e543–e546. [Google Scholar] [CrossRef]
- Gultekin, B.A.; Bedeloglu, E.; Kose, T.E.; Mijiritsky, E. Comparison of Bone Resorption Rates after Intraoral Block Bone and Guided Bone Regeneration Augmentation for the Reconstruction of Horizontally Deficient Maxillary Alveolar Ridges. BioMed Res. Int. 2016, 2016, 4987437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johansson, B.; Grepe, A.; Wannfors, K.; Hirsch, J.M. A clinical study of changes in the volume of bone grafts in the atrophic maxilla. Dentomaxillofac. Radiol. 2001, 30, 157–161. [Google Scholar] [CrossRef]
- Fourcade, C.; Lesclous, P.; Guiol, J. Assignment of autogenous bone grafts for reconstruction of the alveolar ridge before implant placement. J. Oral Med. Oral Surg. 2019, 25, 1. [Google Scholar] [CrossRef] [Green Version]
- Von Arx, T.; Buser, D. Horizontal ridge augmentation using autogenous block grafts and the guided bone regeneration technique with collagen membranes: A clinical study with 42 patients. Clin. Oral Implant. Res. 2006, 17, 359–366. [Google Scholar] [CrossRef]
- Maiorana, C.; Beretta, M.; Salina, S.; Santoro, F. Reduction of autogenous bone graft resorption by means of bio-oss coverage: A prospective study. Int. J. Periodontics Restor. Dent. 2005, 25, 19–25. [Google Scholar]
- Khojasteh, A.; Motamedian, S.R.; Khojaste, M. Success rate of implants placed in autogenous bone blocks versus allogenic bone blocks: A systematic literature review. Ann. Maxillofac. Surg. 2016, 6, 78–90. [Google Scholar] [CrossRef] [Green Version]
- Al-Dajani, M. Incidence, Risk Factors, and Complications of Schneiderian Membrane Perforation in Sinus Lift Surgery. Implant. Dent. 2016, 25, 409–415. [Google Scholar] [CrossRef]
- Baj, A.; Trapella, G.; Lauritano, D.; Candotto, V.; Mancini, G.E.; Giannì, A.B. An overview on bone reconstruction of atrophic maxilla: Success parameters and critical issues. J. Biol. Regul. Homeost. Agents 2016, 30 (Suppl. 1), 209–215. [Google Scholar]
- Bortoluzzi, M.C.; Cecconello, R.; Derech, E.D.; Fabris, V.; Manfro, R. Comparative study of immediately inserted dental implants in sinus lift: 24 months of follow-up. Ann. Maxillofac. Surg. 2014, 4, 30–33. [Google Scholar] [CrossRef]
- Infante, A.; Rodríguez, C.I. Osteogenesis and aging: Lessons from mesenchymal stem cells. Stem Cell Res. Ther. 2018, 9, 244. [Google Scholar] [CrossRef] [Green Version]
- Moy, P.K.; Aghaloo, T. Risk factors in bone augmentation procedures. Periodontol. 2000 2019, 81, 76–90. [Google Scholar] [CrossRef]
- O’Connell, J.; Murphy, C.; Ikeagwuani, O.; Adley, C.; Kearns, G. The fate of titanium miniplates and screws used in maxillofacial surgery: A 10 year retrospective study. Int. J. Oral Maxillofac. Surg. 2009, 38, 731–735. [Google Scholar] [CrossRef]
- Cornelis, M.A.; Scheffler, N.R.; Mahy, P.; Siciliano, S.; De Clerck, H.J.; Tulloch, J.C. Modified Miniplates for Temporary Skeletal Anchorage in Orthodontics: Placement and Removal Surgeries. J. Oral Maxillofac. Surg. 2008, 66, 1439–1445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lavstedt, S.; Bolin, A.; Henrikson, C.O.; Carstensen, J. Proximal alveolar bone loss in a longitudinal radiographic investigation I. Methods of measurement and partial recording. Acta Odontol. Scand. 1986, 44, 149–157. [Google Scholar] [CrossRef] [PubMed]
- Bergström, J.; Henrikson, C.O. Quantitative longitudinal study of alveolar bone tissue in man. J. Periodontal Res. 1970, 5, 237–247. [Google Scholar] [CrossRef] [PubMed]
- Wyatt, C.C. The effect of prosthodontic treatment on alveolar bone loss: A review of the literature. J. Prosthet. Dent. 1998, 80, 362–366. [Google Scholar] [CrossRef]
- Kovacić, I.; Celebić, A.; Zlatarić, D.K. Decreasing of residual alveolar ridge height in complete denture wearers. A five year follow up study. Coll. Antropol. 2010, 34, 1051–1056. [Google Scholar]
- Koodaryan, R.; Hafezeqoran, A. Evaluation of Implant Collar Surfaces for Marginal Bone Loss: A Systematic Review and Meta-Analysis. BioMed Res. Int. 2016, 2016, 4987526. [Google Scholar] [CrossRef] [Green Version]
- Atwood, D.A.; Coy, W.A. Clinical, cephalometric, and densitometric study of reduction of residual ridges. J. Prosthet. Dent. 1971, 26, 280–295. [Google Scholar] [CrossRef]
- Yaffe, A.; Fine, N.; Binderman, I. Regional Accelerated Phenomenon in the Mandible Following Mucoperiosteal Flap Surgery. J. Periodontol. 1994, 65, 79–83. [Google Scholar] [CrossRef]
- Job, S.; Bhat, V.; Naidu, E.M. In vivo evaluation of crestal bone heights following implant placement with ‘flapless’ and ‘with-flap’ techniques in sites of immediately loaded implants. Indian J. Dent. Res. 2008, 19, 320–325. [Google Scholar] [CrossRef] [PubMed]
- Merheb, J.; Vercruyssen, M.; Coucke, W.; Beckers, L.; Teughels, W.; Quirynen, M. The fate of buccal bone around dental implants. A 12-month postloading follow-up study. Clin. Oral Implant. Res. 2016, 28, 103–108. [Google Scholar] [CrossRef]
- Nobuto, T.; Suwa, F.; Kono, T.; Taguchi, Y.; Takahashi, T.; Kanemura, N.; Terada, S.; Imai, H. Microvascular Response in the Periosteum Following Mucoperiosteal Flap Surgery in Dogs: Angiogenesis and Bone Resorption and Formation. J. Periodontol. 2005, 76, 1346–1353. [Google Scholar] [CrossRef] [PubMed]
- Merheb, J.; Quirynen, M.; Teughels, W. Critical buccal bone dimensions along implants. Periodontol. 2000 2014, 66, 97–105. [Google Scholar] [CrossRef]
- Maier, F.-M. Initial Crestal Bone Loss Af ter Implant Placement with Flapped or Flapless Surgery—A Prospective Cohort Study. Int. J. Oral Maxillofac. Implant. 2016, 31, 876–883. [Google Scholar] [CrossRef] [Green Version]
- Engelbrecht, W.P.; Fourie, Z.; Damstra, J.; Gerrits, P.O.; Ren, Y. The influence of the segmentation process on 3D measurements from cone beam computed tomography-derived surface models. Clin. Oral Investig. 2013, 17, 1919–1927. [Google Scholar] [CrossRef]
- Yatabe, M.; Prieto, J.C.; Styner, M.; Zhu, H.; Ruellas, A.C.; Paniagua, B.; Budin, F.; Benavides, E.; Shoukri, B.; Michoud, L.; et al. 3D superimposition of craniofacial imaging—The utility of multicentre collaborations. Orthod. Craniofacial Res. 2019, 22, 213–220. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
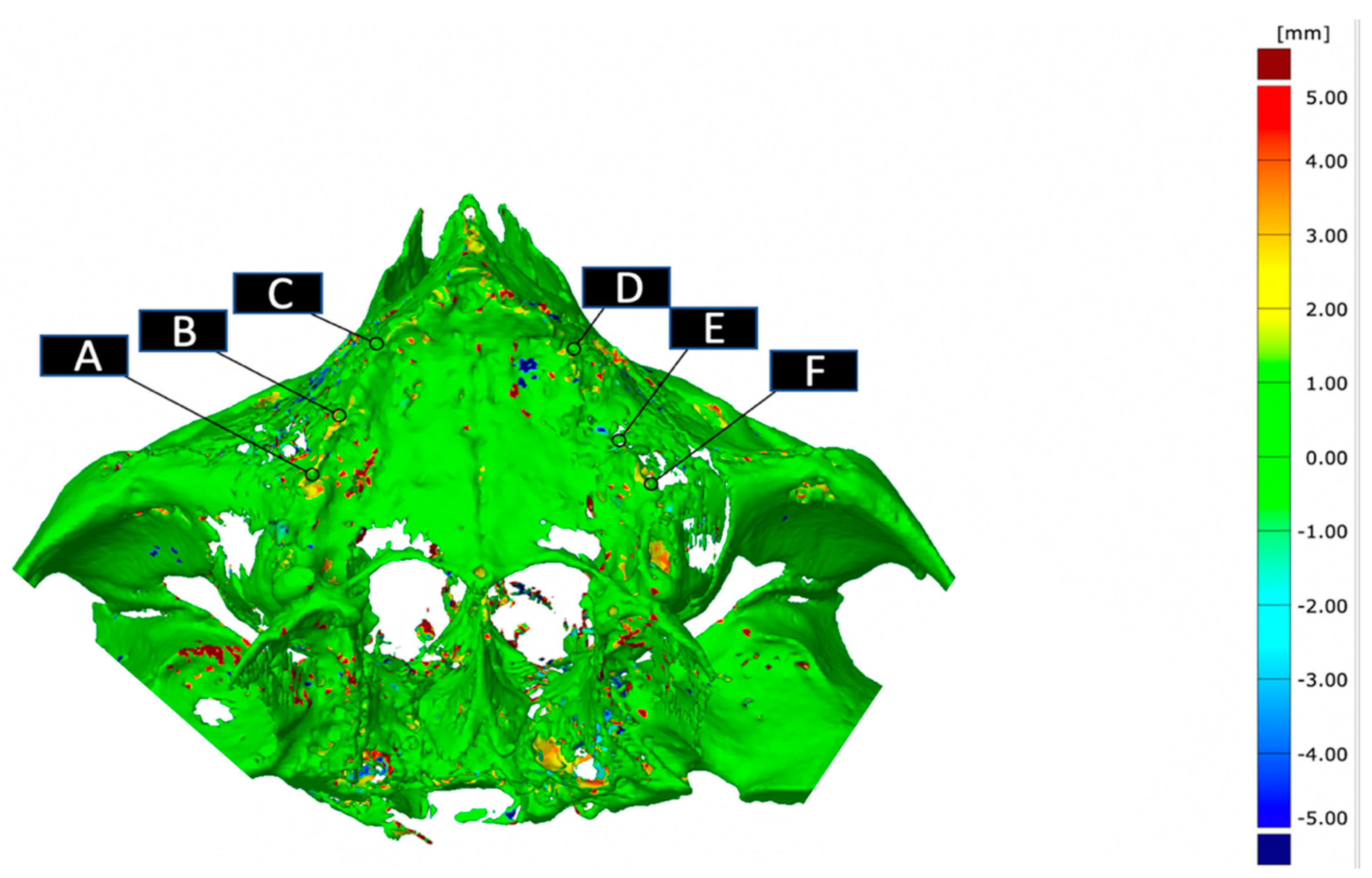
| AMSJI | Point | ∆ Each Point T1–T2 (SD) | ∆ Side T1–T2 (SD) | ∆ AMSJI Total T1–T2 (SD) |
|---|---|---|---|---|
| A | −0.29 (1.04) | −0.24 (0.85) | −0.26 (0.65) | |
| Right | B | −0.24 (0.94) | ||
| C | −0.18 (0.80) | |||
| D | −0.33 (0.89) | −0.27 (0.53) | ||
| Left | E | −0.46 (0.57) | ||
| F | −0.050 (0.55) |
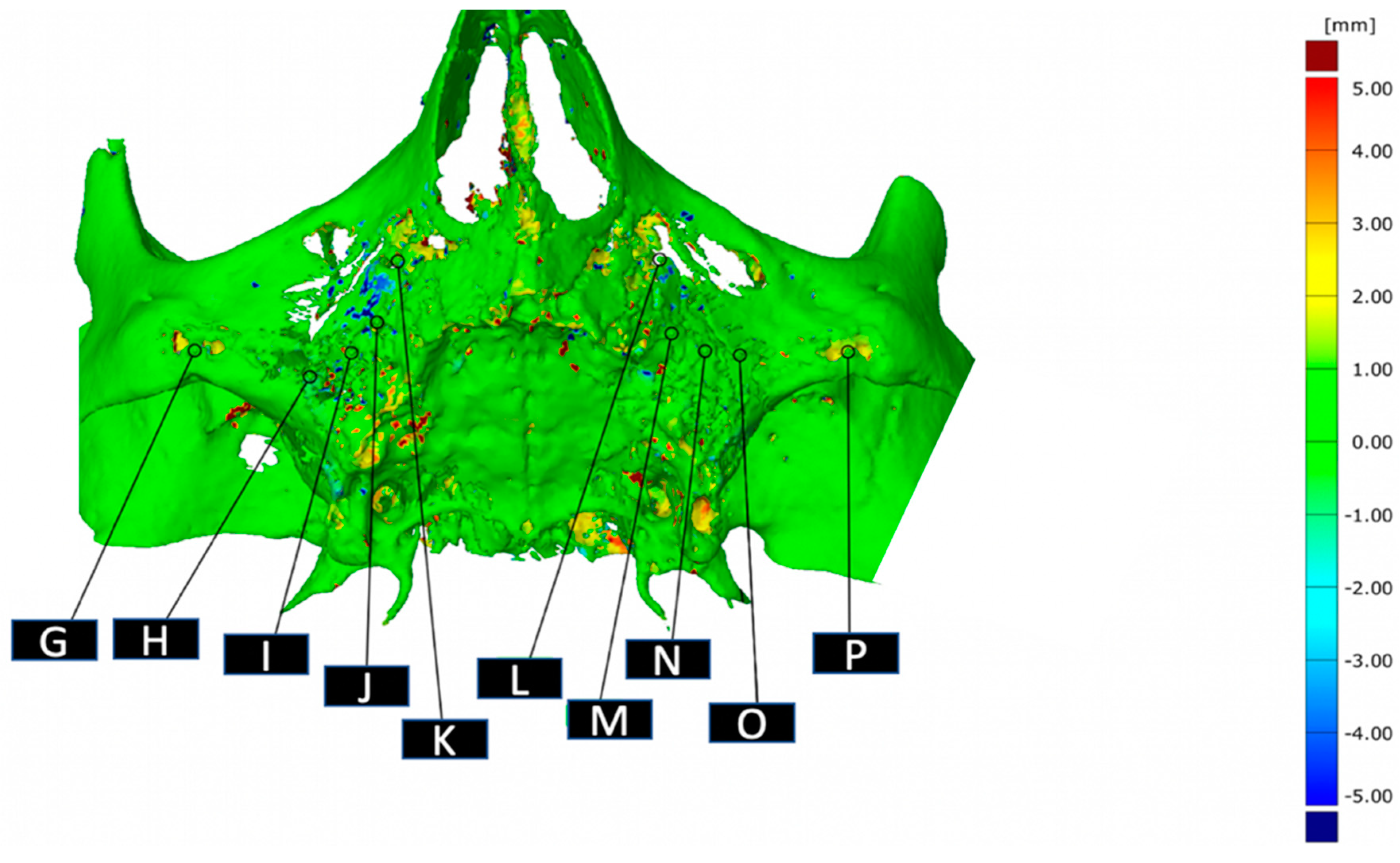
| AMSJI | Point | ∆ Each Point T1–T2 (SD) | ∆ Side T1–T2 (SD) | ∆ AMSJI Total T1–T2 (SD) |
|---|---|---|---|---|
| G | 0.32 (0.67) | −0.060 (0.40) | −0.088 (0.29) | |
| H | −0.040 (1.46) | |||
| Right | I | −0.38 (0.71) | ||
| J | −0.18 (0.57) | |||
| K | −0.03 (0.57) | |||
| L | −0.18 (0.41) | −0.11 (0.26) | ||
| M | −0.44 (0.47) | |||
| Left | N | 0.010 (0.59) | ||
| O | 0.060 (0.75) | |||
| P | −0.030 (0.58) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Van den Borre, C.; Rinaldi, M.; De Neef, B.; Loomans, N.A.J.; Nout, E.; Van Doorne, L.; Naert, I.; Politis, C.; Schouten, H.; Klomp, G.; et al. Radiographic Evaluation of Bone Remodeling after Additively Manufactured Subperiosteal Jaw Implantation (AMSJI) in the Maxilla: A One-Year Follow-Up Study. J. Clin. Med. 2021, 10, 3542. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10163542
Van den Borre C, Rinaldi M, De Neef B, Loomans NAJ, Nout E, Van Doorne L, Naert I, Politis C, Schouten H, Klomp G, et al. Radiographic Evaluation of Bone Remodeling after Additively Manufactured Subperiosteal Jaw Implantation (AMSJI) in the Maxilla: A One-Year Follow-Up Study. Journal of Clinical Medicine. 2021; 10(16):3542. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10163542
Chicago/Turabian StyleVan den Borre, Casper, Marco Rinaldi, Björn De Neef, Natalie A. J. Loomans, Erik Nout, Luc Van Doorne, Ignace Naert, Constantinus Politis, Hylke Schouten, Geert Klomp, and et al. 2021. "Radiographic Evaluation of Bone Remodeling after Additively Manufactured Subperiosteal Jaw Implantation (AMSJI) in the Maxilla: A One-Year Follow-Up Study" Journal of Clinical Medicine 10, no. 16: 3542. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10163542