
Antibiotic Resistance in Wastewater Treatment Plants and Transmission Risks for Employees and Residents: The Concept of the AWARE Study

 , , , , ,
, , , , ,
Abstract
:1. Introduction
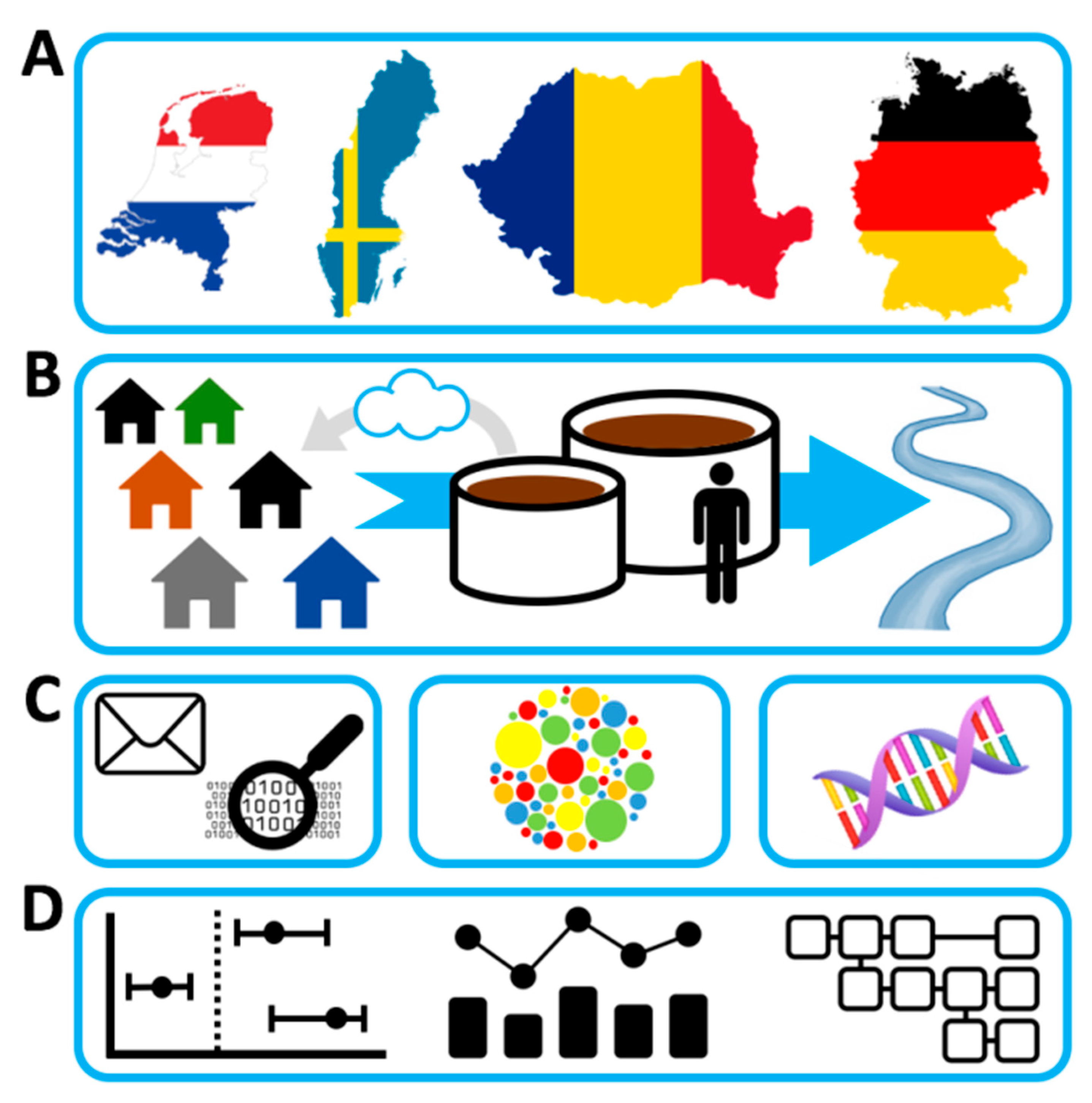
- To study carriage rates of ESBL-EC, CPE, and of a range of clinically relevant ARGs in WWTP workers and nearby residents (living within ≤300 m vicinity of a WWTP) compared to a comparison group (living 1000 m away from the closest WWTP);
- To study waterborne and airborne exposure to ESBL-EC, CPE, and of a range of clinically relevant ARGs in WWTP workers through ingestion and inhalation;
- To assess the efficiency of different WWTP treatment technologies in diminishing ESBL-EC, CPE, and a range of clinically relevant ARGs; and
- To investigate selection and emergence of ESBL-EC, CPE, and a range of clinically relevant ARGs in WWTPs through studying relative changes in resistance genes and exploring putative novel resistance genes from metagenomics data.
2. Materials and Methods
2.1. Study Design
2.2. Study Population
2.3. Recruitment Process
2.4. Pilot Study
2.5. Study Instruments
2.5.1. Study Questionnaires
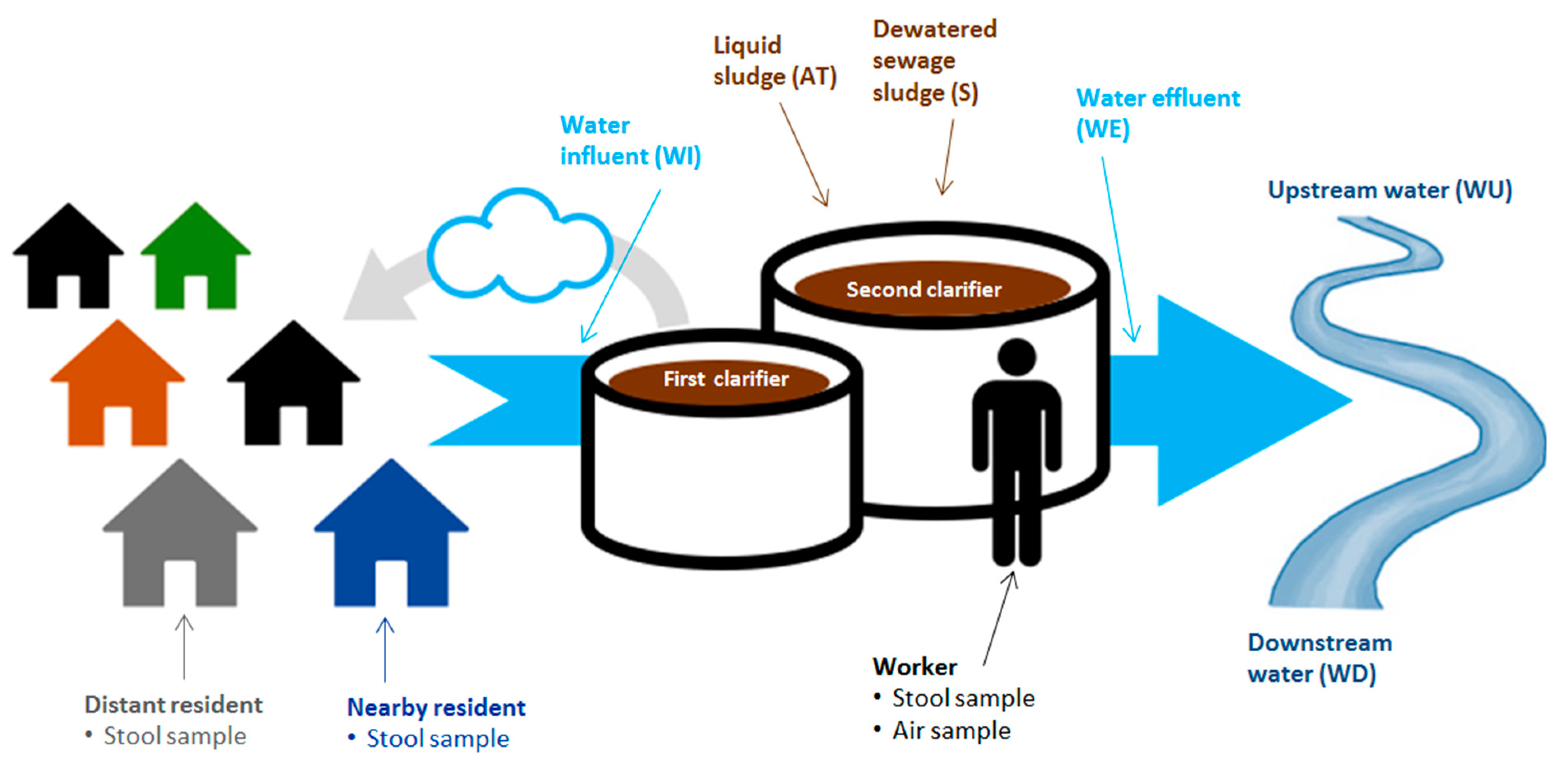
2.5.2. Stool Samples
2.5.3. Water Samples
2.5.4. Air Samples
2.6. Metagenomic Analysis
2.7. Data Management
2.8. Statistical Analysis
3. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Berendonk, T.U.; Manaia, C.M.; Merlin, C.; Fatta-Kassinos, D.; Cytryn, E.; Walsh, F.; Buergmann, H.; Sørum, H.; Norström, M.; Pons, M.-N.; et al. Tackling antibiotic resistance: The environmental framework. Nat. Rev. Genet. 2015, 13, 310–317. [Google Scholar] [CrossRef] [PubMed]
- Martinez, J.L.; Fajardo, A.; Garmendia, L.; Hernandez, A.; Linares, J.F.; Martãnez-Solano, L.; Sánchez, M.B. A global view of antibiotic resistance. FEMS Microbiol. Rev. 2009, 33, 44–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bengtsson-Palme, J.; Kristiansson, E.; Larsson, D.G.J. Environmental factors influencing the development and spread of antibiotic resistance. FEMS Microbiol. Rev. 2018, 42. [Google Scholar] [CrossRef]
- Larsson, D.G.J.; Andremont, A.; Bengtsson-Palme, J.; Brandt, K.K.; Husman, A.M.D.R.; Fagerstedt, P.; Fick, J.; Flach, C.-F.; Gaze, W.H.; Kuroda, M.; et al. Critical knowledge gaps and research needs related to the environmental dimensions of antibiotic resistance. Environ. Int. 2018, 117, 132–138. [Google Scholar] [CrossRef] [PubMed]
- Paltansing, S.; Vlot, J.A.; Kraakman, M.E.; Mesman, R.; Bruijning, M.L.; Bernards, A.T.; Visser, L.G.; Veldkamp, K.E. Extended-Spectrum β-Lactamase–producingEnterobacteriaceaeamong Travelers from the Netherlands. Emerg. Infect. Dis. 2013, 19, 1206–1213. [Google Scholar] [CrossRef] [PubMed]
- Graveland, H.; Wagenaar, J.A.; Heesterbeek, H.; Mevius, D.; Van Duijkeren, E.; Heederik, D. Methicillin Resistant Staphylococcus aureus ST398 in Veal Calf Farming: Human MRSA Carriage Related with Animal Antimicrobial Usage and Farm Hygiene. PLoS ONE 2010, 5, e10990. [Google Scholar] [CrossRef] [Green Version]
- Carrel, M.; Schweizer, M.L.; Sarrazin, M.V.; Smith, T.C.; Perencevich, E.N. Residential Proximity to Large Numbers of Swine in Feeding Operations Is Associated with Increased Risk of Methicillin-Resistant Staphylococcus aureus Colonization at Time of Hospital Admission in Rural Iowa Veterans. Infect. Control. Hosp. Epidemiol. 2014, 35, 190–192. [Google Scholar] [CrossRef]
- Huijbers, P.M.C.; Blaak, H.; De Jong, M.C.M.; Graat, E.A.M.; Vandenbroucke-Grauls, C.M.J.E.; Husman, A.M.D.R. Role of the Environment in the Transmission of Antimicrobial Resistance to Humans: A Review. Environ. Sci. Technol. 2015, 49, 11993–12004. [Google Scholar] [CrossRef]
- Leonard, A.F.; Zhang, L.; Balfour, A.J.; Garside, R.; Hawkey, P.M.; Murray, A.K.; Ukoumunne, O.C.; Gaze, W.H. Exposure to and colonisation by antibiotic-resistant E. coli in UK coastal water users: Environmental surveillance, exposure assessment, and epidemiological study (Beach Bum Survey). Environ. Int. 2018, 114, 326–333. [Google Scholar] [CrossRef]
- Rodríguez-Molina, D.; Mang, P.; Schmitt, H.; Chifiriuc, M.C.; Radon, K.; Wengenroth, L. Do wastewater treatment plants increase antibiotic resistant bacteria or genes in the environment? Protocol for a systematic review. Syst. Rev. 2019, 8, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Søraas, A.; Sundsfjord, A.; Sandven, I.; Brunborg, C.; Jenum, P.A. Risk Factors for Community-Acquired Urinary Tract Infections Caused by ESBL-Producing Enterobacteriaceae—A Case—Control Study in a Low Prevalence Country. PLoS ONE 2013, 8, e69581. [Google Scholar] [CrossRef] [Green Version]
- Wuijts, S.; van den Berg, H.H.; Miller, J.; Abebe, L.; Sobsey, M.; Andremont, A.; Medlicott, K.O.; Van Passel, M.W.J.; Husman, A.M.D.R. Towards a research agenda for water, sanitation and antimicrobial resistance. J. Water Health 2017, 15, 175–184. [Google Scholar] [CrossRef] [Green Version]
- Pal, C.; Bengtsson-Palme, J.; Rensing, C.; Kristiansson, E.; Larsson, D.G.J. BacMet: Antibacterial biocide and metal resistance genes database. Nucleic Acids Res. 2014, 42, D737–D743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pal, C.; Bengtsson-Palme, J.; Kristiansson, E.; Larsson, D.G.J. Co-occurrence of resistance genes to antibiotics, biocides and metals reveals novel insights into their co-Selection potential. BMC Genom. 2015, 16, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Gaze, W.H.; Krone, S.M.; Larsson, D.G.J.; Li, X.-Z.; Robinson, J.A.; Simonet, P.; Smalla, K.; Timinouni, M.; Topp, E.; Wellington, E.M.; et al. Influence of Humans on Evolution and Mobilization of Environmental Antibiotic Resistome. Emerg. Infect. Dis. 2013, 19. [Google Scholar] [CrossRef]
- Finley, R.L.; Collignon, P.; Larsson, D.G.J.; McEwen, S.A.; Li, X.-Z.; Gaze, W.H.; Reid-Smith, R.; Timinouni, M.; Graham, D.W.; Topp, E. The Scourge of Antibiotic Resistance: The Important Role of the Environment. Clin. Infect. Dis. 2013, 57, 704–710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boulund, F.; Johnning, A.; Pereira, M.B.; Larsson, D.G.J.; Kristiansson, E. A novel method to discover fluoroquinolone antibiotic resistance (qnr) genes in fragmented nucleotide sequences. BMC Genom. 2012, 13, 695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berglund, F.; Marathe, N.P.; Österlund, T.; Bengtsson-Palme, J.; Kotsakis, S.; Flach, C.-F.; Larsson, D.G.J.; Kristiansson, E. Identification of 76 novel B1 metallo-β-lactamases through large-scale screening of genomic and metagenomic data. Microbiome 2017, 5, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Bréchet, C.; Plantin, J.; Sauget, M.; Thouverez, M.; Talon, D.; Cholley, P.; Guyeux, C.; Hocquet, D.; Bertrand, X. Wastewater Treatment Plants Release Large Amounts of Extended-Spectrum β-Lactamase–Producing Escherichia coli Into the Environment. Clin. Infect. Dis. 2014, 58, 1658–1665. [Google Scholar] [CrossRef] [PubMed]
- Wilson, H.; Török, M.E. Corrigendum: Extended-spectrum β-lactamase-producing and carbapenemase-producing Enterobacteriaceae. Microb. Genom. 2018, 4, e000218. [Google Scholar] [CrossRef]
- Thakali, O.; Brooks, J.P.; Shahin, S.; Sherchan, S.P.; Haramoto, E. Removal of Antibiotic Resistance Genes at Two Conventional Wastewater Treatment Plants of Louisiana, USA. Water 2020, 12, 1729. [Google Scholar] [CrossRef]
- Pruden, A.; Larsson, D.G.J.; Amézquita, A.; Collignon, P.; Brandt, K.K.; Graham, D.W.; Lazorchak, J.M.; Suzuki, S.; Silley, P.; Snape, J.R.; et al. Management Options for Reducing the Release of Antibiotics and Antibiotic Resistance Genes to the Environment. Environ. Health Perspect. 2013, 121, 878–885. [Google Scholar] [CrossRef]
- Rizzo, L.; Manaia, C.; Merlin, C.; Schwartz, T.; Dagot, C.; Ploy, M.C.; Michael, I.; Fatta-Kassinos, D. Urban wastewater treatment plants as hotspots for antibiotic resistant bacteria and genes spread into the environment: A review. Sci. Total Environ. 2013, 447, 345–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pallares-Vega, R.; Blaak, H.; van der Plaats, R.; Husman, A.M.D.R.; Leal, L.H.; van Loosdrecht, M.C.; Weissbrodt, D.G.; Schmitt, H. Determinants of presence and removal of antibiotic resistance genes during WWTP treatment: A cross-Sectional study. Water Res. 2019, 161, 319–328. [Google Scholar] [CrossRef] [PubMed]
- Yang, K.; Li, L.; Wang, Y.; Xue, S.; Han, Y.; Liu, J. Airborne bacteria in a wastewater treatment plant: Emission characterization, source analysis and health risk assessment. Water Res. 2019, 149, 596–606. [Google Scholar] [CrossRef]
- Cyprowski, M.; Stobnicka-Kupiec, A.; Ławniczek-Wałczyk, A.; Bakal-Kijek, A.; Gołofit-Szymczak, M.; Górny, R.L. Anaerobic bacteria in wastewater treatment plant. Int. Arch. Occup. Environ. Health 2018, 91, 571–579. [Google Scholar] [CrossRef] [Green Version]
- Xu, P.; Zhang, C.; Mou, X.; Wang, X.C. Bioaerosol in a typical municipal wastewater treatment plant: Concentration, size distribution, and health risk assessment. Water Sci. Technol. 2020, 82, 1547–1559. [Google Scholar] [CrossRef] [PubMed]
- Heinonen-Tanski, H.; Reponen, T.; Koivunen, J. Airborne enteric coliphages and bacteria in sewage treatment plants. Water Res. 2009, 43, 2558–2566. [Google Scholar] [CrossRef]
- Xu, G.; Han, Y.; Li, L.; Liu, J. Characterization and source analysis of indoor/outdoor culturable airborne bacteria in a municipal wastewater treatment plant. J. Environ. Sci. 2018, 74, 71–78. [Google Scholar] [CrossRef]
- Thorn, J.; Beijer, L. Work-related Symptoms and Inflammation among Sewage Plant Operatives. Int. J. Occup. Environ. Health 2004, 10, 84–89. [Google Scholar] [CrossRef]
- Schöniger-Hekele, M.; Petermann, D.; Weber, B.; Müller, C. Tropheryma whipplei in the Environment: Survey of Sewage Plant Influxes and Sewage Plant Workers. Appl. Environ. Microbiol. 2007, 73, 2033–2035. [Google Scholar] [CrossRef] [Green Version]
- Van Hooste, W.; Charlier, A.-M.; Rotsaert, P.; Bulterys, S.; Moens, G.; Van Sprundel, M.; De Schryver, A. Work-related Helicobacter pylori infection among sewage workers in municipal wastewater treatment plants in Belgium. Occup. Environ. Med. 2010, 67, 91–97. [Google Scholar] [CrossRef]
- Albatanony, M.A.; El-Shafie, M.K. Work-related health effects among wastewater treatment plants workers. Int. J. Occup. Environ. Med. 2011, 2, 237–244. [Google Scholar]
- Gilchrist, M.J.; Greko, C.; Wallinga, D.B.; Beran, G.W.; Riley, D.G.; Thorne, P.S. The Potential Role of Concentrated Animal Feeding Operations in Infectious Disease Epidemics and Antibiotic Resistance. Environ. Health Perspect. 2007, 115, 313–316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dohmen, W.; Van Gompel, L.; Schmitt, H.; Liakopoulos, A.; Heres, L.; Urlings, B.A.; Mevius, D.; Bonten, M.J.M.; Heederik, D.J.J. ESBL carriage in pig slaughterhouse workers is associated with occupational exposure. Epidemiol. Infect. 2017, 145, 2003–2010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burney, P.; Luczynska, C.; Chinn, S.; Jarvis, D. The European Community Respiratory Health Survey. Eur. Respir. J. 1994, 7, 954–960. [Google Scholar] [CrossRef] [PubMed]
- Németh, G. Health related quality of life outcome instruments. Eur. Spine J. 2005, 15, S44–S51. [Google Scholar] [CrossRef] [Green Version]
- Heinrich, S.; Peters, A.; Kellberger, J.; Ellenberg, D.; Genuneit, J.; Nowak, D.; Vogelberg, C.; Von Mutius, E.; Weinmayr, G.; Radon, K. Study on Occupational Allergy Risks (SOLAR II) in Germany: Design and methods. BMC Public Health 2011, 11, 298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sandrock, S.; Schutte, M.; Griefahn, B. The reliability of the noise sensitivity questionnaire in a cross-National analysis. Noise Health 2007, 9, 8–14. [Google Scholar] [CrossRef]
- Schutte, M.; Marks, A.; Wenning, E.; Griefahn, B. The development of the noise sensitivity questionnaire. Noise Health 2007, 9, 15–24. [Google Scholar] [CrossRef]
- Schutte, M.; Sandrock, S.; Griefahn, B. Factorial validity of the noise sensitivity questionnaire. Noise Health 2007, 9, 96–100. [Google Scholar] [CrossRef] [PubMed]
- Alavanja, M.C.; Sandler, D.P.; McMaster, S.B.; Zahm, S.H.; McDonnell, C.J.; Lynch, C.F.; Pennybacker, M.; Rothman, N.; Dosemeci, M.; Bond, A.E.; et al. The Agricultural Health Study. Environ. Health Perspect. 1996, 104, 362–369. [Google Scholar] [CrossRef] [PubMed]
- Bisdorff, B.; Scholhölter, J.L.; Claußen, K.; Pulz, M.; Nowak, D.; Radon, K. MRSA-ST398 in livestock farmers and neighbouring residents in a rural area in Germany. Epidemiol. Infect. 2012, 140, 1800–1808. [Google Scholar] [CrossRef] [Green Version]
- O’Loughlin, J.; Dugas, E.N.; Brunet, J.; DiFranza, J.; Engert, J.C.; Gervais, A.; Gray-Donald, K.; Karp, I.; Low, N.C.; Sabiston, C.; et al. Cohort Profile: The Nicotine Dependence in Teens (NDIT) Study. Int. J. Epidemiol. 2014, 44, 1537–1546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Council, N.R. National Survey Data on Food Consumption: Uses and Recommendations; The National Academies Press: Washington, DC, USA, 1984; p. 142. [Google Scholar]
- LimeSurvey. LimeSurvey: An Open Source Survey Tool; LimeSurvey: Hamburg, Germany, 2012. [Google Scholar]
- Ebengtsson-Palme, J.; Eboulund, F.; Efick, J.; Ekristiansson, E.; Larsson, D.G.J. Shotgun metagenomics reveals a wide array of antibiotic resistance genes and mobile elements in a polluted lake in India. Front. Microbiol. 2014, 5, 648. [Google Scholar] [CrossRef] [Green Version]
- Bengtsson-Palme, J.; Angelin, M.; Huss, M.; Kjellqvist, S.; Kristiansson, E.; Palmgren, H.; Larsson, D.G.J.; Johansson, A. The Human Gut Microbiome as a Transporter of Antibiotic Resistance Genes between Continents. Antimicrob. Agents Chemother. 2015, 59, 6551–6560. [Google Scholar] [CrossRef] [Green Version]
- Lundström, S.V.; Östman, M.; Bengtsson-Palme, J.; Rutgersson, C.; Thoudal, M.; Sircar, T.; Blanck, H.; Eriksson, K.M.; Tysklind, M.; Flach, C.-F.; et al. Minimal selective concentrations of tetracycline in complex aquatic bacterial biofilms. Sci. Total. Environ. 2016, 553, 587–595. [Google Scholar] [CrossRef] [Green Version]
- Gweon, H.S.; on behalf of the REHAB consortium; Shaw, L.P.; Swann, J.; De Maio, N.; AbuOun, M.; Niehus, R.; Hubbard, A.T.M.; Bowes, M.J.; Bailey, M.J.; et al. The impact of sequencing depth on the inferred taxonomic composition and AMR gene content of metagenomic samples. Environ. Microbiome 2019, 14, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Bengtsson-Palme, J.; Larsson, D.G.J. Concentrations of antibiotics predicted to select for resistant bacteria: Proposed limits for environmental regulation. Environ. Int. 2016, 86, 140–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jutkina, J.; Marathe, N.; Flach, C.-F.; Larsson, D.G.J. Antibiotics and common antibacterial biocides stimulate horizontal transfer of resistance at low concentrations. Sci. Total. Environ. 2018, 616–617, 172–178. [Google Scholar] [CrossRef]
- Wilkinson, M.D.; Dumontier, M.; Aalbersberg, I.J.; Appleton, G.; Axton, M.; Baak, A.; Blomberg, N.; Boiten, J.-W.; da Silva Santos, L.B.; Bourne, P.E.; et al. The FAIR Guiding Principles for scientific data management and stewardship. Sci. Data 2016, 3, 160018, Addendum in 2019, 6, 1–2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2018; Available online: https://cran.r-project.org/doc/manuals/r-release/fullrefman.pdf (accessed on 20 April 2021).



{kind=link}
{kind=link}
| Germany | The Netherlands | Romania | |
|---|---|---|---|
| Selection of WWTPs | Eligible WWTPs are selected due to the following criteria: There are residents living in <300 m vicinity of WWTP, WWTP is located close enough to laboratories for the analyses of samples | All 21 regional waterboards 3 are included. | WWTPs are chosen to assure a good representativeness of different regions across the country. |
| Invitation of WWTPs | The operators of the WWTPs are contacted by the local study team and asked to participate. | The waterboards are informed of the study through the Dutch Water Authorities and asked to participate. | The operators of the WWTPs are contacted by the local study team and asked to participate. |
| Response in WWTPs | 8 WWTPs are interested in participating. | 12 waterboards are interested in participating 4. | 9 WWTPs are interested in participating. |
| Study presentation and informing of WWTP workers | The study team visits 6 interested WWTPs and presents the project to the workers 1. | The WWTP workers of 10 waterboards are invited to attend a presentation of the study by the local study team 5. The workers of the remaining 2 waterboards are recruited internally through email. By sending the presentation to all workers via email, also workers not attending the meeting are reached. | The WWTP operators inform and invite the employees to participate. Afterwards, several short information sessions are organized at the WWTPs for recruiting participants. |
| Informing of nearby residents | The study team researches the street names of all streets within ≤300 m vicinity of a participating WWTP through Google Maps and asks the local registration office 2 for the full address of all persons aged 16–67 years and having their main residence in those streets. | Due to concerns of the waterboards, residents living in ≤300 m vicinity of a WWTP cannot be included. | Invitations to the study are done using door-to-door approach. Additionally, in public places like streets, parks, and markets, potential participants are orally addressed and information sheets with details about the study are distributed. The participants are at least 18 years old. |
| Informing of comparison group | The addresses are collected in the same way as for the nearby residents, except that addresses >1000 m away from the closest WWTP and close to a train station are chosen to allow fast transportation of samples by the study team. | All addresses within a 500 m radius of GPs, who are willing to cooperate, are identified 6. Then, 300–500 addresses per GP are randomly selected to extract personal data from the Dutch Personal Records Database (BRP). Information on the study is sent to all residents living at the selected addresses over 16 years of age. | Same procedure as for nearby residents |
| Incentives for participants 7 | Participants participate in a raffle with 10 shopping vouchers with a total value of 1500 Euros. | Every participant receives a gift card worth 20 Euro. | Every participant is granted 5 Euro. |
| Timing of sample taking | To control for seasonal variation of ESBL-EC, CPE, and ARGs all samples (water, air, stool) from the surroundings of one WWTP are aimed to be taken within eight weeks. | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wengenroth, L.; Berglund, F.; Blaak, H.; Chifiriuc, M.C.; Flach, C.-F.; Pircalabioru, G.G.; Larsson, D.G.J.; Marutescu, L.; van Passel, M.W.J.; Popa, M.; et al. Antibiotic Resistance in Wastewater Treatment Plants and Transmission Risks for Employees and Residents: The Concept of the AWARE Study. Antibiotics 2021, 10, 478. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10050478
Wengenroth L, Berglund F, Blaak H, Chifiriuc MC, Flach C-F, Pircalabioru GG, Larsson DGJ, Marutescu L, van Passel MWJ, Popa M, et al. Antibiotic Resistance in Wastewater Treatment Plants and Transmission Risks for Employees and Residents: The Concept of the AWARE Study. Antibiotics. 2021; 10(5):478. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10050478
Chicago/Turabian StyleWengenroth, Laura, Fanny Berglund, Hetty Blaak, Mariana Carmen Chifiriuc, Carl-Fredrik Flach, Gratiela Gradisteanu Pircalabioru, D. G. Joakim Larsson, Luminita Marutescu, Mark W. J. van Passel, Marcela Popa, and et al. 2021. "Antibiotic Resistance in Wastewater Treatment Plants and Transmission Risks for Employees and Residents: The Concept of the AWARE Study" Antibiotics 10, no. 5: 478. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10050478