
Impact of the COVID-19 Pandemic on the Prescribing Patterns of First-Line Antibiotics in English Primary Care: A Longitudinal Analysis of National Prescribing Dataset


Abstract
:1. Introduction
2. Results
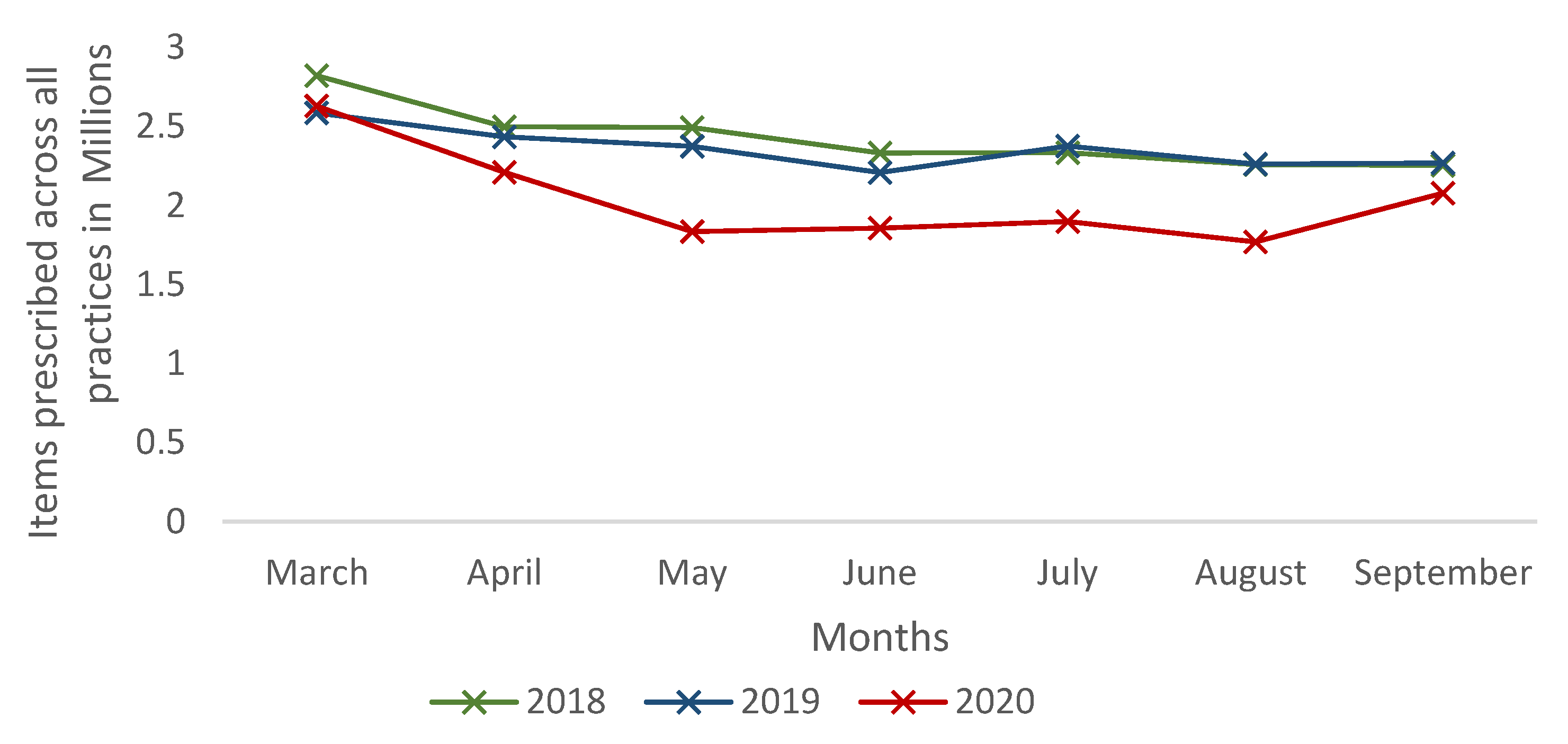
2.1. Prescribing of First-Line Antibiotics between 2018 and 2020
2.2. Prescribing Patterns of First-Line Antibiotics by Pharmacological Drug Classification and Anatomical Infection Sites
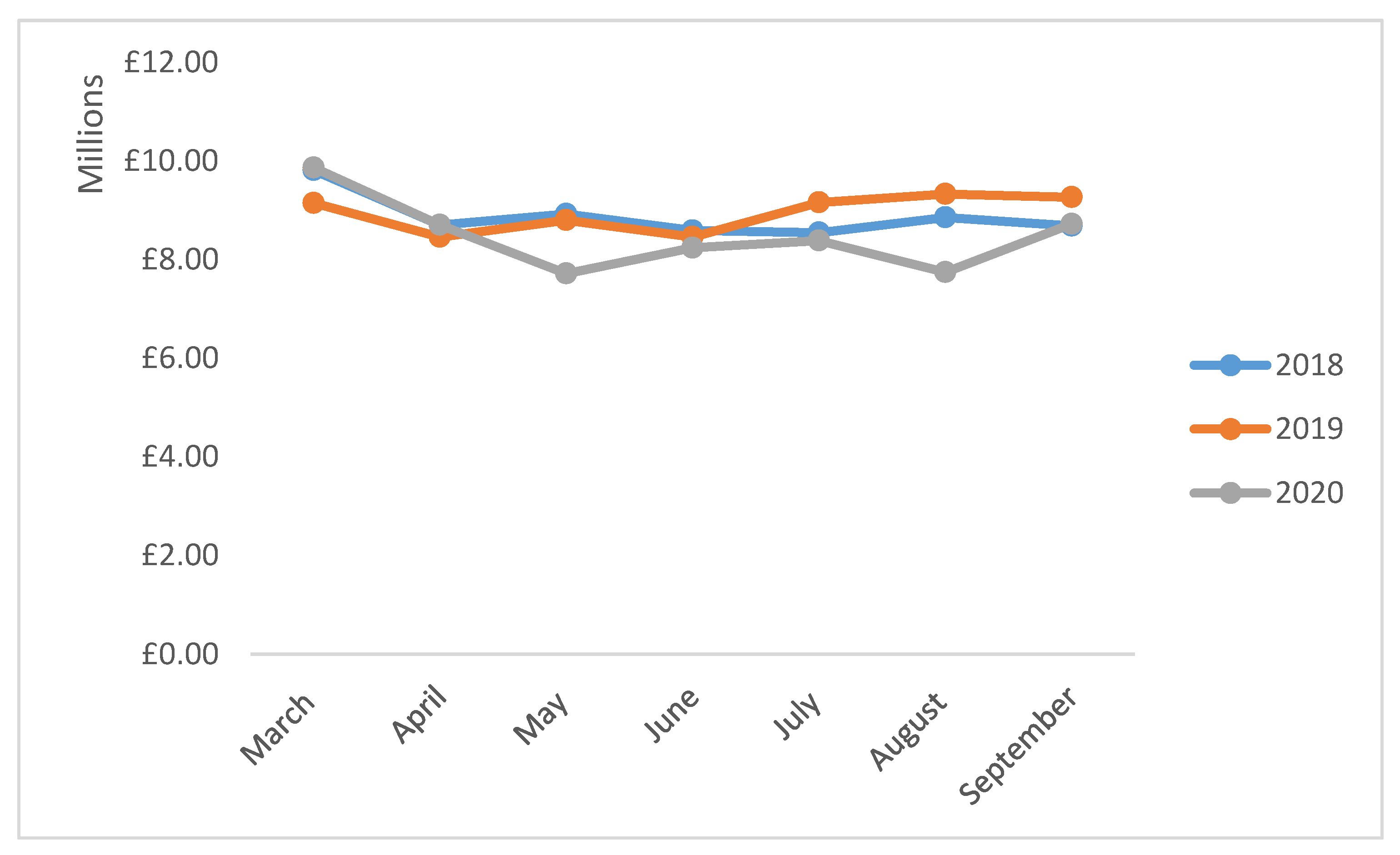
2.3. Costs Associated with Prescribing of First-Line Antibiotics between 2018 and 2020
3. Discussion
Strengths and Limitations
4. Materials and Methods
4.1. Study Design and Population
4.2. Data Extraction and Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. World Health Organization COVID-19 Dashboard. Available online: https://covid19.who.int/ (accessed on 28 April 2021).
- The UK Government. Coronavirus (COVID-19) in the UK. Available online: https://coronavirus.data.gov.uk/ (accessed on 28 April 2021).
- The Independent. Coronavirus: Timeline of Key Events Since UK Was Put into Lockdown Six Months Ago. Available online: https://www.independent.co.uk/news/uk/home-news/coronavirus-uk-timeline-lockdown-boris-johnson-pubs-test-and-trace-vaccine-b547630.html (accessed on 28 April 2021).
- The Health Foundation. How Are Total Triage and Remote Consolation Changing The Use Of Emergence Care? Available online: https://www.health.org.uk/news-and-comment/charts-and-infographics/how-are-total-triage-and-remote-consultation-changing-the-us (accessed on 28 April 2021).
- The Health Foundation. How Might COVID-19 Have Affected People’s Ability to See Their GP? Available online: https://www.health.org.uk/news-and-comment/charts-and-infographics/how-might-covid-19-have-affected-peoples-ability-to-see-GP (accessed on 28 April 2021).
- NHS Digital Appointments in General Practice Report. Available online: https://digital.nhs.uk/data-and-information/data-tools-and-services/data-services/general-practice-data-hub/appointments-in-general-practice (accessed on 28 April 2021).
- Paudyal, V.; Cadogan, C.; Fialová, D.; Henman, M.C.; Hazen, A.; Okuyan, B.; Lutters, M.; Stewart, D. Provision of clinical pharmacy services during the COVID-19 pandemic: Experiences of pharmacists from 16 European countries. Res. Soc. Adm. Pharm. 2020. [Google Scholar] [CrossRef] [PubMed]
- Nuffield Trust. Antibiotics Prescribing. Available online: https://www.nuffieldtrust.org.uk/resource/antibiotic-prescribing#background (accessed on 18 March 2021).
- Rimmer, A. I don’t feel confident providing remote consultations. What do I need to know? BMJ 2020, 369, m1746. [Google Scholar] [CrossRef] [PubMed]
- Van de Pol, A.C.; Boeijen, J.A.; Venekamp, R.P.; Platteel, T.; Damoiseaux, R.A.M.J.; Kortekaas, M.F.; van der Velden, A.W. Impact of the COVID-19 Pandemic on Antibiotic Prescribing for Common Infections in The Netherlands: A Primary Care-Based Observational Cohort Study. Antibiotics 2021, 10, 196. [Google Scholar] [CrossRef] [PubMed]
- McBride, J.A.; Eickhoff, J.; Wald, E.R. Impact of COVID-19 Quarantine and School Cancelation on Other Common Infectious Diseases. Pediatr. Infect. Dis. J. 2020, 39, e449–e452. [Google Scholar] [CrossRef] [PubMed]
- King, L.M.; Lovegrove, M.C.; Shehab, N.; Tsay, S.; Budnitz, D.S.; Geller, A.I.; Lind, J.N.; Roberts, R.M.; Hicks, L.A.; Kabbani, S. Trends in US Outpatient Antibiotic Prescriptions During the Coronavirus Disease 2019 Pandemic. Clin. Infect. Dis. 2020, ciaa1896. [Google Scholar] [CrossRef] [PubMed]
- Gautret, P.; Lagier, J.C.; Parola, P.; Hoang, V.T.; Meddeb, L.; Mailhe, M.; Doudier, B.; Courjon, J.; Giordanengo, V.; Vieira, V.E.; et al. Hydroxychloroquine and azithromycin as a treatment of COVID-19: Results of an open-label non-randomized clinical trial. Int. J. Antimicrob. Agents 2020, 105949. [Google Scholar] [CrossRef] [PubMed]
- Mulvihill, C.; Cooper, J.; Pavey, J.; Laake, J.-P. Remote consultations in primary care during the COVID-19 pandemic: Student prospective. Postgrad Med. J. 2020. [Google Scholar] [CrossRef] [PubMed]
- Watt, T.; Firth, Z.; Fisher, R.; Thorlby, R. Elaine Kelly Use of Primary Care during the COVID_19 Pandemic. Available online: https://www.health.org.uk/news-and-comment/charts-and-infographics/use-of-primary-care-during-the-covid-19-pandemic (accessed on 8 January 2021).
- Bostock, N. Millions of Patients ‘Avoiding Calls to GP’ during COVID-19 Pandemic. Available online: https://www.gponline.com/millions-patients-avoiding-calls-gp-during-covid-19-pandemic/article/1681384 (accessed on 10 January 2021).
- Lin, C.-F.; Huang, Y.-H.; Cheng, C.-Y.; Wu, K.-H.; Tang, K.-S.; Chiu, I.-M. Public Health Interventions for the COVID-19 Pandemic Reduce Respiratory Tract Infection-Related Visits at Pediatric Emergency Departments in Taiwan. Front. Public Health 2020, 8, 604089. [Google Scholar] [CrossRef] [PubMed]
- Armitage, R.; Nellums, L.B. Antibiotic prescribing in general practice during COVID-19. Lancet 2020. [Google Scholar] [CrossRef]
- Public Health England. English Surveillance Programme for Antimicrobial Utilization and Resistance (ESPAUR) 2019–2020. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/936199/ESPAUR_Report_2019-20.pdf (accessed on 14 May 2021).
- Dolk, F.C.K.; Pouwels, K.B.; Smith, D.R.M.; Robotham, J.V.; Smieszek, T. Antibiotics in primary care in England: Which antibiotics are prescribed and for which conditions? J. Ant Chem. 2018, 73, ii2–ii10. [Google Scholar] [CrossRef] [PubMed]
- Spivak, E.S.; Cosgrove, S.E.; Srinivasan, A. Measuring appropriate antimicrobial use: Attempts at opening the black box. Clin. Infect. Dis. 2016, 63, 1639–1644. [Google Scholar] [PubMed] [Green Version]
- Costelloe, C.; Metcalf, C.; Lovering, A.; Mant, D.; Hay, A.D. Effects of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: Systematic review and meta-analysis. BMJ 2010, 340, c2096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lipsitch, M.; Samore, M.H. Antimicrobial use and antimicrobial resistance: A population perspective. Emerg. Infect. Dis. 2002, 8, 347–354. [Google Scholar] [CrossRef]
- Auta, A.; Hadi, M.A.; Oga, E.; Adewuyi, E.O.; Abdu-Aguye, S.N.; Adeloye, D.; Strickland-Hodge, B.; Morgan, D.J. Global access to antibiotics without prescription in community pharmacies: A systematic review and meta-analysis. J. Infect. 2019, 78, 8–18. [Google Scholar] [CrossRef] [PubMed]
- Hadi, M.A.; Karami, N.A.; Al-Muwalid, A.S.; Al-Otabi, A.; Al-Subahi, E.; Bamomen, A.; Mohamed, M.M.; Elrggal, M.E. Community pharmacists’ knowledge, attitude, and practices towards dispensing antibiotics without prescription (DAwP): A cross-sectional survey in Makkah Province, Saudi Arabia. Int. J. Infect. Dis. 2016, 47, 95–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Institute for Health and Care Excellence (NICE). Summary of Antimicrobial Prescribing Guidance-Managing Common Infections. Available online: https://www.nice.org.uk/Media/Default/About/what-we-do/NICE-guidance/antimicrobial%20guidance/summary-antimicrobial-prescribing-guidance.pdf (accessed on 11 January 2021).
- Evidence-Based Medicine (EBM). DataLab. OpenPrescribing London: EBM Datalab. 2020. Available online: https://openprescribing.net/ (accessed on 20 December 2020).
- Vohra, N.; Hadi, M.A.; Khanal, S.; Kurmi, O.P.; Paudyal, V. Impact of deprivation, dementia prevalence and regional demography on prescribing of antidementia drugs in England: A time trend analysis. Br. J. Clin. Pharmacol. 2021, 1–9. [Google Scholar] [CrossRef]
- Bell, C.; Hadi, M.A.; Khanal, S.; Paudyal, V. Prescribing patterns and costs associated with erectile dysfunction drugs in England: A time trend analysis. BJGP Open 2021. [Google Scholar] [CrossRef] [PubMed]
- UK. Inflation Calculator. 2020. Available online: https://www.in2013dollars.com/UK-inflation (accessed on 20 December 2020).



{kind=link}
{kind=link}
| Antibiotic | Items Prescribed (March–September) | % Difference 2020 and 2018 (p-Value) * | % Difference 2020 and 2019 (p-Value) * | ||
|---|---|---|---|---|---|
| 2018 | 2019 | 2020 | |||
| Amoxicillin | 3,788,146 | 3,656,355 | 2,548,155 | −32.7 (0.035) | −43.5 (0.035) |
| Phenoxymethylpenicillin | 1,345,567 | 1,224,614 | 938,718 | −30.2 (0.048) | −23.35 (0.025) |
| Doxycycline | 1,418,699 | 1,552,700 | 1,512,059 | 6.6 (0.949) | −2.6 (0.225) |
| Clarithromycin | 1,150,884 | 1,114,988 | 914,060 | −20.6 (0.048) | −18.0 (0.064) |
| Co-amoxiclav | 781,027 | 733,962 | 730,055 | −6.5 (0.085) | −1.0 (0.565) |
| Nitrofurantoin | 2,296,145 | 2,436,156 | 2,418,624 | 5.3 (0.048) | −0.7 (0.749) |
| Trimethoprim | 1,131,986 | 952,513 | 892,998 | −21.1 (0.002) | −6.3 (0.009) |
| Ciprofloxacin | 333,774 | 280,746 | 258,309 | −22.6 (0.002) | −7.9 (0.013) |
| Ofloxacin | 20,222 | 19,525 | 23,413 | 15.8 (0.004) | 19.9 (0.002) |
| Cefalexin | 428,462 | 422,528 | 445,779 | 4.0 (0.0085) | 5.5 (0.025) |
| Benzylpenicillin | 373 | 297 | 112 | −69.9 (0.002) | −62.3 (0.002) |
| Metronidazole (Oral) | 337,999 | 331,865 | 304,898 | −9.8 (0.002) | −8.1 (0.002) |
| Vancomycin | 2710 | 2417 | 3152 | 16.3 (0.018) | 30.4 (0.013) |
| Metronidazole (Topical) | 17,028 | 19,821 | 21,406 | 25.7 (0.002) | 8.0 (0.064) |
| Clindamycin (Topical) | 18,676 | 17,213 | 15,139 | −18.9 (0.002) | −12.1 (0.002) |
| Fusidic acid | 637,990 | 627,026 | 473,193 | −25.8 (0.002) | −24.5 (0.002) |
| Mupirocin | 38,692 | 38,398 | 31,038 | −19.8 (0.003) | −19.8 (0.002) |
| Flucloxacillin | 2,502,571 | 2,388,848 | 2,256,687 | −9.8 (0.110) | −5.5 (0.655) |
| Ceftriaxone | 828 | 616 | 570 | −31.2 (0.005) | −7.5 (0.749) |
| Chloramphenicol | 735,945 | 683,392 | 482,716 | −34.4 (0.004) | −29.4 (0.002) |
| All antibiotics | 16,987,724 | 16,503,980 | 14,271,081 | −15.99 (0.018) | −13.5 (0.002) |
| Number of Items Prescribed between March and September in Millions * | % Difference 2020–2018 (p-Value) * | % Difference 2020–2019 (p-Value) * | |||
|---|---|---|---|---|---|
| 2018 | 2019 | 2020 | |||
| Upper respiratory tract | 5.13 | 4.88 | 2.97 | −42.13 (0.025) | −39.13 (0.035) |
| Lower respiratory tract | 7.13 | 7.05 | 4.90 | −31.40 (0.064) | −30.62 (0.085) |
| Urinary tract infection | 4.99 | 4.84 | 4.07 | −18.52 (0.002) | −16.06 (0.002) |
| Meningitis | 0.0004 | 0.0003 | 0.00009 | −69.9 (0.002) | −62.3 (0.002) |
| Gastro-intestinal tract | 6.07 | 5.84 | 3.85 | −36.42 (0.035) | −34.01 (0.048) |
| Genital tract | 2.14 | 2.22 | 1.84 | −14.33 (0.482) | −17.23 (0.18) |
| Skin and soft tissue | 10.67 | 10.44 | 7.50 | −29.59 (0.025) | −28.17 (0.035) |
| Eye infection | 0.74 | 0.69 | 0.42 | −42.63 (0.004) | −38.22 (0.002) |
| Dental infection | 5.47 | 5.21 | 3.23 | −40.95 (0.025) | −38.02 (0.035) |
| Number of Items Prescribed in Millions | % Difference 2018–2020 (p-Value)* | % Difference 2019–2020 (p-Value) * | |||
|---|---|---|---|---|---|
| 2018 | 2019 | 2020 | |||
| Penicillin | 8.41 | 8.00 | 6.47 | −23.09 (0.018) | −19.12 (0.025) |
| Cephalosporins | 0.43 | 0.42 | 0.45 | 3.98 (0.085) | 5.49 (0.025) |
| Macrolides | 1.15 | 1.11 | 0.91 | −20.58 (0.048) | −18.02 (0.064) |
| Quinolones | 0.35 | 0.30 | 0.28 | −20.42 (0.002) | −6.18 (0.0035) |
| Tetracyclines | 1.42 | 1.55 | 1.51 | 6.58 (0.949) | −2.62 (0.225) |
| Others | 5.41 | 5.30 | 4.80 | −11.19 (0.002) | −9.43 (0.002) |
| Antibiotic | Costs in Millions | % Difference 2020–2018 (p-Value) * | % Difference2020–2019 (p-Value) * | ||
|---|---|---|---|---|---|
| 2018 | 2019 | 2020 | |||
| Amoxicillin | 4.12 | 4.49 | 4.26 | 3.18 (0.482) | −5.22 (0.277) |
| Phenoxymethylpenicillin | 7.46 | 5.43 | 3.86 | −48.21 (0.006) | −28.90 (0.018) |
| Co-amoxiclav | 1.82 | 1.87 | 2.04 | 11.90 (0.013) | 9.03 (0.064) |
| Benzylpenicillin | 0.004 | 0.002 | 0.002 | −57.59 (0.025) | −17.33 (0.085) |
| Flucloxacillin | 11.24 | 11.29 | 8.13 | −27.70 (0.002) | −28.05 (0.002) |
| Cefalexin | 0.73 | 0.78 | 1.06 | 45.78 (0.002) | 36.27 (0.002) |
| Ceftriaxone | 0.08 | 0.06 | 0.05 | −36.85 (0.006) | −15.70 (0.085) |
| Ciprofloxacin | 0.90 | 0.84 | 0.86 | −4.90 (0.482) | 2.50 (0.620) |
| Ofloxacin | 0.78 | 0.72 | 0.87 | 12.58 (0.004) | 20.61 (0.003) |
| Doxycycline | 1.75 | 2.38 | 4.16 | 137.37 (0.002) | 74.61 (0.002) |
| Clarithromycin | 2.81 | 2.81 | 3.00 | 6.54 (0.482) | 6.74 (0.277) |
| Clindamycin | 1.12 | 0.82 | 0.87 | −22.06 (0.002) | 6.45 (0.003) |
| Nitrofurantoin | 20.91 | 20.96 | 20.81 | −0.489 (0.949) | −0.75 (0.902) |
| Trimethoprim | 1.59 | 1.78 | 1.82 | 14.62 (0.064) | 2.70 (1.000) |
| Metronidazole oral | 1.68 | 2.08 | 4.25 | −5.74 (0.655) | −23.87 (0.001) |
| Metronidazole ointment | 2.11 | 2.19 | 3.86 | −16.86 (0.655) | −19.98 (0.001) |
| Vancomycin | 0.57 | 0.50 | 2.04 | −13.64 (0.225) | −1.48 (0.710) |
| Fusidic acid | 1.33 | 1.62 | 0.002 | 33.24 (0.002) | 8.93 (0.142) |
| Mupirocin | 0.24 | 0.23 | 8.12 | −18.78 (0.003) | −18.20 (0.002) |
| Chloramphenicol | 1.24 | 1.79 | 1.07 | 52.88 (0.003) | 6.19 (0.001) |
| All antibiotics | 62.08 | 62.58 | 59.34 | −4.42% (0.180) | −5.18 (0.097) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hussain, A.Z.; Paudyal, V.; Hadi, M.A. Impact of the COVID-19 Pandemic on the Prescribing Patterns of First-Line Antibiotics in English Primary Care: A Longitudinal Analysis of National Prescribing Dataset. Antibiotics 2021, 10, 591. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10050591
Hussain AZ, Paudyal V, Hadi MA. Impact of the COVID-19 Pandemic on the Prescribing Patterns of First-Line Antibiotics in English Primary Care: A Longitudinal Analysis of National Prescribing Dataset. Antibiotics. 2021; 10(5):591. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10050591
Chicago/Turabian StyleHussain, Alisha Zubair, Vibhu Paudyal, and Muhammad Abdul Hadi. 2021. "Impact of the COVID-19 Pandemic on the Prescribing Patterns of First-Line Antibiotics in English Primary Care: A Longitudinal Analysis of National Prescribing Dataset" Antibiotics 10, no. 5: 591. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10050591