
A Multi-Criteria Assessment Strategy for 3D Printed Porous Polyetheretherketone (PEEK) Patient-Specific Implants for Orbital Wall Reconstruction

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
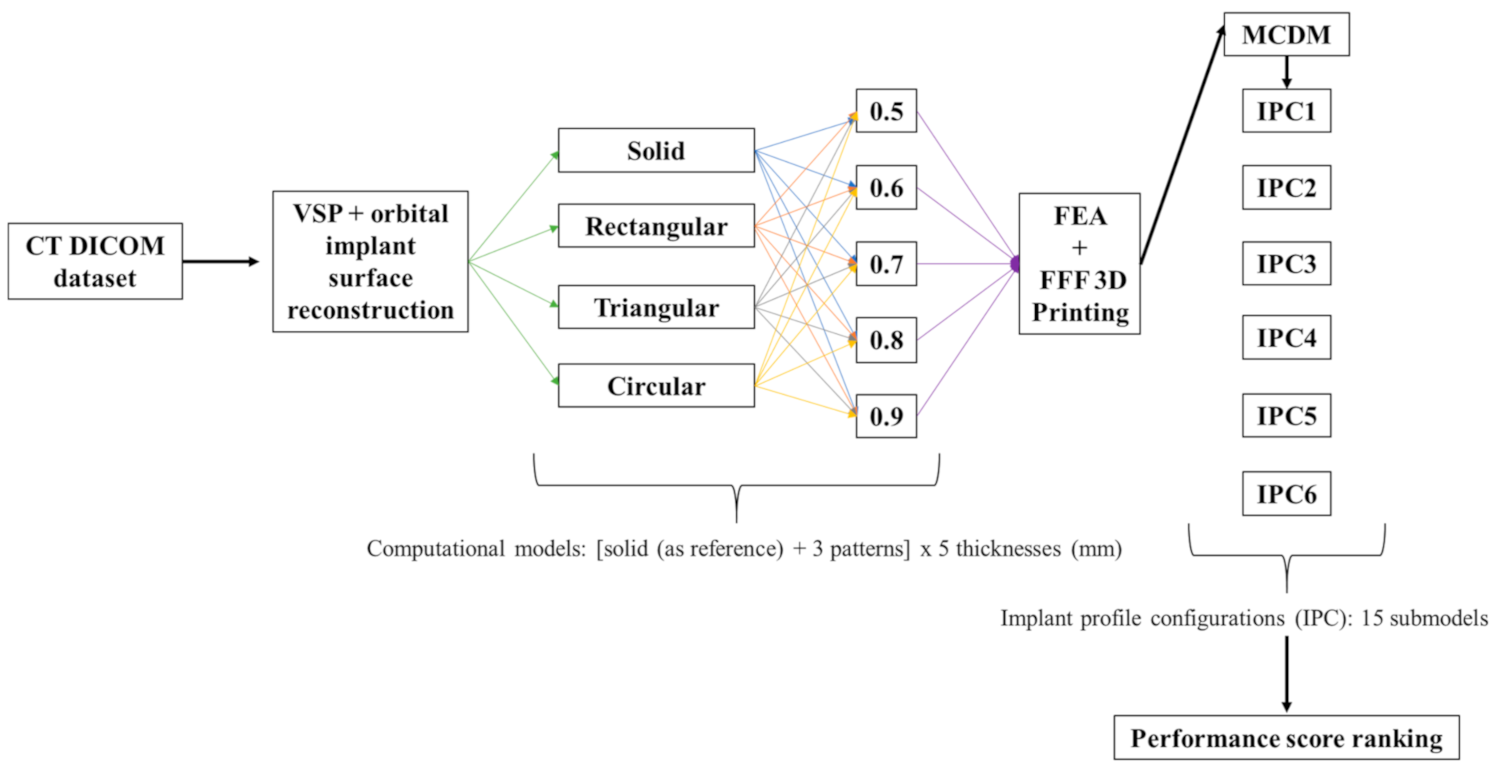
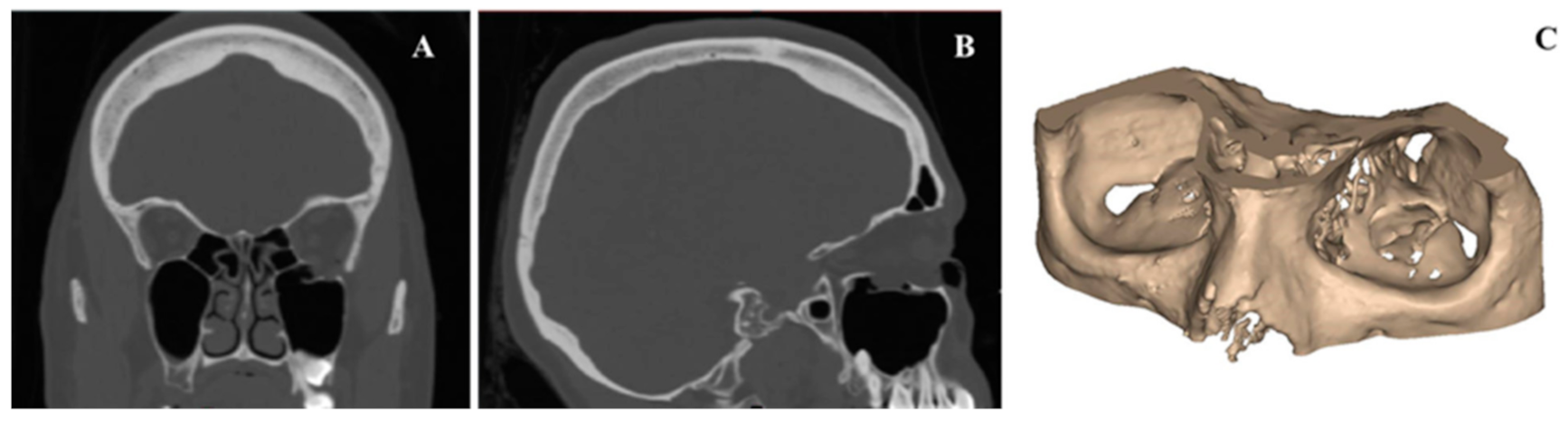
2.1. Medical Image Processing and Modeling of Patient-Specific Orbital Implants
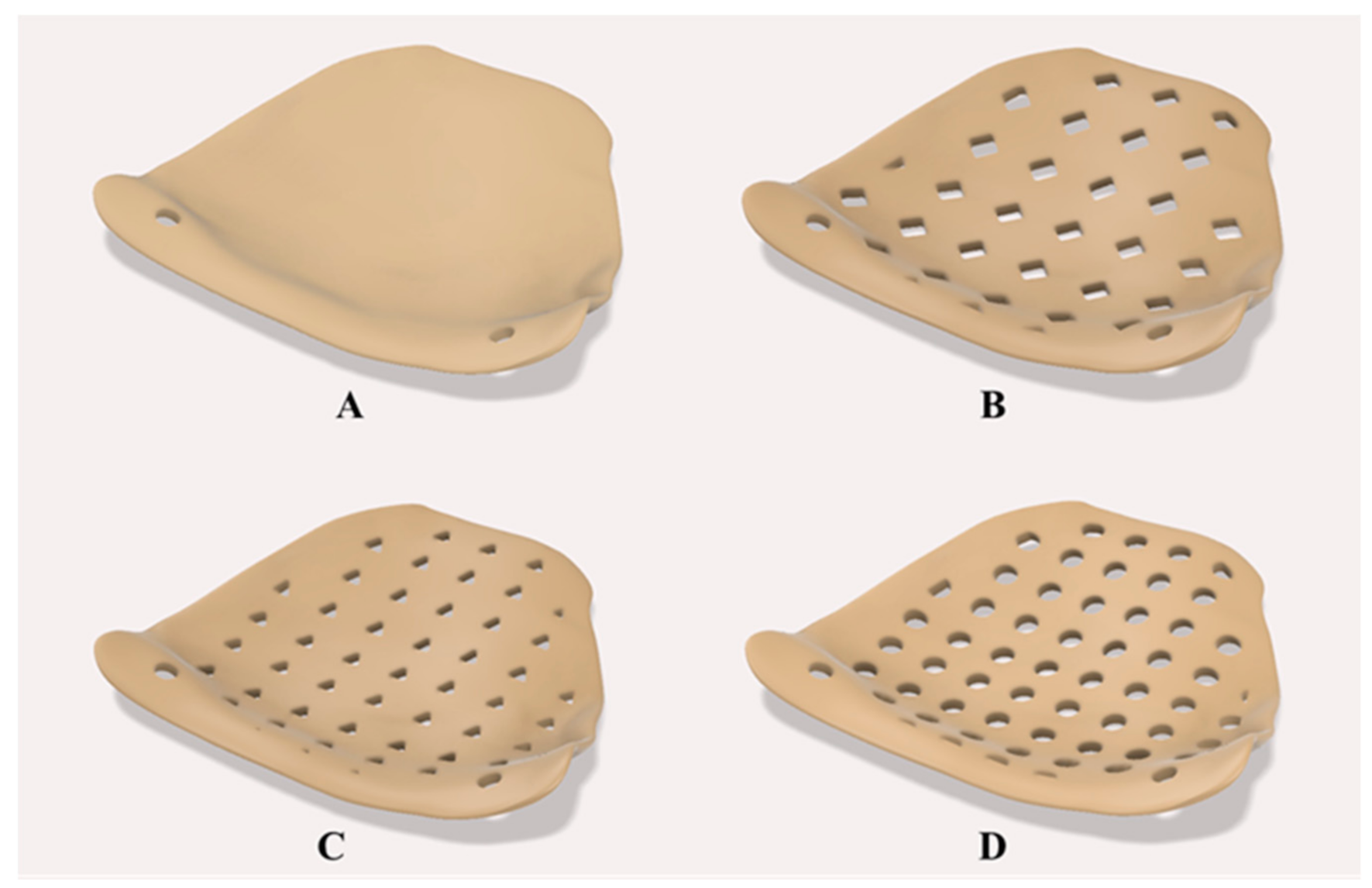
2.2. Construction of PEEK Orbital Mesh Implant Design Variants
2.3. Construction of Computational Models
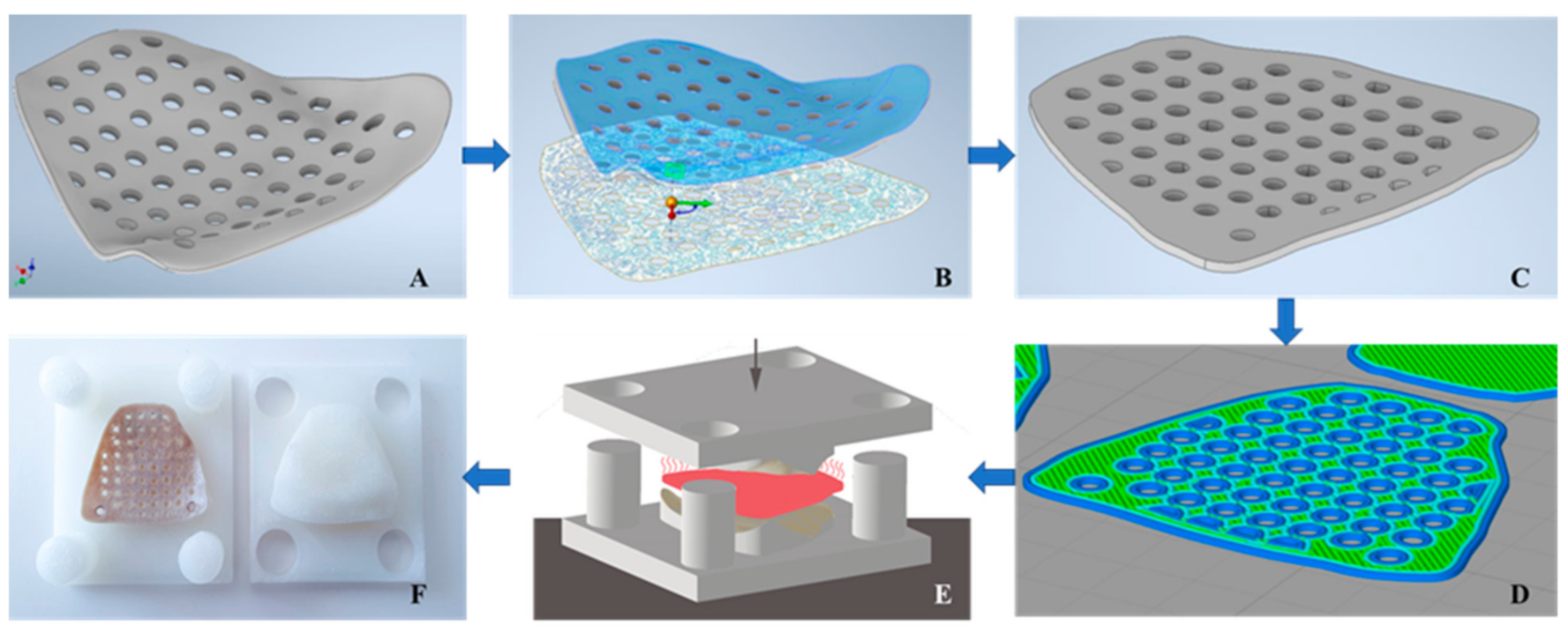
2.4. Additive Manufacturing Processes for PEEK Orbital Mesh Implants
2.5. Multi-Criteria Decision-Making (MCDM)—Configuration Assessment
3. Results
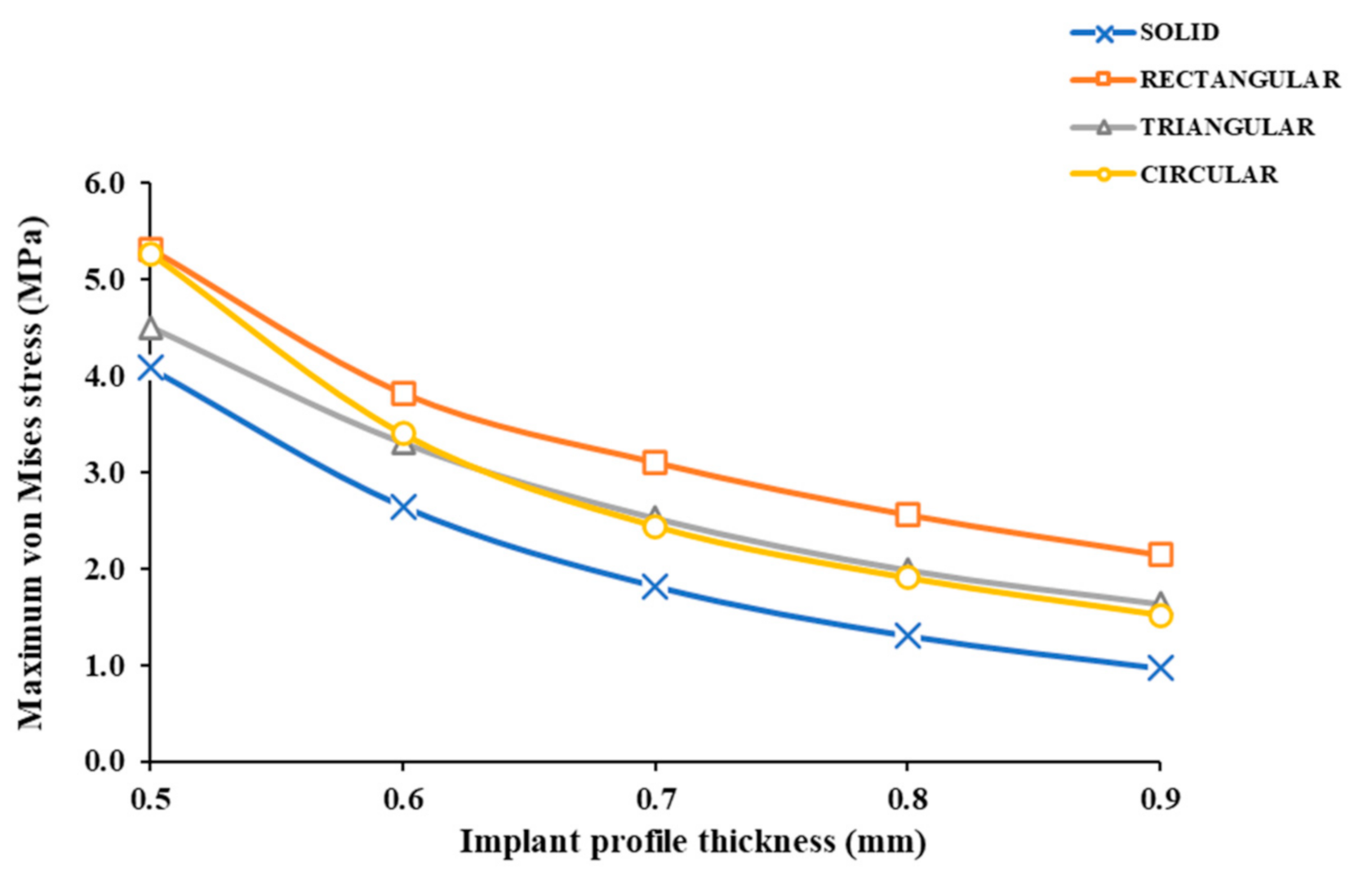
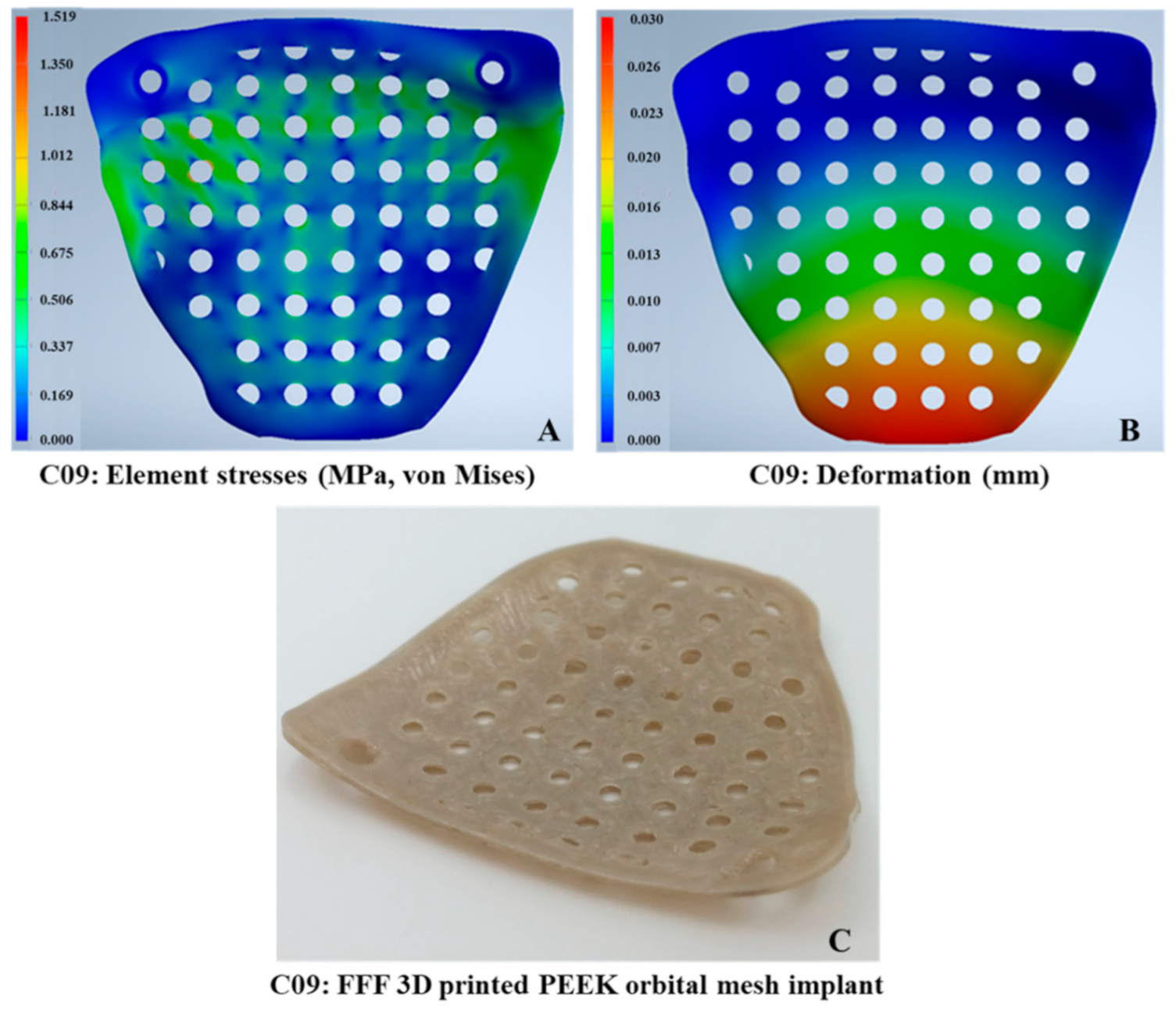
3.1. Stress Intensity Patterns in the Thin PEEK Orbital Mesh Implants
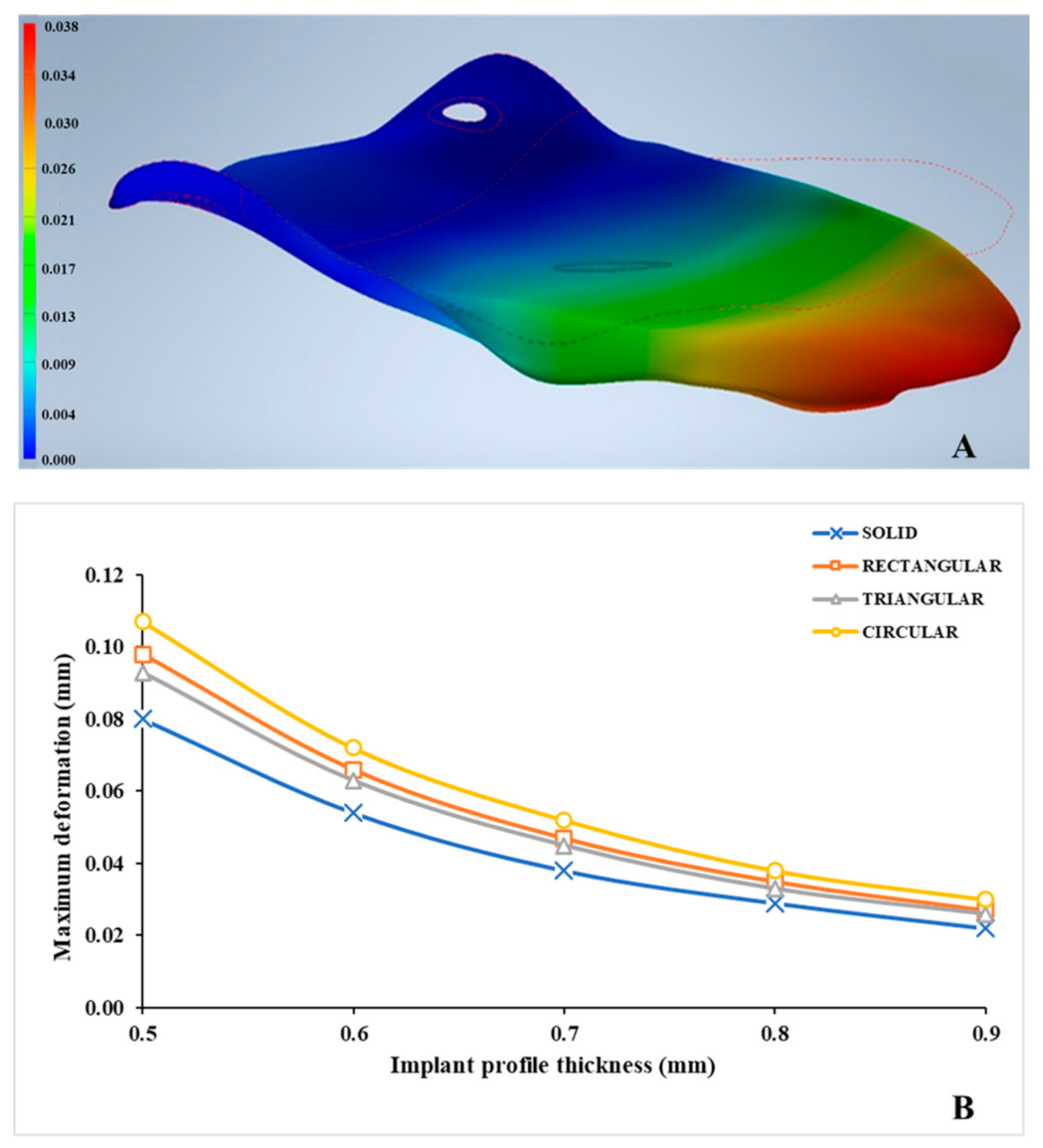
3.2. Deformation Patterns in the Thin PEEK Orbital Mesh Implants
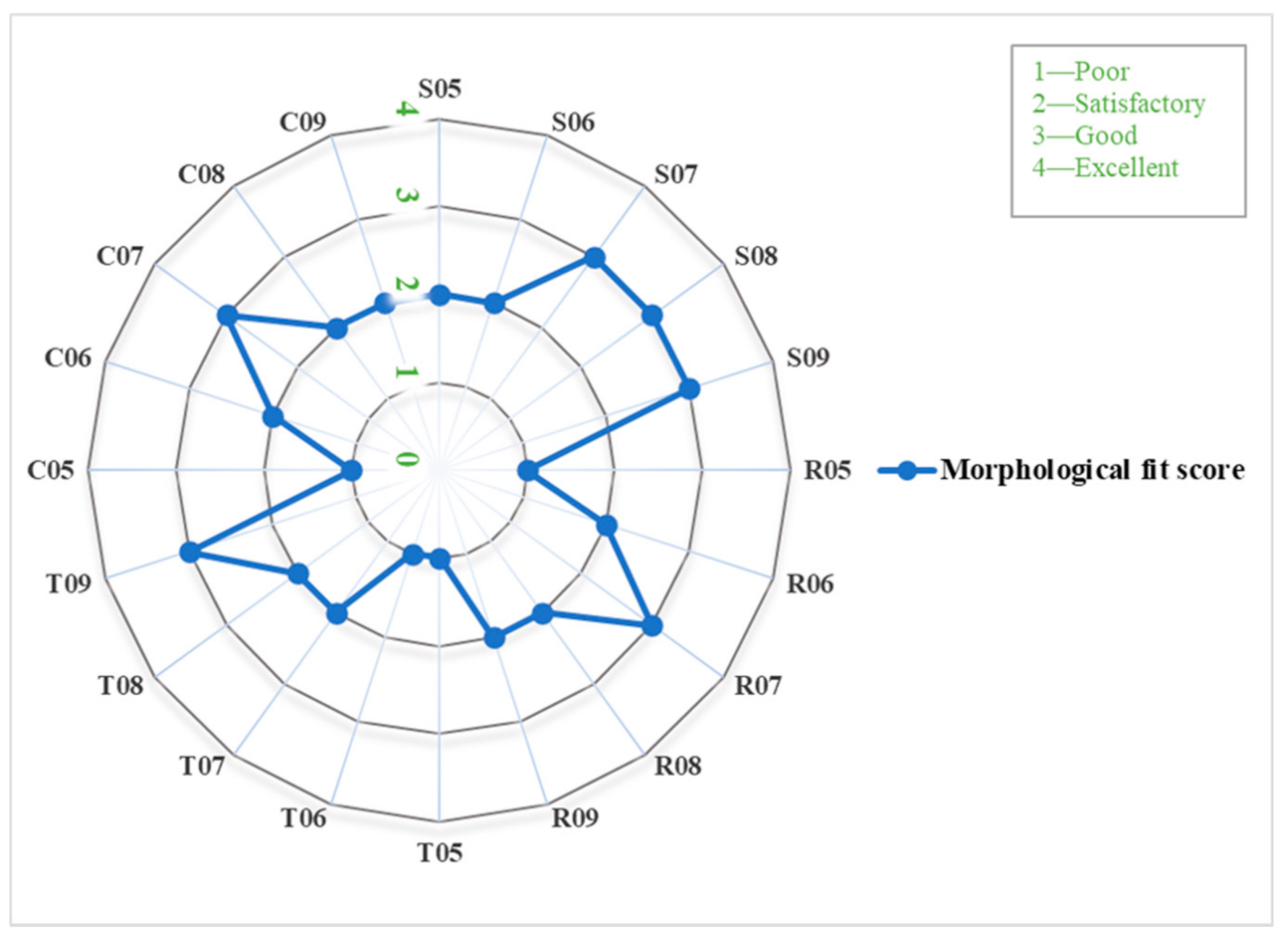
3.3. Morphological Assessment of the Thin PEEK Orbital Mesh Implants
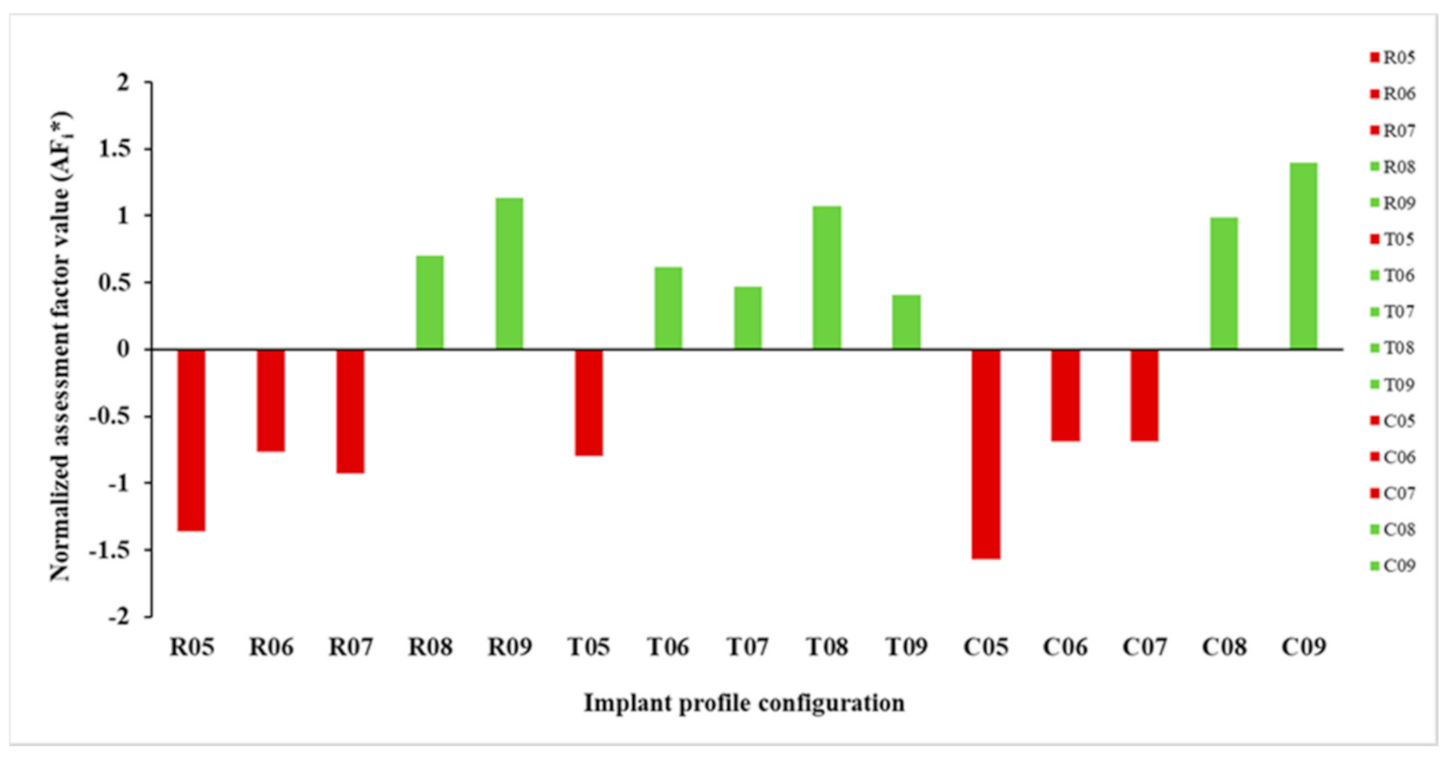
3.4. Configuration Assessment Using Multi-Criteria Decision Making (MCDM) Approach
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviation
| 2D | Two-Dimensional |
| 3D | Three-Dimensional |
| AF | Assessment Factor |
| AM | Additive Manufacturing |
| ASTM | American Society for Testing and Materials |
| CAD | Computer-Aided Design |
| CAM | Computer-Aided Manufacturing |
| CAS | Computer-Assisted Surgery |
| CT | Computed Tomography |
| DfAM | Design for Additive Manufacturing |
| DICOM | Digital Imaging and Communications in Medicine |
| DOF | Degree of Freedom |
| FE | Finite Element |
| FFF | Fused Filament Fabrication |
| ISO | International Organization for Standardization |
| MCDM | Multi-Criteria Decision Making |
| PEEK | Polyetheretherketone |
| POC | Point-of-Care |
| PSIs | Patient Specific Implants |
| ROI | Region of Interest |
| SD | Standard Deviation |
| STL | Standard Tessellation Language |
| VSP | Virtual Surgical Planning |
| WSM | Weight Sum Method |
References
- Smith, B.; Regan, W.F., Jr. Blow-out fracture of the orbit; mechanism and correction of internal orbital fracture. Am. J. Ophthalmol. 1957, 44, 733–739. [Google Scholar] [CrossRef]
- Ahmad Nasir, S.; Ramli, R.; Abd Jabar, N. Predictors of enophthalmos among adult patients with pure orbital blowout fractures. PLoS ONE 2018, 13, e0204946. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hwang, K.; You, S.H.; Sohn, I.A. Analysis of orbital bone fractures: A 12-year study of 391 patients. J. Craniofac. Surg. 2009, 20, 1218–1223. [Google Scholar] [CrossRef]
- Boyette, J.R.; Pemberton, J.D.; Bonilla-Velez, J. Management of orbital fractures: Challenges and solutions. Clin. Ophthalmol. 2015, 9, 2127–2137. [Google Scholar] [CrossRef] [Green Version]
- Parameswaran, A.; Marimuthu, M.; Panwar, S.; Hammer, B. Orbital Fractures. In Oral and Maxillofacial Surgery for the Clinician, 1st ed.; Bonanthaya, K., Panneerselvam, E., Manuel, S., Kumar, V.V., Rai, A., Eds.; Springer: Singapore, 2021; pp. 1201–1250. [Google Scholar]
- Gunarajah, D.R.; Samman, N. Biomaterials for repair of orbital floor blowout fractures: A systematic review. J. Oral Maxillofac. Surg. 2013, 71, 550–570. [Google Scholar] [CrossRef]
- Baumann, A.; Sinko, K.; Dorner, G. Late reconstruction of the orbit with patient-specific implants using computer-aided planning and navigation. J. Oral Maxillofac. Surg. 2015, 73, S101–S106. [Google Scholar] [CrossRef]
- Hwang, K.; Kim, D.H. Comparison of the supporting strength of a poly-L-lactic acid sheet and porous polyethylene (Medpor) for the reconstruction of orbital floor fractures. J. Craniofac. Surg. 2010, 21, 847–853. [Google Scholar] [CrossRef] [PubMed]
- Romano, J.J.; Iliff, N.T.; Manson, P.N. Use of Medpor porous polyethylene implants in 140 patients with facial fractures. J. Craniofac. Surg. 1993, 4, 142–147. [Google Scholar] [CrossRef]
- Mommaerts, M.; Büttner, M.; Vercruysse, H., Jr.; Wauters, L.; Beerens, M. Orbital wall reconstruction with two-piece puzzle 3d printed implants: Technical note. Craniomaxillofac. Trauma Reconstr. 2016, 9, 55–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dubois, L.; Jansen, J.; Schreurs, R.; Saeed, P.; Beenen, L.; Maal, T.J.; Gooris, P.J.; Becking, A.G. Predictability in orbital reconstruction: A human cadaver study. Part I: Endoscopic-assisted orbital reconstruction. J. Craniomaxillofac. Surg. 2015, 43, 2034–2041. [Google Scholar] [CrossRef]
- Kunz, C.; Audigé, L.; Cornelius, C.; Buitrago-Téllez, C.; Rudderman, R.; Prein, J. The comprehensive AOCMF classification system: Orbital fractures—Level 3 tutorial. Craniomaxillofac. Trauma Reconstr. 2014, 7, S92–S102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dubois, L.; Schreurs, R.; Jansen, J.; Maal, T.J.; Essig, H.; Gooris, P.J.; Becking, A.G. Predictability in orbital reconstruction: A human cadaver study. Part II: Navigation-assisted orbital reconstruction. J. Craniomaxillofac. Surg. 2015, 43, 2042–2049. [Google Scholar] [CrossRef]
- Dubois, L.; Essig, H.; Schreurs, R.; Jansen, J.; Maal, T.J.; Gooris, P.J.; Becking, A.G. Predictability in orbital reconstruction. A human cadaver study, part III: Implant-oriented navigation for optimized reconstruction. J. Craniomaxillofac. Surg. 2015, 43, 2050–2056. [Google Scholar] [CrossRef] [PubMed]
- Schreurs, R.; Dubois, L.; Becking, A.G.; Maal, T.J. Quantitative Assessment of Orbital Implant Position—A Proof of Concept. PLoS ONE 2016, 11, e0150162. [Google Scholar] [CrossRef]
- Dubois, L.; Steenen, S.A.; Gooris, P.J.J.; Mourits, M.P.; Becking, A.G. Controversies in orbital reconstruction-II. Timing of post-traumatic orbital reconstruction: A systematic review. Int. J. Oral Maxillofac. Surg. 2015, 44, 433–440. [Google Scholar] [CrossRef] [PubMed]
- Gander, T.; Essig, H.; Metzler, P.; Lindhorst, D.; Dubois, L.; Rücker, M.; Schumann, P. Patient specific implants (PSI) in reconstruction of orbital floor and wall fractures. J. Craniomaxillofac. Surg. 2015, 43, 126–130. [Google Scholar] [CrossRef] [Green Version]
- Rana, M.; Chui, C.H.; Wagner, M.; Zimmerer, R.; Rana, M.; Gellrich, N.C. Increasing the accuracy of orbital reconstruction with selective laser-melted patient-specific implants combined with intraoperative navigation. J. Oral Maxillofac. Surg. 2015, 73, 1113–1118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chepurnyi, Y.; Chernogorskyi, D.; Kopchak, A.; Petrenko, O. Clinical efficacy of peek patient-specific implants in orbital reconstruction. J. Oral Biol. Craniofac. Res. 2020, 10, 49–53. [Google Scholar] [CrossRef]
- Sigron, G.R.; Rüedi, N.; Chammartin, F.; Meyer, S.; Msallem, B.; Kunz, C.; Thieringer, F.M. Three-Dimensional Analysis of Isolated Orbital Floor Fractures Pre- and Post-Reconstruction with Standard Titanium Meshes and “Hybrid” Patient-Specific Implants. J. Clin. Med. 2020, 9, 1579. [Google Scholar] [CrossRef] [PubMed]
- Baino, F. Biomaterials and implants for orbital floor repair. Acta Biomater. 2011, 7, 3248–3266. [Google Scholar] [CrossRef] [Green Version]
- Avashia, Y.J.; Sastry, A.; Fan, K.L.; Mir, H.S.; Thaller, S.R. Materials used for reconstruction after orbital floor fracture. J. Craniofac. Surg. 2012, 23, S49–S55. [Google Scholar] [CrossRef]
- Mok, D.; Lessard, L.; Cordoba, C.; Harris, P.G.; Nikolis, A. A review of materials currently used in orbital floor reconstruction. Can. J. Plast Surg. 2004, 12, 134–140. [Google Scholar] [CrossRef] [Green Version]
- Gu, R.D.; Xiao, F.; Wang, L.; Sun, K.J.; Chen, L.L. Biocompatibility of polyetheretherketone for the treatment of orbital bone defects. Int. J. Ophthalmol. 2020, 13, 725–730. [Google Scholar] [CrossRef] [PubMed]
- Sharma, N.; Aghlmandi, S.; Cao, S.; Kunz, C.; Honigmann, P.; Thieringer, F.M. Quality Characteristics and Clinical Relevance of In-House 3D-Printed Customized Polyetheretherketone (PEEK) Implants for Craniofacial Reconstruction. J. Clin. Med. 2020, 9, 2818. [Google Scholar] [CrossRef] [PubMed]
- Honigmann, P.; Sharma, N.; Schumacher, R.; Rueegg, J.; Haefeli, M.; Thieringer, F. In-Hospital 3D Printed Scaphoid Prosthesis Using Medical-Grade Polyetheretherketone (PEEK) Biomaterial. Biomed. Res. Int. 2021, 11, 1301028. [Google Scholar] [CrossRef]
- Panayotov, I.V.; Orti, V.; Cuisinier, F.; Yachouh, J. Polyetheretherketone (PEEK) for medical applications. J. Mater. Sci. Mater. Med. 2016, 27, 118. [Google Scholar] [CrossRef] [PubMed]
- Han, X.; Sharma, N.; Xu, Z.; Scheideler, L.; Geis-Gerstorfer, J.; Rupp, F.; Thieringer, F.M.; Spintzyk, S. An In Vitro Study of Osteoblast Response on Fused-Filament Fabrication 3D Printed PEEK for Dental and Cranio-Maxillofacial Implants. J. Clin. Med. 2019, 8, 771. [Google Scholar] [CrossRef] [Green Version]
- Basgul, C.; Spece, H.; Sharma, N.; Thieringer, F.M.; Kurtz, S.M. Structure, properties, and bioactivity of 3D printed PAEKs for implant applications: A systematic review. J. Biomed. Mater. Res. B Appl. Biomater. 2021. online ahead of print. [Google Scholar] [CrossRef]
- Honigmann, P.; Sharma, N.; Okolo, B.; Popp, U.; Msallem, B.; Thieringer, F.M. Patient-Specific Surgical Implants Made of 3D Printed PEEK: Material, Technology, and Scope of Surgical Application. Biomed. Res. Int. 2018, 2018, 4520636. [Google Scholar] [CrossRef] [Green Version]
- Nazimi, A.J.; Md Yusoff, M.; Nordin, R.; Nabil, S. Use of polyetheretherketone (PEEK) in orbital floor fracture reconstruction—A case for concern. J. Oral Maxillofac. Surg. Med. Pathol. 2015, 27, 536–539. [Google Scholar] [CrossRef]
- Pedemonte Trewhela, C.; Díaz Reiher, M.; Muñoz Zavala, T.; González Mora, L.E.; Vargas Farren, I. Correction of Delayed Traumatic Enophthalmos Using Customized Orbital Implants. J. Oral Maxillofac. Surg. 2018, 76, 1937–1945. [Google Scholar] [CrossRef]
- Kurtz, S.M.; Devine, J.N. PEEK biomaterials in trauma, orthopedic, and spinal implants. Biomaterials 2007, 28, 4845–4869. [Google Scholar] [CrossRef] [Green Version]
- Johansson, P.; Jimbo, R.; Kjellin, P.; Currie, F.; Chrcanovic, B.R.; Wennerberg, A. Biomechanical evaluation and surface characterization of a nano-modified surface on PEEK implants: A study in the rabbit tibia. Int. J. Nanomed. 2014, 9, 3903–3911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feng, X.; Ma, L.; Liang, H.; Liu, X.; Lei, J.; Li, W.; Wang, K.; Song, Y.; Wang, B.; Li, G.; et al. Osteointegration of 3D-Printed Fully Porous Polyetheretherketone Scaffolds with Different Pore Sizes. ACS Omega 2020, 5, 26655–26666. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Wei, W.; Yang, L.; Pan, Y.; Wang, X.; Wang, T.; Tang, S.; Yao, Y.; Hong, H.; Wei, J. Stimulation of cell responses and bone ingrowth into macro-microporous implants of nano-bioglass/polyetheretherketone composite and enhanced antibacterial activity by release of hinokitiol. Colloids Surf. B 2018, 164, 347–357. [Google Scholar] [CrossRef] [PubMed]
- Baştan, F.E.; Atiq Ur Rehman, M.; Avcu, Y.Y.; Avcu, E.; Üstel, F.; Boccaccini, A.R. Electrophoretic co-deposition of PEEKhydroxyapatite composite coatings for biomedical applications. Colloids Surf. B 2018, 169, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Spece, H.; Yu, T.; Law, A.W.; Marcolongo, M.; Kurtz, S.M. 3D printed porous PEEK created via fused filament fabrication for osteoconductive orthopaedic surfaces. J. Mech. Behav. Biomed. Mater. 2020, 109, 103850. [Google Scholar] [CrossRef]
- Torstrick, F.B.; Safranski, D.L.; Burkus, J.K.; Chappuis, J.L.; Lee, C.S.D.; Guldberg, R.E.; Gall, K.; Smith, K.E. Getting PEEK to Stick to Bone: The Development of Porous PEEK for Interbody Fusion Devices. Tech. Orthop. 2017, 32, 158–166. [Google Scholar] [CrossRef]
- Landy, B.C.; Vangordon, S.B.; McFetridge, P.S.; Sikavitsas, V.I.; Jarman-Smith, M. Mechanical and in vitro investigation of a porous PEEK foam for medical device implants. J. Appl. Biomater. Funct. Mater. 2013, 11, e35–e44. [Google Scholar] [CrossRef]
- Wang, X.; Xu, S.; Zhou, S.; Xu, W.; Leary, M.; Choong, P.; Qian, M.; Brandt, M.; Xie, Y.M. Topological design and additive manufacturing of porous metals for bone scaffolds and orthopaedic implants: A review. Biomaterials 2016, 83, 127–141. [Google Scholar] [CrossRef]
- Guddati, S.; Kiran, A.S.K.; Leavy, M.; Ramakrishna, S. Recent advancements in additive manufacturing technologies for porous material applications. Int. J. Adv. Manuf. Technol. 2019, 105, 193–215. [Google Scholar] [CrossRef]
- Vaezi, M.; Yang, S. Extrusion-based additive manufacturing of PEEK for biomedical applications. Virtual Phys. Prototyp. 2015, 10, 123–135. [Google Scholar] [CrossRef]
- Han, D.H.; Chi, M. Comparison of the outcomes of blowout fracture repair according to the orbital implant. J. Craniofac. Surg. 2011, 22, 1422–1425. [Google Scholar] [CrossRef] [PubMed]
- El Halabi, F.; Rodriguez, J.F.; Rebolledo, L.; Hurtos, E.; Doblare, M. Mechanical characterization and numerical simulation of polyether-ether-ketone (PEEK) cranial implants. J. Mech. Behav. Biomed. Mater. 2011, 4, 1819–1832. [Google Scholar] [CrossRef] [PubMed]
- Ridwan-Pramana, A.; Marcián, P.; Borák, L.; Narra, N.; Forouzanfar, T.; Wolff, J. Finite element analysis of 6 large PMMA skull reconstructions: A multi-criteria evaluation approach. PLoS ONE 2017, 12, e0179325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guillaume, O.; Geven, M.A.; Varjas, V.; Varga, P.; Gehweiler, D.; Stadelmann, V.A.; Smidt, T.; Zeiter, S.; Sprecher, C.; Bos, R.R.M.; et al. Orbital floor repair using patient specific osteoinductive implant made by stereolithography. Biomaterials 2020, 233, 119721. [Google Scholar] [CrossRef]
- Birkenfeld, F.; Behrens, E.; Kern, M.; Gassling, V.; Wiltfang, J. Mechanical properties of collagen membranes: Are they sufficient for orbital floor reconstructions? J. Craniomaxillofac. Surg. 2015, 43, 260–263. [Google Scholar] [CrossRef] [PubMed]
- Rae, P.J.; Brown, E.N.; Orler, E.B. The mechanical properties of poly(etherether-ketone) (PEEK) with emphasis on the large compressive strain response. Polymer 2007, 48, 598–615. [Google Scholar] [CrossRef]
- Garcia-Leiner, M.; Ghita, O.; McKay, R.; Kurtz, S. Additive Manufacturing of Polyaryletherketones. In PEEK Biomaterials Handbook, 2nd ed.; Kurtz, S., Ed.; William Andrew Publishing: New York, NY, USA, 2019; pp. 89–103. [Google Scholar]
- Graham, J.; Peck, J. FDA Regulation of PEEK Implants. In PEEK Biomaterials Handbook, 2nd ed.; Kurtz, S., Ed.; William Andrew Publishing: New York, NY, USA, 2019; pp. 431–445. [Google Scholar]
- Basgul, C.; Thieringer, F.M.; Kurtz, S.M. Heat transfer-based non-isothermal healing model for the interfacial bonding strength of fused filament fabricated polyetheretherketone. Addit. Manuf. 2021, 46, 102097. [Google Scholar] [CrossRef]
- Jahan, A.; Edwards, K.L. A state-of-the-art survey on the influence of normalization techniques in ranking: Improving the materials selection process in engineering design. Mater. Des. 2015, 65, 335–342. [Google Scholar] [CrossRef]
- Alasseri, N.; Alasraj, A. Patient-specific implants for maxillofacial defects: Challenges and solutions. Maxillofac. Plast. Reconstr. Surg. 2020, 42, 15. [Google Scholar] [CrossRef]
- Punchak, M.; Chung, L.K.; Lagman, C.; Bui, T.T.; Lazareff, J.; Rezzadeh, K.; Jarrahy, R.; Yang, I. Outcomes following polyetheretherketone (PEEK) cranioplasty: Systematic review and meta-analysis. J. Clin. Neurosci. 2017, 41, 30–35. [Google Scholar] [CrossRef]
- Rammos, C.K.; Cayci, C.; Castro-Garcia, J.A.; Feiz-Erfan, I.; Lettieri, S.C. Patient-specific polyetheretherketone implants for repair of craniofacial defects. J. Craniofac. Surg. 2015, 26, 631–633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Järvinen, S.; Suojanen, J.; Kormi, E.; Wilkman, T.; Kiukkonen, A.; Leikola, J.; Stoor, P. The use of patient specific polyetheretherketone implants for reconstruction of maxillofacial deformities. J. Craniomaxillofac. Surg. 2019, 47, 1072–1076. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ding, L.; Chen, X.; Zhang, J.; Wang, R.; Wu, G. Digital fabrication of a maxillary obturator prosthesis by using a 3-dimensionally-printed polyetheretherketone framework. J. Prosthet. Dent. 2021. [Google Scholar] [CrossRef]
- Olate, S.; Uribe, F.; Huentequeo-Molina, C.; Goulart, D.R.; Sigua-Rodriguez, E.A.; Alister, J.P. Mandibular Angle Contouring Using Porous Polyethylene Stock or PEEK-based Patient Specific Implants. A Critical Analysis. J. Craniofac. Surg. 2021, 32, 242–246. [Google Scholar] [CrossRef]
- Herford, A.S.; Miller, M.; Lauritano, F.; Cervino, G.; Signorino, F.; Maiorana, C. The use of virtual surgical planning and navigation in the treatment of orbital trauma. Chin. J. Traumatol. 2017, 20, 9–13. [Google Scholar] [CrossRef]
- Chepurnyi, Y.; Chernogorskyi, D.; Petrenko, O.; Kopchak, A. Reconstruction of Post-Traumatic Orbital Defects and Deformities with Custom-Made Patient-Specific Implants: Evaluation of the Efficacy and Clinical Outcome. Craniomaxillofac. Trauma Reconstr. Open 2019, 3, e9–e17. [Google Scholar] [CrossRef]
- Yang, C.; Tian, X.; Li, D.; Cao, Y.; Zhao, F.; Shi, C. Influence of thermal processing conditions in 3D printing on the crystallinity and mechanical properties of PEEK material. J. Mater. Process. Technol. 2017, 248, 1–7. [Google Scholar] [CrossRef]
- Zadpoor, A.A. Design for Additive Bio-Manufacturing: From Patient-Specific Medical Devices to Rationally Designed Meta-Biomaterials. Int. J. Mol. Sci. 2017, 18, 1607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, N.; Ostas, D.; Rotar, H.; Brantner, P.; Thieringer, F.M. Design and Additive Manufacturing of a Biomimetic Customized Cranial Implant based on Voronoi Diagram. Front. Physiol. 2021, 12, 443. [Google Scholar] [CrossRef]
- Shidid, D.; Leary, M.; Choong, P.; Brandt, M. Just-in-time design and additive manufacture of patient-specific medical implants. Phys. Procedia 2016, 83, 4–14. [Google Scholar] [CrossRef] [Green Version]
- Alfaify, A.; Saleh, M.; Abdullah, F.M.; Al-Ahmari, A.M. Design for Additive Manufacturing: A Systematic Review. Sustainability 2020, 12, 7936. [Google Scholar] [CrossRef]
- Haug, R.H.; Nuveen, E.; Bredbenner, T. An evaluation of the support provided by common internal orbital reconstruction materials. J. Oral Maxillofac. Surg. 1999, 57, 564–570. [Google Scholar] [CrossRef]
- Birkenfeld, F.; Steiner, M.; Kern, M.; Witlfang, J.; Möller, B.; Lucius, R.; Becker, S.T. Maximum forces applied to the orbital floor after fractures. J. Craniofac. Surg. 2012, 23, 1491–1494. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Solid | Rectangular | Triangular | Circular | |
|---|---|---|---|---|
| Number of elements | 18,883 | 26,806 | 31,915 | 26,474 |
| Number of nodes | 57,124 | 82,296 | 97,995 | 83,036 |
| Implant Profile Configuration | Max. Von Mises (MPa) | Max. Deformation (mm) |
|---|---|---|
| R05 | 5.313 | 0.098 |
| R06 | 3.821 | 0.066 |
| R07 | 3.104 | 0.047 |
| R08 | 2.563 | 0.035 |
| R09 | 2.147 | 0.027 |
| T05 | 4.502 | 0.093 |
| T06 | 3.304 | 0.063 |
| T07 | 2.522 | 0.045 |
| T08 | 1.986 | 0.033 |
| T09 | 1.636 | 0.026 |
| C05 | 5.267 | 0.107 |
| C06 | 3.397 | 0.072 |
| C07 | 2.439 | 0.052 |
| C08 | 1.904 | 0.038 |
| C09 | 1.519 | 0.030 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sharma, N.; Welker, D.; Aghlmandi, S.; Maintz, M.; Zeilhofer, H.-F.; Honigmann, P.; Seifert, T.; Thieringer, F.M. A Multi-Criteria Assessment Strategy for 3D Printed Porous Polyetheretherketone (PEEK) Patient-Specific Implants for Orbital Wall Reconstruction. J. Clin. Med. 2021, 10, 3563. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10163563
Sharma N, Welker D, Aghlmandi S, Maintz M, Zeilhofer H-F, Honigmann P, Seifert T, Thieringer FM. A Multi-Criteria Assessment Strategy for 3D Printed Porous Polyetheretherketone (PEEK) Patient-Specific Implants for Orbital Wall Reconstruction. Journal of Clinical Medicine. 2021; 10(16):3563. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10163563
Chicago/Turabian StyleSharma, Neha, Dennis Welker, Soheila Aghlmandi, Michaela Maintz, Hans-Florian Zeilhofer, Philipp Honigmann, Thomas Seifert, and Florian M. Thieringer. 2021. "A Multi-Criteria Assessment Strategy for 3D Printed Porous Polyetheretherketone (PEEK) Patient-Specific Implants for Orbital Wall Reconstruction" Journal of Clinical Medicine 10, no. 16: 3563. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm10163563