Kidney Involvement in Patients with Type 1 Autoimmune Pancreatitis

 , ,
, ,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Study Design
2.2. Cohort
2.3. Imaging
2.4. Ethics
3. Results
Imaging Features
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
Abbreviations
| AIP | Autoimmune Pancreatitis |
| OOI | Other Organ Involvement |
| IgG4-RKD | IgG4-Related Kidney Disease |
| LPSP | Lymphoplasmacytic Sclerosing Pancreatitis |
| IDCP | Idiopathic Duct-centric Pancreatitis |
| IAC | Immune Associated Cholangitis |
| ICDC | International Consensus Diagnostic Criteria |
| TIN | Tubulointerstitial Nephritis |
| JSN | Japanese Society of Nephrology |
| PACS | Picture Archiving and Communication System |
| SI | Signal Intensity |
| DWI | Diffusion-Weighted Imaging |
| ADC | Apparent Diffusion Coefficient |
| GFR | Glomerular Filtration Rate |
| DM | Diabetes Mellitus |
| AH | Arterial Hypertension |
References
- Klöppel, G.; Luttges, J.; Löhr, M.; Zamboni, G.; Longnecker, D. Autoimmune pancreatitis: Pathological, clinical, and immunological features. Pancreas 2003, 27, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Hart, P.A.; Kamisawa, T.; Brugge, W.R.; Chung, J.B.; Culver, E.L.; Czakó, L.; Frulloni, L.; Go, V.L.W.; Gress, T.M.; Kim, M.H.; et al. Long-term outcomes of autoimmune pancreatitis: A multicentre, international analysis. Gut 2013, 62, 1771–1776. [Google Scholar] [CrossRef] [PubMed]
- Vujasinovic, M.; Valente, R.; Maier, P.; von Beckerath, V.; Haas, S.L.; Arnelo, U.; Del Chiaro, M.; Kartalis, N.; Pozzi-Mucelli, R.M.; Fernandez-Moro, C.; et al. Diagnosis, treatment and long-term outcome of autoimmune pancreatitis in Sweden. Pancreatology 2018, 18, 900–904. [Google Scholar] [CrossRef] [PubMed]
- Shimosegawa, T.; Chari, S.T.; Frulloni, L.; Kamisawa, T.; Kawa, S.; Mino-Kenudson, M.; Kim, M.H.; Klöppel, G.; Lerch, M.M.; Löhr, M.; et al. International consensus diagnostic criteria for autoimmune pancreatitis: Guidelines of the International Association of Pancreatology. Pancreas 2011, 40, 352–358. [Google Scholar] [CrossRef] [PubMed]
- Frulloni, L.; Scattolini, C.; Falconi, M.; Zamboni, G.; Capelli, P.; Manfredi, R.; Graziani, R.; D’onofrio, M.; Katsotourchi, A.M.; Amodio, A.; et al. Autoimmune pancreatitis: Differences between the focal and diffuse forms in 87 patients. Am. J. Gastroenterol. 2009, 104, 2288–2294. [Google Scholar] [CrossRef] [PubMed]
- Czakó, L.; Gyökeres, T.; Topa, L.; Sahin, P.; Takács, T.; Vincze, Á.; Dubravcsik, Z.; Szepes, A.; Pap, Á.; Földesi, I.; et al. Autoimmune pancreatitis in Hungary: A multicenter nationwide study. Pancreatology 2011, 11, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Church, N.I.; Pereira, S.P.; Deheragoda, M.G.; Sandanayake, N.; Amin, Z.; Lees, W.R.; Gillams, A.; Rodriguez-Justo, M.; Novelli, M.; Seward, E.W.; et al. Autoimmune pancreatitis: Clinical and radiological features and objective response to steroid therapy in a UK series. Am. J. Gastroenterol. 2007, 102, 2417–2425. [Google Scholar] [CrossRef] [PubMed]
- López-Serrano, A.; Crespo, J.; Pascual, I.; Salord, S.; Bolado, F.; del-Pozo-García, A.J.; Ilzarbe, L.; de-Madaria, E.; Moreno-Osset, E.; Autoimmune Pancreatitis in Spain Study Group. Diagnosis, treatment and long-term outcomes of autoimmune pancreatitis in Spain based on the International Consensus Diagnostic Criteria: A multi-centre study. Pancreatology 2016, 16, 382–390. [Google Scholar] [CrossRef] [PubMed]
- Uchiyama-Tanaka, Y.; Mori, Y.; Kimura, T.; Sonomura, K.; Umemura, S.; Kishimoto, N.; Nose, A.; Tokoro, T.; Kijima, Y.; Yamahara, H.; et al. Acute tubulointerstitial nephritis associated with autoimmune-related pancreatitis. Am. J. Kidney Dis. 2004, 43, e18–e25. [Google Scholar] [CrossRef]
- Takeda, S.; Haratake, J.; Kasai, T.; Takaeda, C.; Takazakura, E. IgG4-associated idiopathic tubulointerstitial nephritis complicating autoimmune pancreatitis. Nephrol. Dial. Transplant. 2004, 19, 474–476. [Google Scholar] [CrossRef] [Green Version]
- Rudmik, L.; Trpkov, K.; Nash, C.; Kinnear, S.; Falck, V.; Dushinski, J.; Dixon, E. Autoimmune pancreatitis associated with renal lesions mimicking metastatic tumours. Cmaj 2006, 175, 367–369. [Google Scholar] [CrossRef] [Green Version]
- Shimoyama, K.; Ogawa, N.; Sawaki, T.; Karasawa, H.; Masaki, Y.; Kawabata, H.; Fukushima, T.; Wano, Y.; Hirose, Y.; Umehara, H. A case of Mikulicz’s disease complicated with interstitial nephritis successfully treated by high-dose corticosteroid. Mod. Rheumatol. 2006, 16, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Tsubata, Y.; Akiyama, F.; Oya, T.; Ajiro, J.; Saeki, T.; Nishi, S.; Narita, I. IgG4-related chronic tubulointerstitial nephritis without autoimmune pancreatitis and the time course of renal function. Intern. Med. 2010, 49, 1593–1598. [Google Scholar] [CrossRef] [PubMed]
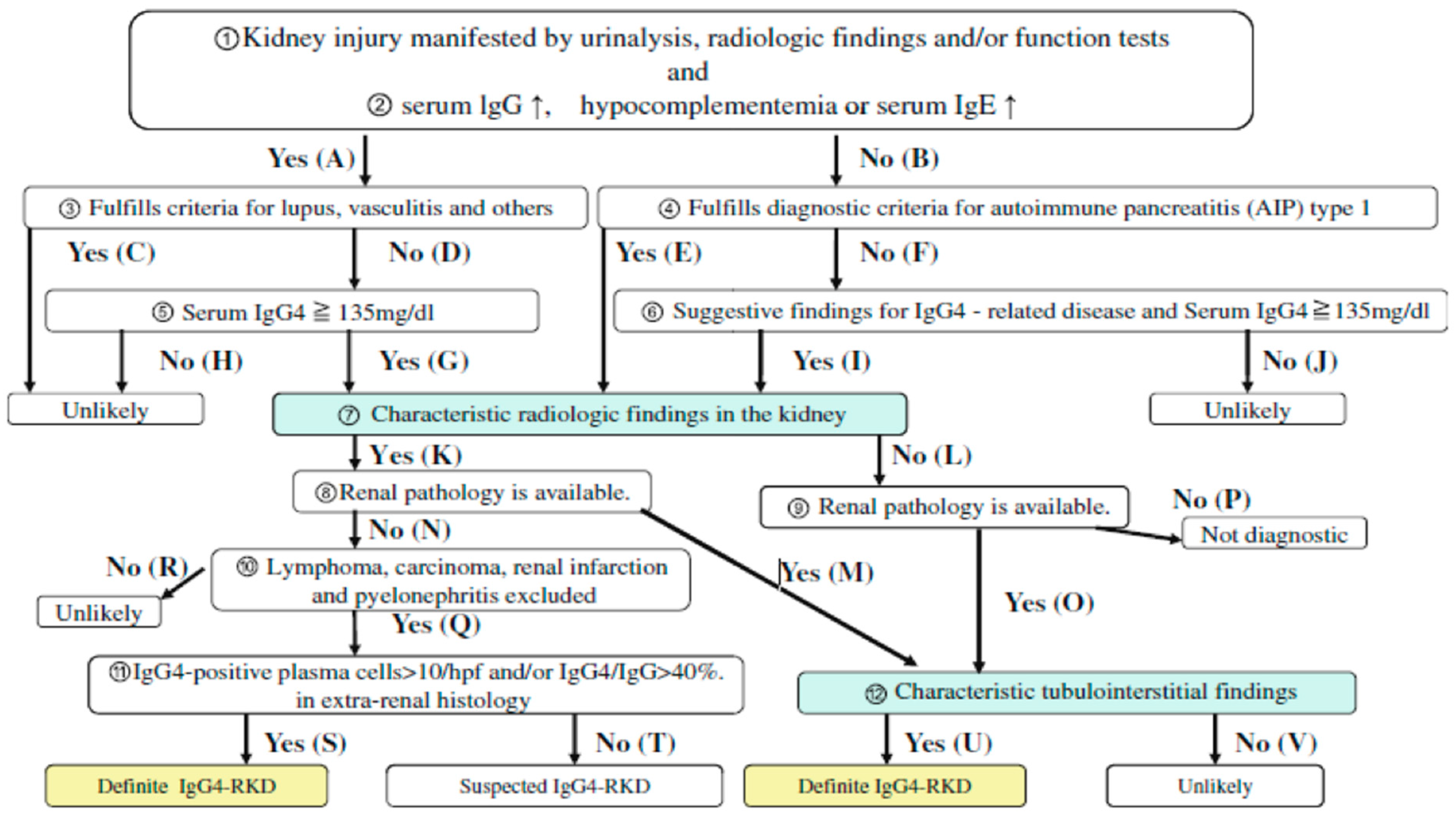
- Kawano, M.; Saeki, T.; Nakashima, H.; Nishi, S.; Yamaguchi, Y.; Hisano, S.; Yamanaka, N.; Inoue, D.; Yamamoto, M.; Takahashi, H.; Nomura, H. Proposal for diagnostic criteria for IgG4-related kidney disease. Clin. Exp. Nephrol. 2011, 15, 615–626. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.; Kim, J.H.; Byun, J.H.; Kim, H.J.; Lee, S.S.; Kim, S.Y.; Lee, M.G. IgG4-related kidney disease: MRI findings with emphasis on the usefulness of diffusion-weighted imaging. Eur. J. Radiol. 2014, 83, 1057–1062. [Google Scholar] [CrossRef] [PubMed]
- Naitoh, I.; Nakazawa, T.; Ohara, H.; Ando, T.; Hayashi, K.; Tanaka, H.; Okumura, F.; Miyabe, K.; Yoshida, M.; Sano, H.; et al. Clinical significance of extrapancreatic lesions in autoimmune pancreatitis. Pancreas 2010, 39, e1–e5. [Google Scholar] [CrossRef] [PubMed]
- Hirth, M.; Vujasinovic, M.; Münch, M.; Weiss, C.; Löhr, M.; Ebert, M.P.; Schneider, A. Monitoring and predicting disease activity in autoimmune pancreatitis with the M-ANNHEIM-AiP-Activity-Score. Pancreatology 2018, 18, 29–38. [Google Scholar] [CrossRef]
- Saeki, T.; Nishi, S.; Imai, N.; Ito, T.; Yamazaki, H.; Kawano, M.; Yamamoto, M.; Takahashi, H.; Matsui, S.; Nakada, S.; et al. Clinicopathological characteristics of patients with IgG4-related tubulointerstitial nephritis. Kidney Int. 2010, 78, 1016–1023. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.; Notohara, K.; Levy, M.J.; Chari, S.T.; Smyrk, T.C. IgG4-positive plasma cell infiltration in the diagnosis of autoimmune pancreatitis. Mod. Pathol. 2007, 20, 23–28. [Google Scholar] [CrossRef]
- Aalberse, R.C.; Schuurman, J. IgG4 breaking the rules. Immunology 2002, 105, 9–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sporek, M.; Dumnicka, P.; Gala-Bladzinska, A.; Ceranowicz, P.; Warzecha, Z.; Dembinski, A.; Stepien, E.; Walocha, J.; Drozdz, R.; Kuzniewski, M.; et al. Angiopoietin-2 Is an Early Indicator of Acute Pancreatic-Renal Syndrome in Patients with Acute Pancreatitis. Mediat. Inflamm. 2016, 2016, 5780903. [Google Scholar] [CrossRef] [PubMed]
- Sporek, M.; Gala-Błądzińska, A.; Dumnicka, P.; Mazur-Laskowska, M.; Kielczewski, S.; Walocha, J.; Ceranowicz, P.; Kuźniewski, M.; Mituś, J.; Kuśnierz-Cabala, B. Urine NGAL is useful in the clinical evaluation of renal function in the early course of acute pancreatitis. Folia Med. Cracov. 2016, 56, 13–25. [Google Scholar] [PubMed]
- Cornell, L.D. IgG4-related tubulointerstitial nephritis. Kidney Int. 2010, 78, 951–953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raissian, Y.; Nasr, S.H.; Larsen, C.P.; Colvin, R.B.; Smyrk, T.C.; Takahashi, N.; Bhalodia, A.; Sohani, A.R.; Zhang, L.; Chari, S.; et al. Diagnosis of IgG4-related tubulointerstitial nephritis. J. Am. Soc. Nephrol. 2011, 22, 1343–1352. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| N | Gender | Age | Treatment | OOI (Other than Kidney/Pancreas) | Imaging | Type of Kidney Involvement | Unilateral vs. Bilateral Involvement | Onset of Kidney Involvement |
|---|---|---|---|---|---|---|---|---|
| 1 | M | 74 | steroids, surgery | cholangitis | CEMR | multiple lesions | bilateral | 6 y after AIP |
| vasculitis (aorta) | ||||||||
| retroperitoneal fibrosis | ||||||||
| 2 | F | 73 | steroids | cholangitis | CECT CEMR | multiple lesions | bilateral | 3 m after AIP |
| Sjögren’s Syndrome enlarge mediastinal LN | ||||||||
| 3 | M | 52 | steroids, biliary stent | cholangitis | CECT MRw/o c | multiple lesions | bilateral | synchronous |
| 4 | M | 49 | steroids, surgery | cholangitis | CECT CEMR | soft tissue in the perinephric space, diffuse swelling | bilateral | 6 m after AIP |
| hepatitis | ||||||||
| enlarge abdominal LN | ||||||||
| 5 | M | 60 | steroids | cholangitis | CEMR | multiple lesions | unilateral (left) | 11 m after AIP |
| 6 | M | 57 | steroids, azathioprine | cholangitis | CECT CEMR | solitary lesion | unilateral (right) | synchronous |
| enlarge abdominal LN vasculitis (aorta) | ||||||||
| 7 | M | 42 | steroids | cholangitis | CECT CEMR | multiple lesions | bilateral | synchronous |
| 8 | F | 39 | none | cholangitis | CECT CEMR | multiple lesions | bilateral | synchronous |
| lung involvement | ||||||||
| 9 | M | 39 | none | cholangitis | CECT CEMR | multiple lesions | bilateral | synchronous |
| 10 | M | 73 | none | cholangitis | CEMR | multiple lesions | bilateral | synchronous |
| 11 | M | 68 | steroids | none | CECT CEMR | multiple lesions | bilateral | synchronous |
| 12 | M | 68 | steroids, surgery | cholangitis | CECT CEMR | focal thinning of renal cortex | bilateral | synchronous |
| 13 | M | 85 | biliary stent | cholangitis | CECT CEMR | multiple lesions | bilateral | synchronous |
| lung involvement | ||||||||
| vasculitis (aorta) | ||||||||
| 14 | M | 71 | steroids | cholangitis | CECT * | multiple lesions | bilateral | 2 y after AIP |
| 15 | M | 65 | steroids | cholangitis | CEMR | multiple lesions | bilateral | 8 y after AIP |
| vasculitis (aorta) | ||||||||
| 16 | M | 52 | none | cholangitis | CEMR | multiple lesions | bilateral | 4 y after AIP |
| 17 | M | 64 | none | cholangitis | CEMR | solitary lesion | unilateral (right) | synchronous |
| Signal Intensity (SI) | MRI Sequences | |||||
|---|---|---|---|---|---|---|
| T2-Weigthed | T1-Weighted (w/o Contrast Agent) | T1-Weighted Arterial Phase | T1-Weighted Venous Phase | T1-Weighted Delayed Phase | DWI * | |
| Hypointense | 10/15 (66.6%) | 2/15 (13.4%) | 9/15 (60%) | 8/15 (53.4%) | 9/15 (60%) | 1/15 (6.6%) |
| Isointense | 5/15 (33.4%) | 13/15 (86.6%) | 6/15 (40%) | 7/15 (46.6%) | 6/15 (40%) | 0 |
| Hyperintense | 0 | 0 | 0 | 0 | 0 | 14/15 (93.4%) |
| Restricted SI | - | - | - | - | - | 10/11 (90.9%) |
| Parameter | Present Study | Saeki et al. [18] | Kawano et al. [14] |
|---|---|---|---|
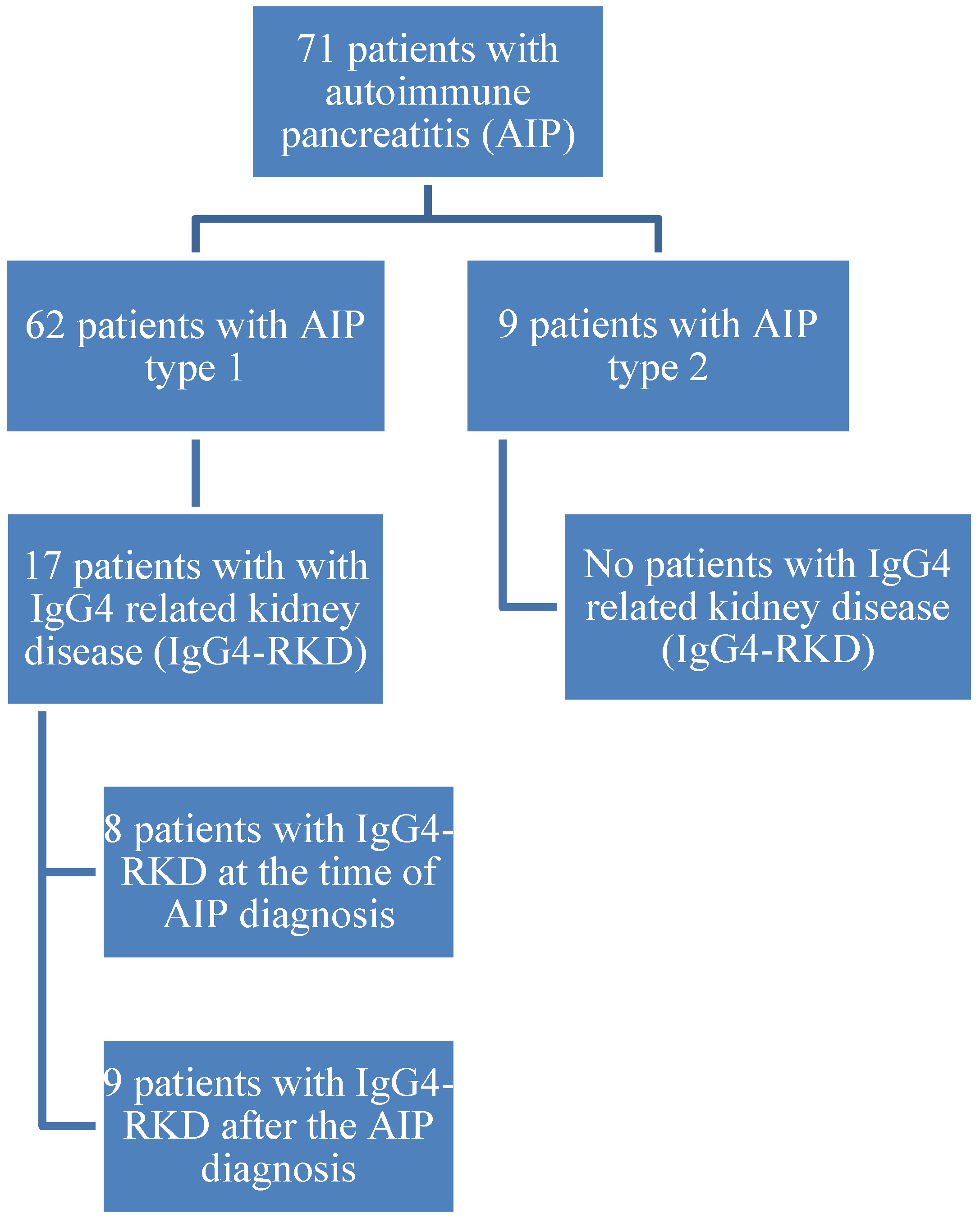
| Number of patients | 17 | 23 | 41 |
| Gender | 15 (88.2%) male and 2 (11.8%) female | 20 (86.9%) male and 3 (13.1%) female | 30 (73.2%) male and 11 (26.8%) female |
| Age at diagnosis (years) | 60.6 ± 13.1 (range 39–85) | 65.2 ± 10.1 (range 40–83) | 63.7 ± 12.3 years (range 27–83) |
| OOI % | 94.1 | 95.7 | 95.1 |
| Haematuria % | 23.5 | 34.8 | 41.7 |
| Proteinuria % | 23.5 | 8.7 | 58.3 |
| Elevated creatinine values % | 47.1 | 56.5 | 58.5 |
| Elevated IgG4 values % | 58.8 | 100 | 100 |
| Treatment with corticosteroids % | 76.5 | 91.3 | 92.7 |
| Improvement after steroid therapy % | 100 | 94.7 | 92.1 |
| Haemodialysis after steroid therapy % | 0 | 5.2 | 2.6 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vujasinovic, M.; Pozzi Mucelli, R.M.; Valente, R.; Verbeke, C.S.; Haas, S.L.; Löhr, J.-M. Kidney Involvement in Patients with Type 1 Autoimmune Pancreatitis. J. Clin. Med. 2019, 8, 258. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8020258
Vujasinovic M, Pozzi Mucelli RM, Valente R, Verbeke CS, Haas SL, Löhr J-M. Kidney Involvement in Patients with Type 1 Autoimmune Pancreatitis. Journal of Clinical Medicine. 2019; 8(2):258. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8020258
Chicago/Turabian StyleVujasinovic, Miroslav, Raffaella Maria Pozzi Mucelli, Roberto Valente, Caroline Sophie Verbeke, Stephan L. Haas, and J.-Matthias Löhr. 2019. "Kidney Involvement in Patients with Type 1 Autoimmune Pancreatitis" Journal of Clinical Medicine 8, no. 2: 258. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm8020258