
Photodynamic Therapy for the Treatment of Infected Leg Ulcers—A Pilot Study


 ,
,  and
and
Abstract
:1. Introduction
1.1. LUs—Epidemiology
1.2. LUs—Etiopathogenesis
1.3. Symptoms of LUs
1.4. LU Infection
1.5. LU Therapy
1.6. PDT
2. Results
Adverse Reactions
3. Discussion
4. Materials and Methods
- -
- advanced atherosclerotic changes requiring angiosurgical treatment (color Doppler ultrasounds, 3D computed tomography angiography—angiogram);
- -
- cancer;
- -
- severe debilitating diseases;
- -
- severe respiratory and cardiovascular diseases;
- -
- venous thromboembolism;
- -
- increased side effects of therapy;
- -
- presence of hypersensitivity or allergy to any of the substances under study;
- -
- pregnancy.
- -
- patients of both sexes aged 40–85 years (Figure 10), with chronic leg ulcers, who had not responded well to conventional treatment;
- -
- no use of topical pharmaceutical products or systemic drugs (antibiotics) for at least 4 weeks.
4.1. Diagnostics
4.2. Drug Application
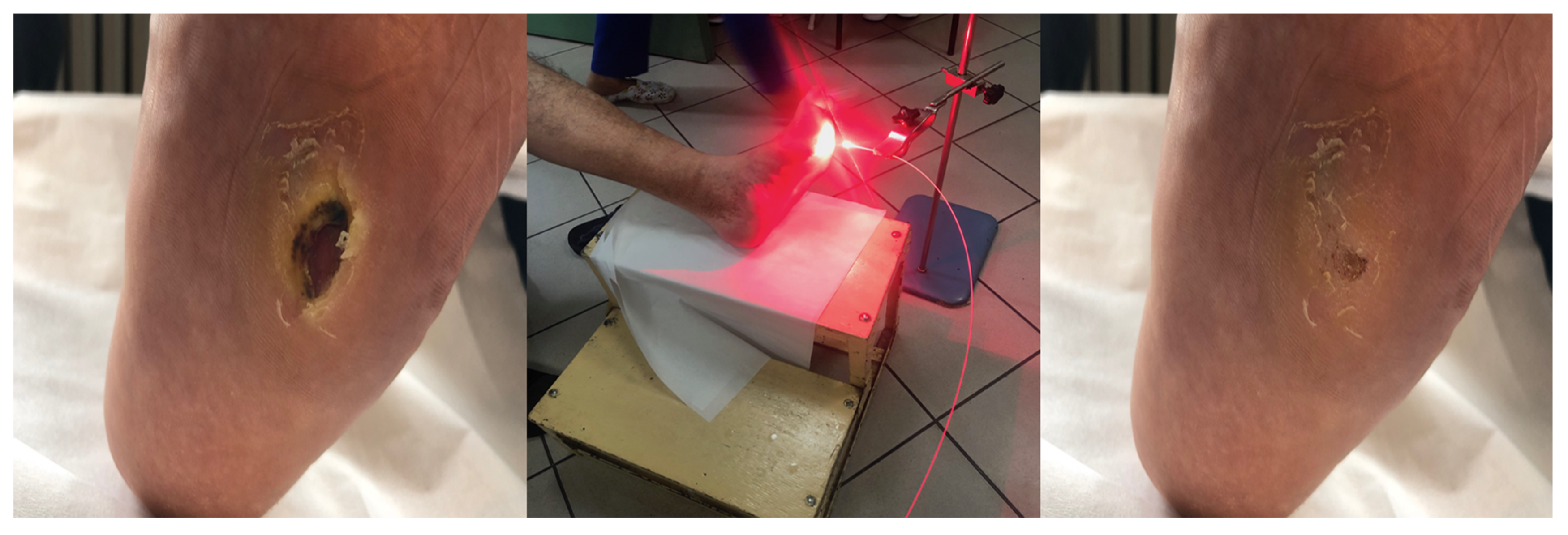
4.3. PDT Procedure
4.4. Follow-Up Study
4.5. Statistics
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nelson, E.A.; Adderley, U. Venous leg ulcers. BMJ Clin. Evid. 2016, 2016, 1902. [Google Scholar] [PubMed]
- Lim, C.S.; Baruah, M.; Bahia, S.S. Diagnosis and management of venous leg ulcers. BMJ 2018, 362, k3115. [Google Scholar] [CrossRef] [PubMed]
- Sen, C.K.; Gordillo, G.M.; Roy, S.; Kirsner, R.; Lambert, L.; Hunt, T.K.; Gottrup, F.; Gurtner, G.C.; Longaker, M.T. Human skin wounds: A major and snowballing threat to public health and the economy. Wound Repair Regen. 2009, 17, 763–771. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Platsidaki, E.; Kouris, A.; Christodoulou, C. Psychosocial Aspects in Patients With Chronic Leg Ulcers. Wounds 2017, 29. [Google Scholar] [CrossRef] [PubMed]
- Brown, E.D.; Wright, G.D. Antibacterial drug discovery in the resistance era. Nature 2016, 529, 336–343. [Google Scholar] [CrossRef] [PubMed]
- Davies, J.; Davies, D. Origins and Evolution of Antibiotic Resistance. Microbiol. Mol. Biol. Rev. 2010, 74, 417–433. [Google Scholar] [CrossRef] [Green Version]
- Bui, U.T.; Finlayson, K.; Edwards, H. The diagnosis of infection in chronic leg ulcers: A narrative review on clinical practice. Int. Wound J. 2019, 16, 601–620. [Google Scholar] [CrossRef]
- Vestby, L.K.; Grønseth, T.; Simm, R.; Nesse, L.L. Bacterial Biofilm and its Role in the Pathogenesis of Disease. Antibiotic 2020, 9, 59. [Google Scholar] [CrossRef] [Green Version]
- Hafner, J.; Buset, C.; Anzengruber, F.; Barysch-Bonderer, M.; Läuchli, S.; Müller, H.; Meier, T.O.; Ulmer, N.; Reutter, D.; Kucher, N.; et al. Ulcus cruris: Die häufigen, makrovaskulären Ursachen [Leg ulcers (ulcus cruris): The frequent macrovascular causes]. Ther. Umsch. 2018, 75, 506–514. [Google Scholar] [CrossRef]
- Abbade, L.P.F.; Frade, M.A.C.; Pegas, J.R.P.; Dadalti-Granja, P.; Garcia, L.C.; Filho, R.B.; Parenti, C.E.F. Consensus on the diagnosis and management of chronic leg ulcers—Brazilian Society of Dermatology. An. Bras. Dermatol. 2020, 95 (Suppl. 1), 1–18. [Google Scholar] [CrossRef]
- Dissemond, J. Chronisches Ulcus cruris Chronic leg ulcers. Der Hautarzt 2017, 68, 614–620. [Google Scholar] [CrossRef] [PubMed]
- Anaya-López, J.L.; López-Meza, J.E.; Ochoa-Zarzosa, A. Bacterial resistance to cationic antimicrobial peptides. Crit. Rev. Microbiol. 2013, 39, 180–195. [Google Scholar] [CrossRef] [PubMed]
- Agostinis, P.; Berg, K.; Cengel, K.A.; Foster, T.H.; Girotti, A.W.; Gollnick, S.O.; Hahn, S.M.; Hamblin, M.R.; Juzeniene, A.; Kessel, D.; et al. Photodynamic therapy of cancer: An update. CA Cancer J. Clin. 2011, 61, 250–281. [Google Scholar] [CrossRef]
- Hamblin, M.R.; Hasan, T. Photodynamic therapy: A new antimicrobial approach to infectious disease? Photochem. Photobiol. Sci. 2004, 3, 436–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Callam, M.J.; Harper, D.R.; Dale, J.J.; Ruckley, C.V. Chronic ulcer of the leg: Clinical history. BMJ 1987, 294, 1389–1391. [Google Scholar] [CrossRef] [Green Version]
- Nicolaides, A.N.; Cardiovascular Disease Educational and Research Trust; European Society of Vascular Surgery; The International Angiology Scientific Activity Congress Organization; International Union of Angiology; Union Internationale de Phlebologie at the Abbaye des Vaux de Cernay. Investigation of chronic venous insufficiency: A consensus statement (France, 5–9 March 1997). Circulation 2000, 102, e126–e163. [Google Scholar] [CrossRef]
- Lin, M.-H.; Lee, J.Y.-Y.; Pan, S.-C.; Wong, T.-W. Enhancing wound healing in recalcitrant leg ulcers with aminolevulinic acid-mediated antimicrobial photodynamic therapy. Photodiagn. Photodyn. Ther. 2021, 33, 102149. [Google Scholar] [CrossRef]
- Mosti, G.; Picerni, P.; Licau, M.; Mattaliano, V. Photodynamic therapy in infected venous and mixed leg ulcers: A pilot experience. J. Wound Care 2018, 27, 816–821. [Google Scholar] [CrossRef]
- Morley, S.; Griffiths, J.; Philips, G.; Moseley, H.; O’Grady, C.; Mellish, K.; Lankester, C.; Faris, B.; Young, R.; Brown, S.; et al. Phase IIa randomized, placebo-controlled study of antimicrobial photodynamic therapy in bacterially colonized, chronic leg ulcers and diabetic foot ulcers: A new approach to antimicrobial therapy. Br. J. Dermatol. 2012, 168, 617–624. [Google Scholar] [CrossRef]
- Aspiroz, C.; Sevil, M.; Toyas, C.; Gilaberte, Y. Photodynamic Therapy With Methylene Blue for Skin Ulcers Infected With Pseudomonas aeruginosa and Fusarium spp. Actas Dermosifiliogr. 2017, 108, e45–e48. [Google Scholar] [CrossRef]
- Cappugi, P.; Comacchi, C.; Torchia, D. Photodynamic therapy for chronic venous ulcers. Acta Dermatovenerol. Croat. ADC 2014, 22, 129–131. [Google Scholar]
- Monami, M.; Scatena, A.; Schlecht, M.; Lobmann, R.; Landi, L.; Ricci, L.; Mannucci, E. Antimicrobial Photodynamic Therapy in Infected Diabetic Foot Ulcers: A Multicenter Preliminary Experience. J. Am. Podiatr. Med Assoc. 2020, 110, 5. [Google Scholar] [CrossRef] [PubMed]
- Corsi, A.; Lecci, P.P.; Bacci, S.; Cappugi, P.; Pimpinelli, N. Early activation of fibroblasts during PDT treatment in leg ulcers. G. Ital. Dermatol. Venereol. 2016, 151, 223–229. [Google Scholar]
- Bochenek, K.; Aebisher, D.; Międzybrodzka, A.; Cieślar, G.; Kawczyk-Krupka, A. Methods for bladder cancer diagnosis—The role of autofluorescence and photodynamic diagnosis. Photodiagn. Photodyn. Ther. 2019, 27, 141–148. [Google Scholar] [CrossRef]
- Bochynek, K.; Aebisher, D.; Gasiorek, M.; Cieślar, G.; Kawczyk-Krupka, A. Evaluation of autofluorescence and photodynamic diagnosis in assessment of bladder lesions. Photodiagn. Photodyn. Ther. 2020, 30, 101719. [Google Scholar] [CrossRef]
- Latos, W.; Sieroń, A.; Cieślar, G.; Kawczyk-Krupka, A. The benefits of targeted endoscopic biopsy performed using the autofluorescence based diagnostic technique in 67 cases of diagnostically difficult gastrointestinal tumors. Photodiagn. Photodyn. Ther. 2018, 23, 63–67. [Google Scholar] [CrossRef]
- Latos, W.; Kawczyk-Krupka, A.; Strzelczyk, N.; Sieroń, A.; Cieślar, G. Benign and non-neoplastic tumours of the duodenum. Gastroenterol. Rev. 2019, 14, 233–241. [Google Scholar] [CrossRef]
- Krupka, M.; Bartusik-Aebisher, D.; Strzelczyk, N.; Latos, M.; Sieroń, A.; Cieślar, G.; Aebisher, D.; Czarnecka, M.; Kawczyk-Krupka, A.; Latos, W. The role of autofluorescence and photodynamic diagnosis in malignant tumors of the duodenum. Photodiagn. Photodyn. Ther. 2020, 32, 101981. [Google Scholar] [CrossRef]
- Kawczyk-Krupka, A.; Bartusik-Aebisher, D.; Latos, W.; Cieślar, G.; Sieroń, K.; Kwiatek, S.; Oleś, P.; Kwiatek, B.; Aebisher, D.; Krupka, M.; et al. Clinical Trials and Basic Research in Photodynamic Diagnostics and Therapies from the Center for Laser Diagnostics and Therapy in Poland. Photochem. Photobiol. 2020, 96, 539–549. [Google Scholar] [CrossRef] [Green Version]
- Kawczyk-Krupka, A.; Pucelik, B.; Międzybrodzka, A.; Sieroń, A.R.; Dąbrowski, J.M. Photodynamic therapy as an alternative to antibiotic therapy for the treatment of infected leg ulcers. Photodiagn. Photodyn. Ther. 2018, 23, 132–143. [Google Scholar] [CrossRef]
- Wulf, H.C.; Karlsmark, T. Photodynamic therapy of infected ulcers. Br. J. Dermatol. 2013, 168, 466. [Google Scholar] [CrossRef] [PubMed]
- Lv, X.; Zhang, J.; Yang, D.; Shao, J.; Wang, W.; Zhang, Q.; Dong, X. Recent advances in pH-responsive nanomaterials for anti-infective therapy. J. Mater. Chem. B 2020, 8, 10700–10711. [Google Scholar] [CrossRef] [PubMed]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ulcers Types | Venous | Ischemic | Neuropathic |
|---|---|---|---|
| Gender | More often women | More often men | Women/men |
| Interview | History of thrombophlebitis | overweight, high blood pressure, smoking, diabetes | diabetes |
| Localisation | medial, lateral or on the back of the calf, above the ankles | toes, pressure points, medial edge of the heel, edge of the foot, dorsal side of the toes | sole, bone prominences, often under the callus |
| Appearance | thick cylindrical wound edge, pink base, exudate | irregular edges, white/blue, visible tendons or bones, weak granulation tissue | irregular, indented edges, red granulation, deep, infected, often visible deeper structures |
| Exudation | intense yellow-pink discharge, pus | little or no exudate | medium oozing |
| Foot warmth | warm | cool, dry | warm, humid |
| Pain | Medium when standing | medium, when standing, disappears when the limb is lifted | absent |
| Puls | present | absent | Present or absent |
| Veins | varicose veins, telangiectasias | collapsed veins | Dilated veins |
| Feel | present | variables | absent |
| Ulcerationin the calluses | absent | rare | present |
| Group | No. | Age | Wound Area before [cm2] | Wound Area after [cm2] | Complete Response (CR) | Partial Response (PR) | No Response (NR) | Reducing Bacterial Load * | Etiology ** | Numeric Pain Rating Scale (NPRS) | Side Effect: Edema | Side Effects: Swelling Erythema Inflamation | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PDT | 1 | 72 | 49 | 9 | 0 | 1 | 0 | 4 | 3 | CVI + PAD | 7 | 1 | 0 |
| PDT | 2 | 84 | 25 | 0 | 1 | 0 | 0 | 4 | 2 | CVI + PAD | 6 | 0 | 0 |
| PDT | 3 | 78 | 9 | 0 | 1 | 0 | 0 | 3 | 1 | CVI | 4 | 0 | 0 |
| PDT | 4 | 82 | 20 | 20 | 0 | 0 | 1 | 3 | 3 | CVI + PAD | 10 | 1 | 1 |
| PDT | 5 | 67 | 4 | 0 | 1 | 0 | 0 | 2 | 0 | NF | 2 | 0 | 0 |
| PDT | 6 | 70 | 9 | 2 | 0 | 1 | 0 | 3 | 2 | CVI | 3 | 0 | 0 |
| PDT | 7 | 58 | 2.25 | 0 | 1 | 0 | 0 | 2 | 0 | NF | 1 | 0 | 0 |
| PDT | 8 | 60 | 18 | 6 | 0 | 1 | 0 | 3 | 2 | CVI | 5 | 0 | 0 |
| PDT | 9 | 54 | 20 | 8 | 0 | 1 | 0 | 4 | 3 | CVI + PAD | 6 | 0 | 0 |
| PDT | 10 | 76 | 16 | 16 | 0 | 0 | 1 | 3 | 3 | CVI | 10 | 1 | 1 |
| Sum | 4 | 4 | 2 | 5.5 | 3 | 2 | |||||||
| Average | 70.1 | 17.225 | 6.1 | ||||||||||
| Control | 1 | 68 | 9 | 2 | 0 | 1 | 0 | 3 | 3 | CVI + PAD | 4 | 0 | 0 |
| Control | 2 | 81 | 16 | 18 | 0 | 0 | 1 | 4 | 2 | CVI + PAD | 5 | 1 | 0 |
| Control | 3 | 70 | 3 | 0 | 1 | 0 | 0 | 2 | 1 | NF | 5 | 0 | 0 |
| Control | 4 | 56 | 21 | 3 | 0 | 1 | 0 | 4 | 2 | CVI + PAD | 1 | 0 | 0 |
| Control | 5 | 77 | 24 | 24 | 0 | 0 | 1 | 4 | 4 | CVI + PAD | 2 | 0 | 0 |
| Control | 6 | 71 | 18 | 0 | 1 | 0 | 0 | 4 | 4 | CVI | 4 | 1 | 1 |
| Control | 7 | 82 | 12 | 15 | 0 | 0 | 1 | 3 | 2 | CVI | 3 | 0 | 0 |
| Control | 8 | 83 | 15 | 12 | 0 | 0 | 1 | 3 | 2 | CVI | 3 | 0 | 0 |
| Control | 9 | 74 | 18 | 12 | 0 | 0 | 1 | 2 | 2 | CVI + PAD | 6 | 0 | 0 |
| Control | 10 | 66 | 45 | 15 | 0 | 1 | 0 | 4 | 4 | CVI | 7 | 0 | 0 |
| Sum | 2 | 3 | 5 | 3.2 | 2 | 1 | |||||||
| Average | 72.8 | 18.1 | 10.1 | ||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krupka, M.; Bożek, A.; Bartusik-Aebisher, D.; Cieślar, G.; Kawczyk-Krupka, A. Photodynamic Therapy for the Treatment of Infected Leg Ulcers—A Pilot Study. Antibiotics 2021, 10, 506. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10050506
Krupka M, Bożek A, Bartusik-Aebisher D, Cieślar G, Kawczyk-Krupka A. Photodynamic Therapy for the Treatment of Infected Leg Ulcers—A Pilot Study. Antibiotics. 2021; 10(5):506. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10050506
Chicago/Turabian StyleKrupka, Magdalena, Andrzej Bożek, Dorota Bartusik-Aebisher, Grzegorz Cieślar, and Aleksandra Kawczyk-Krupka. 2021. "Photodynamic Therapy for the Treatment of Infected Leg Ulcers—A Pilot Study" Antibiotics 10, no. 5: 506. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10050506