
Cross-Contamination versus Outbreak: Pre-XDR Mycobacterial Strains Confirmed by Whole-Genome Sequencing

 ,
,
Abstract
:1. Introduction
2. Results
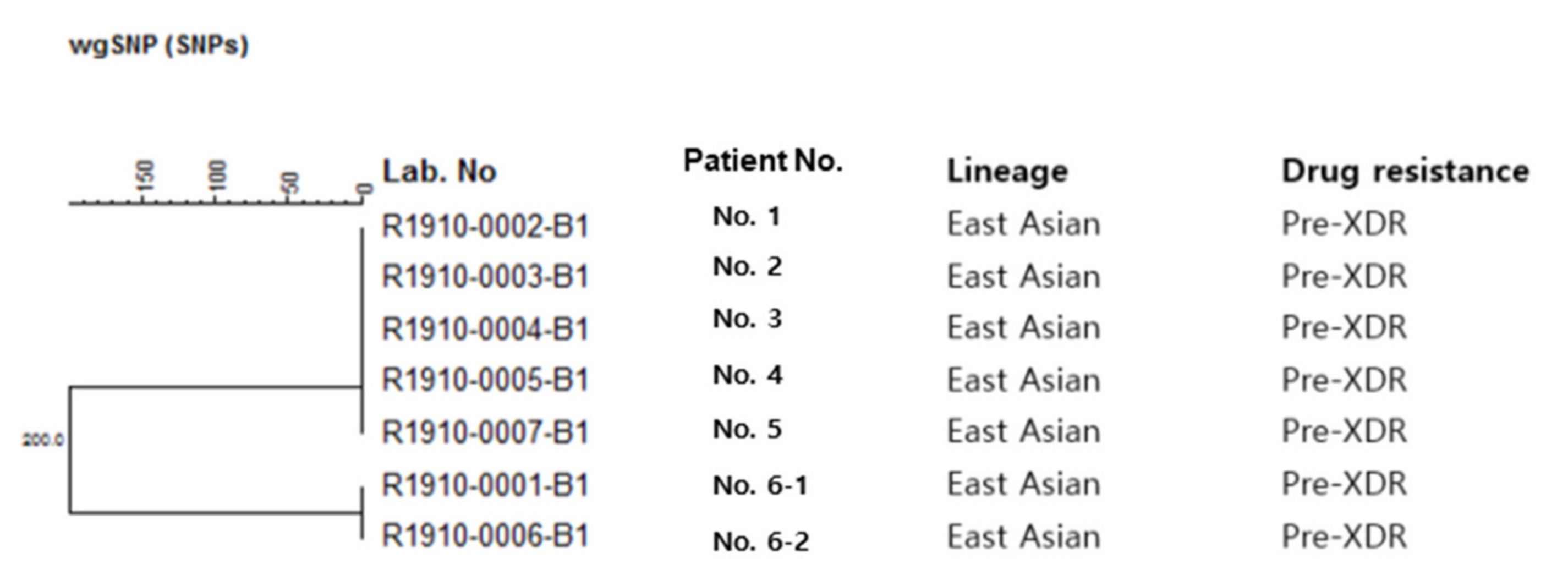
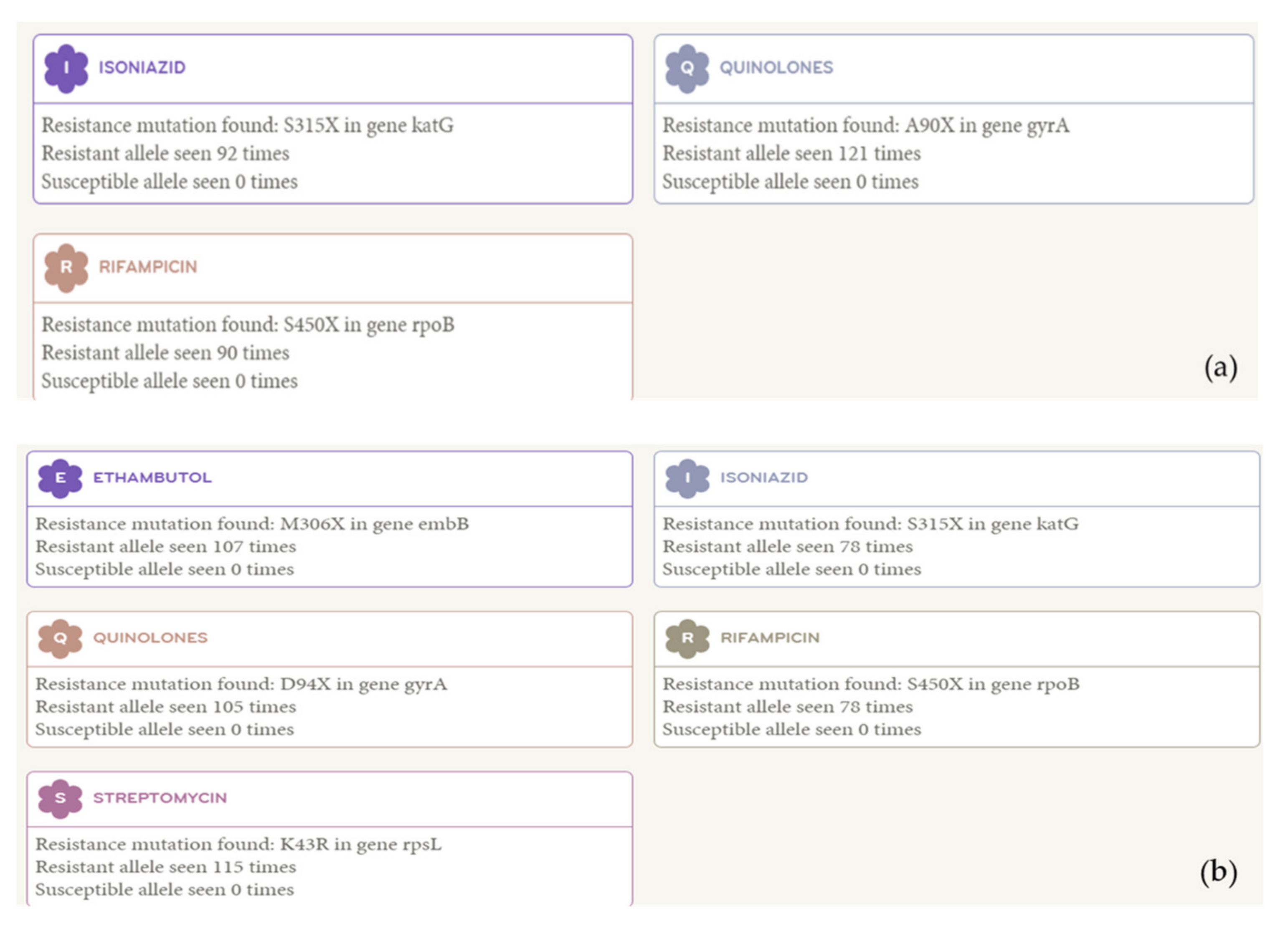
2.1. Whole-Genome Sequencing Data
2.2. Correlation with Epidemiological and Clinical Information
3. Discussion
4. Materials and Methods
4.1. Correlation with Epidemiological and Clinical Information
4.2. Whole-Genome Sequencing
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bao, H.; Liu, K.; Wu, Z.; Wang, X.; Chai, C.; He, T.; Wang, W.; Wang, F.; Peng, Y.; Chen, B. Tuberculosis outbreaks among students in mainland China: A systematic review and meta-analysis. BMC Infect. Dis. 2019, 19, 1–12. [Google Scholar] [CrossRef]
- Mindra, G.; Wortham, J.M.; Haddad, M.B.; Powell, K.M. Tuberculosis outbreaks in the United States, 2009–2015. Public Health Rep. 2017, 132, 157–163. [Google Scholar] [CrossRef] [Green Version]
- Barac, A.; Karimzadeh-Esfahani, H.; Pourostadi, M.; Rahimi, M.T.; Ahmadpour, E.; Rashedi, J.; Mahdavipoor, B.; Kafil, H.S.; Spotin, A.; Abate, K.H.; et al. Laboratory cross-contamination of Mycobacterium tuberculosis: A systematic review and meta-analysis. Lung 2019, 197, 651–661. [Google Scholar] [CrossRef] [PubMed]
- Takeda, K.; Murase, Y.; Kawashima, M.; Suzukawa, M.; Suzuki, J.; Yamane, A.; Igarashi, Y.; Chikamatsu, K.; Morishige, Y.; Aono, A.; et al. A case of Mycobacterium tuberculosis laboratory cross-contamination. J. Infect. Chemother. 2019, 25, 610–614. [Google Scholar] [CrossRef] [PubMed]
- Jasmer, R.M.; Roemer, M.; Hamilton, J.; Bunter, J.; Braden, C.R.; Shinnick, T.M.; Desmond, E.P. A prospective, multicenter study of laboratory cross-contamination of Mycobacterium tuberculosis cultures. Emerg. Infect. Dis. 2002, 8, 1260–1263. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.; Yang, C.; Lu, L.; Dai, W. Detection of tuberculosis laboratory cross-contamination using whole-genome sequencing. Tuberculosis 2019, 115, 121–125. [Google Scholar] [CrossRef]
- Asgharzadeh, M.; Ozma, M.A.; Rashedi, J.; Poor, B.M.; Agharzadeh, V.; Vegari, A.; Shokouhi, B.; Ganbarov, K.; Ghalehlou, N.N.; Leylabadlo, H.E. False-positive Mycobacterium tuberculosis detection: Ways to prevent cross-contamination. Tuberc. Respir. Dis. 2020, 83, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Allix, C.; Supply, P.; Fauville-Dufaux, M. Utility of fast Mycobacterial interspersed repetitive unit—variable number tandem repeat genotyping in clinical Mycobacteriological analysis. Clin. Infect. Dis. 2004, 39, 783–789. [Google Scholar] [CrossRef]
- Cohen, K.A.; Manson, A.L.; Desjardins, C.A.; Abeel, T.; Earl, A.M. Deciphering drug resistance in Mycobacterium tuberculosis using whole-genome sequencing: Progress, promise, and challenges. Genome Med. 2019, 11, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wyllie, D.H.; Davidson, J.A.; Grace, S.E.; Rathod, P.; Crook, D.W.; Peto, T.E.A.; Robinson, E.; Walker, T.; Campbell, C. A Quantitative evaluation of MIRU-VNTR typing against whole-genome sequencing for identifying Mycobacterium tuberculosis transmission: A prospective observational cohort study. EBioMedicine 2018, 34, 122–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryoo, S.; Lee, J.; Oh, J.Y.; Kim, B.K.; Kim, Y.; Kim, J.H.; Shin, C.; Lee, S.H. Comparing two Mycobacterium tuberculosis genomes from Chinese immigrants with native genomes using Mauve alignments. Tuberc. Respir. Dis. 2018, 81, 216–221. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, L.; Braden, C.; Cronin, W.; English, J.; Campbell, E.; Valway, S.; Onorato, I. Investigation of laboratory cross-contamination of Mycobacterium tuberculosis cultures. Clin. Infect. Dis. 2004, 38, e52–e54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seto, J.; Wada, T.; Suzuki, Y.; Ikeda, T.; Araki, K.; Umetsu, Y.; Ishikawa, H.; Mizuta, K.; Ahiko, T. A case of laboratory cross-contamination of Mycobacterium tuberculosis identified using comparative genomics. Int. J. Tuberc. Lung Dis. 2018, 22, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Simsek, H. Requirement of quality assessment for modern tuberculosis laboratory services. Mycobact. Dis. 2011, 1, 2. [Google Scholar] [CrossRef] [Green Version]
- Comin, J.; Chaure, A.; Cebollada, A.; Ibarz, D.; Viñuelas, J.; Vitoria, M.A.; Iglesias, M.J.; Samper, S. Investigation of a rapidly spreading tuberculosis outbreak using whole-genome sequencing. Infect. Genet. Evol. 2020, 81, 104184. [Google Scholar] [CrossRef] [PubMed]
- Bradley, P.; Gordon, N.C.; Walker, T.M.; Dunn, L.; Heys, S.; Huang, B.; Earle, S.; Pankhurst, L.J.; Anson, L.; Cesare, M.; et al. Rapid antibiotic-resistance predictions from genome sequence data for Staphylococcus aureus and Mycobacterium tuberculosis. Nat. Commn. 2015, 6, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Case No. | Smear Date | Smear Results * | Culture Date | Culture Results | Concordance of Strain | H | RFP | SM | E | Km | Cm | PTH | CS | PAS | Ofx | Mfx | Amk | Lfx | Rib | Z | LNZ |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No. 1 | 21 May | − | 21 May | 1+ | Concordant 1 | R | R | R | R | S | S | S | S | S | R | R | S | R | R | R | S |
| 23 May | 4+ | 23 May | 4+ | ||||||||||||||||||
| 24 May | 4+ | 24 May | 1+ | ||||||||||||||||||
| 25 May | 4+ | 25 May | 1+ | ||||||||||||||||||
| 26 May | 4+ | 26 May | 1+ | ||||||||||||||||||
| 1st June | 2+ | 1 June | 1+ | ||||||||||||||||||
| No. 1 WGS | R | R | S | S | S | S | S | S | S | R | R | S | R | R | R | S | |||||
| No. 2 | 24 May | − | 25 May | 1+ | R | R | R | R | S | S | S | S | S | R | R | S | R | R | R | S | |
| No. 2. WGS | R | R | S | S | S | S | S | S | S | R | R | S | R | R | R | S | |||||
| No. 3 | 27 May | − | 27 May | 2+ | R | R | R | R | S | S | S | S | S | R | R | S | R | R | R | S | |
| No. 3 WGS | R | R | S | S | S | S | S | S | S | R | R | S | R | R | R | S | |||||
| No. 4 | 24 May | − | 24 May | 1+ | R | R | R | R | S | S | S | S | S | R | R | S | R | R | R | S | |
| No. 4 WGS | R | R | S | S | S | S | S | S | S | R | R | S | R | R | R | S | |||||
| No. 5 | 27 May | − | 27 May | 2+ | R | R | R | R | S | S | S | S | S | R | R | S | R | R | R | S | |
| No. 5 WGS | R | R | S | S | S | S | S | S | S | R | R | S | R | R | R | S | |||||
| No. 6-1 (sputum) | 2 June | + | 26 June | 1+ | Concordant 2 | R | R | R | R | S | S | S | S | S | S | S | S | S | R | R | S |
| No. 6-1 WGS | R | R | R | R | S | S | S | S | S | R | R | S | R | R | R | S | |||||
| No. 6-2 (bfs) | 4 July | 2+ | 4 July | 1+ | R | R | R | R | S | S | S | S | S | R | R | S | R | R | R | S | |
| No. 6-2 WGS | R | R | R | R | S | S | S | S | S | R | R | S | R | R | R | S |
| Case No. | Age/Sex | Underlying Disease | Symptoms | Past TB History | Chest CT Findings | Bronchoscopy | TB Treatment | Clinical Diagnosis | Laboratory Investigation | |
|---|---|---|---|---|---|---|---|---|---|---|
| Previous Hospital | After Referral | |||||||||
| 1 | 58/Male | Chronic alcoholics | Fever, anorexia | − | Multiple cavities and consolidation in both lungs | Not done | Yes | Expired | Active TB | True strain |
| 2 | 69/Male | DM, HTN, Cerebral infarction | Cough, sputum | + | Multiple centrilobular GGOs and nodules in RML/RLL | No endobronchial lesion | Yes | No | CAP | Contamination |
| 3 | 73/Female | HTN, Spinal stenosis | Cough, sputum | − | Diffuse ill-defined centrilobular nodules and GGO in both lungs | Anthracofibrosis | Yes | No | Bronchitis | Contamination |
| 4 | 71/Male | HTN, Asthma, Unstable angina, CKD, Panic disorder | General weakness | + | Multiple calcified granulomas, irregular pleural thickening, and bronchiectasis | Anthracofibrosis | Yes | Yes | Bronchitis | Contamination |
| 5 | 32/Female | none | Cough, sputum | + | Consolidation, calcified granulomas, fibrosis, and pleural thickening in both lungs | Anthracotic pigmentation | Yes | No | CAP | Contamination |
| 6 | 55/Female | HTN | Cough, sputum | − | Multiple ill-defined centrilobular nodules and patchy consolidations in LUL | Endobronchial TB (left main) | Yes | Yes | Active TB | True strain |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, J.Y.; Park, K.H.; Lee, J.; Kim, D.; Seok, K.H.; Oh, I.-H.; Lee, S.H. Cross-Contamination versus Outbreak: Pre-XDR Mycobacterial Strains Confirmed by Whole-Genome Sequencing. Antibiotics 2021, 10, 297. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10030297
Oh JY, Park KH, Lee J, Kim D, Seok KH, Oh I-H, Lee SH. Cross-Contamination versus Outbreak: Pre-XDR Mycobacterial Strains Confirmed by Whole-Genome Sequencing. Antibiotics. 2021; 10(3):297. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10030297
Chicago/Turabian StyleOh, Jee Youn, Kyung Ho Park, Jisoon Lee, Donghyeok Kim, Kwang Hyuk Seok, In-Hwan Oh, and Seung Heon Lee. 2021. "Cross-Contamination versus Outbreak: Pre-XDR Mycobacterial Strains Confirmed by Whole-Genome Sequencing" Antibiotics 10, no. 3: 297. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10030297