Validation of Clinical Characteristics and Effectiveness of Pulmonary Rehabilitation in a COPD Population with Discrepancy between Exercise Tolerance and FEV1

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
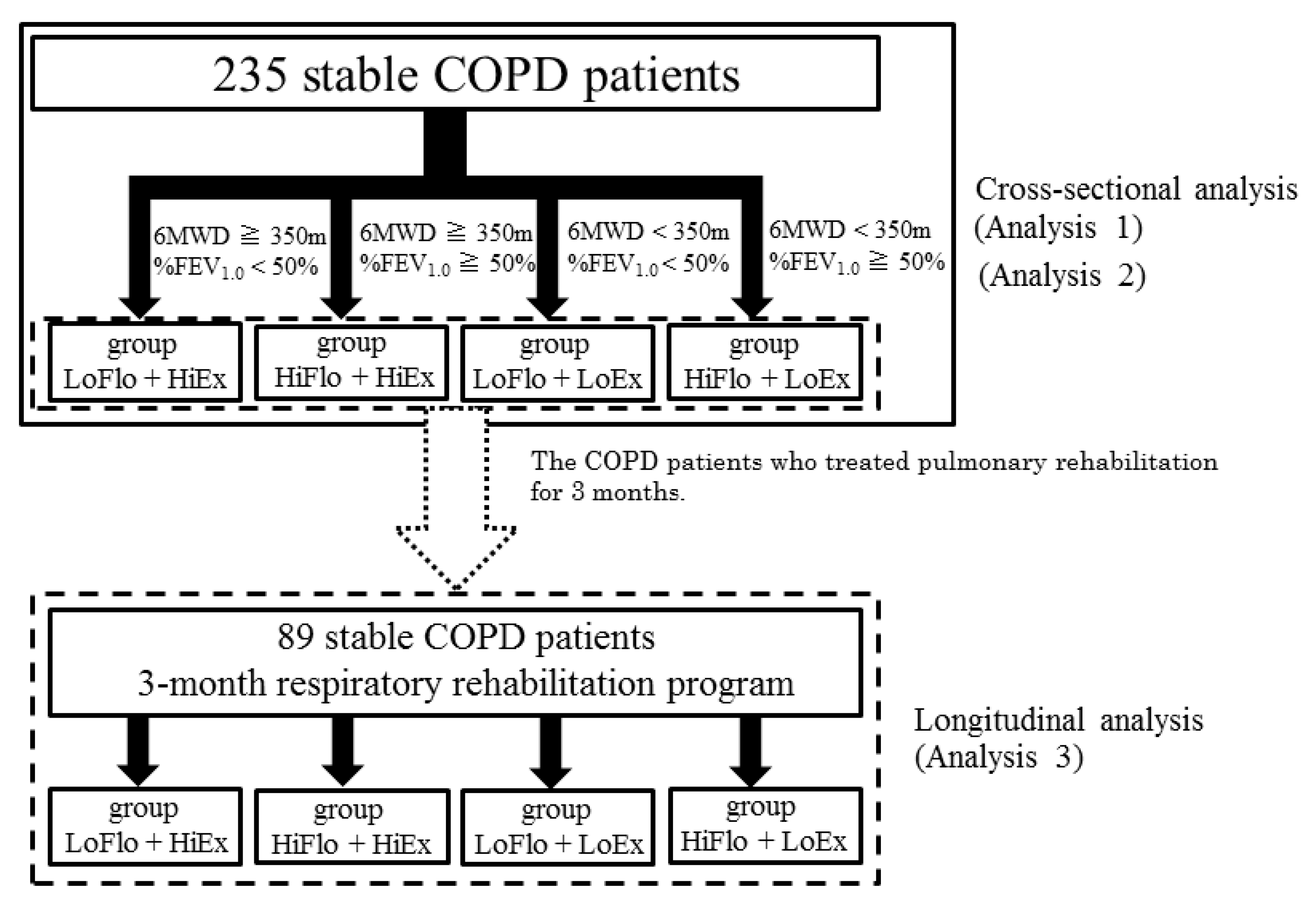
2.1. Study Design and Setting
2.2. Subjects
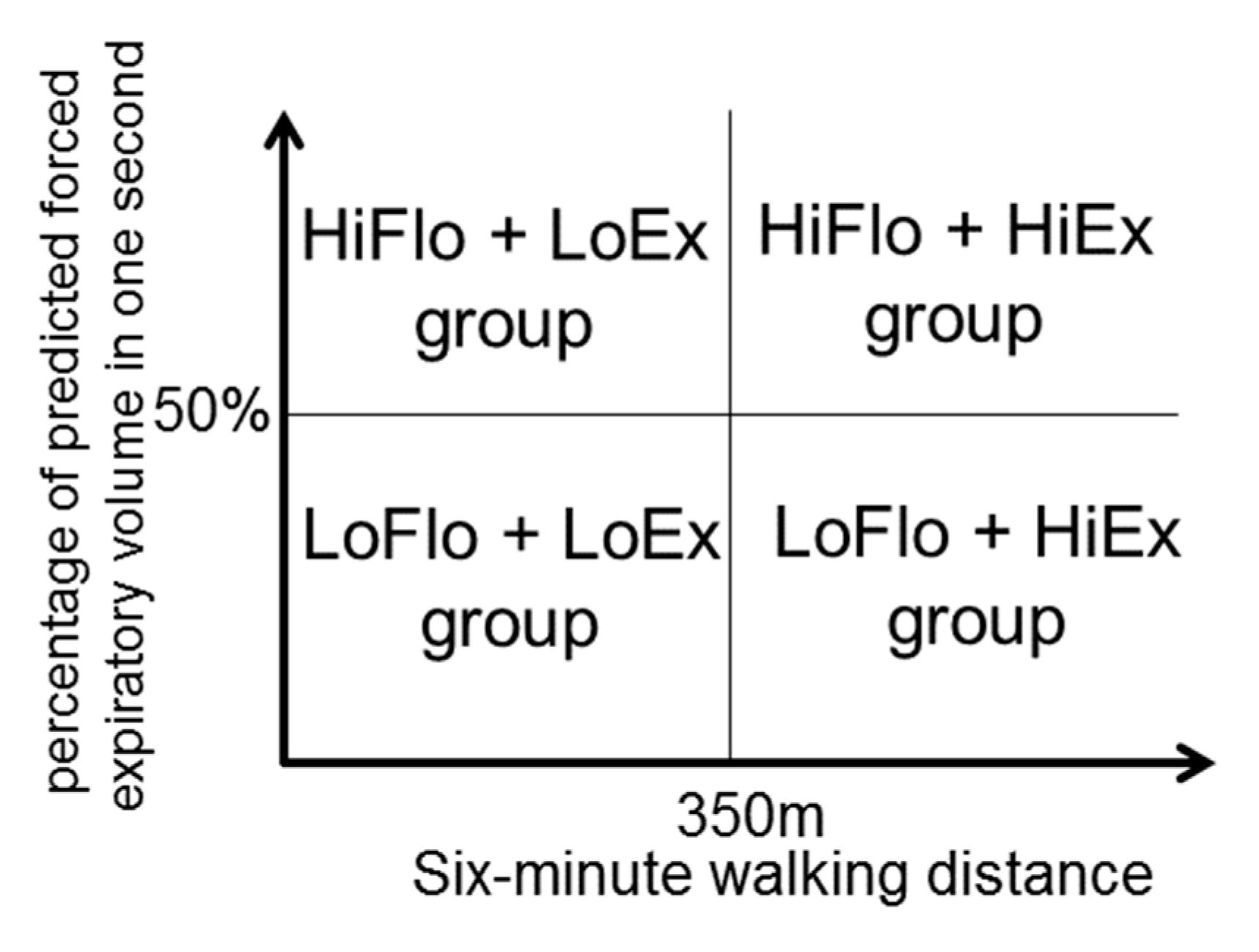
2.3. Group Assignment
2.4. Measurement Indicators
2.5. Study Protocol
2.6. Statistical Analysis
3. Results
3.1. The Characteristics of Four Groups in Patients with COPD
3.2. Relationship with Social Background in the LoFlo + HiEx and HiFlo + LoEx Groups
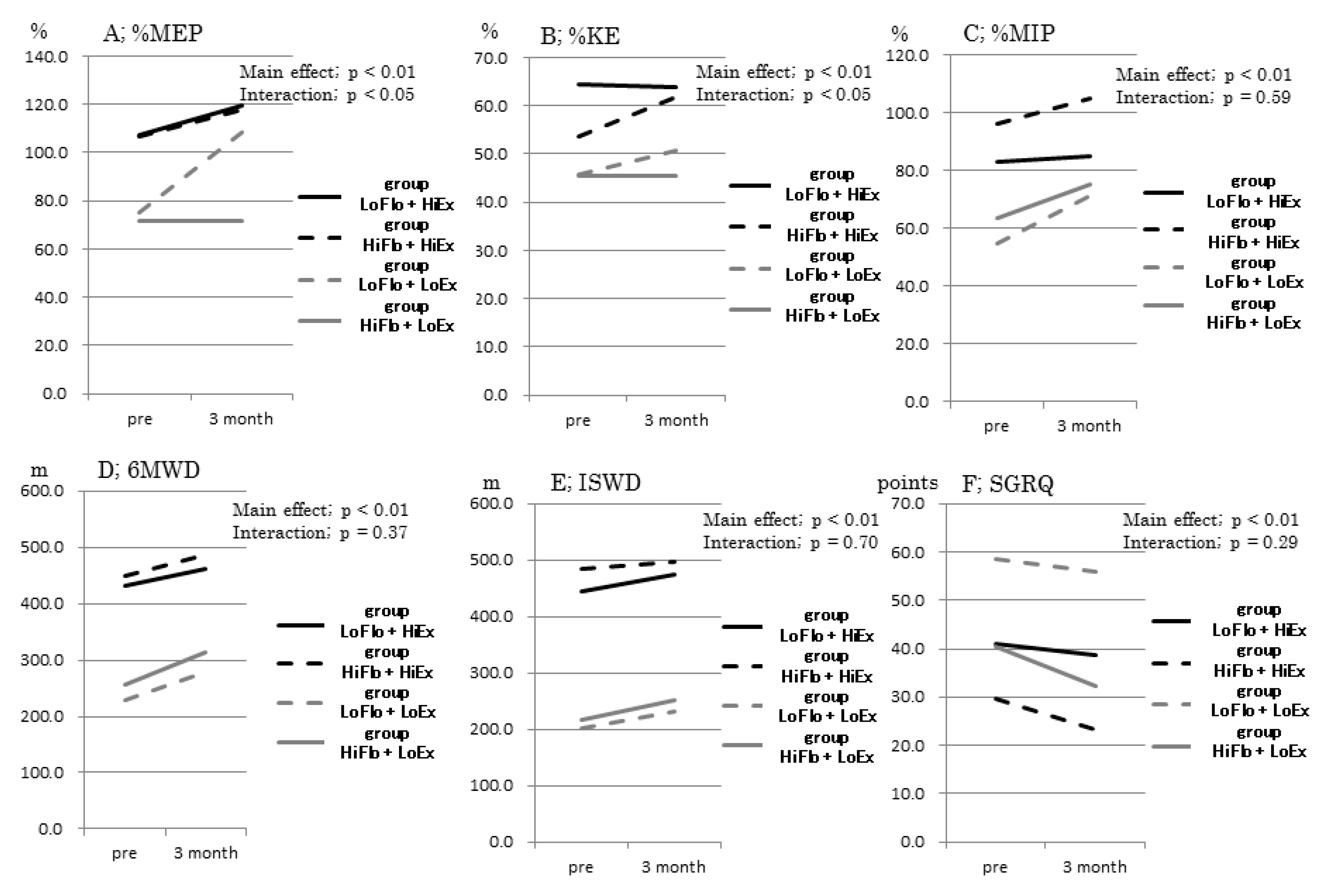
3.3. Comparison of Rehabilitation Effects in the LoFlo + HiEx and HiFlo + LoEx Groups
4. Discussion
5. Conclusions
5.1. What is Already Known on This Topic
5.2. What This Study Adds
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- O’Donnell, D.E.; Ora, J.; Webb, K.A.; Laveneziana, P.; Jensen, D. Mechanisms of activity-related dyspnea in pulmonary diseases. Respir. Physiol. Neurobiol. 2009, 167, 116–132. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, D.E.; Revill, S.M.; Webb, K.A. Dynamic hyperinflation and exercise intolerance in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2001, 164, 770–777. [Google Scholar] [CrossRef] [PubMed]
- Van Meerhaeghe, A.; Delpire, P.; Stenuit, P.; Kerkhofs, M. Flow limitation and dynamic hyperinflation. Eur. Respir. J. 2005, 25, 772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinto-Plata, V.M.; Celli-Cruz, R.A.; Vassaux, C.; Torre-Bouscoulet, L.; Mendes, A.; Rassulo, J.; Celli, B.R. Differences in cardiopulmonary exercise test results by American Thoracic Society/European Respiratory Society-Global Initiative for Chronic Obstructive Lung Disease stage categories and gender. Chest 2007, 132, 1204–1211. [Google Scholar] [CrossRef]
- O’Donnell, D.E.; Webb, K.A. The major limitation to exercise performance in COPD is dynamic hyperinflation. J. Appl. Physiol. 2008, 105, 753–755. [Google Scholar] [CrossRef]
- Vogiatzis, I.; Stratakos, G.; Athanasopoulos, D.; Georgiadou, O.; Golemati, S.; Koutsoukou, A.; Weisman, I.; Roussos, C.; Zakynthinos, S. Chest wall volume regulation during exercise in COPD patients with GOLD stages II to IV. Eur. Respir. J. 2008, 32, 42–52. [Google Scholar] [CrossRef]
- Garcia-Rio, F.; Lores, V.; Mediano, O.; Rojo, B.; Hernanz, A.; López-Collazo, E.; Alvarez-Sala, R. Daily physical activity in patients with chronic obstructive pulmonary disease is mainly associated with dynamic hyperinflation. Am. J. Respir. Crit. Care Med. 2009, 180, 506–512. [Google Scholar] [CrossRef]
- Tudorache, V.; Oancea, C.; Avram, C.; Fira-Mlădinescu, O. Changes in physical activity in healthy people and COPD patients. Wien. Klin. Wochenschr. 2014, 126, 30–35. [Google Scholar] [CrossRef]
- Global Initiative for Chronic Obstructive Lung Disease—GOLD. Available online: https://goldcopd.org (accessed on 14 December 2020).
- McCarthy, B.; Casey, D.; Devane, D.; Murphy, K.; Murphy, E.; Lacasse, Y. Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2015, 23, CD003793. [Google Scholar] [CrossRef]
- Sahin, H.; Naz, I.; Varol, Y.; Aksel, N.; Tuksavul, F.; Ozsoz, A. Is a pulmonary rehabilitation program effective in COPD patients with chronic hypercapnic failure? Expert Rev. Respir. Med. 2016, 10, 593–598. [Google Scholar] [CrossRef]
- Spruit, M.A.; Watkins, M.L.; Edwards, L.D.; Vestbo, J.; Calverley, P.M.; Pinto-Plata, V.; Celli, B.R.; Tal-Singer, R.; Wouters, E.F. Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) study investigators. Determinants of poor 6-min walking distance in patients with COPD: The ECLIPSE cohort. Respir. Med. 2010, 104, 849–857. [Google Scholar] [CrossRef] [PubMed]
- Celli, B.R.; Cote, C.G.; Marin, J.M.; Casanova, C.; Montes de Oca, M.; Mendez, R.A.; Pinto Plata, V.; Cabral, H.J. The body mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease. N. Engl. J. Med. 2004, 350, 1005–1012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; van der Grinten, C.P.; Gustafsson, P.; et al. ATS/ERS Task Force. ATS/ERS Task Force. Standardization of Spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [Green Version]
- Seymour, J.M.; Spruit, M.A.; Hopkinson, N.S.; Natanek, S.A.; Man, W.D.; Jackson, A.; Gosker, H.R.; Schols, A.M.; Moxham, J.; Polkey, M.I.; et al. The prevalence of quadriceps weakness in COPD and the relationship with disease severity. Eur. Respir. J. 2010, 36, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Casaburi, R.; Patessio, A.; Ioli, F.; Zanaboni, S.; Donner, C.F.; Wasserman, K. Reductions in exercise lactic acidosis and ventilation as a result of exercise training in patients with obstructive lung disease. Am. Rev. Respir. Dis. 1991, 143, 9–18. [Google Scholar] [CrossRef]
- Cesari, M.; Pedone, C.; Chiurco, D.; Cortese, L.; Conte, M.E.; Scarlata, S.; Incalzi, R.A. Physical performance, sarcopenia and respiratory function in older patients with chronic obstructive pulmonary disease. Age Ageing 2012, 41, 237–241. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.C.; Mofarrahi, M.; Hussain, S.N. Skeletal muscle dysfunction in patients with chronic obstructive pulmonary disease. Int. J. Chronic Obstr. Pulm. Dis. 2008, 3, 637–658. [Google Scholar] [CrossRef] [Green Version]
- Agusti, A.; Calverley, P.M.; Celli, B.; Coxson, H.O.; Edwards, L.D.; Lomas, D.A.; MacNee, W.; Miller, B.E.; Rennard, S.; Silverman, E.K.; et al. Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) investigators. Characterisation of COPD heterogeneity in the ECLIPSE cohort. Respir. Res. 2010, 11, 122. [Google Scholar] [CrossRef]
- Spencer, S.; Calverley, P.M.; Sherwood Burge, P.; Jones, P.W. ISOLDE Study Group. Inhaled Steroids in Obstructive Lung Disease. Health status deterioration in patients with chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2001, 163, 122–128. [Google Scholar] [CrossRef]
- Oga, T.; Nishimura, K.; Tsukino, M.; Sato, S.; Hajiro, T. Analysis of the factors related to mortality in chronic obstructive pulmonary disease: Role of exercise capacity and health status. Am. J. Respir. Crit. Care Med. 2003, 167, 544–549. [Google Scholar] [CrossRef] [Green Version]
- Hajiro, T.; Nishimura, K.; Tsukino, M.; Ikeda, A.; Koyama, H.; Izumi, T. Comparison of discriminative properties among disease-inconsistent questionnaires for measuring health-related quality of life in patients with chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 1998, 157, 785–790. [Google Scholar] [CrossRef] [PubMed]
- Troosters, T.; van der Molen, T.; Polkey, M.; Rabinovich, R.A.; Vogiatzis, I.; Weisman, I.; Kulich, K. Improving physical activity in COPD: Towards a new paradigm. Respir. Res. 2013, 14, 115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wedzicha, J.A.; Bestall, J.C.; Garrod, R.; Garnham, R.; Paul, E.A.; Jones, P.W. Randomized controlled trial of pulmonary rehabilitation in severe chronic obstructive pulmonary disease patients, stratified with the MRC dyspnoea scale. Eur. Respir. J. 1998, 12, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Katsura, H.; Kanemaru, A.; Yamada, K.; Motegi, T.; Wakabayashi, R.; Kida, K. Long-term effectiveness of an inpatient pulmonary rehabilitation program for elderly COPD patients: Comparison between young-elderly and old-elderly groups. Respirology 2004, 9, 230–236. [Google Scholar] [CrossRef]
- Holland, A.E.; Hill, C.J.; Rasekaba, T.; Lee, A.; Naughton, M.T.; McDonald, C.F. Updating the minimal important difference for six-minute walk distance in patients with chronic obstructive pulmonary disease. Arch. Phys. Med. Rehabil. 2010, 91, 221–225. [Google Scholar] [CrossRef]
- Puhan, M.A.; Mador, M.J.; Held, U.; Goldstein, R.; Guyatt, G.H.; Schünemann, H.J. Interpretation of treatment changes in 6-minute walk distance in patients with COPD. Eur. Respir. J. 2008, 32, 637–643. [Google Scholar] [CrossRef] [Green Version]
- Polkey, M.I.; Spruit, M.A.; Edwards, L.D.; Watkins, M.L.; Pinto-Plata, V.; Vestbo, J.; Calverley, P.M.; Tal-Singer, R.; Agustí, A.; Bakke, P.S.; et al. Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) Study Investigators. Six-minute-walk test in chronic obstructive pulmonary disease: Minimal clinically important difference for death or hospitalization. Am. J. Respir. Crit. Care Med. 2013, 187, 382–386. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| LoFlo + HiEx Group | HiFlo + HiEx Group | LoFlo + LoEx Group | HiFlo + LoEx Group | ||
|---|---|---|---|---|---|
| n | 50 | 78 | 69 | 38 | |
| male, % | 96 | 87.2 | 92.8 | 94.7 | |
| age, years old | 69.1 ± 10.0 | 71.9 ± 7.3 | 75.7 ± 7.8 | 79.2 ± 7.3 | ††, ‡‡ |
| %FEV1.0, % | 36.0 ± 7.9 | 74.5 ± 16.8 | 33.2 ± 9.6 | 74.4 ± 17.6 | **, ‡‡, |||| |
| 6MWD, m | 433 ± 59 | 456 ± 71 | 225 ± 99 | 252 ± 68 | ††, ‡‡, §§ |
| %FVC, % | 72.7 ± 19.3 | 91.7 ± 16.1 | 59.4 ± 16.1 | 86.1 ± 21.9 | **, ††, ‡‡, |||| |
| %MEP, % | 96.5 ± 35.7 | 89.0 ± 32.9 | 65.0 ± 32.0 | 65.0 ± 32.2 | ††, ‡‡, §§ |
| %MIP, % | 95.4 ± 41.3 | 90.9 ± 35.2 | 71.3 ± 40.5 | 67.0 ± 31.8 | †, ‡‡, § |
| %IBW, % | 99.1 ± 18.9 | 100.9 ± 17.1 | 91.1 ± 18.9 | 97.2 ± 15.9 | |
| mMRC | 1.7 ± 0.8 | 1.2 ± 0.7 | 2.8 ± 0.9 | 2.2 ± 0.8 | **, ††, ‡, §§, || |
| GP, kg | 34.2 ± 7.6 | 30.2 ± 8.3 | 25.2 ± 7.6 | 24.8 ± 7.4 | *, ††, ‡‡, §§ |
| %KE, % | 60.5 ± 15.3 | 55.3 ± 14.2 | 44.2 ± 14.3 | 45.1 ± 10.7 | ††, ‡‡, §§ |
| MGS, m/min | 113.6 ± 20.3 | 114.0 ± 22.3 | 81.0 ± 27.1 | 86.1 ± 18.0 | ††, ‡‡, §§ |
| TUG, sec | 5.9 ± 0.9 | 6.1 ± 1.3 | 9.7 ± 5.2 | 9.5 ± 4.0 | ††, ‡‡, §§ |
| CS-30, times | 18.0 ± 4.2 | 18.2 ± 4.3 | 12.0 ± 4.7 | 12.6 ± 3.3 | ††, ‡‡, §§ |
| ISWD, m | 404 ± 125 | 446 ± 156 | 193 ± 90 | 197 ± 95 | ††, ‡‡, §§ |
| NRADA, points | 80.5 ± 13.8 | 88.5 ± 12.9 | 54.7 ± 22.7 | 67.0 ± 20.5 | ††, ‡‡, §§, |||| |
| SGRQ points | 43.2 ± 17.1 | 34.9 ±1 7.5 | 55.8 ± 17.0 | 41.7 ± 13.3 | ††, |||| |
| HADS(A), points (n = 86) | 6.2 ± 2.8 | 4.4 ± 3.0 | 6.0 ± 3.6 | 5.7 ± 3.9 | |
| HADS(D), points (n = 86) | 7.9 ± 3.4 | 5.8 ± 3.0 | 8.2 ± 3.7 | 7.4 ± 2.9 |
| χ2 Value | p Value | |
|---|---|---|
| Employment status (employed or unemployed) | 5.04 | 0.54 |
| Marital status (married or not married) | 5.64 | 0.13 |
| Alcohol consumption (yes or no) | 10.59 | 0.01 |
| Smoking (yes or no) | 2.19 | 0.53 |
| Exercise habits (yes or no) | 7.79 | 0.05 |
| Driving a car (yes or no), | 10.89 | 0.01 |
| Comorbidities: cancer (yes or no) | 7.22 | 0.07 |
| Comorbidities: heart disease (yes or no) | 6.51 | 0.09 |
| Comorbidities: hyperlipidemia (yes or no) | 2.29 | 0.52 |
| Comorbidities: hypertension (yes or no) | 3.12 | 0.38 |
| Comorbidities: diabetes mellitus (yes or no) | 1.64 | 0.65 |
| Home oxygen therapy (yes or no) | 26.01 | <0.01 |
| House structure (one-story or two-story) | 2.59 | 0.46 |
| Environment around the home (flat or hilly) | 9.01 | 0.03 |
| Hospitalization for respiratory illness within the past year (yes or no) | 10.97 | 0.01 |
| Exacerbation within the past year (yes or no) | 7.27 | 0.06 |
| LoFlo + HiEx Group (n = 19) | HiFlo + HiEx Group (n = 30) | LoFlo + LoEx Group (n = 24) | HiFlo + LoEx Group (n = 16) | ||
|---|---|---|---|---|---|
| %MEP | 14.8 ± 17.9 | 14.7 ± 24.8 | 59.5 ± 78.4 | 35.9 ± 48.5 | § |
| %MIP | 9.0 ± 44.9 | 11.2 ± 29.9 | 33.9 ± 62.3 | 26.2 ± 39.1 | |
| %IBW | −0.2 ± 2.2 | −1.8 ± 6.9 | −0.5 ± 4.5 | 4.3 ± 19.2 | |
| mMRC | −32.0 ± 40.7 | −16.7 ± 42.2 | −4.2 ± 29.3 | −17.8 ± 23.1 | |
| GP | 2.1 ± 13.3 | 4.4 ± 17.2 | 7.8 ± 23.2 | 1.9 ± 8.9 | |
| %KE | −1.1 ± 16.9 | 18.8 ± 29.4 | 22.4 ± 33.4 | 1.6 ± 13.9 | † |
| MGS | 11.1 ± 16.5 | 3.9 ± 9.3 | 24.9 ± 47.1 | 15.9 ± 15.7 | |
| TUG | −5.9 ± 10.9 | −6.8 ± 9.2 | −9.2 ± 26.9 | −11.5 ± 9.5 | |
| CS-30 | 6.6 ± 18.9 | 12.1 ± 18.3 | 8.7 ± 11.5 | 13.8 ± 12.2 | |
| 6MWD | 7.7 ± 16.2 | 8.0 ± 8.6 | 31.0 ± 47.1 | 27.6 ± 31.2 | § |
| ISWD | 7.3 ± 14.4 | 4.2 ± 13.7 | 20.9 ± 27.3 | 23.1 ± 30.8 | # |
| NRADL | −0.2 ± 15.4 | 2.7 ± 6.2 | 8.6 ± 22.7 | 1.0 ± 27.8 | |
| SGRQ | 0.5 ± 33.2 | −17.7 ± 34.6 | −2.8 ± 20.7 | −20.2 ± 24.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Horie, J.; Takahashi, K.; Shiranita, S.; Anami, K.; Hayashi, S. Validation of Clinical Characteristics and Effectiveness of Pulmonary Rehabilitation in a COPD Population with Discrepancy between Exercise Tolerance and FEV1. Healthcare 2021, 9, 53. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9010053
Horie J, Takahashi K, Shiranita S, Anami K, Hayashi S. Validation of Clinical Characteristics and Effectiveness of Pulmonary Rehabilitation in a COPD Population with Discrepancy between Exercise Tolerance and FEV1. Healthcare. 2021; 9(1):53. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9010053
Chicago/Turabian StyleHorie, Jun, Koichiro Takahashi, Shuuichi Shiranita, Kunihiko Anami, and Shinichiro Hayashi. 2021. "Validation of Clinical Characteristics and Effectiveness of Pulmonary Rehabilitation in a COPD Population with Discrepancy between Exercise Tolerance and FEV1" Healthcare 9, no. 1: 53. https://0-doi-org.brum.beds.ac.uk/10.3390/healthcare9010053