
Elution Kinetics from Antibiotic-Loaded Calcium Sulfate Beads, Antibiotic-Loaded Polymethacrylate Spacers, and a Powdered Antibiotic Bolus for Surgical Site Infections in a Novel In Vitro Draining Knee Model

 , , , , , ,
, , , , , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
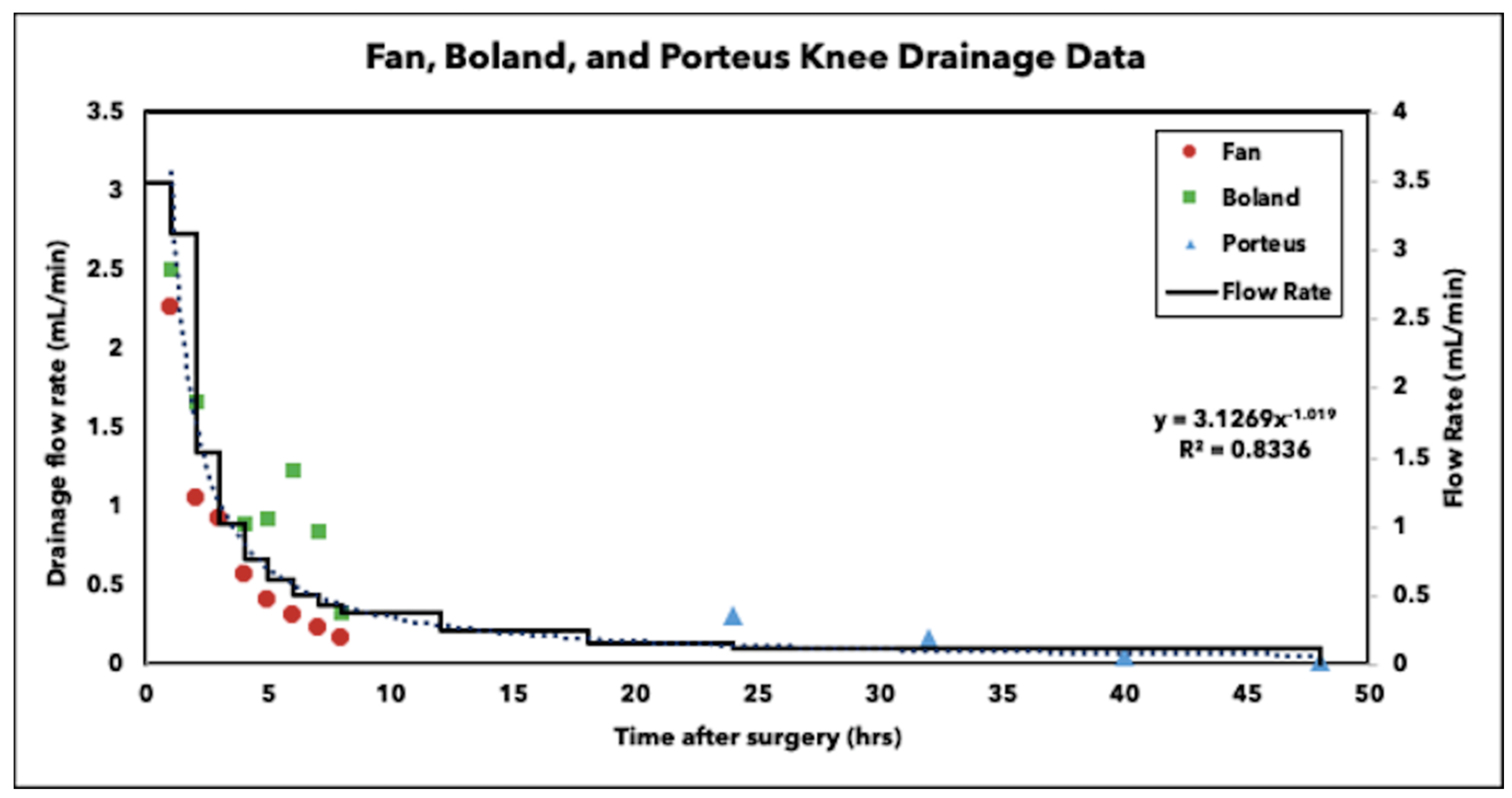
2.1. Drainage Flow
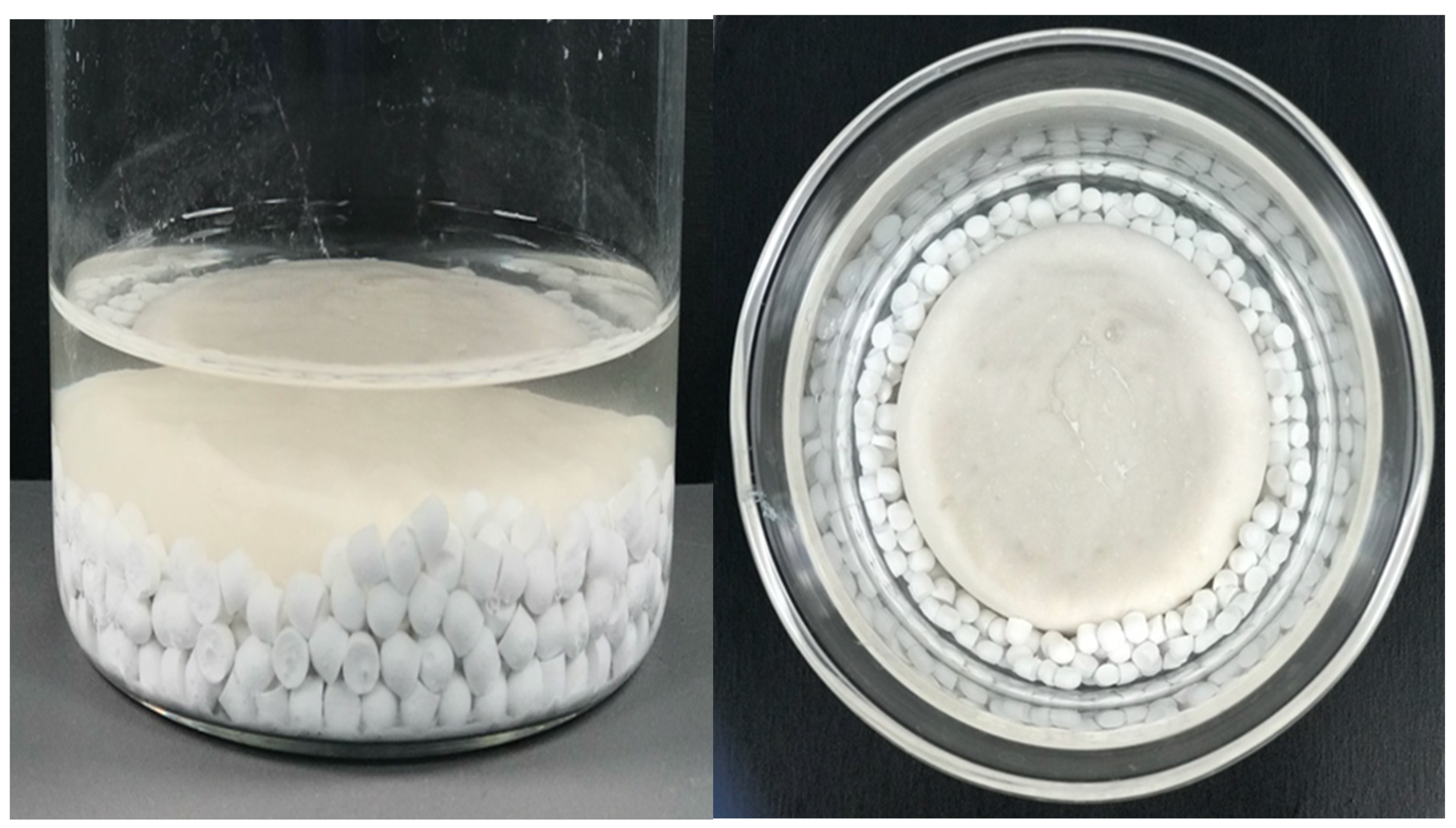
2.2. Calcium Sulfate Beads Stability
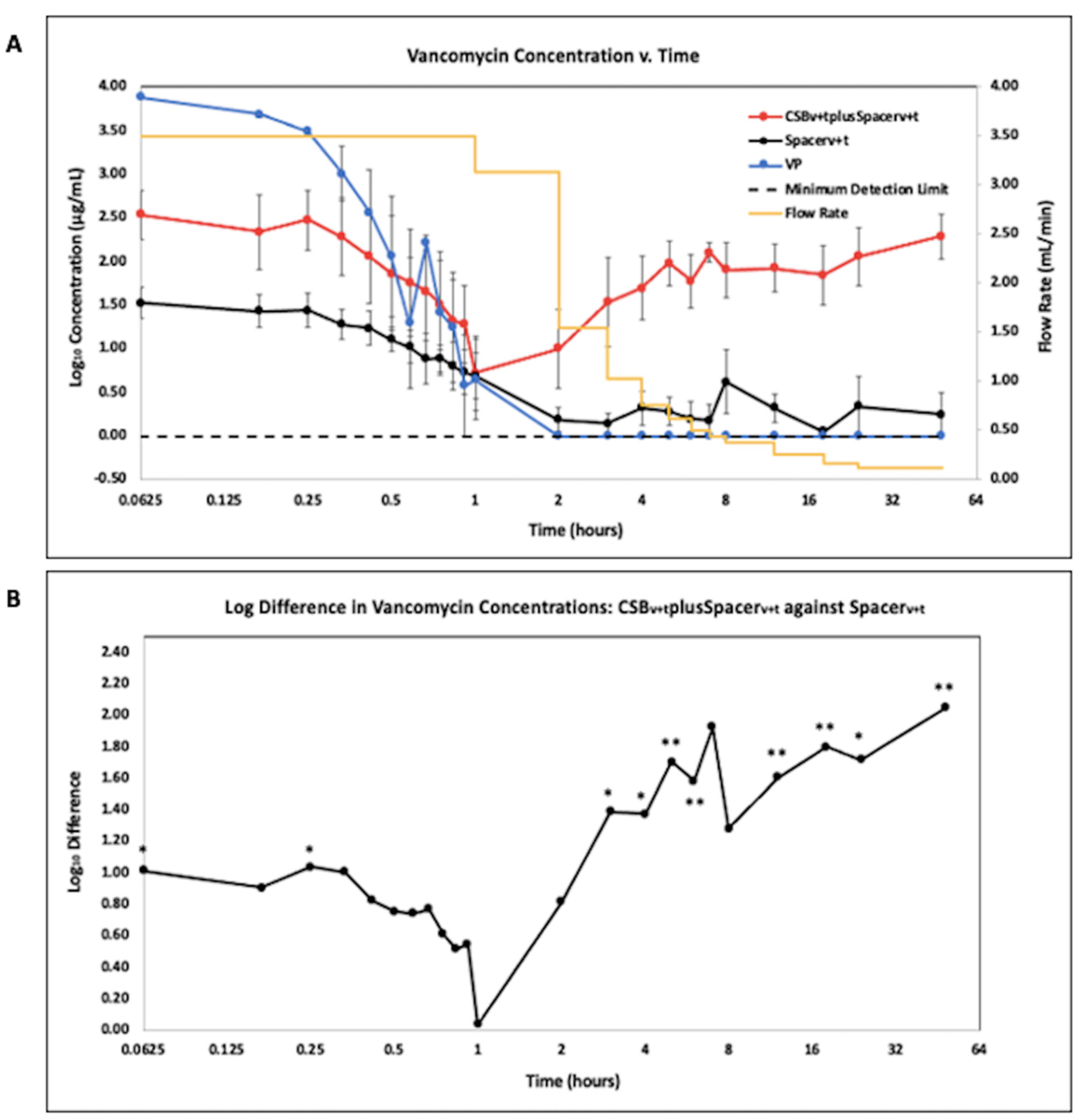
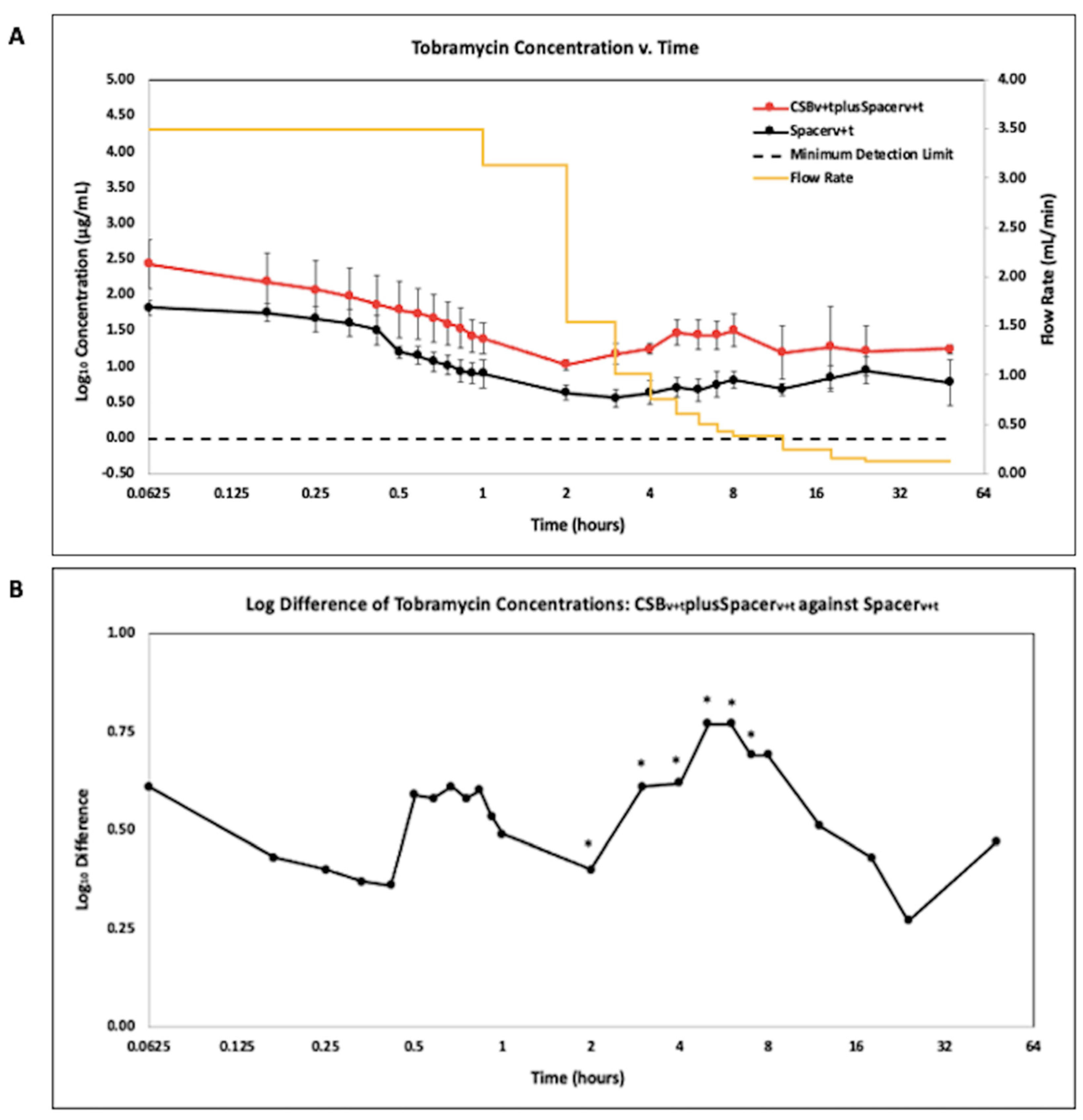
2.3. Liquid Chromatography Mass Spectrometry (LCMS)
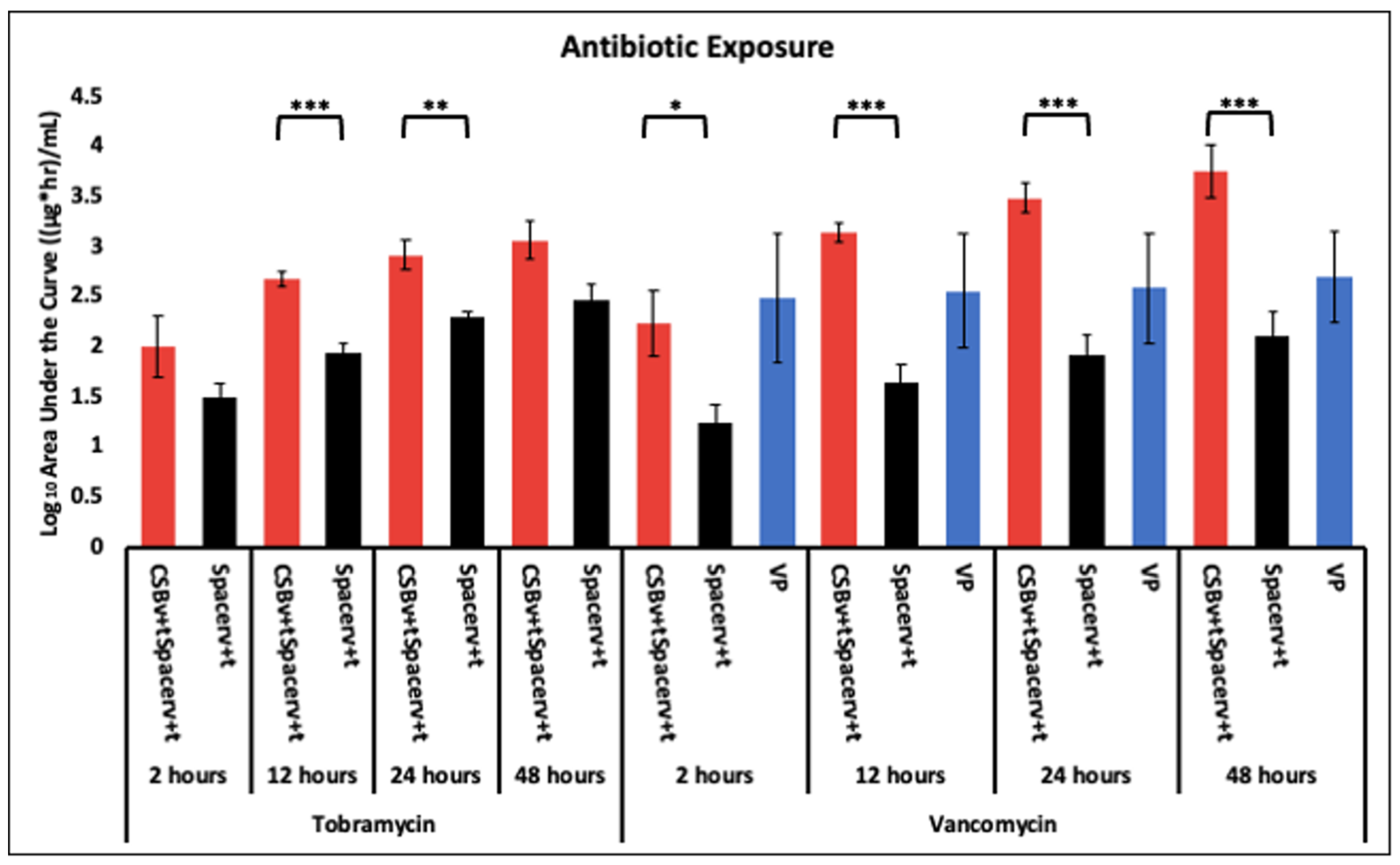
2.4. Antibiotic Profile Measured as Area under the Curve (AUC)
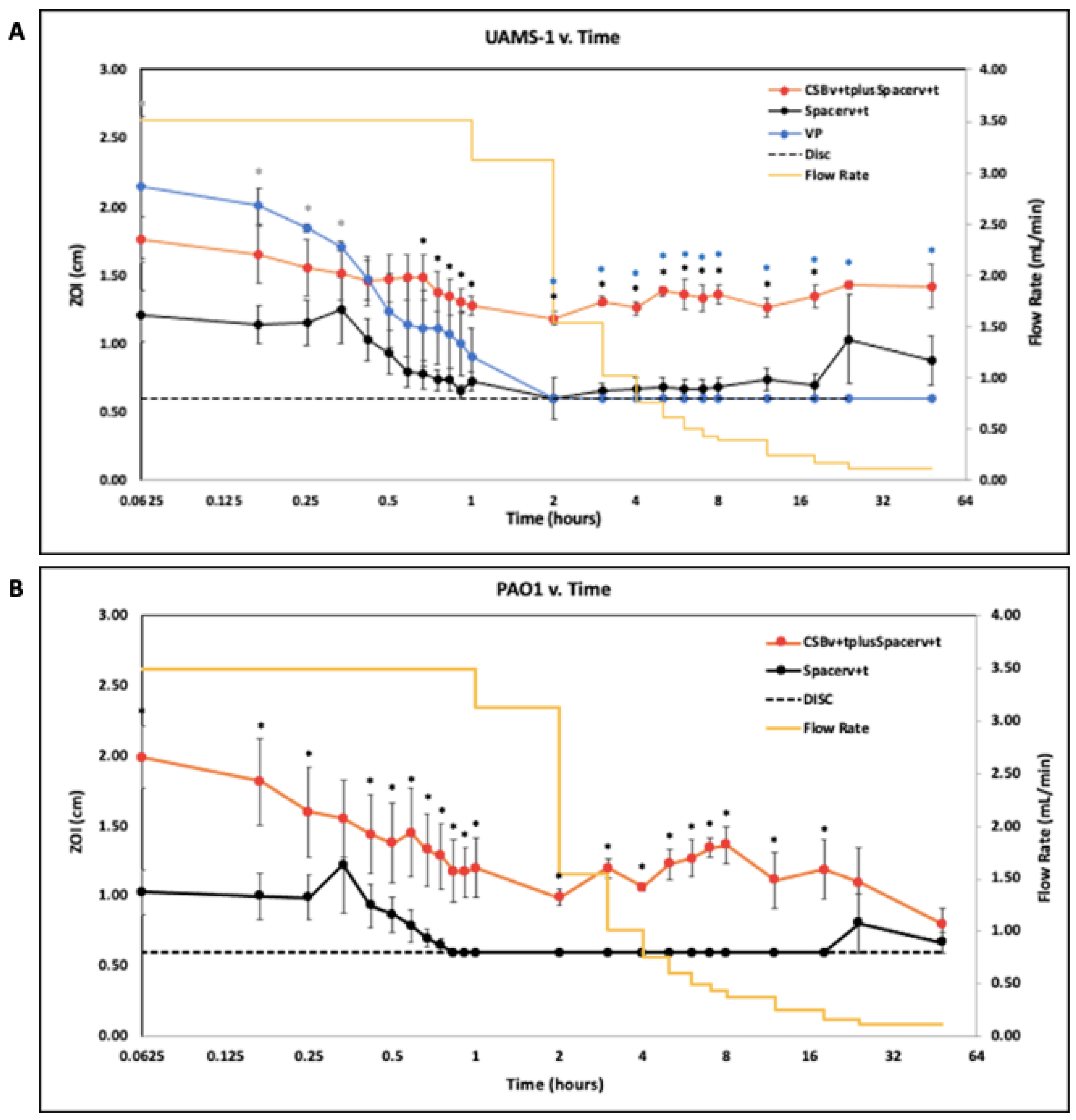
2.5. Zone of Inhibition (ZOI)
3. Discussion
4. Materials and Methods
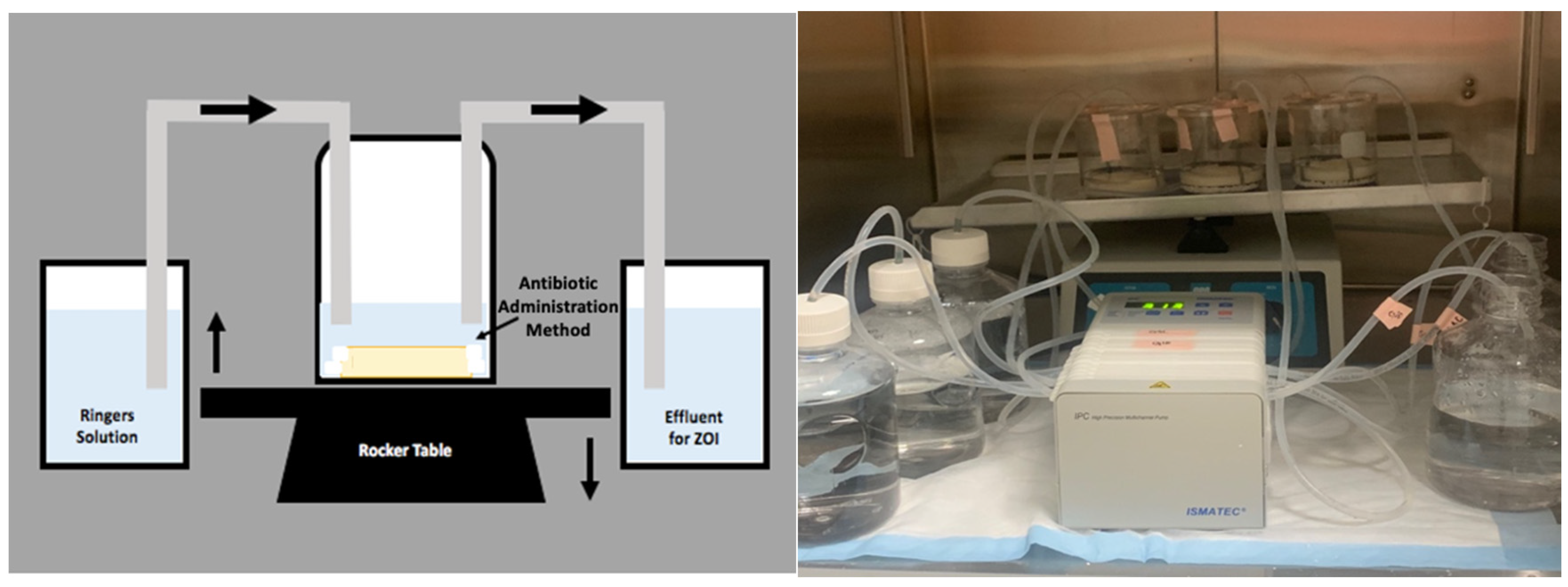
4.1. Reactor System
4.2. Preparation of Antibiotic Vehicles
4.2.1. Preparation of Antibiotic Loaded Calcium Sulfate Beads
4.2.2. Preparation of Antibiotic Loaded and Unloaded Polymethylmethacrylate (PMMA) Bone Cement Space Mimics
4.2.3. Preparation of Vancomycin Powder Bolus (VP)
4.3. Methods of Antibiotic Administration
4.4. Liquid Chromatography Mass Spectrometry (LCMS)
4.5. Area under the Curve (AUC)
4.6. Kirby-Bauer Assessment of Effluent Potency by Zones of Inhibition (ZOI)
4.7. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kurtz, S.M.; Lau, E.; Watson, H.; Schmier, J.K.; Parvizi, J. Economic burden of periprosthetic joint infection in the united states. J. Arthroplast. 2012, 27, 61–65.e1. [Google Scholar] [CrossRef]
- Owens, C.D.; Stoessel, K. Surgical site infections: Epidemiology, microbiology and prevention. J. Hosp. Infect. 2008, 70, 3–10. [Google Scholar] [CrossRef]
- McConoughey, S.J.; Howlin, R.; Granger, J.F.; Manring, M.M.; Calhoun, J.H.; Shirtliff, M.; Kathju, S.; Stoodley, P. Biofilms in periprosthetic orthopedic infections. Future Microbiol. 2014, 9, 987–1007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howlin, R.; Winnard, C.; Frapwell, C.; Webb, J.; Cooper, J.; Aiken, S.; Stoodley, P. Biofilm prevention of gram-negative bacterial pathogens involved in periprosthetic infection by antibiotic-loaded calcium sulfate beads in vitro. Biomed. Mater. 2016, 12, 015002. [Google Scholar] [CrossRef] [PubMed]
- Costerton, J.; Lewandowski, Z.; Caldwell, D.; Korber, D.; Lappin-Scott, H. Microbial biofilms. Ann. Rev. Microbiol. 1995, 49, 711–745. [Google Scholar] [CrossRef]
- Anagnostakos, K. What do we (not) know about antibiotic-loaded hip spacers? Orthopedics 2014, 37, 297–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leekha, S.; Terrell, C.L.; Edson, R.S. General principles of antimicrobial therapy. Mayo Clin. Proc. 2011, 86, 156–167. [Google Scholar] [CrossRef] [Green Version]
- Om, C.; Daily, F.; Vlieghe, E.; McLaughlin, J.C.; McLaws, M.L. “If it’s a broad spectrum, it can shoot better”: Inappropriate antibiotic prescribing in Cambodia. Antimicrob. Resist. Infect. Control 2016, 5, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Ostermann, P.; Seligson, D.; Henry, S. Local antibiotic therapy for severe open fractures. A review of 1085 consecutive cases. J. Bone Jt. Surg. Br. 1995, 77-B, 93–97. [Google Scholar] [CrossRef]
- Laycock, P.A.; Cooper, J.J.; Howlin, R.P.; Delury, C.; Aiken, S.; Stoodley, P. In vitro efficacy of antibiotics released from calcium sulfate bone void filler beads. Materials 2018, 11, 2265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oliver, R.A.; Lovric, V.; Christou, C.; Aiken, S.S.; Cooper, J.J.; Walsh, W.R. Application of Calcium Sulfate for Dead Space Management in Soft Tissue: Characterisation of a Novel in Vivo Response. Biomed. Res. Int. 2018, 2018. [Google Scholar] [CrossRef] [Green Version]
- Kelly, C.M.; Wilkins, R.M.; Gitelis, S.; Hartjen, C.; Watson, J.T.; Kim, P.T.; Camozzi, A.B. The use of a surgical grade calcium sulfate as a bone graft substitute: Results of a multicenter trial. Clin. Orthop. Relat. Res. 2001, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Howlin, R.P.; Brayford, M.J.; Webb, J.S.; Cooper, J.J.; Aiken, S.S.; Stoodley, P. Antibiotic-Loaded Synthetic Calcium Sulfate Beads for Prevention of Bacterial Colonization and Biofilm Formation in Periprosthetic Infections. Antimicrob. Agents Chemother. 2014, 59, 111–120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Otte, J.E.; Politi, J.R.; Chambers, B.; Smith, C.A. Intrawound Vancomycin Powder Reduces Early Prosthetic Joint Infections in Revision Hip and Knee Arthroplasty. Surg. Technol. Int. 2017, 30, 284–289. Available online: http://europepmc.org/abstract/MED/28182821 (accessed on 8 January 2020).
- Boddapati, V.; Fu, M.; Mayman, D.; Su, E.; Sculco, P.; McLawhorn, A. Revision Total Knee Arthroplasty for Periprosthetic Joint Infection Is Associated With Increased Postoperative Morbidity and Mortality Relative to Noninfectious Revisions. J Arthroplast. 2018, 33, 521–526. [Google Scholar] [CrossRef]
- Slane, J.; Gietman, B.; Squire, M. Antibiotic elution from acrylic bone cement loaded with high doses of tobramycin and vancomycin. J. Orthop. Res. 2018, 36, 1078–1085. [Google Scholar] [CrossRef] [Green Version]
- Luo, S.; Jiang, T.; Long, L.; Yang, Y.; Yang, X.; Luo, L.; Li, J.; Chen, Z.; Zou, C.; Luo, S. A dual PMMA/calcium sulfate carrier of vancomycin is more effective than PMMA-vancomycin at inhibiting Staphylococcus aureus growth in vitro. FEBS Open Bio 2020, 10, 552–560. [Google Scholar] [CrossRef]
- Galvez-Lopez, R.; Pena-Monje, A.; Antelo-Lorenzo, R.; Guardia-Olmedo, J.; Moliz, J.; Hernandez-Quero, J.; Parra-Ruiz, J. Elution kinetics, antimicrobial activity, and mexhanical properties of 11 different antibiotics loaded acrylic bone cement. Diagn. Microbiol. Infect. Dis. 2014, 78, 70–74. [Google Scholar] [CrossRef]
- Cacciola, G.; De Meo, F.; Cavaliere, P. Mechanical and elution properties of G3 Low Viscosity bone cement loaded up to three antibiotics. J. Orthop. 2018, 15, 1004–1007. [Google Scholar] [CrossRef] [PubMed]
- Samuel, S.; Mathew, B.S.; Veeraraghavan, B.; Fleming, D.H.; Chittaranjan, S.B.; Prakash, J.A.J. In vitro study of elution kinetics and bio-activity of meropenem-loaded acrylic bone cement. J. Orthop. Traumatol. 2012, 13, 131–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Porteous, A.; Bartlett, R. Post-operative drainage after cemented, hybrid and uncemented total knee replacement. KNEE 2003, 10, 371–374. [Google Scholar] [CrossRef]
- Fan, C.H.; Hung, H.H.; Chiu, K.H. Rate of drainage following total knee replacement. Hong Kong J. Orthop. Surg. 2006, 10, 10–13. [Google Scholar]
- Sterling, G.; McBain, G.D.; Harris, J.A.; Boland, M. Drainage after total knee replacement. ANZIAM J. 2006, 48, 199–210. [Google Scholar] [CrossRef] [Green Version]
- Freese, D.; Weidler, P.G.; Grolimund, D.; Sticher, H. A Flow-Through Reactor with an Infinite Sink for Monitoring Desorption Processes. J. Environ. Qual. 1999, 28, 537–543. [Google Scholar] [CrossRef]
- Miller, R.; McLaren, A.; Leon, C.; McLemore, R. Mixing method affects elution and strength of high-dose ALBC: A pilot study infection. Clin. Orthop. Relat. Res. 2012, 470, 2677–2683. [Google Scholar] [CrossRef] [Green Version]
- Matziolis, G.; Brodt, S.; Böhle, S.; Kirschberg, J.; Jacob, B.; Röhner, E. Intraarticular vancomycin powder is effective in preventing infections following total hip and knee arthroplasty. Sci. Rep. 2020, 10, 1–6. [Google Scholar] [CrossRef]
- Yavuz, I.A.; Oken, O.F.; Yildirim, A.O.; Inci, F.; Ceyhan, E.; Gurhan, U. No effect of vancomycin powder to prevent infection in primary total knee arthroplasty: A retrospective review of 976 cases. Knee Surg. Sport. Traumatol. Arthrosc. 2020, 28, 3055–3060. [Google Scholar] [CrossRef] [PubMed]
- Hanada, M.; Nishikino, S.; Hotta, K.; Furuhashi, H.; Hoshino, H.; Matsuyama, Y. Intrawound vancomycin powder increases post-operative wound complications and does not decrease periprosthetic joint infection in primary total and unicompartmental knee arthroplasties. Knee Surg. Sport. Traumatol. Arthrosc. 2019, 27, 2322–2327. [Google Scholar] [CrossRef]
- Johnson, J.D.; Nessler, J.M.; Horazdovsky, R.D.; Vang, S.; Thomas, A.J.; Marston, S.B. Serum and Wound Vancomycin Levels After Intrawound Administration in Primary Total Joint Arthroplasty. J. Arthroplast. 2017, 32, 924–928. [Google Scholar] [CrossRef]
- Tailaiti, A.; Shang, J.; Shan, S.; Muheremu, A. Effect of intrawound vancomycin application in spinal surgery on the incidence of surgical site infection: A meta-analysis. Ther. Clin. Risk Manag. 2018, 14, 2149–2159. [Google Scholar] [CrossRef] [Green Version]
- Badha, V.; Moore, R.; Heffernan, J.; Castaneda, P.; McLaren, A.; Overstreet, D. Determination of Tobramycin and Vancomycin Exposure Required to Eradicate Biofilms on Muscle and Bone Tissue In Vitro. J. Bone Jt. Infect. 2019, 4, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parker, A.C.; Smith, J.K.; Courtney, H.S.; Haggard, W.O. Evaluation of two sources of calcium sulfate for a local drug delivery system: A pilot study. Clin. Orthop. Relat. Res. 2011, 469, 3008–3015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mccarty, W.J.; Masuda, K.; Sah, R.L. Fluid movement and joint capsule strains due to flexion in rabbit knees. J. Biomech. 2011, 44, 2761–2767. [Google Scholar] [CrossRef] [Green Version]
- Kallala, R.; Edwin Harris, W.; Ibrahim, M.; Dipane, M.; McPherson, E. Use of stimulan absorbable calcium sulphate beads in revision lower limb arthroplasty. Bone Jt. Res. 2018, 7, 570–579. [Google Scholar] [CrossRef]
- Anagnostakos, K.; Meyer, C. Antibiotic Elution from Hip and Knee Acrylic Bone Cement Spacers: A Systematic Review. Biomed. Res. Int. 2017, 2017, 4657874. [Google Scholar] [CrossRef] [Green Version]
- Biocomposites Ltd. Stimulan® Rapid Cure: Instructions for Use; Biocomposites Ltd.: Keele, UK, 2019. [Google Scholar]
- Stryker® Howmedica Osteonics Corporation. Simplex™ P SpeedSet™ Radiopaque Bone Cement: Instructions for Use; Stryker® Orthopedics: Mahwah, NJ, USA, 2006. [Google Scholar]
- Cooper, J.J.; Florance, H.; McKinnon, J.L.; Laycock, P.A.; Aiken, S.S. Elution profiles of tobramycin and vancomycin from high-purity calcium sulphate beads incubated in a range of simulated body fluids. J. Biomater. Appl. 2016, 31, 357–365. [Google Scholar] [CrossRef] [PubMed]
- Biemer, J.J. Antimicrobial susceptibility testing by the Kirby-Bauer disc diffusion method. Ann. Clin. Lab. Sci. 1973, 3, 135–140. [Google Scholar] [PubMed]
- Rasband, W.S.; Imagej, U.S. National Institutes of Health: Bethesda, MD, USA, 1997–2018. Available online: https://imagej.nih.gov/ij/ (accessed on 8 January 2020).







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moore, K.; Os, R.W.-v.; Dusane, D.H.; Brooks, J.R.; Delury, C.; Aiken, S.S.; Laycock, P.A.; Sullivan, A.C.; Granger, J.F.; Dipane, M.V.; et al. Elution Kinetics from Antibiotic-Loaded Calcium Sulfate Beads, Antibiotic-Loaded Polymethacrylate Spacers, and a Powdered Antibiotic Bolus for Surgical Site Infections in a Novel In Vitro Draining Knee Model. Antibiotics 2021, 10, 270. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10030270
Moore K, Os RW-v, Dusane DH, Brooks JR, Delury C, Aiken SS, Laycock PA, Sullivan AC, Granger JF, Dipane MV, et al. Elution Kinetics from Antibiotic-Loaded Calcium Sulfate Beads, Antibiotic-Loaded Polymethacrylate Spacers, and a Powdered Antibiotic Bolus for Surgical Site Infections in a Novel In Vitro Draining Knee Model. Antibiotics. 2021; 10(3):270. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10030270
Chicago/Turabian StyleMoore, Kelly, Rebecca Wilson-van Os, Devendra H. Dusane, Jacob R. Brooks, Craig Delury, Sean S. Aiken, Phillip A. Laycock, Anne C. Sullivan, Jeffrey F. Granger, Matthew V. Dipane, and et al. 2021. "Elution Kinetics from Antibiotic-Loaded Calcium Sulfate Beads, Antibiotic-Loaded Polymethacrylate Spacers, and a Powdered Antibiotic Bolus for Surgical Site Infections in a Novel In Vitro Draining Knee Model" Antibiotics 10, no. 3: 270. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10030270