
Chronic Endothelial Dysfunction after COVID-19 Infection Shown by Transcranial Color-Coded Doppler: A Cross-Sectional Study
 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
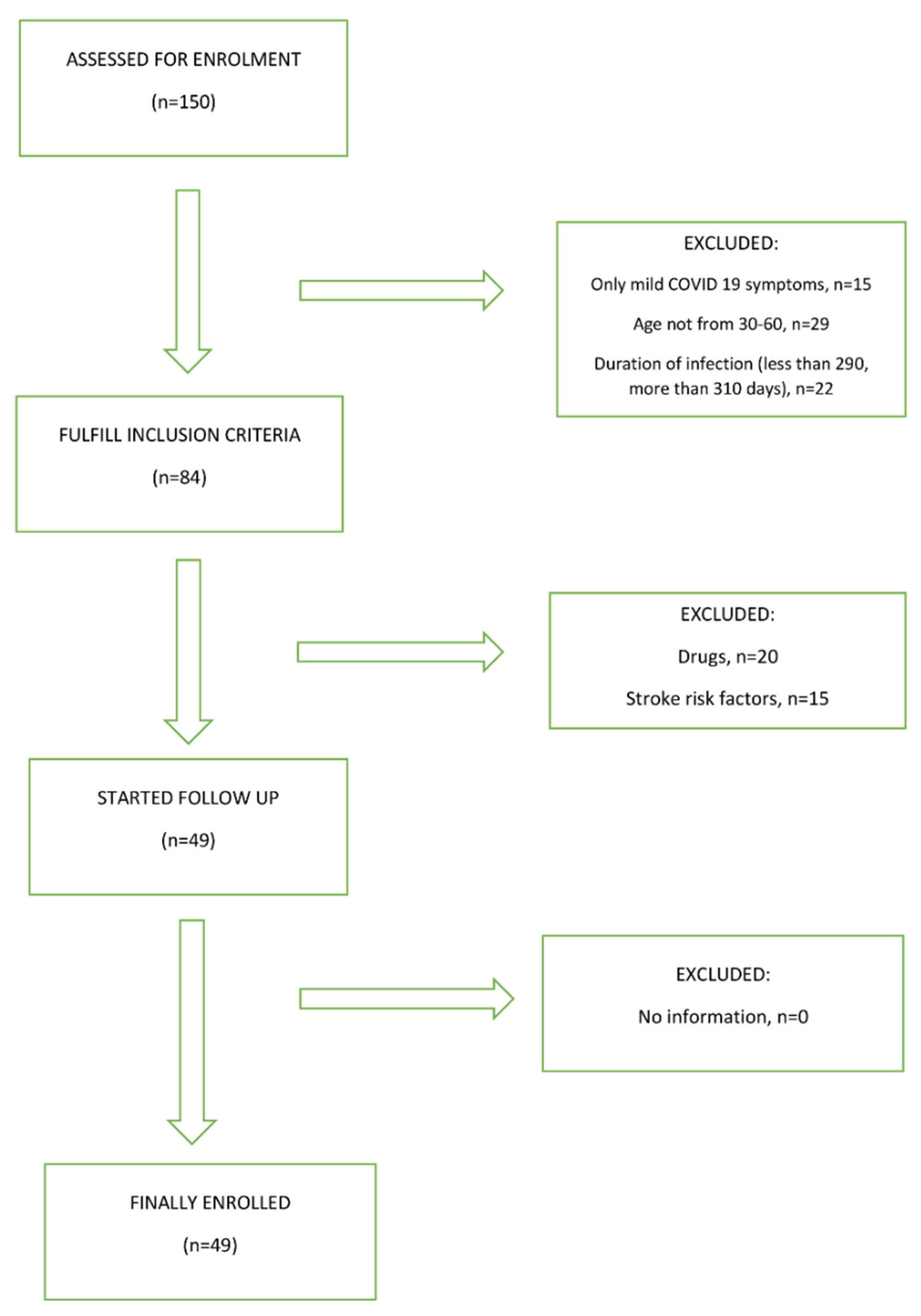
2.2. Sample Size and Cohort
2.3. Clinical Evaluation and TCCD Measurements
2.4. Statistics
3. Results
3.1. Participants
3.2. Comparison of Flow Velocities through Middle Cerebral Artery at Rest and after Breath Holding Test between Test Groups
3.3. Comparison of the Flow Rate through the MCA at Rest and after BHT in the COVID-19 Group 40 Days and 300 Days after COVID-19 Infection
3.4. Comparison of Relative Changes in the Examined Flow Rates through the MCA in Relation to the Time Elapsed since the Onset of COVID-19 Infection
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization (WHO). Coronavirus COVID-19 Dashboard. Available online: https://covid19.who.int (accessed on 8 December 2021).
- Novak, P.; Mukerji, S.S.; Alabsi, H.S.; Systrom, D.; Marciano, S.P.; Felsenstein, D.; Mullally, W.J.; Pilgrim, D.M. Multisystem Involvement in Post-Acute Sequelae of Coronavirus Disease 19. Ann. Neurol. 2022, 91, 367–379. [Google Scholar] [CrossRef] [PubMed]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef] [PubMed]
- Domènech-Montoliu, S.; Puig-Barberà, J.; Pac-Sa, M.R.; Vidal-Utrillas, P.; Latorre-Poveda, M.; Del Rio-González, A.; Ferrando-Rubert, S.; Ferrer-Abad, G.; Sánchez-Urbano, M.; Aparisi-Esteve, L.; et al. Complications Post-COVID-19 and Risk Factors among Patients after Six Months of a SARS-CoV-2 Infection: A Population-Based Prospective Cohort Study. Epidemiologia 2022, 3, 49–67. [Google Scholar] [CrossRef]
- Yuki, K.; Fujiogi, M.; Koutsogiannaki, S. COVID-19 pathophysiology: A review. Clin. Immunol. 2020, 215, 108427. [Google Scholar] [CrossRef]
- Gross, L.Z.F.; Sacerdoti, M.; Piiper, A.; Zeuzem, S.; Leroux, A.E.; Biondi, R.M. ACE2, the Receptor that Enables Infection by SARS-CoV-2: Biochemistry, Structure, Allostery and Evaluation of the Potential Development of ACE2 Modulators. ChemMedChem 2020, 15, 1682–1690. [Google Scholar] [CrossRef]
- Devaux, C.A.; Rolain, J.M.; Raoult, D. ACE2 receptor polymorphism: Susceptibility to SARS-CoV-2, hypertension, multi-organ failure, and COVID-19 disease outcome. J. Microbiol. Immunol. Infect. 2020, 53, 425–435. [Google Scholar] [CrossRef]
- Song, P.; Li, W.; Xie, J.; Hou, Y.; You, C. Cytokine storm induced by SARS-CoV-2. Clin. Chim. Acta 2020, 509, 280–287. [Google Scholar] [CrossRef]
- Olbei, M.; Hautefort, I.; Modos, D. SARS-CoV-2 Causes a Different Cytokine Response Compared to Other Cytokine Storm-Causing Respiratory Viruses in Severely Ill Patients. Front. Immunol. 2021, 12, 629193. [Google Scholar] [CrossRef]
- Buszko, M.; Nita-Lazar, A.; Park, J.-H.; Schwartzberg, P.L.; Verthelyi, D.; Young, H.A.; Rosenberg, A.S. Lessons learned: New insights on the role of cytokines in COVID-19. Nat. Immunol. 2021, 22, 404–411. [Google Scholar] [CrossRef]
- Shrestha, G.S.; Khanal, S.; Sharma, S.; Nepal, G. COVID-19: Current Understanding of Pathophysiology. J. Nepal Health Res. Counc. 2020, 18, 351–359. [Google Scholar] [CrossRef]
- Iadecola, C.; Anrather, J.; Kamel, H. Effects of COVID-19 on the Nervous System. Cell 2020, 183, 16–27.e1. [Google Scholar] [CrossRef] [PubMed]
- Levi, M.; Thachil, J.; Iba, T.; Levy, J.H. Coagulation abnormalities and thrombosis in patients with COVID-19. Lancet Haematol. 2020, 7, e438–e440. [Google Scholar] [CrossRef]
- Marcic, L.; Marcic, M.; Kojundzic, S.L.; Marcic, B.; Capkun, V.; Vukojevic, K. Personalized Approach to Patient with MRI Brain Changes after SARS-CoV-2 Infection. J. Pers. Med. 2021, 11, 442. [Google Scholar] [CrossRef]
- Mehta, O.P.; Bhandari, P.; Raut, A.; Kacimi, S.E.O.; Huy, N.T. Coronavirus Disease (COVID-19): Comprehensive Review of Clinical Presentation. Front. Public Health 2021, 8, 582932. [Google Scholar] [CrossRef] [PubMed]
- Whittaker, A.; Anson, M.; Harky, A. Neurological Manifestations of COVID-19: A systematic review and current update. Acta Neurol. Scand. 2020, 142, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Guerrero, J.I.; Barragán, L.A.; Martínez, J.D.; Montoya, J.P.; Peña, A.; Sobrino, F.E.; Tovar-Spinoza, Z.; Ghotme, K.A. Central and peripheral nervous system involvement by COVID-19: A systematic review of the pathophysiology, clinical manifestations, neuropathology, neuroimaging, electrophysiology, and cerebrospinal fluid findings. BMC Infect. Dis. 2021, 21, 515. [Google Scholar] [CrossRef]
- Andalib, S.; Biller, J.; Di Napoli, M.; Moghimi, N.; McCullough, L.D.; Rubinos, C.A.; Nobleza, C.O.; Azarpazhooh, M.R.; Catanese, L.; Elicer, I.; et al. Peripheral Nervous System Manifestations Associated with COVID-19. Curr. Neurol. Neurosci. Rep. 2021, 21, 9. [Google Scholar] [CrossRef]
- Marcic, M.; Marcic, L.; Marcic, B. SARS-CoV-2 Infection Causes Relapse of Kleine-Levin Syndrome: Case Report and Review of Literature. Neurol. Int. 2021, 13, 328–334. [Google Scholar] [CrossRef]
- Nolen, L.T.; Mukerji, S.S.; Mejia, N.I. Post-acute neurological consequences of COVID-19: An unequal burden. Nat. Med. 2022, 28, 20–23. [Google Scholar] [CrossRef]
- World Health Organization. COVID-19 Clinical Management: Living Guidance, 25 January 2021. World Health Organization. License: CC BY-NC-SA 3.0 IGO. 2021. Available online: https://apps.who.int/iris/handle/10665/338882 (accessed on 28 May 2022).
- Marcic, M.; Marcic, L.; Marcic, B.; Capkun, V.; Vukojevic, K. Cerebral Vasoreactivity Evaluated by Transcranial Color Doppler and Breath-Holding Test in Patients after SARS-CoV-2 Infection. J. Pers. Med. 2021, 11, 379. [Google Scholar] [CrossRef] [PubMed]
- Xia, H.; Lazartigues, E. Angiotensin-converting enzyme 2 in the brain: Properties and future directions. J. Neurochem. 2008, 107, 1482–1494. [Google Scholar] [CrossRef] [Green Version]
- Keyhanian, K.; Umeton, R.P.; Mohit, B.; Davoudi, V.; Hajighasemi, F.; Ghasemi, M. SARS-CoV-2 and nervous system: From pathogenesis to clinical manifestation. J. Neuroimmunol. 2020, 350, 577436. [Google Scholar] [CrossRef]
- Willie, C.; Colino, F.; Bailey, D.; Tzeng, Y.; Binsted, G.; Jones, L.; Haykowsky, M.; Bellapart, J.; Ogoh, S.; Smith, K.; et al. Utility of transcranial Doppler ultrasound for the integrative assessment of cerebrovascular function. J. Neurosci. Methods 2011, 196, 221–237. [Google Scholar] [CrossRef]
- Castro, P.; Azevedo, E.; Sorond, F. Cerebral Autoregulation in Stroke. Curr. Atheroscler. Rep. 2018, 20, 37. [Google Scholar] [CrossRef]
- Carfì, A.; Bernabei, R.; Landi, F. Persistent Symptoms in Patients After Acute COVID-19. JAMA 2020, 324, 603–605. [Google Scholar] [CrossRef]
- Nuzzo, D.; Vasto, S.; Scalisi, L.; Cottone, S.; Cambula, G.; Rizzo, M.; Giacomazza, D.; Picone, P. Post-Acute COVID-19 Neurological Syndrome: A New Medical Challenge. J. Clin. Med. 2021, 10, 1947. [Google Scholar] [CrossRef]
- Carvalho-Schneider, C.; Laurent, E.; Lemaignen, A.; Beaufils, E.; Bourbao-Tournois, C.; Laribi, S.; Flament, T.; Ferreira-Maldent, N.; Bruyère, F.; Stefic, K.; et al. Follow-up of adults with noncritical COVID-19 two months after symptom onset. Clin. Microbiol. Infect. 2020, 27, 258–263. [Google Scholar] [CrossRef]
- Garrigues, E.; Janvier, P.; Kherabi, Y.; Le Bot, A.; Hamon, A.; Gouze, H.; Doucet, L.; Berkani, S.; Oliosi, E.; Mallart, E.; et al. Post-discharge persistent symptoms and health-related quality of life after hospitalization for COVID-19. J. Infect. 2020, 81, e4–e6. [Google Scholar] [CrossRef]
- Yan, Z.; Yang, M.; Lai, C.-L. Long COVID-19 Syndrome: A Comprehensive Review of Its Effect on Various Organ Systems and Recommendation on Rehabilitation Plans. Biomedicines 2021, 9, 966. [Google Scholar] [CrossRef] [PubMed]
- Haffke, M.; Freitag, H.; Rudolf, G.; Seifert, M.; Doehner, W.; Scherbakov, N.; Hanitsch, L.; Wittke, K.; Bauer, S.; Konietschke, F.; et al. Endothelial dysfunction and altered endothelial biomarkers in patients with post-COVID-19 syndrome and chronic fatigue syndrome (ME/CFS). J. Transl. Med. 2022, 20, 138. [Google Scholar] [CrossRef] [PubMed]
- Ambrosino, P.; Calcaterra, I.; Molino, A.; Moretta, P.; Lupoli, R.; Spedicato, G.; Papa, A.; Motta, A.; Maniscalco, M.; Di Minno, M. Persistent Endothelial Dysfunction in Post-Acute COVID-19 Syndrome: A Case-Control Study. Biomedicines 2021, 9, 957. [Google Scholar] [CrossRef] [PubMed]
- Elkind, M.S.; Boehme, A.K.; Smith, C.J.; Meisel, A.; Buckwalter, M.S. Infection as a Stroke Risk Factor and Determinant of Outcome After Stroke. Stroke 2020, 51, 3156–3168. [Google Scholar] [CrossRef]
- McAlpine, L.S.; Zubair, A.S.; Maran, I.; Chojecka, P.; Lleva, P.; Jasne, A.S.; Navaratnam, D.; Matouk, C.; Schindler, J.; Sheth, K.N.; et al. Ischemic Stroke, Inflammation, and Endotheliopathy in COVID-19 Patients. Stroke 2021, 52, e233–e238. [Google Scholar] [CrossRef]
- Staszewski, J.; Skrobowska, E.; Piusińska-Macoch, R.; Brodacki, B.; Stępień, A. Cerebral and Extracerebral Vasoreactivity in Patients With Different Clinical Manifestations of Cerebral Small-Vessel Disease: Data From the Significance of Hemodynamic and Hemostatic Factors in the Course of Different Manifestations of Cerebral Small-Vessel Disease Study. J. Ultrasound Med. 2019, 38, 975–987. [Google Scholar]
- Fotuhi, M.; Mian, A.; Meysami, S.; Raji, C.A. Neurobiology of COVID-19. J. Alzheimers Dis. 2020, 76, 3–19. [Google Scholar] [CrossRef] [PubMed]
- de Sire, A.; Demeco, A.; Marotta, N.; Spanò, R.; Curci, C.; Farì, G.; Fortunato, F.; Iona, T.; Lippi, L.; Paolucci, T.; et al. Neuromuscular Impairment of Knee Stabilizer Muscles in a COVID-19 Cluster of Female Volleyball Players: Which Role for Rehabilitation in the Post-COVID-19 Return-to-Play? Appl. Sci. 2022, 12, 557. [Google Scholar] [CrossRef]
- Callen, A.L.; Tanabe, J.; Thaker, A.A.; Pollard, R.; Sauer, B.; Jones, W.; Pattee, J.; Steach, B.; Timpone, V. Evaluation of Cerebrovascular Reactivity and Vessel-Wall Imaging in Patients With Prior COVID-19: A Prospective Case-Control MRI Study. Am. J. Roentgenol. 2022; Epub ahead of print. [Google Scholar] [CrossRef]


{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Age from 30 to 60 years | Less than 30 and more than 60 years |
| Mild form of COVID-19 disease | Severe or critical COVID-19 disease |
| Neurological symptoms: anosmia, dysgeusia, vertigo, headache, vertigo, fatigue | Severe neurological symptoms: acute cerebrovascular disease (ischemic or hemorrhagic stroke, subarachnoid hemorrhage), encephalopathy, encephalitis, meningitis, polyneuropathy, seizures, disturbance of consciousness |
| COVID-19 disease: from 290 to 310 days from infection start | COVID-19 disease: less than 290 or more than 310 days from infection start |
| Supportive therapy only | Antibiotics, corticosteroids, or oxygen use for COVID-19 infection |
| COVID-19 disease confirmation: positive real-time reverse PCR test, positive nasal/pharyngeal swabs test | Uncontrolled diabetes mellitus or arterial hypertension, cerebrovascular disease, hematologic disease, atrial fibrillation, chronic heart disease, cancer |
| Severe alcohol consumption (more than 10 drinks per week) | |
| Stenosis of extracranial vertebral or carotid artery >20% or occlusive disease of intracranial cerebral arteries | |
| Using anticoagulant therapy, vasodilatory drugs, hormone replacement therapy, β-blocking agents, calcium channel blockers |
| COVID-19 Group (N = 49) | Control Group (N = 50) | ||
|---|---|---|---|
| Gender | M | 25 (51%) * | 25 (50%) |
| F | 24 (49%) * | 25 (50%) | |
| Diabetes melitus | 5 (10%) | 4 (8%) | |
| Arterial hypertension | 7 (14%) | 8 (16%) | |
| Hyperlipidemia | 4 (8%) | 5 (10%) | |
| Alcohol consumption | 0 (0%) | 0 (0%) | |
| Smoking | 3 (6%) | 3 (6%) | |
| Age (years) | 47 ± 6 ** | 48 ± 5 ** | |
| BMI (kg/m2) | 26 ± 3.3 ** | 26 ± 3.2 ** | |
| SBP(mmHg) | 125 ± 12 ** | 124 ± 10 ** | |
| DBP (mmHg) | 77 ± 9.6 ** | 76 ± 9.1 ** | |
| COVID-19 (N = 49) | Control (N = 50) | |
|---|---|---|
| Total vaccination (N) | 23 (47%) | 36 (72%) |
| BioNTech | 15 (65%) | 20 (55%) |
| Johnson & Johnson | 5 (22%) | 9 (25%) |
| Moderna | 3 (13%) | 7 (20%) |
| Neurological Symptoms | N (49) |
|---|---|
| Anosmia | 1 (2%) |
| Dysgeusia | 2 (4%) |
| Vertigo | 5 (10%) |
| Headache | 7 (14%) |
| Fatigue | 3 (6%) |
| Cognitive symptoms | 2 (4%) |
| Sleep disorders | 1 (2%) |
| Myalgia | 0 (0%) |
| Quantitative Laboratory Variables 300 Days after COVID-19 Infection | |||
|---|---|---|---|
| Control Group | COVID-19 | p | |
| Body temperature (°C) | 36.5 (36–37.1) | 36.5 (36–36.9) | 0.791 * |
| Hgb g/L | 153 (137–165) | 149.3 (131–162) | 0.249 * |
| Hct L/L | 0.525 (0.490–0.590) | 0.499(0.447–0.571) | 0.067 * |
| Leukocytes ×109/L | 6.5 (4.8–8.2) | 6.4 (4.9–8.1) | 0.956 * |
| Platelets ×109/L | 411 (389–426) | 409 (386–425) | 0.121 * |
| Erythrocytes ×1012/L | 5.2 (4.9–5.9) | 4.9 (4.6–5.3) | 0.061 * |
| Urea mm/L | 4.9 (3.1–7.2) | 5.1 (3.8–6.9) | 0.557 * |
| Creatinine µm/L | 73.5 (54–83) | 75.5 (54–85) | 0.138 * |
| Cholesterol mm/L | 4.8 (4–5) | 4.7 (4–5) | 0.305 * |
| D-dimers ng/mL | 0.17 (0.14–0.27) | 0.19 (0.16–0.25) | 0.422 * |
| Triglycerides mm/L | 1.3 (1.1–1.6) | 1.5 (1.2–1.7) | 0.077 * |
| LDH U/L | 159 (136–171) | 157 (138–170) | 0.097 * |
| Subject Groups | p * | ||
|---|---|---|---|
| COVID-19 | Controls | ||
| At rest | |||
| PSV (cm/s) | 106 ± 12.5 (101–112) | 121 ± 5.8 (117–122) | <0.001 |
| EDV (cm/s) | 52.1 ± 4.7 (50–55) | 56.4 ± 5.3 (53–59) | <0.001 |
| MV (cm/s) | 72.2 ± 7.1 (68–76) | 81.4 ± 7.4 (77–84) | <0.001 |
| RI | 0.52 ± 0.03 (0.50–0.53) | 0.55 ± 0.03 (0.54–0.57) | <0.001 |
| PI | 0.74 ± 0.06 (0.72–0.77) | 0.78 ± 0.04 (0.76–0.79) | <0.001 |
| After BHT | |||
| PSV (cm/s) | 122 ± 11.1 (116–127) | 162 ± 7.4 (157–164) | <0.001 |
| EDV (cm/s) | 69.1 ± 3.1 (66–71) | 86 ± 5.6 (81–89) | <0.001 |
| MV (cm/s) | 94.3 ± 8.1 (90–98) | 112.1 ± 4 (107–116) | <0.001 |
| RI | 0.53 ± 0.04 (0.51–0.53) | 0.50 ± 0.01 (0.49.-0.52) | <0.001 |
| PI | 0.78 ± 0.07 (0.74–0.81) | 0.75 ± 0.04 (0.73–0.77) | <0.001 |
| Subjects Groups | p * | ||
|---|---|---|---|
| COVID-19 | Controls | ||
| Relative change of velocities parameters after BHT compared to values at resting period (%) | |||
| ∆PSV (%) | 16 (11–18) | 41 (37–45) | <0.001 |
| ∆EDV (%) | 17 (15–24) | 32 (29–37) | <0.001 |
| ∆MV (%) | 22 (20–26) | 33 (28–39) | <0.001 |
| ∆RI (%) | 1.4 (−0.6 to 2.1) | −5 (−12 to −2) | <0.001 |
| ∆PI (%) | 3.3 (1.9–3.7) | −4 (−6 to −1.4) | <0.001 |
| BHI | 0.43 (0.35–0.54) | 0.97 (0.88–1.07) | <0.001 |
| Flow Rates during Resting Period in a Group of Subjects after COVID-19 Infection | ||||
|---|---|---|---|---|
| 40 Days | 300 Days | Difference | p * | |
| PSV (cm/s) | 109 ± 12 (103–115) | 106 ± 12.5 (101–112) | −2.83 ± 2.4 (−2 to 0.35) | 0.156 |
| EDV (cm/s) | 53 ± 4 (51–55) | 52 ± 4.7 (51–54) | −1.2 ± 1.1 (−1.2 to −0.69) | 0.021 |
| MV (cm/s) | 72 ± 7.4 (68–75) | 72 ± 7.1 (70–76) | −0.5 ± 2.9 (−2.9 to −0.11) | 0.066 |
| RI | 0.52 ± 0.027 (0.51–0.54) | 0.52 ± 0.03 (0.50–0.53) | −0.01 ± 0.02 (−0.02 to 0.0008) | 0.170 |
| PI | 0.75 ± 0.07 (0.73–0.79) | 0.74 ± 0.06 (0.75–0.82) | −09 ± 0.02 (−1.02–−0.01) | 0.128 |
| Flow Rates in MCA after BHT | ||||
|---|---|---|---|---|
| 40 Days | 300 Days | Difference | p * | |
| PSV (cm/s) | 124 ± 10 (120–129) | 122 ± 11.1 (121–131) | −1.4 ± 2.7 (−2.7 to −0.11) | 0.065 |
| EDV (cm/s) | 70 ± 3.5 (68–72) | 69.1 ± 3.1 (66–71) | −0.35 ± 1.1 (−0.58–0.5) | 0.837 |
| MV (cm/s) | 94.1 ± 8.8 (90–98) | 94.3 ± 8.1 (91–97) | 0.2 ± 1.4 (−0–33–2.2) | 0–118 |
| RI | 0.53 ± 0.02 (0.52–0.54) | 0.53 ± 0.04 (0.52–0.55) | −0.006 ± 0.01 (−0.1–−0.0007) | 0.028 |
| PI | 0.78 ± 0.08 (0.75–0.82) | 0.78 ± 0.07 (0.76–0.82) | −0.008 ± 0.03 (−0.02–0.008) | 0.286 |
| Subjects after COVID-19 Infection | |||
|---|---|---|---|
| Relative Change in Value after BHT and Value at Rest (%) | 40 Days | 300 Days | p * |
| PSV | 15(11–20) | 16 (11–18) | 0.211 |
| EDV | 18 (16–24) | 17 (14–22) | 0.037 |
| MV | 25 (21–28) | 22 (20–26) | 0.015 |
| RI | 1.5 (−0.5–1.9) | 1.4 (−0.6–2.1) | 0.691 |
| PI | 3.1 (1.7–3.5) | 3.3 (1.9–3.7) | 0.199 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marcic, M.; Marcic, L.; Lovric Kojundzic, S.; Marinovic Guic, M.; Marcic, B.; Caljkusic, K. Chronic Endothelial Dysfunction after COVID-19 Infection Shown by Transcranial Color-Coded Doppler: A Cross-Sectional Study. Biomedicines 2022, 10, 2550. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10102550
Marcic M, Marcic L, Lovric Kojundzic S, Marinovic Guic M, Marcic B, Caljkusic K. Chronic Endothelial Dysfunction after COVID-19 Infection Shown by Transcranial Color-Coded Doppler: A Cross-Sectional Study. Biomedicines. 2022; 10(10):2550. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10102550
Chicago/Turabian StyleMarcic, Marino, Ljiljana Marcic, Sanja Lovric Kojundzic, Maja Marinovic Guic, Barbara Marcic, and Kresimir Caljkusic. 2022. "Chronic Endothelial Dysfunction after COVID-19 Infection Shown by Transcranial Color-Coded Doppler: A Cross-Sectional Study" Biomedicines 10, no. 10: 2550. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10102550