
Premenopausal Syndrome and NAFLD: A New Approach Based on Gender Medicine
 , , ,
, , , 
Abstract
:1. Introduction
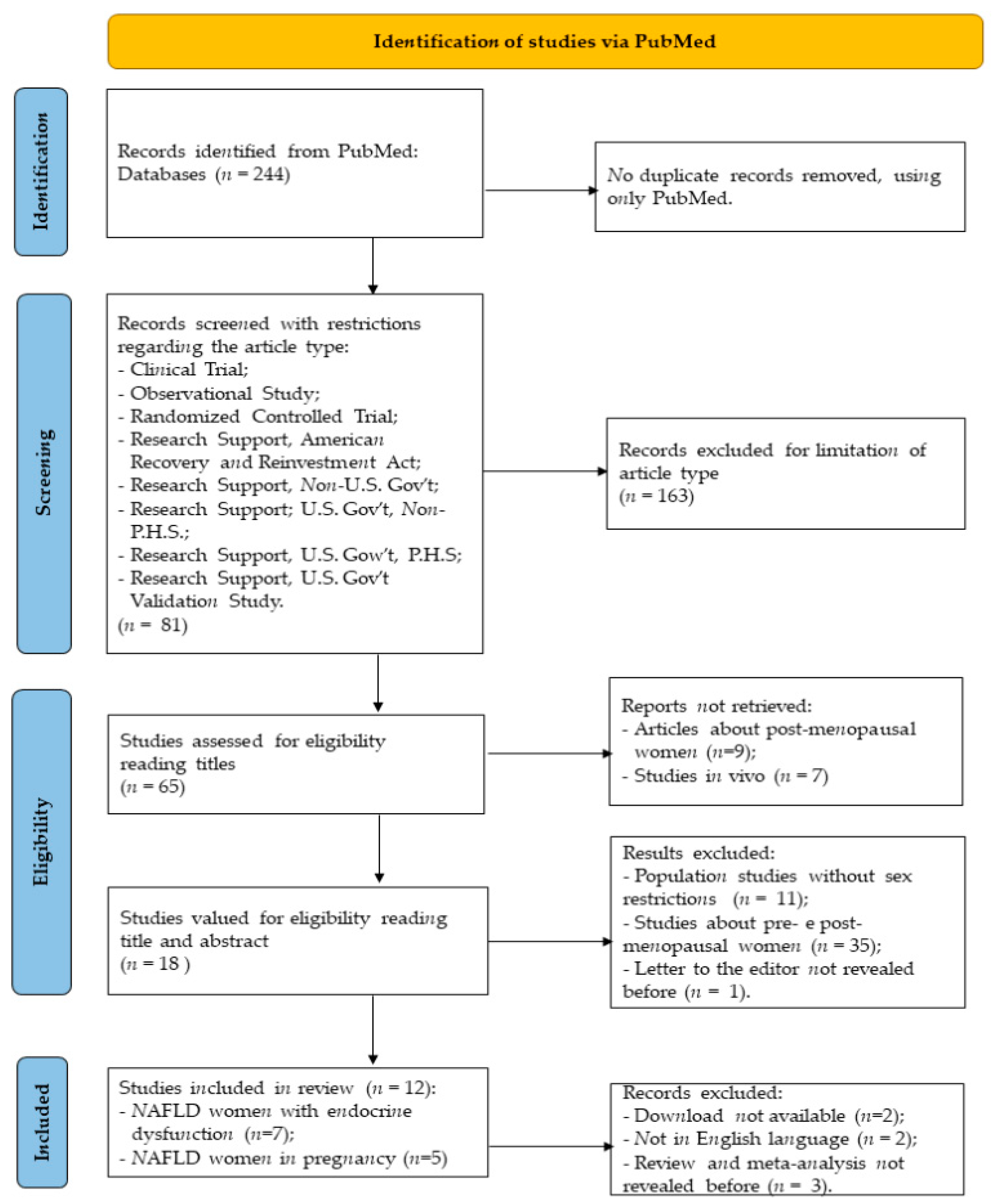
2. Identification of Studies
3. Hormones Involved in Development of NAFLD
4. PCOS Syndrome in Premenopausal Woman
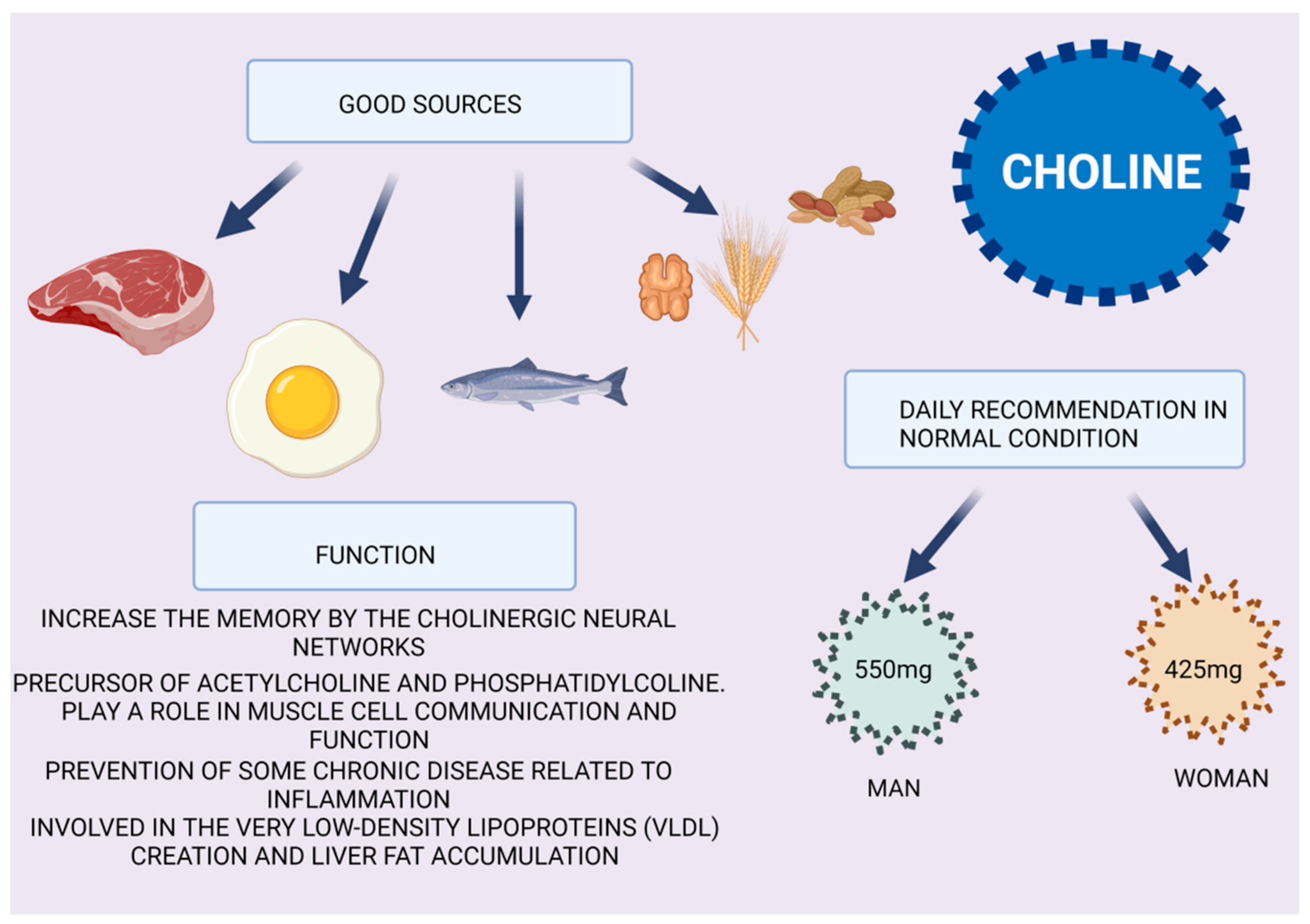
5. Choline
6. Pregnancy and Breast Feeding Are Alarm Bells for NAFLD in Premenopausal Women
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Younossi, Z.; Tacke, F.; Arrese, M.; Sharma, B.C.; Mostafa, I.; Bugianesi, E.; Wong, V.W.-S.; Yilmaz, Y.; George, J.; Fan, J.; et al. Global Perspectives on Nonalcoholic Fatty Liver Disease and Nonalcoholic Steatohepatitis. Hepatology 2019, 69, 2672–2682. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global epidemiology of nonalcoholic fatty liver disease—Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef] [PubMed]
- Farrell, G.C.; Wong, V.W.-S.; Chitturi, S. NAFLD in Asia—As common and important as in the West. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 307–318. [Google Scholar] [CrossRef]
- Mundi, M.S.; Velapati, S.; Patel, J.; Kellogg, T.A.; Abu Dayyeh, B.K.; Hurt, R.T. Evolution of NAFLD and Its Management. Nutr. Clin. Pr. 2019, 35, 72–84. [Google Scholar] [CrossRef] [PubMed]
- Neuschwander-Tetri, B.A. Non-alcoholic fatty liver disease. BMC Med. 2017, 15, 45. [Google Scholar] [CrossRef]
- Robinson, M.; Harmon, C.; O’Farrelly, C. Liver immunology and its role in inflammation and homeostasis. Cell. Mol. Immunol. 2016, 13, 267–276. [Google Scholar] [CrossRef]
- Czaja, A.J. Hepatic inflammation and progressive liver fibrosis in chronic liver disease. World J. Gastroenterol. 2014, 20, 2515–2532. [Google Scholar] [CrossRef]
- Hijona, E.; Hijona, L.; Arenas, J.I.; Bujanda, L. Inflammatory Mediators of Hepatic Steatosis. Mediat. Inflamm. 2010, 2010, 837419. [Google Scholar] [CrossRef]
- Martínez-Esparza, M.; Tristán, M.; Ruiz-Alcaraz, A.J.; García-Peñarrubia, P. Inflammatory status in human hepatic cirrhosis. World J. Gastroenterol. 2015, 21, 11522–11541. [Google Scholar] [CrossRef]
- Kautzky-Willer, A.; Handisurya, A. Metabolic diseases and associated complications: Sex and gender matter! Eur. J. Clin. Investig. 2009, 39, 631–648. [Google Scholar] [CrossRef]
- Della Torre, S.; Maggi, A. Sex Differences: A Resultant of an Evolutionary Pressure? Cell Metab. 2017, 25, 499–505. [Google Scholar] [CrossRef] [PubMed]
- Della Torre, S.; Benedusi, V.; Fontana, R.; Maggi, A. Energy metabolism and fertility—A balance preserved for female health. Nat. Rev. Endocrinol. 2013, 10, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Barone, M.; Margiotta, M.; Scavo, M.; Gentile, A.; Francioso, D.; Papagni, S.; Castellaneta, A.; Mallamaci, R.; Di Leo, A.; Francavilla, A. Possible involvement of androgen receptor alterations in hepatocarcinogenesis. Dig. Liver Dis. 2009, 41, 665–670. [Google Scholar] [CrossRef] [PubMed]
- Barone, M.; Maiorano, E.; Scavo, M.P.; Panella, E.; Castellaneta, A.; Napoli, A.; Francioso, D.; Di Leo, A.; Francavilla, A. Ep-idemiological data demonstrate that HCC is prevalent in men compared to women. Dig. Liver Dis. 2009, 41, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 88, 105906. [Google Scholar] [CrossRef]
- Setji, T.L.; Holland, N.D.; Sanders, L.L.; Pereira, K.C.; Diehl, A.M.; Brown, A.J. Nonalcoholic Steatohepatitis and Nonalcoholic Fatty Liver Disease in Young Women with Polycystic Ovary Syndrome. J. Clin. Endocrinol. Metab. 2006, 91, 1741–1747. [Google Scholar] [CrossRef]
- Cerda, C.; Pérez-Ayuso, R.M.; Riquelme, A.; Soza, A.; Villaseca, P.; Sir-Petermann, T.; Espinoza, M.; Pizarro, M.; Solis, N.; Miquel, J.F.; et al. Nonalcoholic fatty liver disease in women with polycystic ovary syndrome. J. Hepatol. 2007, 47, 412–417. [Google Scholar] [CrossRef]
- Forbes, S.; Taylor-Robinson, S.D.; Patel, N.; Allan, P.; Walker, B.R.; Johnston, D.G. Increased prevalence of non-alcoholic fatty liver disease in European women with a history of gestational diabetes. Diabetologia 2010, 54, 641–647. [Google Scholar] [CrossRef]
- Liu, Y.; Lu, J.; Xu, M.; Xu, Y.; Li, M.; Wang, T.; Zhang, J.; Xu, B.; Sun, J.; Dai, M.; et al. Association between history of abortion and nonalcoholic fatty liver disease in middle-aged and elderly Chinese women. Ann. Epidemiology 2013, 23, 119–123. [Google Scholar] [CrossRef]
- Vassilatou, E.; A Vassiliadi, D.; Salambasis, K.; Lazaridou, H.; Koutsomitopoulos, N.; Kelekis, N.; Kassanos, D.; Hadjidakis, D.; Dimitriadis, G. Increased prevalence of polycystic ovary syndrome in premenopausal women with nonalcoholic fatty liver disease. Eur. J. Endocrinol. 2015, 173, 739–747. [Google Scholar] [CrossRef]
- Hagström, H.; Höijer, J.; Ludvigsson, J.F.; Bottai, M.; Ekbom, A.; Hultcrantz, R.; Stephansson, O.; Stokkeland, K. Adverse outcomes of pregnancy in women with non-alcoholic fatty liver disease. Liver Int. 2015, 36, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Vassilatou, E.; Lafoyianni, S.; Vassiliadi, D.A.; Ioannidis, D.; Paschou, S.A.; Mizamtsidi, M.; Panagou, M.; Vryonidou, A. Visceral adiposity index for the diagnosis of nonalcoholic fatty liver disease in premenopausal women with and without polycystic ovary syndrome. Maturitas 2018, 116, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Kumarendran, B.; O’Reilly, M.W.; Manolopoulos, K.N.; Toulis, K.A.; Gokhale, K.M.; Sitch, A.J.; Wijeyaratne, C.N.; Coomarasamy, A.; Arlt, W.; Nirantharakumar, K. Polycystic ovary syndrome, androgen excess, and the risk of nonalcoholic fatty liver disease in women: A longitudinal study based on a United Kingdom primary care database. PLoS Med. 2018, 15, e1002542. [Google Scholar] [CrossRef] [PubMed]
- Ajmera, V.; Terrault, N.A.; VanWagner, L.; Sarkar, M.; Lewis, C.E.; Carr, J.J.; Gunderson, E.P. Longer lactation duration is associated with decreased prevalence of non-alcoholic fatty liver disease in women Veeral. J. Hepatol. 2019, 70, 126–132. [Google Scholar] [CrossRef] [PubMed]
- Sarkar, M.A.; Suzuki, A.; Abdelmalek, M.F.; Yates, K.P.; Wilson, L.A.; Bass, N.M.; Gill, R.; Cedars, M.; Terrault, N. Testosterone is Associated With Nonalcoholic Steatohepatitis and Fibrosis in Premenopausal Women With NAFLD. Clin. Gastroenterol. Hepatol. 2020, 19, 1267–1274.e1. [Google Scholar] [CrossRef] [PubMed]
- Jung, Y.M.; Lee, S.M.; Hong, S.; Koo, J.N.; Oh, I.H.; Kim, B.J.; Kim, S.M.; Kim, S.Y.; Kim, G.M.; Joo, S.K.; et al. The risk of pregnancy-associated hypertension in women with nonalcoholic fatty liver disease. Liver Int. 2020, 40, 2417–2426. [Google Scholar] [CrossRef] [PubMed]
- Di Stasi, V.; Maseroli, E.; Rastrelli, G.; Scavello, I.; Cipriani, S.; Todisco, T.; Marchiani, S.; Sorbi, F.; Fambrini, M.; Petraglia, F.; et al. SHBG as a Marker of NAFLD and Metabolic Impairments in Women Referred for Oligomenorrhea and/or Hirsutism and in Women with Sexual Dysfunction. Front. Endocrinol. 2021, 12, 641446. [Google Scholar] [CrossRef]
- Hamaguchi, M.; Kojima, T.; Ohbora, A.; Takeda, N.; Fukui, M.; Kato, T. Aging is a risk factor of nonalcoholic fatty liver disease in premenopausal women. World J. Gastroenterol. 2012, 18, 237–243. [Google Scholar] [CrossRef]
- Chung, G.E.; Yim, J.Y.; Kim, D.; Lim, S.H.; Yang, J.I.; Kim, Y.S.; Yang, S.Y.; Kwak, M.S.; Kim, J.S.; Cho, S.H. The influence of metabolic factors for nonalcoholic Fatty liver disease in women. Biomed Res. Int. 2015, 2015, 131528. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Anstee, Q.M.; Marietti, M.; Hardy, T.; Henry, L.; Eslam, M.; George, J.; Bugianesi, E. Global burden of NAFLD and NASH: Trends, predictions, risk factors and prevention. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 11–20. [Google Scholar] [CrossRef]
- della Torre, S. Beyond the x factor: Relevance of sex hormones in nafld pathophysiology. Cells 2021, 10, 2502. [Google Scholar] [CrossRef] [PubMed]
- Calabrese, F.M.; Disciglio, V.; Franco, I.; Sorino, P.; Bonfiglio, C.; Bianco, A.; Campanella, A.; Lippolis, T.; Pesole, P.L.; Polignano, M.; et al. A Low Glycemic Index Mediterranean Diet Combined with Aerobic Physical Activity Rearranges the Gut Microbiota Signature in NAFLD Patients. Nutrients 2022, 14, 1773. [Google Scholar] [CrossRef]
- Liu, L.; Fu, Q.; Li, T.; Shao, K.; Zhu, X.; Cong, Y.; Zhao, X. Gut microbiota and butyrate contribute to nonalcoholic fatty liver disease in premenopause due to estrogen deficiency. PLoS ONE 2022, 17, e0262855. [Google Scholar] [CrossRef] [PubMed]
- Abuwani, A.M.; Dash, S.P.; Ganesan, R.; Renu, K.; Vellingiri, B.; Kandasamy, S.; Rajan, S.; Gopalakrishnan, A.V. Gut micro-biome and metabolic response in non-alcoholic fatty liver disease. Clin. Chim. Acta. 2021, 523, 304–314. [Google Scholar] [CrossRef] [PubMed]
- Park, E.; Jeong, J.J.; Won, S.M.; Sharma, S.P.; Gebru, Y.A.; Ganesan, R.; Gupta, H.; Suk, K.T.; Kim, D.J. Gut Microbio-ta-Related Cellular and Molecular Mechanisms in the Progression of Nonalcoholic Fatty Liver Disease. Cells 2021, 10, 2634. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.L.; Yakar, S.; Leroith, D. Conditional knockout of mouse insulin-like growth factor-1 gene using the Cre/loxP system. Proc. Soc. Exp. Biol. Med. 2010, 223, 344–351. [Google Scholar]
- Ohlsson, C.; Bengtsson, B.A.; Isaksson, O.G.; Andreassen, T.T.; Slootweg, M.C. Growth hormone and bone. Endocr. Rev. 1998, 19, 55–79. [Google Scholar]
- Wang, X.B.; Wang, S.B.; Wu, H.B.; Jiang, M.B.; Xue, H.M.; Zhu, Y.M.; Wang, C.M.; Zha, X.M.; Wen, Y. Human growth hormone level decreased in women aged <60 years but increased in men aged >50 years. Medicine 2020, 99, e18440. [Google Scholar] [CrossRef]
- Steyn, F.J.; Ngo, S.T. Endocrine rhythms of growth hormone release: Insights from animal studies. Best Pr. Res. Clin. Endocrinol. Metab. 2017, 31, 521–533. [Google Scholar] [CrossRef]
- Cook, C.B.; Nippoldt, T.B.; Kletter, G.B.; Kelch, R.P.; Marshall, J.C. Naloxone Increases the Frequency of Pulsatile Luteinizing Hormone Secretion in Women with Hyperprolactinemia. J. Clin. Endocrinol. Metab. 1991, 73, 1099–1105. [Google Scholar] [CrossRef]
- van den Berg, G.; Veldhuis, J.D.; Frolich, M.; Roelfsema, F. An amplitude-specific divergence in the pulsatile mode of growth hormone (GH) secretion underlies the gender difference in mean GH concentrations in men and premenopausal women. J. Clin. Endocrinol Metab. 1996, 81, 2460–2467. [Google Scholar] [PubMed]
- Cattini, P.A.; Bock, M.E.; Jin, Y.; Zanghi, J.A.; Vakili, H. A useful model to compare human and mouse growth hormone gene chromosomal structure, expression and regulation, and immune tolerance of human growth hormone analogues. Growth Horm. IGF Res. 2018, 42–43, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Garcia, J.M.; Merriam, G.R.; Kargi, A.Y. Growth Hormone in Aging; Endotex: South Dartmouth, MA, USA, 2019. [Google Scholar]
- Park, Y.-M.; Erickson, C.; Bessesen, D.; Van Pelt, R.E.; Cox-York, K. Age- and menopause-related differences in subcutaneous adipose tissue estrogen receptor mRNA expression. Steroids 2017, 121, 17–21. [Google Scholar] [CrossRef] [PubMed]
- Yuan, L.; Kardashian, A.; Sarkar, M. NAFLD in Women: Unique Pathways, Biomarkers, and Therapeutic Opportunities. Curr. Hepatol. Rep. 2019, 18, 425–432. [Google Scholar] [CrossRef]
- Quigley, C.A.; De Bellis, A.; Marschke, K.B.; EL-Awady, M.K.; Wilson, E.M.; French, F.S. Androgen Receptor Defects: Histori-cal, Clinical, and Molecular Perspectives. Endocr. Rev. 1995, 16, 271–321. [Google Scholar] [CrossRef]
- Jaruvongvanich, V.; Sanguankeo, A.; Riangwiwat, T.; Upala, S. Testosterone, Sex HormoneBinding Globulin and Nonalco-holic Fatty Liver Disease: A Systematic Review and Meta-Analysis. Ann. Hepatol. 2017, 16, 382–394. [Google Scholar] [CrossRef]
- Sarkar, M.; Wellons, M.; Cedars, M.; VanWagner, L.; Gunderson, E.; Ajmera, V.; Torchen, L.; Siscovick, D.; Carr, J.J.; Terry, J.G. For the Coronary Artery Risk Development in Young Adults (CARDIA) Cohort Testosterone Levels in Pre-Menopausal Women are Associated with Nonalcoholic Fatty Liver Disease in Midlife. Am. J. Gastroenterol. 2017, 112, 755–762. [Google Scholar] [CrossRef]
- Evans, S.F.; Hull, M.L.; Hutchinson, M.R.; Rolan, P.E. Androgens, Endometriosis and Pain. Front. Reprod. Health 2021, 3, 792920. [Google Scholar] [CrossRef]
- Pan, J.J.; Fallon, M.B. Gender and Racial Differences in Nonalcoholic Fatty Liver Disease. World J. Hepatol. 2014, 6, 274–283. [Google Scholar] [CrossRef]
- Yang, J.D.; Abdelmalek, M.F.; Guy, C.D.; Gill, R.M.; Lavine, J.E.; Yates, K.; Klair, J.; Terrault, N.A.; Clark, J.M.; Unalp-Arida, A.; et al. Patient sex, reproductive status, and synthetic hormone use associate with histologic severity of nonalcoholic steatohep-atitis. Clin. Gastroenterol Hepatol. 2017, 15, 127–131.e2. [Google Scholar] [CrossRef]
- Fugate Woods, N.; Sullivan Mitchell, E.; Smith-Di Julio, K. Cortisol Levels during the Menopausal Transition and Early Postmenopause: Observations from the Seattle Midlife Women’s Health Study. Menopause 2009, 16, 708–718. [Google Scholar] [CrossRef] [PubMed]
- Dakin, R.S.; Walker, B.R.; Seckl, J.R.; Hadoke, P.W.F.; Drake, A.J. Estrogens protect male mice from obesity complications and influence glucocorticoid metabolism. Int. J. Obes. 2015, 39, 1539–1547. [Google Scholar] [CrossRef] [PubMed]
- El-Sehrawy, A.A.; State, O.; Elzehery, R.R.; Mohamed, A.S. Insulin Resistance and Non-Alcoholic Fatty Liver Disease in Premenopausal Women with Metabolic Syndrome. Horm. Metab. Res. 2021, 53, 100–104. [Google Scholar] [CrossRef] [PubMed]
- di Sessa, A.; Grandone, A.; Marzuillo, P.; Umano, G.R.; Cirillo, G.; del Giudice, E.M. Early menarche is associated with insu-lin-resistance and non-alcoholic fatty liver disease in adolescents with obesity. J. Pediatric Endocrinol. Metab. 2021, 34, 607–612. [Google Scholar] [CrossRef]
- Ballestri, S.; Nascimbeni, F.; Baldelli, E.; Marrazzo, A.; Romagnoli, D.; Lonardo, A. NAFLD as a Sexual Dimorphic Disease: Role of Gender and Reproductive Status in the Development and Progression of Nonalcoholic Fatty Liver Disease and In-herent Cardiovascular Risk. Adv. Ther. 2017, 34, 1291–1326. [Google Scholar] [CrossRef]
- Mueller, N.T.; Pereira, M.A.; Demerath, E.W.; Dreyfus, J.G.; MacLehose, R.F.; Carr, J.J.; Terry, J.G.; Jacobs, D.R. Earlier men-arche is associated with fatty liver and abdominal ectopic fat in midlife, independent of young adult BMI: The CARDIA study. Obesity 2015, 23, 468–474. [Google Scholar] [CrossRef]
- Spremovi’c Radenovi’c, S.; Pupovac, M.; Andji’, M.; Bila, J.; Sre’ckovi, S.; Gudovi, A.; Dragaš, B.; Radunovi, N. Prevalence, Risk Factors, and Pathophysiology of Nonalcoholic Fatty Liver Disease (NAFLD) in Women with Polycystic OvarySyndrome (PCOS). Biomedicines 2022, 10, 131. [Google Scholar] [CrossRef]
- Hashimoto, E.; Tokushige, K. Prevalence, gender, ethnic variations, and prognosis of NASH. J. Gastroenterol. 2010, 46, 63–69. [Google Scholar] [CrossRef]
- Gutierrez-Grobe, Y.; Ponciano-Rodríguez, G.; Ramos, M.H.; Uribe, M.; Méndez-Sánchez, N. Prevalence of non alcoholic fatty liver disease in premenopausal, posmenopausal and polycystic ovary syndrome women. The role of estrogens. Ann. Hepatol. 2010, 9, 402–409. [Google Scholar] [CrossRef]
- Shengir, M.; Chen, T.; Guadagno, E.; Ramanakumar, A.V.; Ghali, P.; Deschenes, M.; Wong, P.; Krishnamurthy, S.; Sebas-tiani, G. Non-alcoholic fatty liver disease in premenopausal women with pol-ycystic ovary syndrome: A systematic review and meta-analysis. JGH Open. 2021, 5, 434–445. [Google Scholar] [CrossRef] [PubMed]
- Cho, I.Y.; Chang, Y.; Kang, J.H.; Kim, Y.; Sung, E.; Shin, H.; Wild, S.H.; Byrne, C.D.; Ryu, S. Long or Irregular Menstrual Cycles and Risk of Prevalent and Incident Nonalcoholic Fatty Liver Disease. J. Clin. Endocrinol. Metab. 2022, 107, e2309–e2317. [Google Scholar] [CrossRef] [PubMed]
- Ajmal, N.; Khan, S.Z.; Shaikh, R. Polycystic ovary syndrome (PCOS) and genetic predisposition: A review article. Eur. J. Obstet. Gynecol. Reprod. Biol. X 2019, 3, 100060. [Google Scholar] [CrossRef] [PubMed]
- Lau, J.K.C.; Zhang, X.; Yu, J. Animal models of non-alcoholic fatty liver disease: Current perspectives and recent advances. J. Pathol. 2016, 241, 36–44. [Google Scholar] [CrossRef] [PubMed]
- Song, J.; da Costa, K.A.; Fischer, L.M.; Kohlmeier, M.; Kwock, L.; Wang, S.; Zeisel, S.H. Polymorphism of the PEMT gene and susceptibility to nonalcoholic fatty liver disease (NAFLD). FASEB J. 2005, 19, 1266Y1271. [Google Scholar] [CrossRef] [PubMed]
- Resseguie, M.; Song, J.; Niculescu, M.D.; da Costa, K.-A.; Randall, T.A.; Zeisel, S.H. PhosphatidylethanolamineN-methyltransferase(PEMT)gene expression is induced by estrogen in human and mouse primary hepatocytes. FASEB J. 2007, 21, 2622–2632. [Google Scholar] [CrossRef] [PubMed]
- Sherriff, J.L.; O’Sullivan, T.A.; Properzi, C.; Oddo, J.-L.; Adams, L.A. Choline, Its Potential Role in Nonalcoholic Fatty Liver Disease, and the Case for Human and Bacterial Genes. Adv. Nutr. Int. Rev. J. 2016, 7, 5–13. [Google Scholar] [CrossRef]
- You, S.Y.; Han, K.; Lee, S.H.; Kim, M.K. Nonalcoholic fatty liver disease and the risk of insulin-requiring gestational diabetes. Diabetol. Metab. Syndr. 2021, 13, 90. [Google Scholar] [CrossRef]
- Sharma, D.L.; Lakhani, H.V.; Klug, R.L.; Snoad, B.; El-Hamdani, R.; Shapiro, J.I.; Sodhiet, K. Investigating molecular connections of non-alcoholic fatty liver disease with associated pathological conditions in West Virginia for biomarker analysis. J. Clin. Cell Immunol. 2017, 8, 523. [Google Scholar] [CrossRef]
- Misu, H.; Takamura, T.; Takayama, H.; Hayashi, H.; Nagata, N.; Kurita, S.; Ishikura, K.; Ando, H.; Takeshita, Y.; Ota, T.; et al. A Liver-Derived Secretory Protein, Selenoprotein P, Causes Insulin Resistance. Cell Metab. 2010, 12, 483–495. [Google Scholar] [CrossRef]
- Isobe, Y.; Asakura, H.; Tsujiguchi, H.; Kannon, T.; Takayama, H.; Takeshita, Y.; Ishii, K.A.; Kanamori, T.; Hara, A.; Yama-shita, T.; et al. Alcohol Intake Is Associated with Elevated Serum Levels of Selenium and Selenoprotein P in Humans. Front. Nutr. 2021, 8, 633703. [Google Scholar] [CrossRef]
- Suliga, E.; Ciesla, E.; Gluszek-Osuch, M.; Lysek-Gladysinska, M.; Wawrzycka, I.; Gluszek, S. Breastfeeding and Prevalence of Metabolic Syndrome among Perimenopausal Women. Nutrients 2020, 12, 2691. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.; Sinn, D.H.; Oh, J.H.; Goh, M.J.; Kim, K.; Kang, W.; Paik, Y.; Choi, M.S.; Lee, J.H.; Koh, K.C.; et al. The Association Between Breastfeeding and Nonalcoholic Fatty Liver Disease in Parous Women: A Nation-wide Cohort Study. Hepatology 2021, 74, 2988–2997. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Beatrice, G.; Zusi, C.; Dalbeni, A. Breastfeeding duration and reduced risk of NAFLD in midlife of parous women. Explor. Med. 2021, 2, 378–381. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age Group | Pathogenesis | Population Study | Study Duration | Reference | Year of Publication | |
|---|---|---|---|---|---|---|
| Young | PCOS | 200 women with PCOS | 1999–2004 | Setji, T. L. et al. | Nonalcoholic steatohepatitis and nonalcoholic fatty liver disease in young women with polycystic ovary syndrome. J. Clin. Endocrinol. Metab. [16] | 2006 |
| Fertile Adult | PCOS | 41 consecutive non-pregnant women with PCOS and 31 non-pregnant heathy women | 2005–2006 | Cerda, C. et al. | Nonalcoholic fatty liver disease in women with polycystic ovary syndrome.J. Hepatol. [17] | 2007 |
| All range age | Hormones | 223 women (110 with previous gestational diabetes and 113 without previous gestational diabetes) | 2002–2010 | Forbes, S. et al. | Increased prevalence of non- alcoholic fatty liver disease in European women with a history of gestational diabetes. Diabetology [18] | 2011 |
| Middle age and elderly | Problematic Pregnancy | 5911 women with known reproductive histories | 2010 | Liu, Y. et al. | Association between history of abortion and nonalcoholic fatty liver disease in middle-aged and elderly Chinese women. Ann. Epidem [19] | 2013 |
| Pre-Menopausal | PCOS | 110 women (71 with hepatosteatosis and 39 without hepatosteatosis) | 2011–2014 | Vassilatou, E. et al | Increased prevalence of polycystic ovary syndrome in premenopausal women with nonalcoholic fatty liver disease.Eur. J. Endocrinol. [20] | 2015 |
| Pre-Menopausal | Problematic Pregnancy | 1960416 women divided into groups of non-NAFLD, non-PCOS and non-NAFLD with PCOS | 1992–2011 | Hagström, H. et al. | Adverse outcomes of pregnancy in women with non-alcoholic fatty liver disease. Liver int. [21] | 2016 |
| Pre-Menopausal | Obesity and PCOS | 250 pre-menopausal women (132 with NAFLD and 158 non-NAFLD) | 2007–2010 | Vassilatou, E. et al. | Visceral adiposity index for the diagnosis of nonalcoholic fatty liver disease in premenopausal women with and without polycystic ovary syndrome. Maturitas [22] | 2018 |
| All range age | PCOS and Hormone imbalance | 2706062 women divided into PCOS cohort and control group | 2000–2016 | Kumarendran, B. et al. | Polycystic ovary syndrome, androgen excess, and the risk of nonalcoholic fatty liver disease in women: A longitudinal study based on a United Kingdom primary care database. PLoS Med. [23] | 2018 |
| Pre-Menopausal | Hormone imbalance | 844 women with reported lactation duration | 1985–2010 | Ajmera, V. et al. | Longer lactation duration is associated with decreased prevalence of non-alcoholic fatty liver disease in women. J.Hepatol. [24] | 2019 |
| Pre-Menopausal | Hormone imbalance | 210 pre-menopausal women with confirmed NAFLD | 2020 | Sarkar, M. A. et al. | Testosterone is Associated With Nonalcoholic Steatohepatitis and Fibrosis in Premenopausal Women With NAFLD.Clin. Gastroenterol. Hepatol. [25] | 2021 |
| Pre-Menopausal | Problematic Pregnancy | 877 pregnant women | 2014–2017 | Jung, Y. M. et al. | The risk of pregnancy-associated hypertension in women with nonalcoholic fatty liver disease. Liver Int. [26] | 2020 |
| All range age | Hormones imbalace and sexual Dysfunction | 66 women with oligomenorrhea and/or hyperandrogenism and 233 women with sexual dysfunction | 2020 | Di Stasi, V. et al. | SHBG as a Marker of NAFLD and Metabolic Impairments in Women Referred for Oligomenorrhea and/or Hirsutism and in Women With Sexual Dysfunction. Front. Endocrinol. (Lausanne) [27] | 2021 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carrieri, L.; Osella, A.R.; Ciccacci, F.; Giannelli, G.; Scavo, M.P. Premenopausal Syndrome and NAFLD: A New Approach Based on Gender Medicine. Biomedicines 2022, 10, 1184. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10051184
Carrieri L, Osella AR, Ciccacci F, Giannelli G, Scavo MP. Premenopausal Syndrome and NAFLD: A New Approach Based on Gender Medicine. Biomedicines. 2022; 10(5):1184. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10051184
Chicago/Turabian StyleCarrieri, Livianna, Alberto Ruben Osella, Fausto Ciccacci, Gianluigi Giannelli, and Maria Principia Scavo. 2022. "Premenopausal Syndrome and NAFLD: A New Approach Based on Gender Medicine" Biomedicines 10, no. 5: 1184. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10051184