
Post-Bariatric Hypoglycemia Is Associated with Endothelial Dysfunction and Increased Oxidative Stress

 ,
,  , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Continuous Glucose Monitoring (CGM)
2.3. Laboratory Parameters
2.4. Brachial Artery FMD
2.5. Statistical Analysis
2.6. Sample Size Calculation
3. Results
3.1. Characteristics of the Study Population
3.2. CGM Data
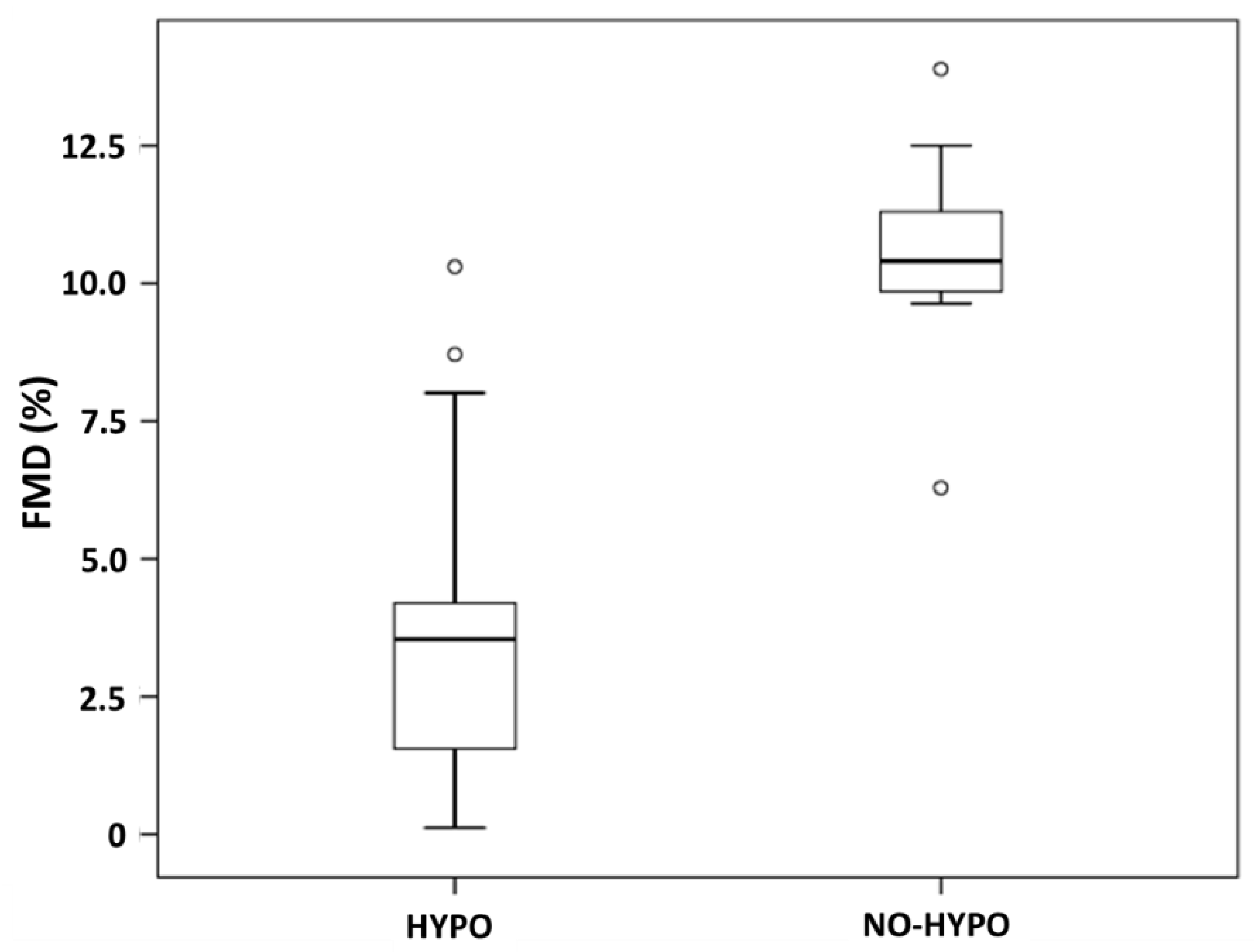
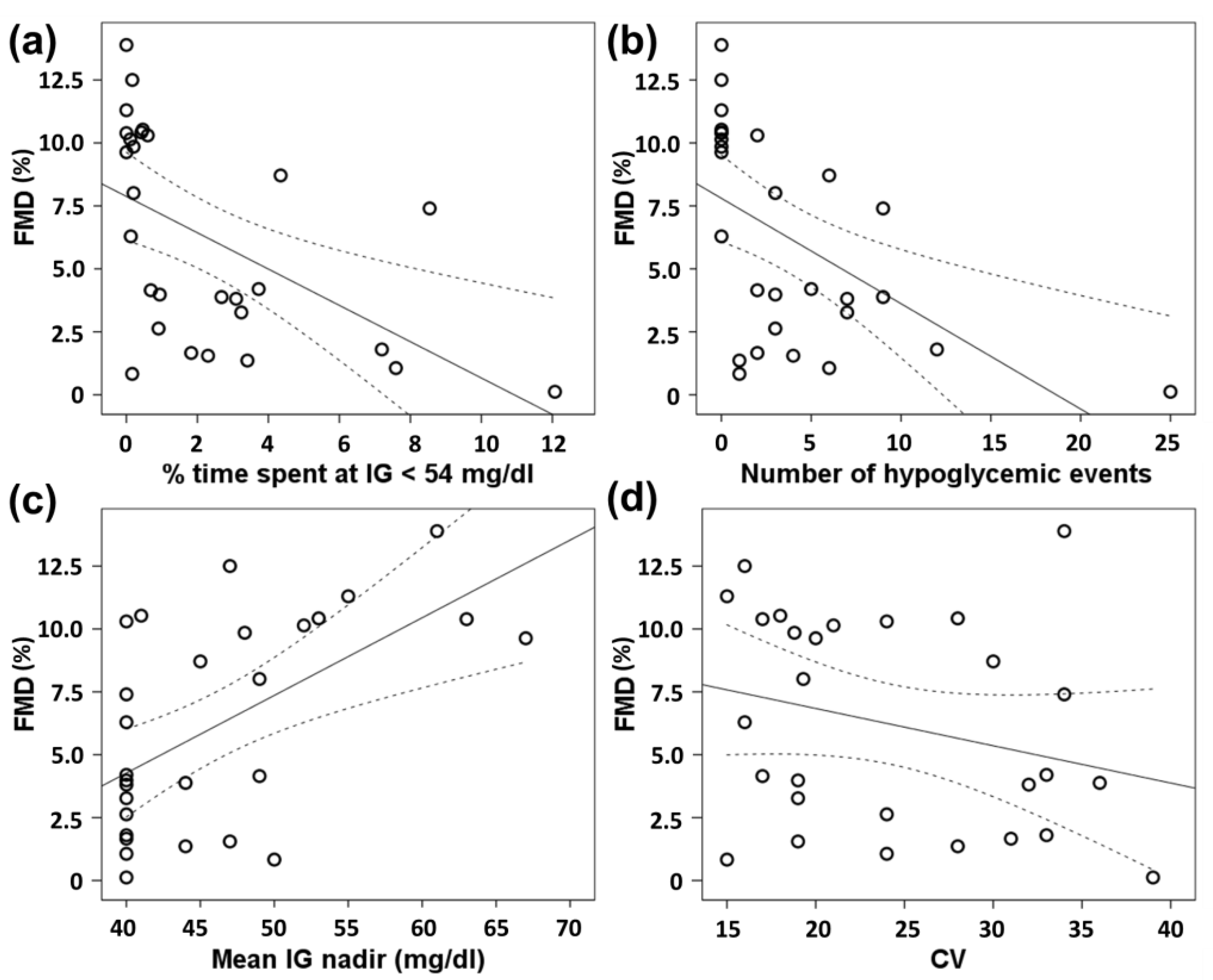
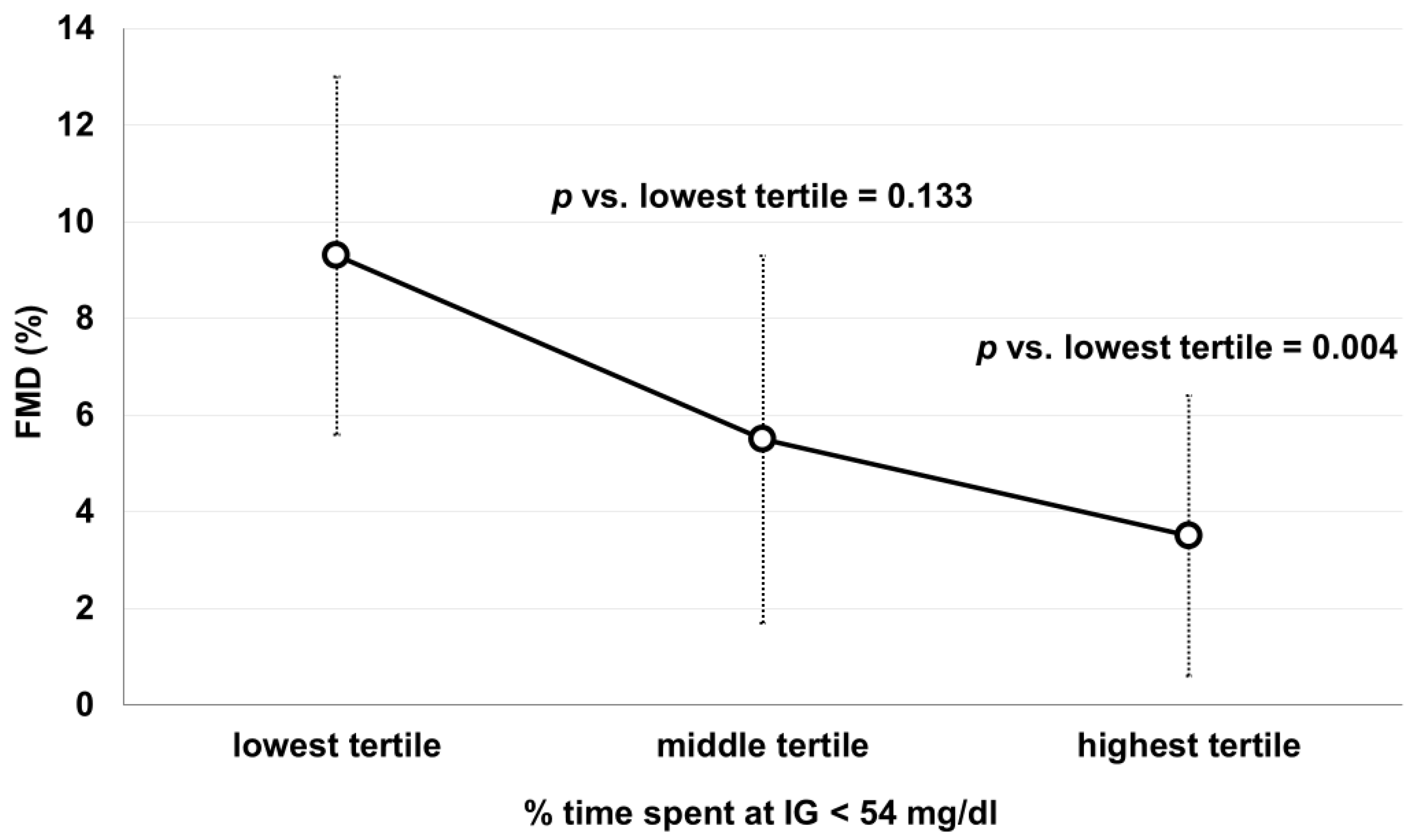
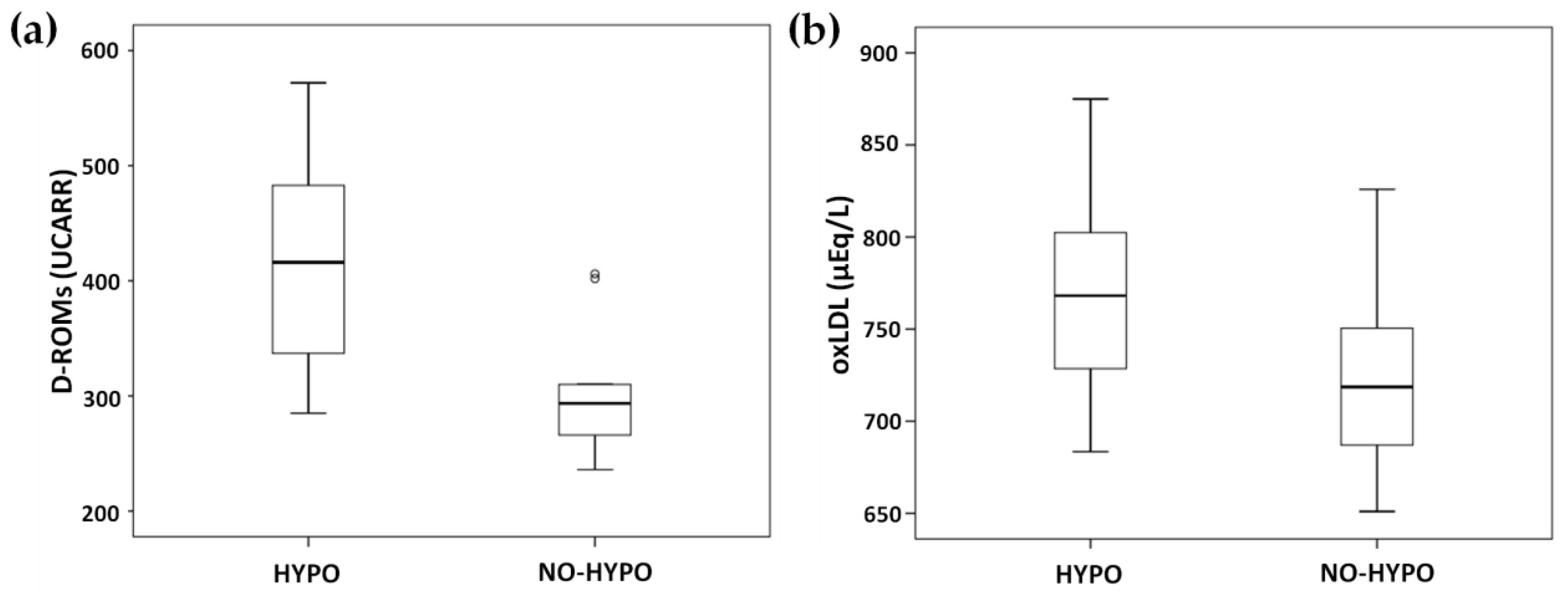
3.3. Vascular Reactivity and Oxidation Markers
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brix, J.M.; Kopp, H.-P.; Höllerl, F.; Schernthaner, G.H.; Ludvik, B.; Schernthaner, G. Frequency of Hypoglycaemia after Different Bariatric Surgical Procedures. Obes. Facts 2019, 12, 397–406. [Google Scholar] [CrossRef] [PubMed]
- Lupoli, R.; Lembo, E.; Ciciola, P.; Schiavo, L.; Pilone, V.; Capaldo, B. Continuous glucose monitoring in subjects undergoing bariatric surgery: Diurnal and nocturnal glycemic patterns. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 1954–1960. [Google Scholar] [CrossRef]
- Salehi, M.; Vella, A.; McLaughlin, T.; Patti, M.-E. Hypoglycemia After Gastric Bypass Surgery: Current Concepts and Controversies. J. Clin. Endocrinol. Metab. 2018, 103, 2815–2826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wei, W.; Zhao, S.; Fu, S.-L.; Yi, L.; Mao, H.; Tan, Q.; Xu, P.; Yang, G.-L. The Association of Hypoglycemia Assessed by Continuous Glucose Monitoring With Cardiovascular Outcomes and Mortality in Patients With Type 2 Diabetes. Front. Endocrinol. 2019, 10, 536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, A.K.; Warren, B.; Lee, C.J.; McEvoy, J.W.; Matsushita, K.; Huang, E.S.; Sharrett, A.R.; Coresh, J.; Selvin, E. The Association of Severe Hypoglycemia With Incident Cardiovascular Events and Mortality in Adults With Type 2 Diabetes. Diabetes Care 2017, 41, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Joy, N.G.; Tate, D.B.; Younk, L.M.; Davis, S.N. Effects of Acute and Antecedent Hypoglycemia on Endothelial Function and Markers of Atherothrombotic Balance in Healthy Humans. Diabetes 2015, 64, 2571–2580. [Google Scholar] [CrossRef] [Green Version]
- Danne, T.; Nimri, R.; Battelino, T.; Bergenstal, R.M.; Close, K.L.; DeVries, J.H.; Garg, S.; Heinemann, L.; Hirsch, I.; Amiel, S.A.; et al. International Consensus on Use of Continuous Glucose Monitoring. Diabetes Care 2017, 40, 1631–1640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Annunziata, G.; Ciampaglia, R.; Maisto, M.; D’Avino, M.; Caruso, D.; Tenore, C.G.; Novellino, E. Taurisolo(R), a Grape Pomace Polyphenol Nutraceutical Reducing the Levels of Serum Biomarkers As-sociated With Atherosclerosis. Front. Cardiovasc. Med. 2021, 8, 697272. [Google Scholar] [CrossRef]
- Annunziata, G.; Maisto, M.; Schisano, C.; Ciampaglia, R.; Narciso, V.; Hassan, S.T.S.; Tenore, G.C.; Novellino, E. Effect of Grape Pomace Polyphenols With or Without Pectin on TMAO Serum Levels Assessed by LC/MS-Based Assay: A Preliminary Clinical Study on Overweight/Obese Subjects. Front. Pharmacol. 2019, 10, 575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martelli, A.; Flori, L.; Gorica, E.; Piragine, E.; Saviano, A.; Annunziata, G.; Minno, M.N.D.D.; Ciampaglia, R.; Calcaterra, I.; Maione, F.; et al. Vascular Effects of the Polyphenolic Nutraceutical Supplement Taurisolo((R)): Focus on the Protection of the Endothelial Function. Nutrients 2021, 13, 1540. [Google Scholar] [CrossRef] [PubMed]
- Cesarone, M.R.; Belcaro, G.; Carratelli, M.; Cornelli, U.; De Sanctis, M.T.; Incandela, L.; Barsotti, A.; Terranova, R.; Nicolaides, A. A simple test to monitor oxidative stress. Int. Angiol. 1999, 18, 127. [Google Scholar]
- Trotti, R.; Carratelli, M.; Barbieri, M.; Micieli, G.; Bosone, D.; Rondanelli, M.; Bo, P. Oxidative stress and a thrombophilic condition in alcoholics without severe liver disease. Haematologica 2001, 86, 85–91. [Google Scholar]
- Gerardi, G.; Usberti, M.; Martini, G.; Albertini, A.; Sugherini, L.; Pompella, A.; Di, L.D. Plasma total antioxidant capacity in hemodialyzed patients and its relationships to other biomarkers of ox-idative stress and lipid peroxidation. Clin. Chem. Lab. Med. 2002, 40, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Macri, A.; Scanarotti, C.; Bassi, A.M.; Giuffrida, S.; Sangalli, G.; Traverso, C.E.; Iester, M. Evaluation of oxidative stress levels in the conjunctival epithelium of patients with or without dry eye, and dry eye patients treated with preservative-free hyaluronic acid 0.15 % and vitamin B12 eye drops. Graefe’s Arch. Clin. Exp. Ophthalmol. 2014, 253, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Mancini, S.; Mariani, F.; Sena, P.; Benincasa, M.; Roncucci, L. Myeloperoxidase expression in human colonic mucosa is related to systemic oxidative balance in healthy subjects. Redox Rep. 2017, 22, 399–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Zwan, L.P.; Teerlink, T.; Dekker, J.D.; Henry, R.M.A.; Stehouwer, C.D.A.; Jakobs, C.; Heine, R.J.; Scheffer, P.G. Circulating oxidized LDL: Determinants and association with brachial flow-mediated dilation. J. Lipid. Res. 2009, 50, 342–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corretti, M.C.; Anderson, T.J.; Benjamin, E.J.; Celermajer, D.; Charbonneau, F.; Creager, M.A.; Deanfield, J.; Drexler, H.; Gerhard-Herman, M.; Herrington, D.; et al. Guidelines for the ultrasound assessment of endothelial-dependent flow-mediated vasodilation of the brachial artery: A report of the International Brachial Artery Reactivity Task Force. J. Am. Coll. Cardiol. 2002, 39, 257–265. [Google Scholar] [CrossRef] [Green Version]
- Joy, N.G.; Perkins, J.M.; Mikeladze, M.; Younk, L.; Tate, D.B.; Davis, S.N. Comparative effects of acute hypoglycemia and hyperglycemia on pro-atherothrombotic biomarkers and endothelial function in non-diabetic humans. J. Diabetes Complicat. 2016, 30, 1275–1281. [Google Scholar] [CrossRef] [Green Version]
- Gimenez, M.; Gilabert, R.; Monteagudo, J.; Alonso, A.; Casamitjana, R.; Paré, C.; Conget, L. Repeated episodes of hypoglycemia as a potential aggravating factor for preclinical atherosclerosis in subjects with type 1 diabetes. Diabetes Care 2011, 34, 198–203. [Google Scholar] [CrossRef] [Green Version]
- Lee, R.; Margaritis, M.; Channon, K.; Antoniades, C. Evaluating Oxidative Stress in Human Cardiovascular Disease: Methodological Aspects and Considerations. Curr. Med. Chem. 2012, 19, 2504–2520. [Google Scholar] [CrossRef] [Green Version]
- Kotani, K.; Sakane, N. C-Reactive Protein and Reactive Oxygen Metabolites in Subjects with Metabolic Syndrome. J. Int. Med Res. 2012, 40, 1074–1081. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schottker, B.; Brenner, H.; Jansen, E.H.J.M.; Gardiner, J.; Peasey, A.; Kubínová, R.; Pająk, A.; Topor-Madry, R.; Tamosiunas, A.; Saum, K.-U.; et al. Evidence for the free radical/oxidative stress theory of ageing from the CHANCES consortium: A meta-analysis of individual participant data. BMC Med. 2015, 13, 300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vassalle, C. An Easy and Reliable Automated Method to Estimate Oxidative Stress in the Clinical Setting. In Advanced Protocols in Oxidative Stress; Humana press: Totowa, TJ, USA, 2008; Volume 477, pp. 31–39. [Google Scholar]
- Masaki, N.; Sato, A.; Horii, S.; Kimura, T.; Toya, T.; Yasuda, R.; Namba, T.; Yada, H.; Kawamura, A.; Adachi, T. Usefulness of the d-ROMs test for prediction of cardiovascular events. Int. J. Cardiol. 2016, 222, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Xuan, Y.; Bobak, M.; Anusruti, A.; Jansen, E.H.J.M.; Pająk, A.; Tamosiunas, A.; Saum, K.-U.; Holleczek, B.; Gao, X.; Brenner, H.; et al. Association of serum markers of oxidative stress with myocardial infarction and stroke: Pooled results from four large European cohort studies. Eur. J. Epidemiol. 2018, 34, 471–481. [Google Scholar] [CrossRef] [PubMed]
- Malekmohammad, K.; Sewell, R.D.E.; Rafieian-Kopaei, M. Antioxidants and Atherosclerosis: Mechanistic Aspects. Biomolecules 2019, 9, 301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitra, S.; Deshmukh, A.; Sachdeva, R.; Lu, J.; Mehta, J.L. Oxidized Low-Density Lipoprotein and Atherosclerosis Implications in Antioxidant Therapy. Am. J. Med. Sci. 2011, 342, 135–142. [Google Scholar] [CrossRef]
- Ehara, S.; Ueda, M.; Naruko, T.; Haze, K.; Itoh, A.; Otsuka, M.; Komatsu, R.; Matsuo, T.; Itabe, H.; Takano, T.; et al. Elevated levels of oxidized low density lipoprotein show a positive relationship with the severity of acute coronary syndromes. Circulation 2001, 103, 1955–1960. [Google Scholar] [CrossRef] [PubMed]
- Colasanti, M.; Suzuki, H. The dual personality of NO. Trends Pharmacol. Sci. 2000, 21, 249–252. [Google Scholar] [CrossRef]
- Stancu, C.S.; Toma, L.; Sima, A.V. Dual role of lipoproteins in endothelial cell dysfunction in atherosclerosis. Cell Tissue Res. 2012, 349, 433–446. [Google Scholar] [CrossRef] [PubMed]
- Gliozzi, M.; Scicchitano, M.; Bosco, F.; Musolino, V.; Carresi, C.; Scarano, F.; Maiuolo, J.; Nucera, S.; Maretta, A.; Paone, S.; et al. Modulation of Nitric Oxide Synthases by Oxidized LDLs: Role in Vascular Inflammation and Atherosclerosis Development. Int. J. Mol. Sci. 2019, 20, 3294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dagher, Z.; Ruderman, N.; Tornheim, K.; Ido, Y. Acute regulation of fatty acid oxidation and amp-activated protein kinase in human umbilical vein endothelial cells. Circ. Res. 2001, 88, 1276–1282. [Google Scholar] [CrossRef]
- Cardoso, S.; Santos, R.X.; Correia, S.C.; Carvalho, C.; Santos, M.S.; Baldeiras, I.; Oliveira, C.R.; Moreira, P.I. Insulin-induced recurrent hypoglycemia exacerbates diabetic brain mitochondrial dysfunction and oxidative imbalance. Neurobiol. Dis. 2013, 49, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Ceriello, A.; Novials, A.; Ortega, E.; Canivell, S.; La Sala, L.; Pujadas, G.; Bucciarelli, L.; Rondinelli, M.; Genovese, S. Vitamin C Further Improves the Protective Effect of Glucagon-Like Peptide-1 on Acute Hypoglycemia-Induced Oxidative Stress, Inflammation, and Endothelial Dysfunction in Type 1 Diabetes. Diabetes Care 2013, 36, 4104–4108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nosso, G.; Lupoli, R.; Saldalamacchia, G.; Griffo, E.; Cotugno, M.; Costabile, G.; Riccardi, G.; Capaldo, B. Diabetes remission after bariatric surgery is characterized by high glycemic variability and high oxidative stress. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 949–955. [Google Scholar] [CrossRef] [PubMed]
- Ilesanmi, I.; Tharakan, G.; Alexiadou, K.; Behary, P.; Alessimii, H.; Bovill-Taylor, C.; Kenkre, J.; Choudhury, S.; Doyle, C.; Purkayastha, S.; et al. Roux-en-Y Gastric Bypass Increases Glycemic Variability and Time in Hypoglycemia in Patients With Obesity and Prediabetes or Type 2 Diabetes: A Prospective Cohort Study. Diabetes Care 2021, 44, 614–617. [Google Scholar] [CrossRef] [PubMed]
- Peña, A.S.; Couper, J.J.; Harrington, J.; Gent, R.; Fairchild, J.; Tham, E.; Baghurst, P. Hypoglycemia, but Not Glucose Variability, Relates to Vascular Function in Children with Type 1 Diabetes. Diabetes Technol. Ther. 2012, 14, 457–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lupoli, R.; Di Minno, M.N.D.; Guidone, C.; Cefalo, C.; Capaldo, B.; Riccardi, G.; Mingrone, G. Effects of bariatric surgery on markers of subclinical atherosclerosis and endothelial function: A meta-analysis of literature studies. Int. J. Obes. 2016, 40, 395–402. [Google Scholar] [CrossRef]
- Metere, A.; Graves, C.E.; Pietraforte, D.; Casella, G. The Effect of Sleeve Gastrectomy on Oxidative Stress in Obesity. Biomedicines 2020, 8, 168. [Google Scholar] [CrossRef] [PubMed]
- Bouchard, P.; Al-Masrouri, S.; Demyttenaere, S.; Court, O.; Andalib, A. Long-term Impact of Bariatric Surgery on Major Adverse Cardiovascular Events in Patients with Obesity, Diabetes and Hypertension: A Population-level Study. Obes. Surg. 2022, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Aminian, A.; Al-Kurd, A.; Wilson, R.; Bena, J.; Fayazzadeh, H.; Singh, T.; Albaugh, V.L.; Shariff, F.U.; Rodriguez, N.A.; Jin, J.; et al. Association of Bariatric Surgery With Major Adverse Liver and Cardiovascular Outcomes in Patients With Biopsy-Proven Nonalcoholic Steatohepatitis. JAMA 2021, 326, 2031. [Google Scholar] [CrossRef] [PubMed]
- Lupoli, R.; Lembo, E.; Rainone, C.; Schiavo, L.; Iannelli, A.; Di Minno, M.N.; Capaldo, B. Rate of post-bariatric hypoglycemia using continuous glucose monitoring: A meta-analysis of literature studies. Nutr. Metab. Cardiovasc. Dis. 2022, 32, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Ras, R.T.; Streppel, M.T.; Draijer, R.; Zock, P.L. Flow-mediated dilation and cardiovascular risk prediction: A systematic review with meta-analysis. Int. J. Cardiol. 2013, 168, 344–351. [Google Scholar] [CrossRef] [PubMed]
- Inaba, Y.; Chen, J.A.; R, S. Bergmann, Prediction of future cardiovascular outcomes by flow-mediated vasodilatation of brachial artery: A meta-analysis. Int. J. Cardiovasc. Imaging 2010, 26, 631–640. [Google Scholar] [CrossRef]
- Green, D.J.; Jones, H.; Thijssen, D.; Cable, N.T.; Atkinson, G. Flow-mediated dilation and cardiovascular event prediction: Does nitric oxide matter? Hypertension 2011, 57, 363–369. [Google Scholar] [CrossRef] [Green Version]
- Sheehan, A.; Patti, M.E. Hypoglycemia After Upper Gastrointestinal Surgery: Clinical Approach to Assessment, Diagnosis, and Treatment. Diabetes Metab. Syndr. Obes. 2020, 13, 4469–4482. [Google Scholar] [CrossRef] [PubMed]
- Lembo, E.; Lupoli, R.; Ciciola, P.; Creanza, A.; Silvestri, E.; Saldalamacchia, G.; Capaldo, B. Implementation of Low Glycemic Index Diet Together with Cornstarch in Post-Gastric Bypass Hypoglycemia: Two Case Reports. Nutrients 2018, 10, 670. [Google Scholar]
- Nannipieri, M.; Belligoli, A.; Guarino, D.; Busetto, L.; Moriconi, D.; Fabris, R.; Mari, A.; Baldi, S.; Anselmino, M.; Foletto, M.; et al. Risk Factors for Spontaneously Self-Reported Postprandial Hypoglycemia After Bariatric Surgery. J. Clin. Endocrinol. Metab. 2016, 101, 3600–3607. [Google Scholar] [CrossRef]
- Veglia, F.; Amato, M.; Giovannardi, M.; Ravani, A.; Tedesco, C.C.; Frigerio, B.; Sansaro, D.; Tremoli, E.; Baldassarre, D. Potentially Spurious Correlations Between Arterial Size, Flow-Mediated Dilation, and Shear Rate. Hypertension 2014, 64, 1328–1333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phadnis, M.A. Sample size calculation for small sample single-arm trials for time-to-event data: Logrank test with normal approximation or test statistic based on exact chi-square distribution? Contemp. Clin. Trials Commun. 2019, 15, 100360. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total n = 28 | HYPO n = 18 | NO-HYPO n = 10 | p Value HYPO vs. NO-HYPO | |
|---|---|---|---|---|
| Male gender—n (%) | 5 (17.9) | 3 (16.7) | 2 (20) | 1.000 |
| Age (years) | 41 ± 11 | 40 ± 12 | 41 ± 10 | 0.832 |
| Current BMI (Kg/m2) | 27 ± 4 | 27 ± 4 | 26 ± 3 | 0.296 |
| Preoperative BMI (Kg/m2) | 44 ± 7 | 45 ± 7 | 43 ± 6 | 0.377 |
| TBWL (%) | 39 ± 6 | 39 ± 5 | 39 ± 8 | 0.982 |
| EWL (%) | 79 ± 11 | 78 ± 12 | 83 ± 10 | 0.317 |
| RYGB—n (%) | 12 (42.9) | 9 (50) | 3 (30) | 0.434 |
| Fasting blood glucose (mg/dL) | 74 ± 8 | 73 ± 9 | 75 ± 6 | 0.387 |
| Smoking habit n (%) | 10 (35.7) | 7 (38.9) | 3 (30) | 0.703 |
| Dyslipidemia n—(%) | 2 (7.1) | 0 (0) | 2 (20) | 0.119 |
| Hypertension n—(%) | 4 (14.3) | 1 (5.6) | 3 (30) | 0.116 |
| Obesity n—(%) | 5 (17.9) | 4 (22.2) | 1 (10) | 0.626 |
| ≥1 vascular risk factor—n (%) | 18 (64.3) | 11 (61.1) | 7 (70) | 0.703 |
| HYPO n = 18 | NO-HYPO n = 10 | p Value HYPO vs. NO-HYPO | |
|---|---|---|---|
| Mean IG (mg/dL) | 90 ± 8 | 104 ± 14 | 0.009 * |
| Mean IG peak (mg/dL) | 195 ± 41 | 203 ± 58 | 0.832 * |
| Mean IG nadir (mg/dL) | 43 ± 4 | 53 ± 9 | 0.001 * |
| CV (%) | 26 ± 7 | 20 ± 6 | 0.031 |
| SD (mg/dL) | 24.0 ± 6.9 | 21.9 ± 9.5 | 0.506 |
| MAGE (mg/dL) | 69.8 ± 29.7 | 54.2 ± 15.4 | 0.155 |
| % time spent at IG < 54 mg/dL | 3.5 ± 3.3 | 0.15 ± 0.17 | <0.001 |
| % time spent at IG 54–70 mg/dL | 16.0 ± 10.1 | 3.2 ± 3.5 | <0.001 |
| % time spent at IG 71–130 mg/dL | 73.5 ± 13.9 | 85.9 ± 13.0 | 0.035 |
| % time spent at IG 131–190 mg/dl | 6.4 ± 5.0 | 9.4 ± 10.6 | 0.524 * |
| % time spent at IG > 190 mg/dL | 0.5 ± 0.6 | 1.3 ± 3.3 | 0.689 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lupoli, R.; Calcaterra, I.; Annunziata, G.; Tenore, G.; Rainone, C.; Schiavo, L.; Capaldo, B.; Di Minno, M.N.D. Post-Bariatric Hypoglycemia Is Associated with Endothelial Dysfunction and Increased Oxidative Stress. Biomedicines 2022, 10, 916. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10040916
Lupoli R, Calcaterra I, Annunziata G, Tenore G, Rainone C, Schiavo L, Capaldo B, Di Minno MND. Post-Bariatric Hypoglycemia Is Associated with Endothelial Dysfunction and Increased Oxidative Stress. Biomedicines. 2022; 10(4):916. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10040916
Chicago/Turabian StyleLupoli, Roberta, Ilenia Calcaterra, Giuseppe Annunziata, Giancarlo Tenore, Carmen Rainone, Luigi Schiavo, Brunella Capaldo, and Matteo Nicola Dario Di Minno. 2022. "Post-Bariatric Hypoglycemia Is Associated with Endothelial Dysfunction and Increased Oxidative Stress" Biomedicines 10, no. 4: 916. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10040916