The Possible Relationship between the Abuse of Tobacco, Opioid, or Alcohol with COVID-19

 ,
,  and
and
Abstract
:1. Introduction
2. Substances Used Disorders (SUD) and COVID-19
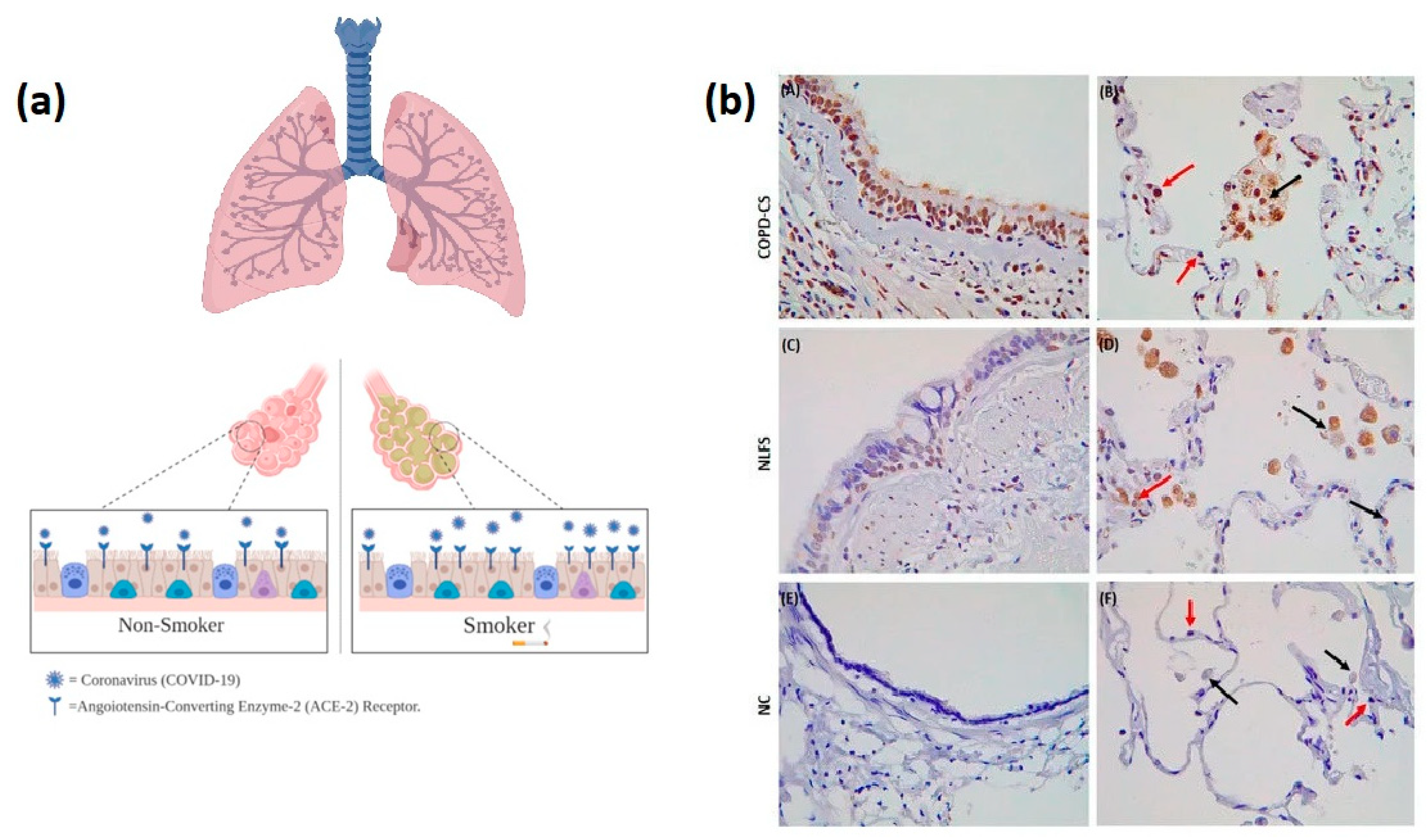
2.1. Tobacco Uses and COVID-19
2.2. Opioid Used Disorders and COVID-19
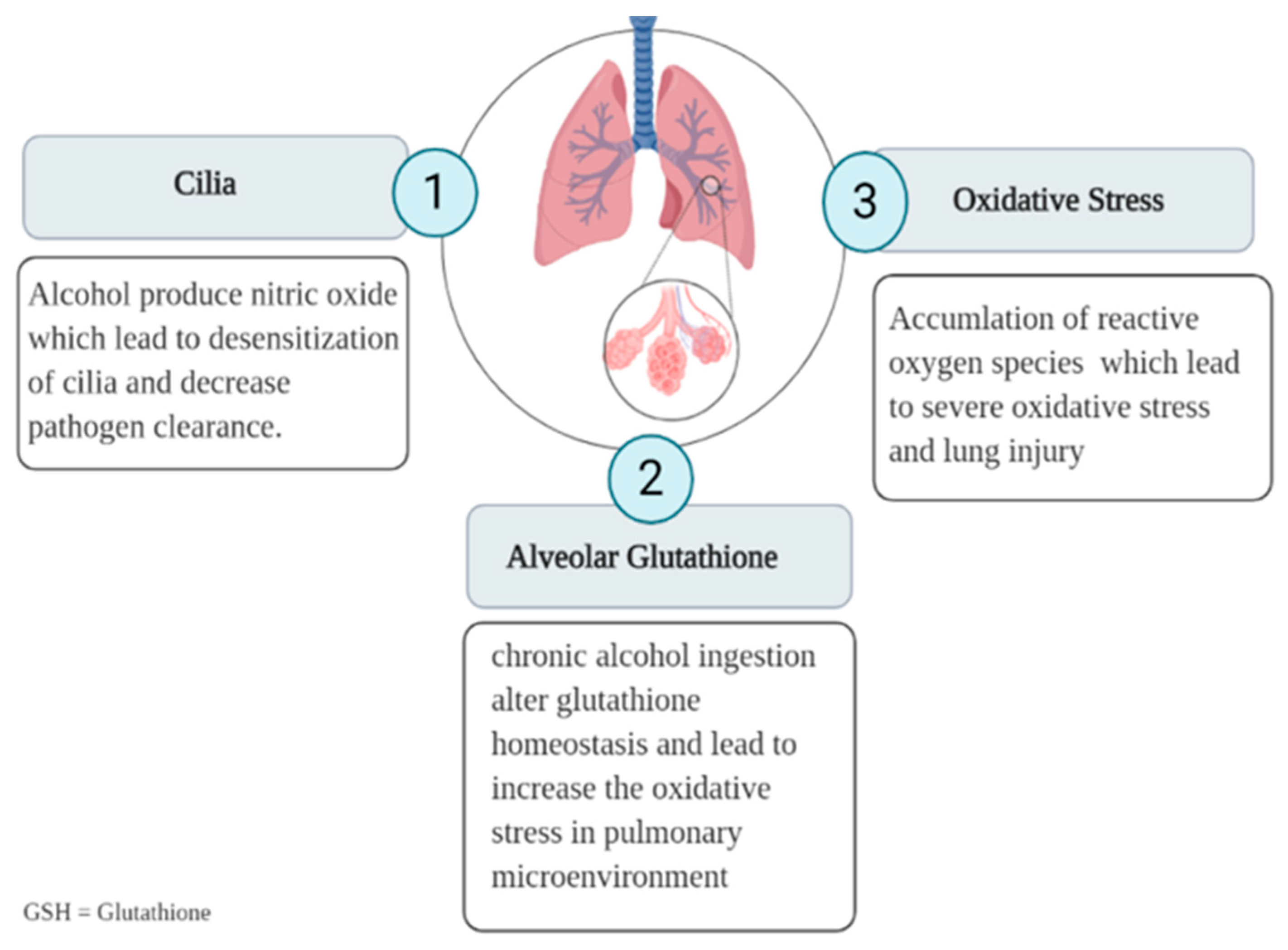
2.3. Alcohol Used and COVID-19
3. Possible COVID-19 Impact on SUDs
4. Conclusions and Future Considerations
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization WHO. Coronavirus. Available online: https://www.who.int/health-topics/coronavirus#tab=tab_1 (accessed on 29 October 2020).
- Ministry of Health, Saudi Arabia, MOH. Coronavirus. Available online: https://www.moh.gov.sa/en/HealthAwareness/EducationalContent/PublicHealth/Pages/corona.aspx (accessed on 29 October 2020).
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72,314 cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- CDC. Coronavirus. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/planning-scenarios.html (accessed on 29 October 2020).
- Serota, D.P.; A Barocas, J.; Springer, S.A. Infectious complications of addiction: A call for a new subspecialty within infectious diseases. Clin. Infect. Dis. 2020, 70, 968–972. [Google Scholar] [CrossRef] [PubMed]
- Nestler, E.J.; Lüscher, C. The molecular basis of drug addiction: Linking epigenetic to synaptic and circuit mechanisms. Neuron 2019, 102, 48–59. [Google Scholar] [CrossRef] [Green Version]
- Schluter, R.S. Stimulation of the Addicted Brain-Magnetic Stimulation as Add-On Treatment for Alcohol Use Disorder. Ph.D. Thesis, The University of Amsterdam, Amsterdam, The Netherlands, 5 June 2020. [Google Scholar]
- Hyman, S.E.; Malenka, R.C.; Nestler, E.J. Neural mechanisms of addiction: The role of reward-related learning and memory. Annu. Rev. Neurosci. 2006, 29, 565–598. [Google Scholar] [CrossRef] [Green Version]
- Brake, S.J.; Barnsley, K.; Lu, W.; McAlinden, K.D.; Eapen, M.S.; Sohal, S.S. Smoking Upregulates Angiotensin-Converting Enzyme-2 Receptor: A Potential Adhesion Site for Novel Coronavirus SARS-CoV-2 (Covid-19). J. Clin. Med. 2020, 9, 841. [Google Scholar] [CrossRef] [Green Version]
- Onor, I.O.; Stirling, D.L.; Williams, S.R.; Bediako, D.; Borghol, A.; Harris, M.B.; Darensburg, T.B.; Clay, S.D.; Okpechi, S.C.; Sarpong, D.F. Clinical effects of cigarette smoking: Epidemiologic impact and review of pharmacotherapy options. Int. J. Environ. Res. Public Health 2017, 14, 1147. [Google Scholar] [CrossRef] [Green Version]
- Vardavas, C.I.; Nikitara, K. COVID-19 and smoking: A systematic review of the evidence. Tob. Induc. Dis. 2020, 18, 20. [Google Scholar] [CrossRef]
- Zhang, J.-J.; Dong, X.; Cao, Y.-Y.; Yuan, Y.-D.; Yang, Y.-B.; Yan, Y.-Q.; A Akdis, C.; Gao, Y. Clinical characteristics of 140 patients infected with SARS-CoV-2 in Wuhan, China. Allergy 2020, 75, 1730–1741. [Google Scholar] [CrossRef]
- Liu, W.; Tao, Z.-W.; Wang, L.; Yuan, M.-L.; Liu, K.; Zhou, L.; Wei, P.-F.; Deng, Y.; Liu, J.; Liu, H.-G.; et al. Analysis of factors associated with disease outcomes in hospitalized patients with 2019 novel coronavirus disease. Chin. Med. J. 2020, 133, 1032–1038. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Patanavanich, R.; Glantz, S.A. Smoking is associated with COVID-19 progression: A meta-analysis. Nicotine Tob. Res. 2020, 22, 1653–1656. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Han, S.-X.; He, G.-M.; Wang, T.; Chen, L.; Ning, Y.-Y.; Luo, F.; An, J.; Yang, T.; Dong, J.-J.; Liao, Z.-L. Losartan attenuates chronic cigarette smoke exposure-induced pulmonary arterial hypertension in rats: Possible involvement of angiotensin-converting enzyme-2. Toxicol. Appl. Pharmacol. 2010, 245, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Vanderbruggen, N.; Matthys, F.; Van Laere, S.; Zeeuws, D.; Santermans, L.; Van den Ameele, S.; Crunelle, C.L. Self-reported alcohol, tobacco, and Cannabis use during COVID-19 lockdown measures: Results from a web-based survey. Eur. Addict. Res. 2020, 26, 309–315. [Google Scholar] [CrossRef]
- Lippi, G.; Henry, B.M. Active smoking is not associated with severity of coronavirus disease 2019 (COVID-19). Eur. J. Intern. Med. 2020, 75, 107–108. [Google Scholar] [CrossRef]
- Yuan, Y.-M.; Luo, L.; Guo, Z.; Yang, M.; Ye, R.-S.; Luo, C. Activation of renin–angiotensin–aldosterone system (RAAS) in the lung of smoking-induced pulmonary arterial hypertension (PAH) rats. J. Renin-Angiotensin-Aldosterone Syst. 2015, 16, 249–253. [Google Scholar] [CrossRef]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; Yu, T.; et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir. Med. 2020, 8, 475–481. [Google Scholar] [CrossRef] [Green Version]
- Cai, H. Sex difference and smoking predisposition in patients with COVID-19. Lancet Respir. Med. 2020, 8, e20. [Google Scholar] [CrossRef]
- Lobmaier, P.P.; Gossop, M.; Waal, H.; Bramness, J. The pharmacological treatment of opioid addiction—A clinical perspective. Eur. J. Clin. Pharmacol. 2010, 66, 537–545. [Google Scholar] [CrossRef]
- Nestler, E.J. Molecular basis of long-term plasticity underlying addiction. Nat. Rev. Neurosci. 2001, 2, 119–128. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, A.; Brown, S.-E.; Ghani, M.A.; Khan, F.; Kamarulzaman, A.; Altice, F.L. Pretreatment drug use characteristics and experiences among patients in a voluntary substance abuse treatment center in Malaysia: A mixed-methods approach. Subst. Abus. 2016, 37, 542–549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farhoudian, A.; Baldacchino, A.; Clark, N.; Gerra, G.; Ekhtiari, H.; Dom, G.; Mokri, A.; Sadeghi, M.; Nematollahi, P.; Demasi, M.; et al. COVID-19 and substance use disorders: Recommendations to a comprehensive healthcare response. An international society of addiction medicine (ISAM) practice and policy interest group position paper. Auton. Neurosci. Basic. Clin. 2020, 11, 129–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kienbaum, P.; Thurauf, N.; Michel, M.C.; Scherbaum, N.; Gastpar, M.; Peters, J. Profound increase in epinephrine concentration in plasma and cardiovascular stimulation after [micro sign]-opioid receptor blockade in opioid-addicted patients during barbiturate-induced anesthesia for acute detoxification. J. Am. Soc. Anesthesiol 1998, 88, 1154–1161. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Luo, R.; Wang, K.; Zhang, M.; Wang, Z.; Dong, L.; Li, J.; Yao, Y.; Ge, S.; Xu, G. Kidney disease is associated with in-hospital death of patients with COVID-19. Kidney Int. 2020, 97, 829–838. [Google Scholar] [CrossRef] [PubMed]
- Mallappallil, M.; Sabu, J.; Friedman, E.A.; Salifu, M. What do we know about opioids and the kidney? Int. J. Mol. Sci. 2017, 18, 223. [Google Scholar] [CrossRef] [Green Version]
- Kuo, Y.-F.; Raji, M.A.; Chen, N.-W.; Hasan, H.; Goodwin, J.S. Trends in opioid prescriptions among Part D Medicare recipients from 2007 to 2012. Am. J. Med. 2016, 129, 221.e21–221.e30. [Google Scholar] [CrossRef] [Green Version]
- Porubsky, S.; Kuppe, C.; Maier, T.; Birk, H.-W.; Wörnle, M.; Moeller, M.J.; Floege, J.; Gröne, H.-J. Renal lipidosis in patients enrolled in a methadone substitution program. Arch. Pathol. Lab. Med. 2014, 138, 689–693. [Google Scholar] [CrossRef]
- Hirsch, J.S.; Ng, J.H.; Ross, D.W.; Sharma, P.; Shah, H.H.; Barnett, R.L.; Hazzan, A.D.; Fishbane, S.; Jhaveri, K.D.; Abate, M.; et al. Acute kidney injury in patients hospitalized with COVID-19. Kidney Int. 2020, 98, 209–218. [Google Scholar] [CrossRef]
- Cheng, Y.; Luo, R.; Wang, K.; Zhang, M.; Wang, Z.; Dong, L.; Li, J.; Yao, Y.; Ge, S.; Xu, G. Kidney impairment is associated with in-hospital death of COVID-19 patients. MedRxiv 2020. [Google Scholar] [CrossRef]
- Davis, M.P.; Srivastava, M. Demographics, assessment and management of pain in the elderly. Drugs Aging 2003, 20, 23–57. [Google Scholar] [CrossRef] [PubMed]
- Feng, G.; Luo, Q.; Guo, E.; Yao, Y.; Yang, F.; Zhang, B.; Li, L. Multiple organ dysfunction syndrome, an unusual complication of heroin intoxication: A case report and review of literature. Int. J. Clin. Exp. Pathol. 2015, 8, 11826–11830. [Google Scholar] [PubMed]
- Pert, C.B.; Snyder, S.H. Opiate receptor: Demonstration in nervous tissue. Science 1973, 179, 1011–1014. [Google Scholar] [CrossRef] [PubMed]
- Kuczeriszka, M.; Lipkowski, A.W.; Sadowski, J.; Kompanowska-Jezierska, E. An endomorphine analog ([d-Ala2]-Endomorphin 2, TAPP) lowers blood pressure and enhances tissue nitric oxide in anesthetized rats. Pharmacol. Reports. 2016, 68, 616–619. [Google Scholar] [CrossRef]
- Schenk, H.D.; Radke, J.; Ensink, F.B.; Drobnik, L.; Kettler, D.; Sonntag, H.; Hellige, G.; Bretschneider, H.J. Interactions between renal and general hemodynamics in fentanyl, droperidol, ketamine, thiopental and in peridural anesthesia--animal studies. Anaesthesiol Reanim. 1995, 20, 60–70. [Google Scholar]
- De Marchi, S.; Cecchin, E.; Basile, A.; Bertotti, A.; Nardini, R.; Bartoli, E. Renal tubular dysfunction in chronic alcohol abuse--effects of abstinence. N. Engl. J. Med. 1993, 329, 1927–1934. [Google Scholar] [CrossRef]
- Ginsberg, M.D.; Hertzman, M.; Schmidt-Nowara, W.W. Amphetamine intoxication with coagulopathy, hyperthermia, and reversible renal failure: A syndrome resembling heatstroke. Ann. Intern. Med. 1970, 73, 81–85. [Google Scholar] [CrossRef]
- Merigian, K.S.; Roberts, J.R. Cocaine intoxication: Hyperpyrexia, rhabdomyolysis and acute renal failure. J. Toxicol. Clin. Toxicol. 1987, 25, 135–148. [Google Scholar] [CrossRef]
- Fabrizio, L.; Regan, T.J. Alcoholic cardiomyopathy. Cardiovasc. Drugs. Ther. 1994, 8, 89–94. [Google Scholar] [CrossRef]
- Routsi, C.; Kolias, S.; Kaskarellis, I.; Politis, P.; Zervou, M.; Filippatos, G.; Roussos, C. Acute cardiomyopathy and cardiogenic pulmonary edema after inhaled heroin use. Acta Anaesthesiol. Scand. 2007, 51, 262–264. [Google Scholar] [CrossRef]
- Duell, P.B. Chronic cocaine abuse and dilated cardiomyopathy. Am. J. Med. 1987, 83, 601. [Google Scholar] [CrossRef]
- O’Connell, J.J. Dying in the shadows: The challenge of providing health care for homeless people. Can. Med Assoc. J. 2004, 170, 1251–1252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sherwood, N.R. A Self-Care Guide to Surviving and Thriving During Covid-19; Mary Hoch Center for Reconciliation, George Mason University: Arlington, VA, USA, 2020. [Google Scholar]
- Kershaw, C.D.; Guidot, D.M. Alcoholic lung disease. Alcohol Res. Heal. 2008, 31, 66. [Google Scholar]
- Kolovou, G.D.; Salpea, K.D.; Anagnostopoulou, K.K.; Mikhailidis, D.P. Alcohol use, vascular disease, and lipid-lowering drugs. J. Pharmacol. Exp. Ther. 2006, 318, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moss, M.; Guidot, D.M.; Wong-Lambertina, M.; Hoor, T.T.; Perez, R.L.; Yeligar, S.M. The effects of chronic alcohol abuse on pulmonary glutathione homeostasis. Am. J. Respir. Crit. Care Med. 2000, 161, 414–419. [Google Scholar] [CrossRef]
- Yeligar, S.M.; Chen, M.M.; Kovacs, E.J.; Sisson, J.H.; Burnham, E.L.; Yeligar, S.M. Alcohol and lung injury and immunity. Alcohol 2016, 55, 51–59. [Google Scholar] [CrossRef] [Green Version]
- Da, B.L.; Im, G.Y.; Schiano, T.D. COVID-19 hangover: A rising tide of alcohol use disorder and alcohol-associated liver disease. Hepatology 2020, 72, 1102–1108. [Google Scholar] [CrossRef]
- Rehm, J.; Kilian, C.; Ferreira-Borges, C.; Jernigan, D.; Monteiro, M.; Parry, C.D.H.; Sanchez, Z.M.; Manthey, J. Alcohol use in times of the COVID 19: Implications for monitoring and policy. Drug Alcohol Rev. 2020, 39, 301–304. [Google Scholar] [CrossRef]
- Clay, J.M.; Parker, M.O. Alcohol use and misuse during the COVID-19 pandemic: A potential public health crisis? Lancet Public Heal. 2020, 5, e259. [Google Scholar] [CrossRef]
- Frank, A.; Fatke, B.; Frank, W.; Förstl, H.; Hölzle, P. Depression, dependence and prices of the COVID-19-Crisis. Brain Behav. Immun. 2020, 87, 99. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.H.; Ho, R.C. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int. J. Environ. Res. Public Heal. 2020, 17, 1729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bolton, J.; Robinson, J.; Sareen, J. Self-medication of mood disorders with alcohol and drugs in the National Epidemiologic Survey on Alcohol and Related Conditions. J. Affect Disord. 2009, 115, 367–375. [Google Scholar] [CrossRef] [PubMed]
- Clay, J.M.; Parker, M.O. The role of stress-reactivity, stress-recovery and risky decision-making in psychosocial stress-induced alcohol consumption in social drinkers. Psychopharmacology 2018, 235, 3243–3257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sayette, M.A. Does drinking reduce stress? Alcohol Res. Heal. 1999, 23, 250–255. [Google Scholar]
- Lau, J.T.-F.; Yang, X.; Pang, E.; Tsui, H.; Wong, E.; Wing, Y.K. SARS-related perceptions in Hong Kong. Emerg. Infect. Dis. 2005, 11, 417–424. [Google Scholar]
- Wu, P.; Liu, X.; Fang, Y.; Fan, B.; Fuller, C.J.; Guan, Z.; Yao, Z.; Kong, J.; Lu, J.; Litvak, I.J. Alcohol abuse/dependence symptoms among hospital employees exposed to a SARS outbreak. Alcohol Alcohol. 2008, 43, 706–712. [Google Scholar] [CrossRef]
- Ahmed, M.Z.; Ahmed, O.; Aibao, Z.; Hanbin, S.; Siyu, L.; Ahmad, A. Epidemic of COVID-19 in China and associated Psychological Problems. Asian J. Psychiatr. 2020, 51, 102092. [Google Scholar] [CrossRef]
- Arya, S.; Gupta, R. COVID-19 outbreak: Challenges for Addiction services in India. Asian J. Psychiatr. 2020, 51, 102086. [Google Scholar] [CrossRef]
- Sinha, R. New findings on biological factors predicting addiction relapse vulnerability. Curr. Psychiatry Rep. 2011, 13, 398–405. [Google Scholar] [CrossRef] [Green Version]
- Bossi, M.M.; Tufoni, M.; Zaccherini, G.; Antognoli, A.; Domenicali, M.; Caraceni, P. A web-based group treatment for patients with alcoholic liver diseases at the time of the COVID-19 pandemic. Dig. Liver Dis. 2020, 52, 956–957. [Google Scholar] [CrossRef]
- Green, T.C.; Bratberg, J.; Finnell, D.S. Opioid use disorder and the COVID 19 pandemic: A call to sustain regulatory easements and further expand access to treatment. Subst. Abus. 2020, 41, 147–149. [Google Scholar] [CrossRef] [PubMed]
- Pouget, E.R.; Sandoval, M.; Nikolopoulos, G.K.; Friedman, S.R. Immediate impact of Hurricane Sandy on people who inject drugs in New York City. Subst. Use Misuse 2015, 50, 878–884. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Authors | Setting | Study Design and Time | Sample Size | Smoking and Severity of COVID-19 | ||
|---|---|---|---|---|---|---|
| Non-Severe | Severe | |||||
| Guan et al. [3] | China | Retrospective 29 January 020 | 1085 | Never smoked | n = 926 | n = 173 |
| 793 (86.9%) | 134 (77.9%) | |||||
| Former smoker | 12 (1.3%) | 9 (5.2%) | ||||
| Current smoker | 108 (11.8%) | 29 (16.9%) | ||||
| Zhang et al. [13] | China | Retrospective 16 January to 3 February 2020 | 140 | Current smoker | n = 82 | n = 58 |
| 0 (0%) | 2 (3.4%) | |||||
| Former smoker | 3 (3.7%) | 4 (6.9%) | ||||
| Liu et al. [14] | China | Retrospective from 30 December 2019 to 15 January 2020 | 78 | Current smoker | n = 67 | n = 11 |
| 2 (3%) | 3 (27.3%) | |||||
| Zhou et al. [15] | China | Retrospective multicenter cohort study until 31 January 2020 | 191 | Current smoker | n = 54 | n = 137 |
| 5 (9%) | 6 (4%) | |||||
| Huang et al. [17] | China | Prospective from 16 December 2019 to 2 January 2020 | 41 | Current smoker | Non-ICU care | ICU care |
| n = 3 (11%) | n = 0 | |||||
| Topic | Year | Author | Sitting | Finding | |
|---|---|---|---|---|---|
| Increased Alcohol intake during COVID 19 | 1 | March 2005 | Lau, et al. | The study conducted among more than 800 Hong Kong residents who were exposed to the Severe Acute Respiratory Syndrome (SARS) pandemic in 2003 conducted through 2 independent telephone surveys—survey 1 were asked about SARS-related perceptions—survey 2 were asked about psychological effects of SARS such as psychosomatic problems; had increased smoking and alcohol consumption; and other. | The study found high percentages of respondents felt helpless, horrified, and apprehensive because of SARS or worried that they or family members would get the virus. Approximately half of the respondents perceived that their mental health had severely or moderately deteriorated because of the SARS epidemic. Among those who consumed alcohol, 4.7% of male respondents and 14.8% of female respondents had increased their frequency of drinking 1 year after the SARS pandemic [63]. |
| 2 | 12 September 2008 | Wu et al. | A survey was conducted among 549 randomly selected hospital employees in Beijing, China, concerning the psychological impact of the 2003 SARS outbreak. | The study found increase in risk of reporting psychiatric symptoms, such as alcohol abuse/dependence 3 years after the SARS outbreak among hospital employees in Beijing who were either in quarantine or worked in high-risk hospital wards, was about 1.5 times higher than for nonexposed hospital employees [64]. | |
| 3 | April 1999 | Sayette, et al. | A review of human studies that investigate the following hypothesis whether drinking reduces stress? (The second part of the hypothesis—i.e., stress induces alcohol consumption) | In a review by Michael et al., a “stress-response-dampening theory” has been discussed, which refers to an increase in alcohol consumption during economic crises, especially among people suffering from anxiety and stress [62]. | |
| 4 | 11 November 2008 | Bolton et al. | A nation-wide household comorbidity survey (n = 43,093) conducted in 2001–2002 by the National Institute on Alcohol Abuse and Alcoholism. | The study conducted in 2001–2002 by the National Institute of Alcohol Abuse and Alcoholism reported of self-medication among people who try to cope with such stressful situations [60]. | |
| 5 | June 2020 | Ahmed, et al. | An online survey was conducted via Tencent on a sample of 1074 Chinese people, majority from Hubei province. To detect the mental health problems due to outbreak of the COVID-19 and mass isolation | The study was conducted among 1074 Chinese who showed an increased risk of potent psychiatric disorder with a higher rate of anxiety, depression, hazardous and harmful alcohol consumption, and lower mental wellbeing owing to the COVID-19 outbreak and mass isolation [65]. | |
| 6 | 6 March 2020 | Wang, et al. | a cross-sectional survey design to assess the public’s immediate psychological response during the epidemic of COVID-19 by using an anonymous online questionnaire that was firstly disseminated to university students and they were encouraged to pass it on to others. Included 1210 respondents from 194 cities in China. | The study mention factors that could trigger increased alcohol consumption as a form of self-medication; more than half of the population surveyed in China reported depression, anxiety, and/or stress [59]. | |
| 7 | 12 September 2018 | Clay, et al. | 39 participants were randomly allocated to ‘stress’ and ‘no-stress’ groups; in the stress group, participants took part in the Trier Social Stress Test (TSST). Participants completed several questionnaires and computer tasks in order to assess prior alcohol use, impulsivity/risk-taking, stress-reactivity, craving and physiological biomarkers of stress. Then, participants completed a voluntary drinking task. | The Trier Social Stress Test conducted among 39 social drinkers found an increase in alcohol craving behaviors among those who were under stressor compared with the non-stressor group [61]. | |
| 8 | 29 April 2020 | Frank, et al. | A cross-sectional evaluation sample of patients who were treated in Department of Psychiatry and Psychotherapy at München, Germany A short standardized interview was employed among 196 patients with main psychiatric diagnoses such as schizophrenia and addictive disorders. The examination included the Clinical Global Impression (CGI) Scale. | A study conducted in München, Germany, found that most people following these strict policies and lockdowns are suffering from the disruption of their daily routines, isolation, social distancing, financial worries, and fear of the future [58]. | |
| Decreased Alcohol intake during COVID 19 | 9 | May 2020 | Rehm, et al. | A systematic review of the effects of past economic crises on alcohol consumption systematic review of the effects of past economic crises on alcohol consumption. A systematic review of the effects of past economic crises on alcohol consumption systematic review of the effects of past economic crises on alcohol consumption. A systematic review of the effects of past economic crises on alcohol consumption and discussed of two possible scenarios of alcohol consumption during COVID 19 pandemic. | Jürgen et al. in a systematic review assessed the alcohol consumption behavior during the COVID-19 pandemic and found 2 scenarios: the first scenario predicts an increase in alcohol consumption and the other predicts a reduction in alcohol consumption. Increase consumption could linked to pandemic psychological effect and social restriction while decrease in alcohol intake could linked to the tight budgets and lower economic status of most population [56]. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Althobaiti, Y.S.; Alzahrani, M.A.; Alsharif, N.A.; Alrobaie, N.S.; Alsaab, H.O.; Uddin, M.N. The Possible Relationship between the Abuse of Tobacco, Opioid, or Alcohol with COVID-19. Healthcare 2021, 9, 2. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9010002
Althobaiti YS, Alzahrani MA, Alsharif NA, Alrobaie NS, Alsaab HO, Uddin MN. The Possible Relationship between the Abuse of Tobacco, Opioid, or Alcohol with COVID-19. Healthcare. 2021; 9(1):2. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9010002
Chicago/Turabian StyleAlthobaiti, Yusuf S., Maram A. Alzahrani, Norah A. Alsharif, Nawal S. Alrobaie, Hashem O. Alsaab, and Mohammad N. Uddin. 2021. "The Possible Relationship between the Abuse of Tobacco, Opioid, or Alcohol with COVID-19" Healthcare 9, no. 1: 2. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9010002