
Antimicrobial Synergy Testing: Comparing the Tobramycin and Ceftazidime Gradient Diffusion Methodology Used in Assessing Synergy in Cystic Fibrosis-Derived Multidrug-Resistant Pseudomonas aeruginosa

Abstract
:1. Introduction
2. Results
2.1. Study Results
2.1.1. Strain Characteristics
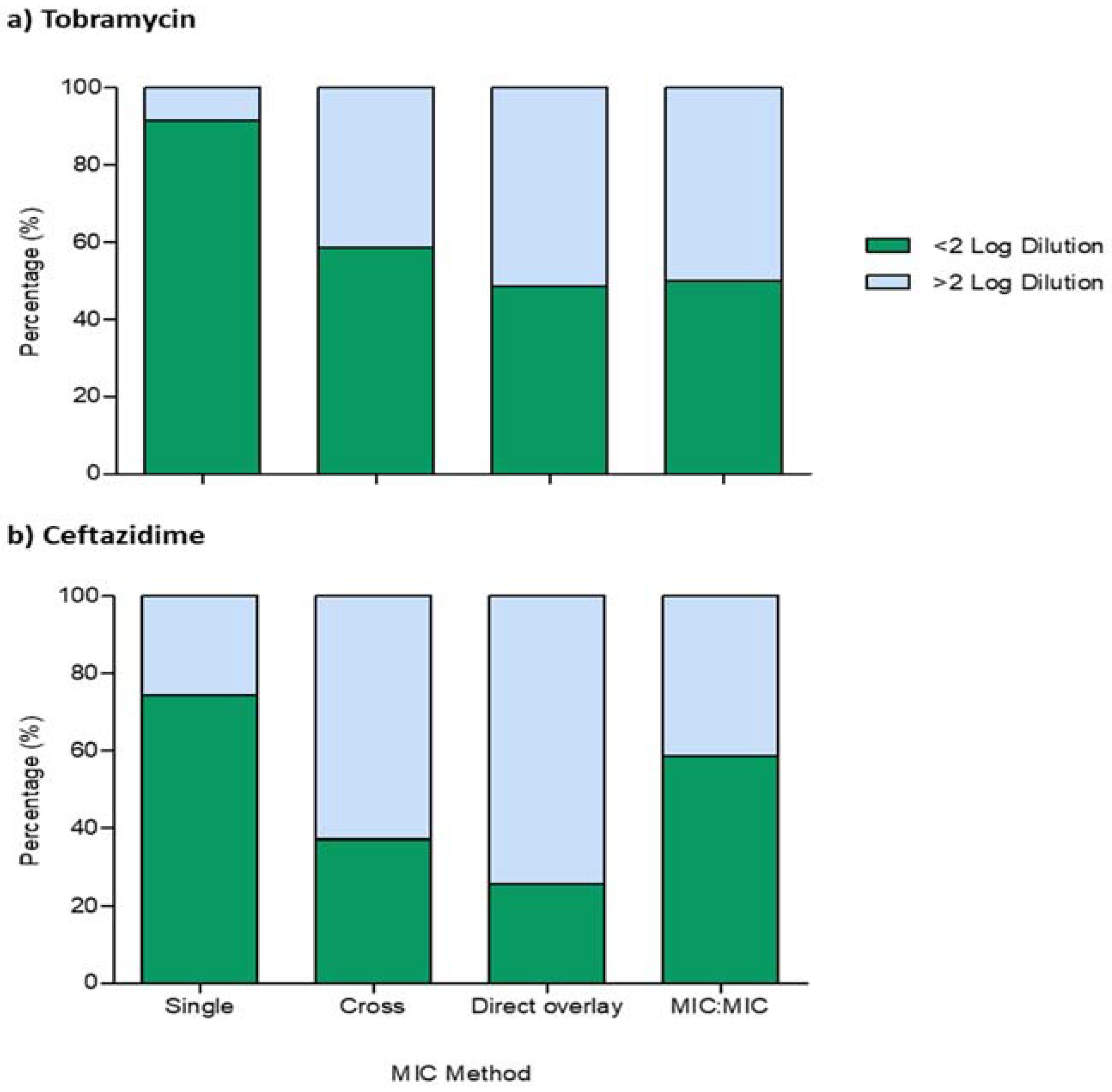
2.1.2. Essential and Categorical Agreement of Single- and Combination-MIC Testing
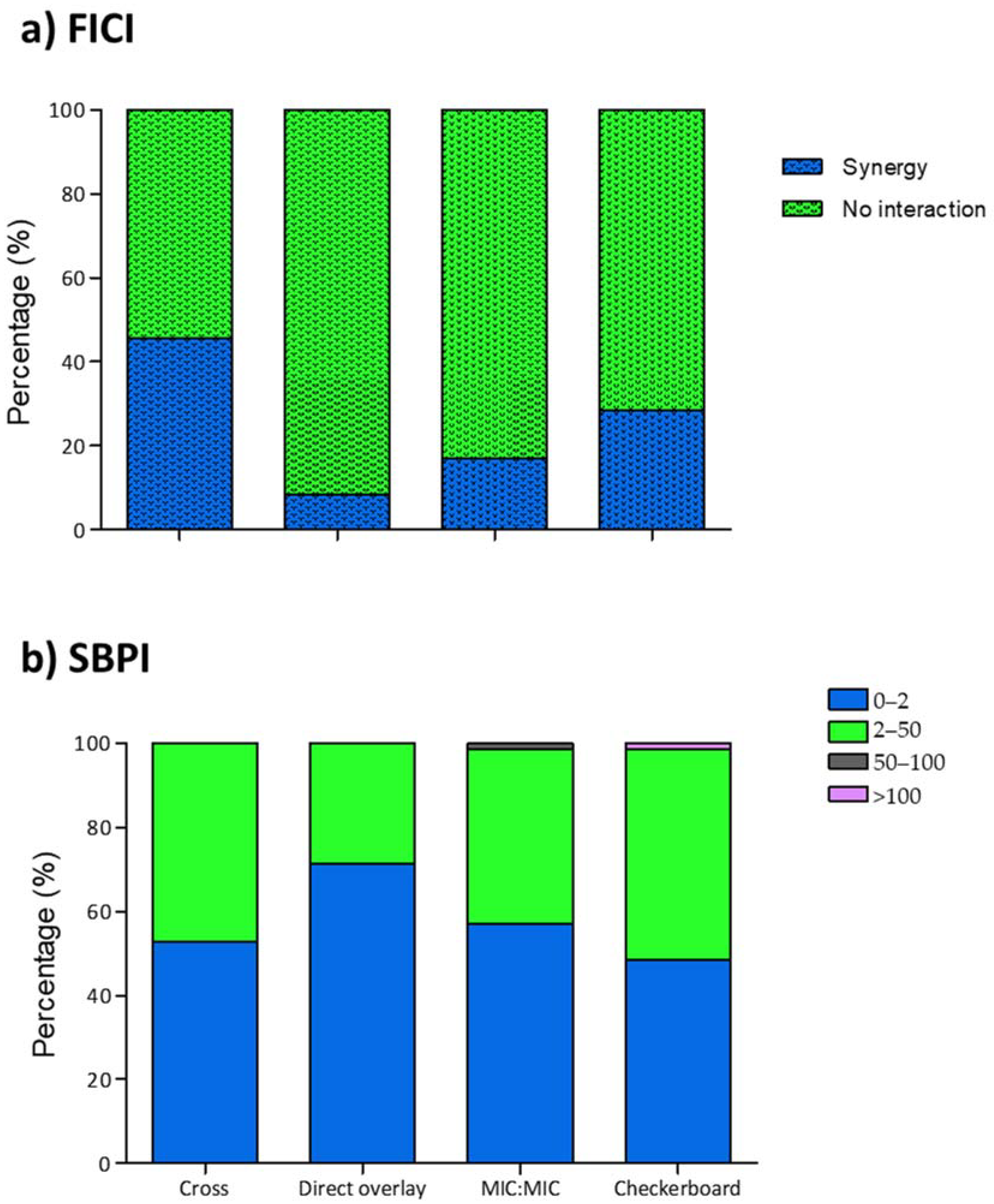
2.1.3. FICI and SBPI of P. aeruginosa Isolate Synergy Testing
2.1.4. FICI and SBPI Comparator Agreement
2.1.5. Effect of Resistance Profiles on FICI and SBPI Values
3. Discussion
4. Materials and Methods
4.1. Study Isolates and Media
4.2. Antimicrobial Agents
4.3. Gradient Diffusion MIC Testing
4.4. Gradient Diffusion Synergy Methods
4.4.1. Cross Method
4.4.2. Direct Overlay Method
4.4.3. MIC:MIC Overlay Method
4.5. Broth Microdilution Checkerboard Method
4.6. Interpretative Criteria
4.6.1. Fractional Inhibitory Concentration Index (FICI)
4.6.2. Susceptible Breakpoint Index (SBPI)
4.7. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| TM | Tobramycin |
| TZ | Ceftazidime |
| FICI | Fractional Inhibitory Concentration Index |
| SBPI | Susceptibilty Breakpoint Index |
| NI | No Interaction |
| SYN | Synergy |
| MIC | Minimum Inhibitory Concentration |
| R | Biological replicate |
| cAv. | Average |
References
- Alvarez-Buylla, A.; Allen, M.; Betts, D.; Bennett, S.; Monahan, I.; Planche, T.; Auckland, C.; Bowker, K.; Chesterfield, H.; Dall’Antonia, M.; et al. Multicentre study of the in vitro activity of ceftolozane/tazobactam and other commonly used antibiotics against Pseudomonas aeruginosa isolates from patients in the UK. JAC Antimicrob. Resist. 2020, 2, dlaa024. [Google Scholar] [CrossRef] [PubMed]
- López-Causapé, C.; Rojo-Molinero, E.; Macia, M.D.; Oliver, A. The problems of antibiotic resistance in cystic fibrosis and solutions. Expert Rev. Respir. Med. 2014, 9, 73–88. [Google Scholar] [CrossRef] [PubMed]
- Forrester, J.B.; Steed, L.L.; Santevecchi, B.A.; Flume, P.; Palmer-Long, G.E.; Bosso, J.A. In vitro Activity of Ceftolozane/Tazobactam vs Nonfermenting, Gram-Negative Cystic Fibrosis Isolates. Open Forum Infect. Dis. 2018, 5, 158. [Google Scholar] [CrossRef]
- Brennan-Krohn, T.; Kirby, J.E. When One Drug Is Not Enough. Clin. Lab. Med. 2019, 39, 345–358. [Google Scholar] [CrossRef] [PubMed]
- Stefani, S.; Campana, S.; Cariani, L.; Carnovale, V.; Colombo, C.; Lleo, M.; Iula, V.; Minicucci, L.; Morelli, P.; Pizzamiglio, G.; et al. Relevance of multidrug-resistant Pseudomonas aeruginosa infections in cystic fibrosis. Int. J. Med. Microbiol. 2017, 307, 353–362. [Google Scholar] [CrossRef]
- Aaron, S.D.; Vandemheen, K.L.; Ferris, W.; Fergusson, D.; Tullis, E.; Haase, D.; Berthiaume, Y.; Brown, N.; Wilcox, P.; Yozghatlian, V.; et al. Combination antibiotic susceptibility testing to treat exacerbations of cystic fibrosis associated with multiresistant bacteria: A randomised, double-blind, controlled clinical trial. Lancet 2005, 366, 463–471. [Google Scholar] [CrossRef]
- Pang, Z.; Raudonis, R.; Glick, B.R.; Lin, T.-J.; Cheng, Z. Antibiotic resistance in Pseudomonas aeruginosa: Mechanisms and alternative therapeutic strategies. Biotechnol. Adv. 2019, 37, 177–192. [Google Scholar] [CrossRef]
- Flume, P.A.; Waters, V.J.; Bell, S.C.; Van Devanter, D.R.; Elborn, J.S. Antimicrobial resistance in cystic fibrosis: Does it matter? J. Cyst. Fibros. 2018, 17, 687–689. [Google Scholar] [CrossRef]
- March, G.A.; Bratos, M.A. A meta-analysis of in vitro antibiotic synergy against Acinetobacter baumannii. J. Microbiol. Methods 2015, 119, 31–36. [Google Scholar] [CrossRef]
- Khan, Z.A.; Siddiqui, M.F.; Park, S. Current and Emerging Methods of Antibiotic Susceptibility Testing. Diagnostics 2019, 9, 49. [Google Scholar] [CrossRef] [Green Version]
- Doern, C.D. When Does 2 Plus 2 Equal 5? A Review of Antimicrobial Synergy Testing. J. Clin. Microbiol. 2014, 52, 4124–4128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pankey, G.A.; Ashcraft, D.S.; Dornelles, A. Comparison of 3 Etest® methods and time-kill assay for determination of antimicrobial synergy against carbapenemase-producing Klebsiella species. Diagn. Microbiol. Infect. Dis. 2013, 77, 220–226. [Google Scholar] [CrossRef]
- Gómara, M.; Ramón-García, S. The FICI paradigm: Correcting flaws in antimicrobial in vitro synergy screens at their inception. Biochem. Pharmacol. 2019, 163, 299–307. [Google Scholar] [CrossRef]
- Kidd, T.J.; Canton, R.; Ekkelenkamp, M.; Johansen, H.K.; Gilligan, P.; LiPuma, J.J.; Bell, S.C.; Elborn, J.S.; Flume, P.A.; VanDevanter, D.R.; et al. Defining antimicrobial resistance in cystic fibrosis. J. Cyst. Fibros. 2018, 17, 696–704. [Google Scholar] [CrossRef] [PubMed]
- Milne, K.E.N.; Gould, I.M. Combination testing of multidrug-resistant cystic fibrosis isolates of Pseudomonas aeruginosa: Use of a new parameter, the susceptible breakpoint index. J. Antimicrob. Chemother. 2009, 65, 82–90. [Google Scholar] [CrossRef] [Green Version]
- Lasko, M.J.; Huse, H.K.; Nicolau, D.P.; Kuti, J.L. Contemporary analysis of ETEST for antibiotic susceptibility and minimum inhibitory concentration agreement against Pseudomonas aeruginosa from patients with cystic fibrosis. Ann. Clin. Microbiol. Antimicrob. 2021, 20, 1–7. [Google Scholar] [CrossRef]
- Gaudereto, J.J.; Neto, L.V.P.; Leite, G.C.; Espinoza, E.P.S.; Martins, R.C.R.; Prado, G.V.B.; Rossi, F.; Guimarães, T.; Levin, A.; Costa, S.F. Comparison of methods for the detection of in vitro synergy in multidrug-resistant gram-negative bacteria. BMC Microbiol. 2020, 20, 97. [Google Scholar] [CrossRef] [Green Version]
- Balke, B.; Hogardt, M.; Schmoldt, S.; Hoy, L.; Weissbrodt, H.; Häussler, S. Evaluation of the E test for the assessment of synergy of antibiotic combinations against multiresistant Pseudomonas aeruginosa isolates from cystic fibrosis patients. Eur. J. Clin. Microbiol. Infect. Dis. 2006, 25, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Reygaert, W.C. An overview of the antimicrobial resistance mechanisms of bacteria. AIMS Microbiol. 2018, 4, 482–501. [Google Scholar] [CrossRef]
- Kapoor, G.; Saigal, S.; Elongavan, A. Action and resistance mechanisms of antibiotics: A guide for clinicians. J. Anaesthesiol. Clin. Pharmacol. 2017, 33, 300–305. [Google Scholar] [CrossRef]
- Odds, F.C. Synergy, antagonism, and what the chequerboard puts between them. J. Antimicrob. Chemother. 2003, 52, 1. [Google Scholar] [CrossRef] [PubMed]
- Basak, S.; Singh, P.; Rajurkar, M. Multidrug Resistant and Extensively Drug Resistant Bacteria: A Study. J. Pathog. 2016, 2016, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- EUCAST. The European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of MICs and Zone Diameters. Version 10.0. 2020. Available online: http://www.eucast.org (accessed on 23 March 2021).
- FDA. Antimicrobial Susceptibility Test (AST) Systems—Class II Special Controls Guidance for Industry and FDA. 2007. Available online: https://www.Fda.Gov/Medical-Devices/Guidance-Documents-Medical-Devices-and-Radiation-Emitting-Products/Antimicrobial-Susceptibility-Test-Ast-Systems-Class-Ii-Special-Controls-Guidance-Industry-and-Fda (accessed on 23 March 2021).
- Laishram, S.; Pragasam, A.K.; Bakthavatchalam, Y.D.; Veeraraghavan, B. An Update on Technical, Interpretative and Clinical Relevance of Antimicrobial Synergy Testing Methodologies. Indian J. Med. Microbiol. 2017, 35, 445–468. [Google Scholar] [CrossRef] [PubMed]
- Leber, A.L. Synergism Testing: Broth Microdilution Checkerboard and Broth Macrodilution Methods. In Clinical Microbiology Procedures Handbook, 4th ed.; ASM Press: Washington, DC, USA, 2016; Volume 1–3. [Google Scholar]
- Sopirala, M.M.; Mangino, J.E.; Gebreyes, W.A.; Biller, B.; Bannerman, T.; Balada-Llasat, J.-M.; Pancholi, P. Synergy Testing by Etest, Microdilution Checkerboard, and Time-Kill Methods for Pan-Drug-Resistant Acinetobacter baumannii. Antimicrob. Agents Chemother. 2010, 54, 4678–4683. [Google Scholar] [CrossRef] [Green Version]
- Fatsis-Kavalopoulos, N.; Roemhild, R.; Tang, P.-C.; Kreuger, J.; Andersson, D.I. CombiANT: Antibiotic interaction testing made easy. PLoS Biol. 2020, 18, e3000856. [Google Scholar] [CrossRef] [PubMed]
- MacKenzie, F.; Smith, S.; Milne, K.; Griffiths, K.; Legge, J.; Gould, I. Antibiograms of resistant Gram-negative bacteria from Scottish CF patients. J. Cyst. Fibros. 2004, 3, 151–157. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Checkerboard | Categorical | Kappa Statistics | ||||
|---|---|---|---|---|---|---|
| Gradient Method | Synergy | Indifference | Total | Agreement (%) | K | p-Value |
| Cross | 60.00 | 0.169 | 0.129 | |||
| Synergy | 12 | 20 | 32 | |||
| Indifference | 8 | 30 | 38 | |||
| Direct overlay | 77.14 | 0.291 | 0.002 | |||
| Synergy | 5 | 1 | 6 | |||
| Indifference | 15 | 49 | 64 | |||
| MIC:MIC | 71.43 | 0.205 | 0.071 | |||
| Synergy | 6 | 6 | 12 | |||
| Indifference | 14 | 44 | 58 | |||
| Checkerboard | Categorical | Kappa Statistics | ||||||
|---|---|---|---|---|---|---|---|---|
| Gradient Method | 0–2 | 2–50 | 50–100 | >100 | Total | Agreement (%) | K | p-Value |
| Cross | 82.86 | 0.662 | <0.001 | |||||
| 0–2 | 30 | 7 | 0 | 0 | 37 | |||
| 2–50 | 4 | 28 | 0 | 1 | 33 | |||
| 50–100 | 0 | 0 | 0 | 0 | 0 | |||
| >100 | 0 | 0 | 0 | 0 | 0 | |||
| Direct overlay | 67.14 | 0.356 | 0.001 | |||||
| 0–2 | 31 | 19 | 0 | 0 | 50 | |||
| 2–50 | 3 | 16 | 0 | 1 | 20 | |||
| 50–100 | 0 | 0 | 0 | 0 | 0 | |||
| >100 | 0 | 0 | 0 | 0 | 0 | |||
| MIC:MIC | 77.14 | 0.556 | <0.001 | |||||
| 0–2 | 30 | 10 | 0 | 0 | 40 | |||
| 2–50 | 4 | 24 | 0 | 1 | 29 | |||
| 50–100 | 0 | 1 | 0 | 0 | 1 | |||
| >100 | 0 | 0 | 0 | 0 | 0 | |||
| Intraclass | 95% Confidence Interval | F Test with True Value 0 | |||||
|---|---|---|---|---|---|---|---|
| Method | Correlation | Lower Bound | Upper Bound | Value | df1 | df2 | p-Value |
| Cross | 0.386 | 0.302 | 0.465 | 2.280 | 419 | 419 | <0.001 |
| Direct Overlay | 0.259 | 0.165 | 0.347 | 1.743 | 419 | 419 | <0.001 |
| MIC:MIC | 0.542 | 0.469 | 0.607 | 3.424 | 419 | 419 | <0.001 |
| Gradient Diffusion Method % a (No. of Isolates) b | Comparator Agreement % a (No. of Isolates) b | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Resistance Profile | No * | Index | Result | CB £ | Cross | DO £ | MIC:MIC | Cross | DO £ | MIC:MIC | |
| TM (R #) | TZ (R #) | 33 | FICI | Syn $ | 21.21 (7) | 33.33 (11) | 15.15 (5) | 18.18 (6) | 57.14 (4) | 57.14 (4) | 28.57 (2) |
| NI $ | 78.79 (26) | 66.67 (22) | 84.85 (28) | 81.82 (27) | 69.23 (18) | 96.15 (25) | 84.62 (22) | ||||
| SBPI | ≤2.0 | 63.64 (21) | 78.79 (26) | 96.97 (32) | 72.73 (24) | 95.24 (20) | 100 (21) | 90.48 (19) | |||
| 2.0–50.00 | 36.36 (12) | 21.21 (7) | 3.03 (1) | 24.24 (8) | 50.00 (6) | 8.33 (1) | 50.00 (6) | ||||
| TM (R #) | TZ (I #) | 18 | FICI | Syn $ | 27.78 (5) | 66.67 (12) | 5.56 (1) | 5.56 (1) | 100.00 (5) | 20.00 (1) | 20.00 (1) |
| NI $ | 72.22 (13) | 33.33 (6) | 94.44 (17) | 94.44 (17) | 46.15 (13) | 100.00 (13) | 100.00 (13) | ||||
| SBPI | ≤2.0 | 66.67 (12) | 55.56 (10) | 61.11 (11) | 83.33 (15) | 83.33 (10) | 75.00 (9) | 91.67 (11) | |||
| 2.0–50.00 | 33.33 (6) | 44.44 (8) | 38.89 (7) | 16.67 (3) | 100.00 (6) | 66.67 (4) | 33.33 (2) | ||||
| TM (S #) | TZ (R #) | 11 | FICI | Syn $ | 45.45 (5) | 36.36 (4) | 0(0) | 45.45 (5) | 20.00 (1) | 0(0) | 60.00 (3) |
| NI $ | 54.55 (6) | 63.64 (7) | 100.00 (11) | 54.55 (6) | 50.00 (3) | 100.00 (6) | 66.67 (4) | ||||
| SBPI | ≤2.0 | 9.09 (1) | 0(0) | 45.45 (5) | 0(0) | 0(0) | 100.00 (1) | 0(0) | |||
| 2.0–50.00 | 81.82 (9) | 100.00 (11) | 54.55 (6) | 100.00 (11) | 100.00 (9) | 55.56 (5) | 100.00 (9) | ||||
| TM (S #) | TZ (I #) | 8 | FICI | Syn $ | 37.50 (3) | 62.50 (5) | 0(0) | 0(0) | 66.67 (2) | 0(0) | 0(0) |
| NI $ | 62.50 (5) | 37.50 (3) | 100.00 (8) | 100.00 (8) | 40.00 (2) | 100.00 (5) | 100.00 (5) | ||||
| SBPI | ≤2.0 | 0(0) | 12.50 (1) | 25.00 (2) | 12.50 (1) | 0(0) | 0(0) | 0(0) | |||
| 2.0–50.00 | 100.00 (8) | 87.50 (7) | 75.00 (6) | 87.50 (7) | 87.50 (7) | 75.00 (6) | 87.50 (7) | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okoliegbe, I.N.; Hijazi, K.; Cooper, K.; Ironside, C.; Gould, I.M. Antimicrobial Synergy Testing: Comparing the Tobramycin and Ceftazidime Gradient Diffusion Methodology Used in Assessing Synergy in Cystic Fibrosis-Derived Multidrug-Resistant Pseudomonas aeruginosa. Antibiotics 2021, 10, 967. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10080967
Okoliegbe IN, Hijazi K, Cooper K, Ironside C, Gould IM. Antimicrobial Synergy Testing: Comparing the Tobramycin and Ceftazidime Gradient Diffusion Methodology Used in Assessing Synergy in Cystic Fibrosis-Derived Multidrug-Resistant Pseudomonas aeruginosa. Antibiotics. 2021; 10(8):967. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10080967
Chicago/Turabian StyleOkoliegbe, Ijeoma N., Karolin Hijazi, Kim Cooper, Corinne Ironside, and Ian M. Gould. 2021. "Antimicrobial Synergy Testing: Comparing the Tobramycin and Ceftazidime Gradient Diffusion Methodology Used in Assessing Synergy in Cystic Fibrosis-Derived Multidrug-Resistant Pseudomonas aeruginosa" Antibiotics 10, no. 8: 967. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10080967