
The Acute Effects of Normobaric Hypoxia on Strength, Muscular Endurance and Cognitive Function: Influence of Dose and Sex

 , ,
, , 
 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
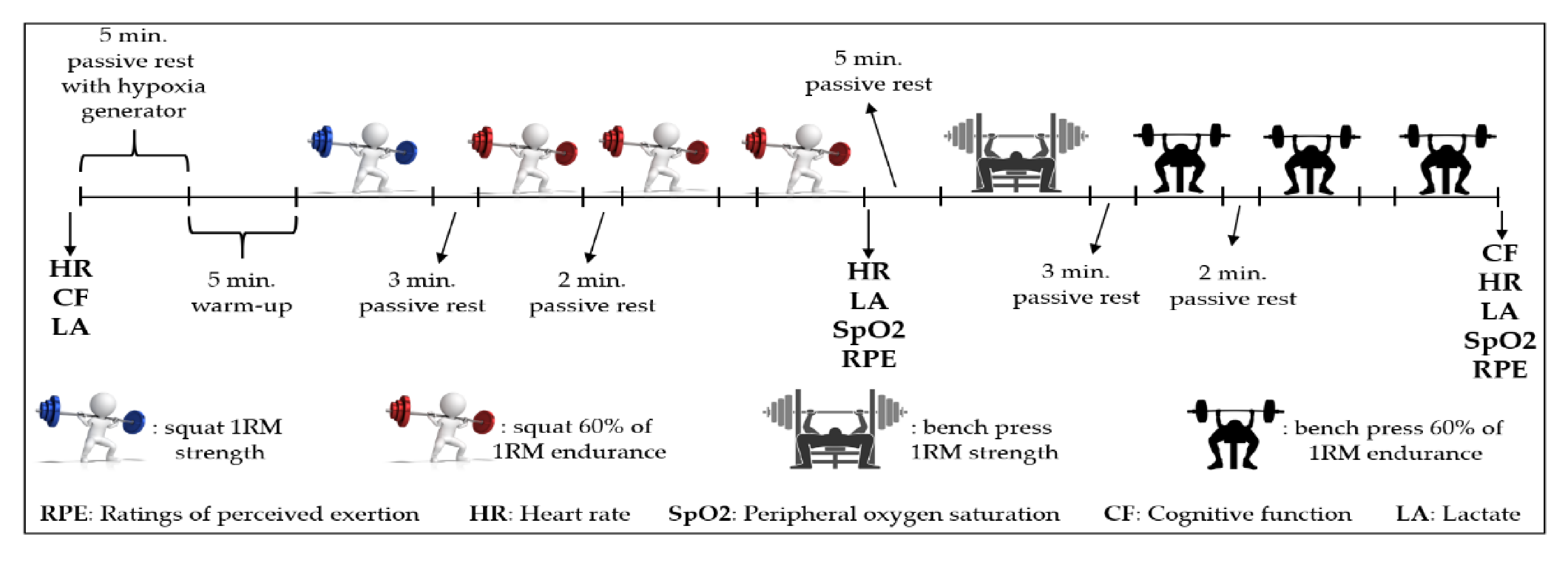
2.2. Study Design
RM Strength and 60% of 1RM Muscular Endurance Test Protocol
2.3. Cognitive Function
2.4. Statistical Analysis
3. Results
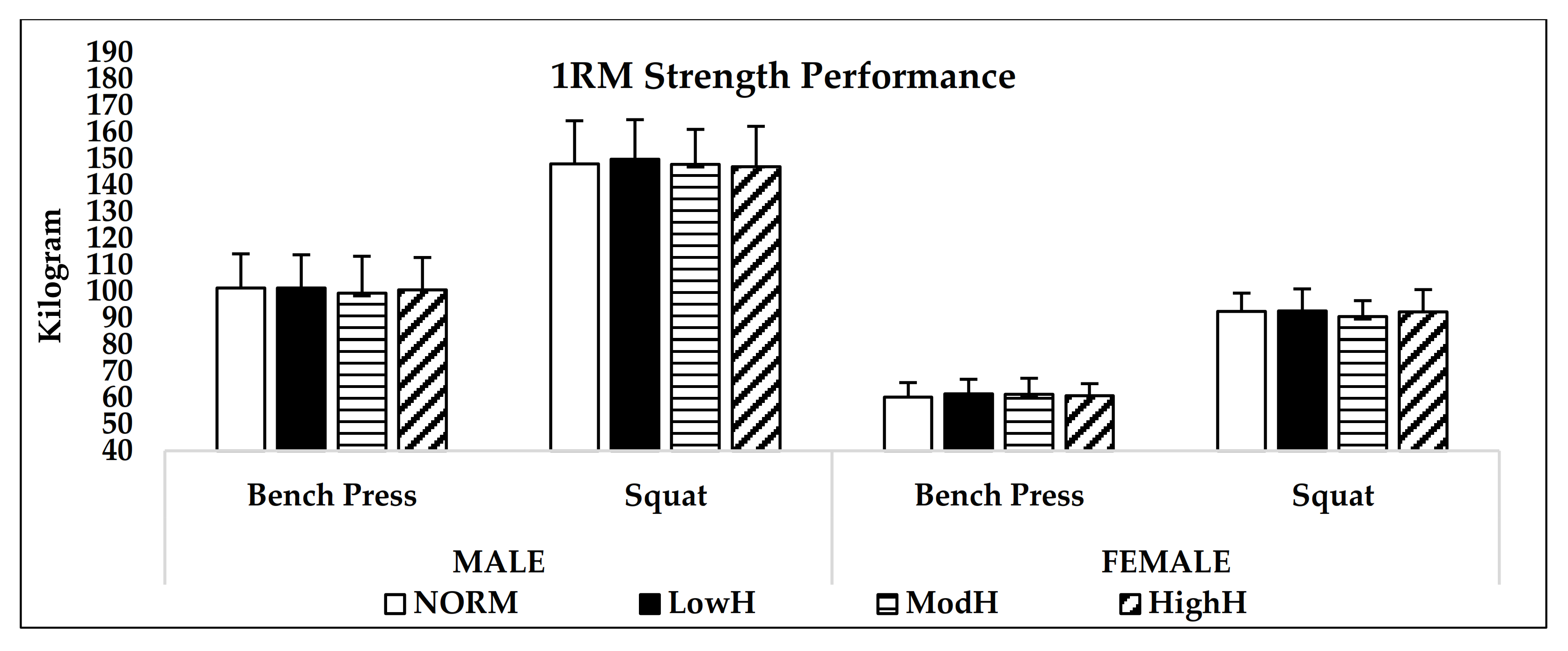
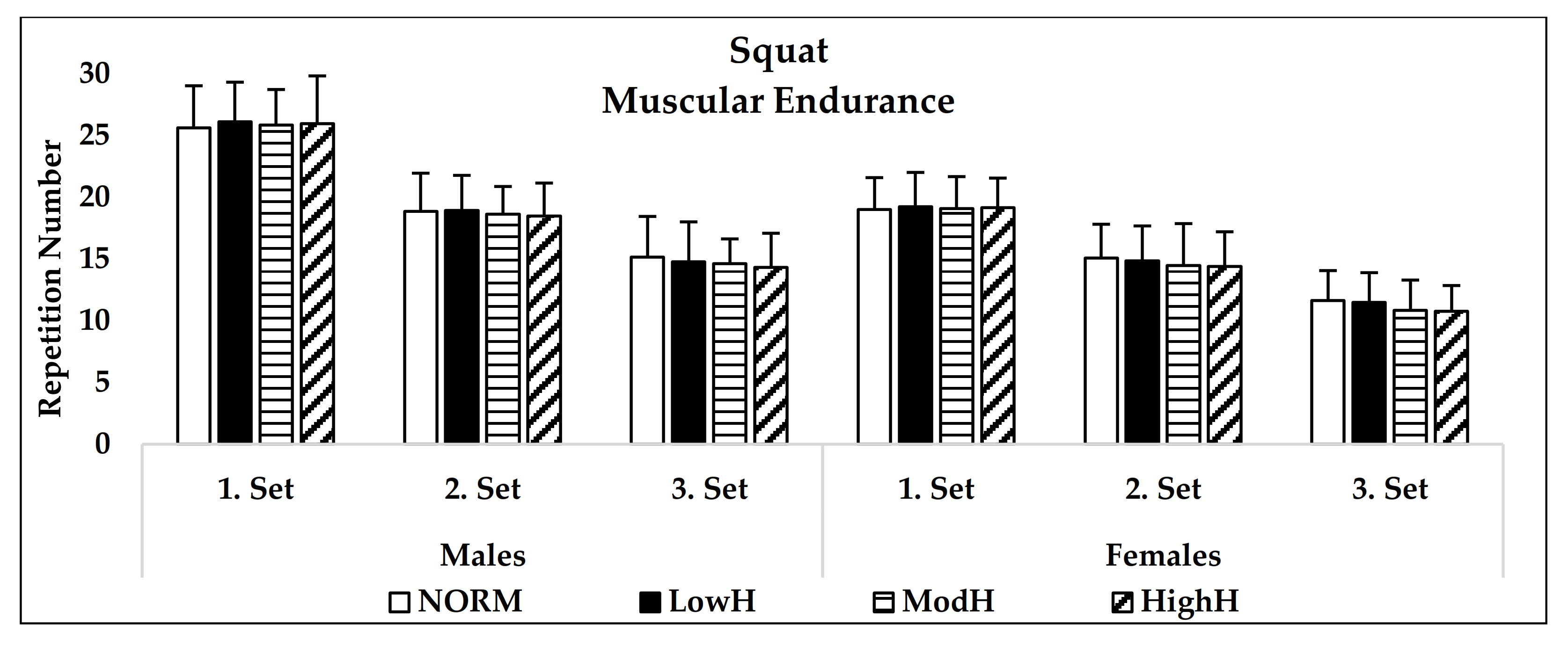
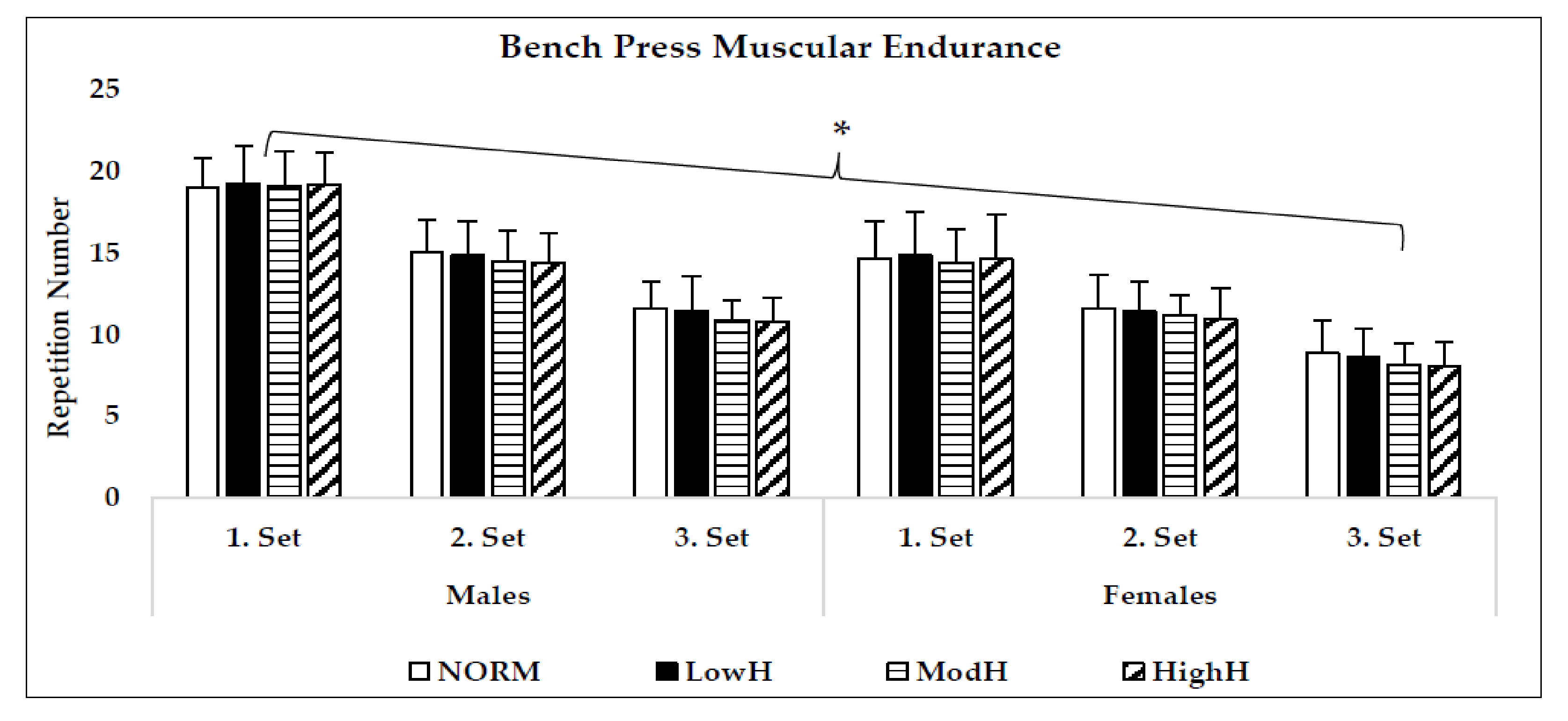
3.1. Maximum Strength (1RM) and 60% of 1RM Muscular Endurance Performance
3.2. Cognitive Function
3.3. Heart Rate, RPE, Lactate and Oxygen Saturation
4. Discussion
4.1. Strength (1RM) Performance
4.2. Muscular Endurance (60% of 1RM) Performance
4.3. Cognitive Performance
4.4. Heart Rate, RPE, Lactate
4.5. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Millet, G.P.; Roels, B.; Schmitt, L.; Woorons, X.; Richalet, J.P. Combining hypoxic methods for peak performance. Sports Med. 2010, 40, 1–25. [Google Scholar] [CrossRef] [PubMed]
- McLean, B.D.; Gore, C.J.; Kemp, J. Application of ‘live low-train high’ for enhancing normoxic exercise performance in team sport athletes. Sports Med. 2014, 44, 1275–1287. [Google Scholar] [CrossRef] [PubMed]
- Girard, O.; Brocherie, F.; Goods, P.S.R.; Millet, G.P. An updated panorama of “living low-train high” altitude/hypoxic methods. Front. Sports Act. Living 2020, 2, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scott, B.R.; Slattery, K.M.; Sculley, D.V.; Lockhart, C.; Dascombe, B.J. Acute physiological responses to moderate-load resistance exercise in hypoxia. J. Strength Cond. Res. 2017, 31, 1973–1981. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Li, Y.; Atakan, M.M.; Kuang, J.; Hu, Y.; Bishop, D.J.; Yan, X. The molecular adaptive responses of skeletal muscle to high-intensity exercise/training and hypoxia. Antioxidants 2020, 9, 656. [Google Scholar] [CrossRef]
- Smith, K.J.; Billaut, F. Influence of cerebral and muscle oxygenation on repeated-sprint ability. Eur. J. Appl. Physiol. 2010, 109, 989–999. [Google Scholar] [CrossRef]
- Amann, M.; Pegelow, D.F.; Jacques, A.J.; Dempsey, J.A. Inspiratory muscle work in acute hypoxia influences locomotor muscle fatigue and exercise performance of healthy humans. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2007, 293, R2036–R2045. [Google Scholar] [CrossRef]
- Jagim, A.R.; Dominy, T.A.; Camic, C.L.; Wright, G.; Doberstein, S.; Jones, M.T.; Oliver, J.M. Acute effects of the elevation training mask on strength performance in recreational weight lifters. J. Strength Cond. Res. 2018, 32, 482–489. [Google Scholar] [CrossRef]
- Feriche, B.; García-Ramos, A.; Morales-Artacho, A.J.; Padial, P. Resistance training using different hypoxic training strategies: A basis for hypertrophy and muscle power development. Sports Med. Open 2017, 3, 12. [Google Scholar] [CrossRef] [Green Version]
- Loenneke, J.; Fahs, C.; Rossow, L.; Abe, T.; Bemben, M. The anabolic benefits of venous blood flow restriction training may be induced by muscle cell swelling. Med. Hypotheses 2012, 78, 151–154. [Google Scholar] [CrossRef]
- Manimmanakorn, A.; Hamlin, M.J.; Ross, J.J.; Taylor, R.; Manimmanakorn, N. Effects of low-load resistance training combined with blood flow restriction or hypoxia on muscle function and performance in netball athletes. J. Sci. Med. Sport 2013, 16, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, A.; Sugita, M.; Kato, K.; Fukuda, A.; Sudo, A.; Uchida, A. Hypoxia increases muscle hypertrophy induced by resistance training. Int. J. Sports Physiol. Perform. 2010, 5, 497–508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaillou, T. Skeletal muscle fiber type in hypoxia: Adaptation to high-altitude exposure and under conditions of pathological hypoxia. Front. Physiol. 2018, 9, 1450. [Google Scholar] [CrossRef] [PubMed]
- Loenneke, J.; Wilson, G.; Wilson, J. A mechanistic approach to blood flow occlusion. Int. J. Sports Med. 2010, 31, 1–4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schoenfeld, B.J. The mechanisms of muscle hypertrophy and their application to resistance training. J. Strength Cond. Res. 2010, 24, 2857–2872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takarada, Y.; Nakamura, Y.; Aruga, S.; Onda, T.; Miyazaki, S.; Ishii, N. Rapid increase in plasma growth hormone after low-intensity resistance exercise with vascular occlusion. J. Appl. Physiol. 2000, 88, 61–65. [Google Scholar] [CrossRef] [Green Version]
- Namboonlue, C.; Hamlin, M.J.; Sirasaporn, P.; Manimmanakorn, N.; Wonnabussapawich, P.; Thuwakum, W.; Sumethanurakkhakun, W.; Manimmanakorn, A. Optimal degree of hypoxia combined with low-load resistance training for muscle strength and thickness in athletes. J. Phys. Educ. Sport 2020, 20, 828–838. [Google Scholar]
- Ramos-Campo, D.J.; Rubio-Arias, J.Á.; Freitas, T.T.; Camacho, A.; Jiménez-Diaz, J.F.; Alcaraz, P.E. Acute physiological and performance responses to high-intensity resistance circuit training in hypoxic and normoxic conditions. J. Strength Cond. Res. 2017, 31, 1040–1047. [Google Scholar] [CrossRef]
- Ramos-Campo, D.J.; Rubio-Arias, J.A.; Dufour, S.; Chung, L.; Ávila-Gandía, V.; Alcaraz, P.E. Biochemical responses and physical performance during high-intensity resistance circuit training in hypoxia and normoxia. Eur. J. Appl. Physiol. 2017, 117, 809. [Google Scholar] [CrossRef]
- Scott, B.R.; Slattery, K.M.; Sculley, D.V.; Hodson, J.A.; Dascombe, B.J. Physical performance during high-intensity resistance exercise in normoxic and hypoxic conditions. J. Strength Cond. Res. 2015, 29, 807–815. [Google Scholar] [CrossRef]
- Desplanches, D.; Hoppeler, H.; Linossier, M.T.; Denis, C.; Claassen, H.; Dormois, D.; Lacour, J.R.; Geyssant, A. Effects of training in normoxia and normobaric hypoxia on human muscle ultrastructure. Pflug. Arch. 1993, 425, 263–267. [Google Scholar] [CrossRef]
- Vieira, J.G.; Sardeli, A.V.; Dias, M.R.; Filho, J.E.; Campos, Y.; Sant’Ana, L.; Leitao, L.; Reis, V.; Wilk, M.; Novaes, J.; et al. Effects of resistance training to muscle failure on acute fatigue: A systematic review and meta-analysis. Sports Med. 2021. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Smith, C.M.; Salmon, O.F.; Jenkins, J.R. Effect of moderate and severe hypoxic exposure coupled with fatigue on psychomotor vigilance testing, muscle tissue exygenation, and muscular performance. Curr. Res. Phyisol. 2021, 4, 223–251. [Google Scholar]
- Martinez-Guardado, I.; Sanchez-Urena, B.; Olcina, G.; Camacho-Cardenosa, A.; Camacho-Cardenosa, M.; Timon, R. Bench press performance during an intermittent hypoxic resistance training to muscle failure. J. Sports Med. Phys. Fit. 2019, 59, 1138–1143. [Google Scholar] [CrossRef]
- Girard, O.; Mariotti-Nesurini, L.; Malatesta, D. Acute performance and physiological responses to upper-limb multi-set exercise to failure: Effects of external resistance and systemic hypoxia: Local and systemic hypoxia combined. Eur. J. Sport Sci. 2021, 1–28, Online ahead of print. [Google Scholar]
- Hunter, S.K. Sex differences in fatigability of dynamic contractions. Exp. Physiol. 2016, 101, 250–255. [Google Scholar] [CrossRef] [Green Version]
- Hively, K.; El-Alayli, A. “You throw like a girl:” The effect of stereotype threat on women’s athletic performance and gender stereotypes. Psychol. Sport Exerc. 2014, 15, 48–55. [Google Scholar] [CrossRef]
- Laurent, C.; Green, J.; Bishop, P.; Sjökvist, J.; Schumacker, R.; Richardson, M.; Curtner-Smith, M. Effect of gender on fatigue and recovery following maximal intensity repeated sprint performance. J. Sports Med. Phys. Fit. 2010, 50, 243–253. [Google Scholar]
- Laurent, C.M.; Vervaecke, L.S.; Kutz, M.R.; Green, J.M. Sex-specific responses to self-paced, high-intensity interval training with variable recovery periods. J. Strength Cond. Res. 2014, 28, 920–927. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sandoval, D.A.; Matt, K.S. Effects of the oral contraceptive pill cycle on physiological responses to hypoxic exercise. High Alt. Med. Biol. 2003, 4, 61–72. [Google Scholar] [CrossRef] [PubMed]
- Slater, J.P.; Guarino, T.; Stack, J.; Vinod, K.; Bustami, R.T.; Brown, J.M., III; Rodriguez, A.L.; Magovern, C.J.; Zaubler, T.; Freundlich, K. Cerebral oxygen desaturation predicts cognitive decline and longer hospital stay after cardiac surgery. Ann. Thorac. Surg. 2009, 87, 36–45. [Google Scholar] [CrossRef] [PubMed]
- Grgic, J.; Mikulic, P. Effects of attentional focus on muscular endurance: A meta-analysis. Int. J. Environ. Res. Public Health 2021, 19, 89. [Google Scholar] [CrossRef]
- Grgic, J.; Mikulic, I.; Mikulic, P. Acute and long-term effects of attentional focus strategies on muscular strength: A meta-analysis. Sports 2021, 9, 153. [Google Scholar] [CrossRef] [PubMed]
- Baechle, T.R.; Earle, R.W. Essentials of Strength Training and Conditioning; Human Kinetics: Champaign, IL, USA, 2008. [Google Scholar]
- Borg, G. Perceived exertion: A note on history and models. Med. Sci. Sports Exerc. 1973, 5, 90–93. [Google Scholar] [CrossRef]
- Eriksen, B.A.; Eriksen, C.W. Effects of noise letters upon the identification of a target letter in a nonsearch task. Percept. Psychophys. 1974, 16, 143–149. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Feriche, B.; Garcia-Ramos, A.; Calderon-Soto, C.; Drobnic, F.; Bonitch-Gongora, J.G.; Galilea, P.A.; Riera, J.; Padial, P. Effect of acute exposure to moderate altitude on muscle power: Hypobaric hypoxia vs. normobaric hypoxia. PLoS ONE 2014, 9, e114072. [Google Scholar] [CrossRef]
- Bazzuchi, I.; Felici, F.; Macaluso, A.; De Vito, G. Differences between young and older women in maximal force, force fluctuations, and surface EMG during isometric knee extension and elbow flexion. Muscle Nerve 2004, 30, 626–635. [Google Scholar] [CrossRef]
- Scott, B.R.; Slattery, K.M.; Dascombe, B.J. Intermittent hypoxic resistance training: Is metabolic stress the key moderator? Med. Hypotheses 2015, 84, 145–149. [Google Scholar] [CrossRef]
- Bowtell, J.L.; Cooke, K.; Turner, R.; Mileva, K.N.; Sumners, D.P. Acute physiological and performance responses to repeated sprints in varying degrees of hypoxia. J. Sci. Med. Sport 2014, 17, 399–403. [Google Scholar] [CrossRef]
- Cerqueira, M.S.; Lira, M.; Barboza, J.A.M.; Burr, J.F.; Wanderley E Lima, T.B.; Maciel, D.G.; De Brito Vieira, W.H. Repetition failure occurs earlier during low-load resistance exercise with high but not low blood flow restriction pressures. a systematic review and meta-analysis. J. Strength Cond. Res. 2021. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Wyatt, F. Physiological responses to altitude: A brief review. J. Exerc. Physiol. Online 2014, 17, 90–96. [Google Scholar]
- Deb, S.K.; Brown, D.R.; Gough, L.A.; Mclellan, C.P.; Swinton, P.A.; Sparks, S.A.; Mcnaughton, L.R. Quantifying the effects of acute hypoxic exposure on exercise performance and capacity: A systematic review and meta-regression. Eur. J. Sport Sci. 2018, 18, 243–256. [Google Scholar] [CrossRef] [PubMed]
- Walden, T.P.; Girard, O.; Jonson, A.M.; Dempsey, A.R.; Marston, K.J.; Scott, B.R. Sessional work-rate does not affect the magnitude to which simulated hypoxia can augment acute physiological responses during resistance exercise. Eur. J. Appl. Physiol. 2020, 120, 2159–2169. [Google Scholar] [CrossRef] [PubMed]
- Mage, D.T.; Donner, M. Female resistance to hypoxia: Does it explain the sex difference in mortality rates? J. Women’s Health 2006, 15, 786–794. [Google Scholar] [CrossRef]
- Koozehchian, M.; Karayigit, R.; Mabrey, G.; Newton, A. The effect of different doses of acute normobaric hypoxia on sprint interval training and cognitive performance. FASEB J. 2021, 35 (Suppl. 1). conference paper. [Google Scholar] [CrossRef]
- Haseler, L.J.; Hogan, M.C.; Richardson, R.S. Skeletal muscle phosphocreatine recovery in exercise-trained humans is dependent on O2 availability. J. Appl. Physiol. 1999, 86, 2013–2018. [Google Scholar] [CrossRef] [Green Version]
- Botek, M.; Krejci, J.; McKune, A. Sex differences in autonomic cardiac control and oxygen saturation response to short-term normobaric hypoxia and following recovery: Effect of aerobic fitness. Front. Endocrinol. 2018, 23, 697. [Google Scholar] [CrossRef]
- Lefferts, W.K.; Babcock, M.C.; Tiss, M.J.; Ives, S.J.; White, C.N.; Brutsaert, T.D.; Heffernan, K.S. Effect of hypoxia on cerebrovascular and cognitive function during moderate intensity exercise. Physiol. Behav. 2016, 165, 108–118. [Google Scholar] [CrossRef]
- Sun, S.; Loprinzi, P.D.; Guan, H.; Zou, L.; Kong, Z.; Hu, Y.; Shi, Q.; Nie, J. The effects of high-intensity interval exercise and hypoxia on cognition in sedentray young adults. Medicine 2019, 55, 43. [Google Scholar]
- Ando, S.; Hatamoto, Y.; Sudo, M.; Kiyonaga, A.; Tanaka, H.; Higaki, Y. The effects of exercise under hypoxia on cognitive function. PLoS ONE 2013, 8, e63630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Komiyama, T.; Sudo, M.; Higaki, Y.; Kiyonaga, A.; Tanaka, H.; Ando, S. Does moderate hypoxia alter working memory and executive function during prolonged exercise? Physiol. Behav. 2015, 139, 290–296. [Google Scholar] [CrossRef]
- Jung, M.; Zou, L.; Yu, J.J.; Ryu, S.; Kong, Z.; Yang, L.; Kang, M.; Lin, J.; Li, H.; Smith, L.; et al. Does exercise have protective effect on cognitive function unders hypoxia? A systematic review with meta-analysis. J. Sport Health Sci. 2020, 9, 562–577. [Google Scholar] [CrossRef] [PubMed]
- Ochi, G.; Kanazawa, Y.; Hyodo, K.; Suwabe, K.; Shimizu, T.; Fukuie, T.; Byun, K.; Soya, H. Hypoxia-induced lowered executive function depends on arterial oxygen desaturation. J. Physiol. Sci. 2018, 68, 847–853. [Google Scholar] [CrossRef] [PubMed]
- Peltonen, G.L.; Harrell, J.W.; Aleckson, B.P.; LaPlante, K.M.; Crain, M.K.; Schrage, W.G. Cerebral blood flow regulation in women across mentrual phase: Differential contribution of cyclooxygenase to basal, hypoxic, and hypercapnic vascular tone. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2016, 311, R222–R231. [Google Scholar] [CrossRef]
- Lei, O.K.; Kong, Z.; Loprinzi, P.D.; Shi, Q.; Sun, S.; Zou, L.; Hu, Y.; Nie, J. Severe hypoxia does not offset the benefits of exercise on cognitive function in sedentary young women. Int. J. Environ. Res. Public Health 2019, 16, 1003. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Males | Females | |||||||
|---|---|---|---|---|---|---|---|---|
| Pre Test | Post Test | Pre Test | Post Test | |||||
| M | SD | M | SD | M | SD | M | SD | |
| Response Accuracy [%]-Congruent Task | ||||||||
| NORM | 96.41 | 1.4 | 95.83 | 1.6 | 96.58 | 1.7 | 96.66 | 1.3 |
| LowH | 96.16 | 2.3 | 95.83 | 2.0 | 96.41 | 2.1 | 97.08 | 1.3 |
| ModH | 96.83 | 2.3 | 96.50 | 1.7 | 97.16 | 2.0 | 96.25 | 1.9 |
| HighH | 96.00 | 1.8 | 96.33 | 1.6 | 97.33 | 1.2 | 95.16 | 1.6 |
| Response Accuracy [%]-Incongruent Task | ||||||||
| NORM | 93.25 | 2.8 | 93.33 | 2.0 | 94.58 | 2.4 | 95.50 | 1.7 |
| LowH | 92.91 | 1.9 | 93.16 | 2.2 | 95.08 | 1.3 | 94.83 | 1.4 |
| ModH | 93.00 | 3.1 | 92.33 | 2.6 | 94.50 | 1.7 | 94.91 | 1.2 |
| HighH | 93.41 | 1.8 | 91.16 | 2.0 | 94.50 | 1.5 | 94.83 | 1.8 |
| Reaction Time [ms]-Congruent Task | ||||||||
| NORM | 493.45 | 42.2 | 480.77 | 46.2 | 533.40 | 44.3 | 517.70 | 47.7 |
| LowH | 496.80 | 38.9 | 485.53 | 46.9 | 541.04 | 39.1 | 518.55 | 30.3 |
| ModH | 497.90 | 42.8 | 494.21 * | 42.6 | 530.83 | 42.4 | 534.35 * | 34.8 |
| HighH | 491.95 | 40.0 | 502.68 * | 35.9 | 531.91 | 32.7 | 542.35 * | 38.2 |
| Reaction Time [ms]-Incongruent Task | ||||||||
| NORM | 531.81 | 31.5 | 516.94 | 25.3 | 608.10 | 49.9 | 596.34 | 55.1 |
| LowH | 546.70 | 31.4 | 528.46 # | 34.2 | 615.10 | 44.5 | 588.52 # | 45.0 |
| ModH | 541.22 | 27.3 | 535.80 * | 36.6 | 603.97 | 51.4 | 625.48 * | 59.1 |
| HighH | 542.53 | 29.7 | 567.42 * | 25.0 | 607.01 | 40.3 | 630.07 * | 34.2 |
| NORM | LowH | ModH | HighH | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Lactate (mmol/L) | |||||||||
| M | SD | M | SD | M | SD | M | SD | ||
| Males | Pretest | 1.2 | 0.1 | 1.23 | 0.2 | 1.14 | 0.1 | 1.15 | 0.1 |
| Postsquat | 6.56 | 1.1 | 6.45 | 1.0 | 6.54 | 1.1 | 6.61 | 1.0 | |
| Postbench | 7.11 | 1.2 | 7.23 # | 1.0 | 7.98 * | 1.2 | 7.94 * | 0.9 | |
| Females | Pretest | 1.26 | 0.1 | 1.2 | 0.1 | 1.11 | 0.1 | 1.13 | 0.1 |
| Postsquat | 5.66 | 0.7 | 5.7 | 0.4 | 5.83 | 0.4 | 5.91 | 0.7 | |
| Postbench | 6.01 | 0.7 | 6.13 # | 0.8 | 6.58 * | 0.5 | 6.91 * | 0.8 | |
| Heart Rate (beat/min) | |||||||||
| Males | Pretest | 64.75 | 4.9 | 63.50 | 5.31 | 64.33 | 3.6 | 64.58 | 4.8 |
| Postsquat | 173.25 | 8.6 | 171.33 | 5.39 | 172.33 | 4.7 | 171.33 | 7.4 | |
| Postbench | 176.08 | 8.4 | 175.08 | 10.4 | 175.33 | 8.1 | 176.08 | 7.6 | |
| Females | Pretest | 64.75 | 3.5 | 60.50 | 3.3 | 62.66 | 4.0 | 64.16 | 3.2 |
| Postsquat | 159.83 | 8.7 | 157.75 | 8.4 | 158.41 | 9.0 | 157.91 | 6.4 | |
| Postbench | 162.33 | 7.8 | 163.50 | 8.8 | 160.83 | 9.7 | 160.58 | 9.2 | |
| Ratings of Perceived Exertion (6–20) | |||||||||
| Males | Postsquat | 13.41 | 1.2 | 13.66 # | 1.0 | 13.58 * | 1.1 | 14.00 * | 1.2 |
| Postbench | 15.91 | 1.9 | 16.33 # | 1.6 | 17.00 * | 2.3 | 17.66 * | 2.1 | |
| Females | Postsquat | 13.50 | 1.7 | 13.83 # | 1.5 | 14.08 * | 1.6 | 13.91 * | 1.6 |
| Postbench | 17.41 | 1.9 | 17.08 # | 2.1 | 17.75 * | 1.9 | 18.33 * | 1.7 | |
| Oxygen Saturation (%) | |||||||||
| Males | Postsquat | 94.83 | 1.9 | 90.75 | 3.2 | 85.16 | 3.7 | 80.91 | 2.3 |
| Postbench | 94.33 | 1.8 | 89.58 | 2.9 | 83.91 | 3.8 | 79.83 | 2.5 | |
| Females | Postsquat | 95.08 | 1.5 | 90.16 | 2.7 | 86.41 | 2.6 | 81.83 | 2.4 |
| Postbench | 94.16 | 2.2 | 90.08 | 2.6 | 85.75 | 3.9 | 80.66 | 2.2 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karayigit, R.; Eser, M.C.; Sahin, F.N.; Sari, C.; Sanchez-Gomez, A.; Dominguez, R.; Koz, M. The Acute Effects of Normobaric Hypoxia on Strength, Muscular Endurance and Cognitive Function: Influence of Dose and Sex. Biology 2022, 11, 309. https://0-doi-org.brum.beds.ac.uk/10.3390/biology11020309
Karayigit R, Eser MC, Sahin FN, Sari C, Sanchez-Gomez A, Dominguez R, Koz M. The Acute Effects of Normobaric Hypoxia on Strength, Muscular Endurance and Cognitive Function: Influence of Dose and Sex. Biology. 2022; 11(2):309. https://0-doi-org.brum.beds.ac.uk/10.3390/biology11020309
Chicago/Turabian StyleKarayigit, Raci, Mustafa Can Eser, Fatma Nese Sahin, Cengizhan Sari, Angela Sanchez-Gomez, Raul Dominguez, and Mitat Koz. 2022. "The Acute Effects of Normobaric Hypoxia on Strength, Muscular Endurance and Cognitive Function: Influence of Dose and Sex" Biology 11, no. 2: 309. https://0-doi-org.brum.beds.ac.uk/10.3390/biology11020309