An In-Vitro Analysis of Peri-Implant Mucosal Seal Following Photofunctionalization of Zirconia Abutment Materials




Abstract
:1. Introduction
2. Materials and Methods
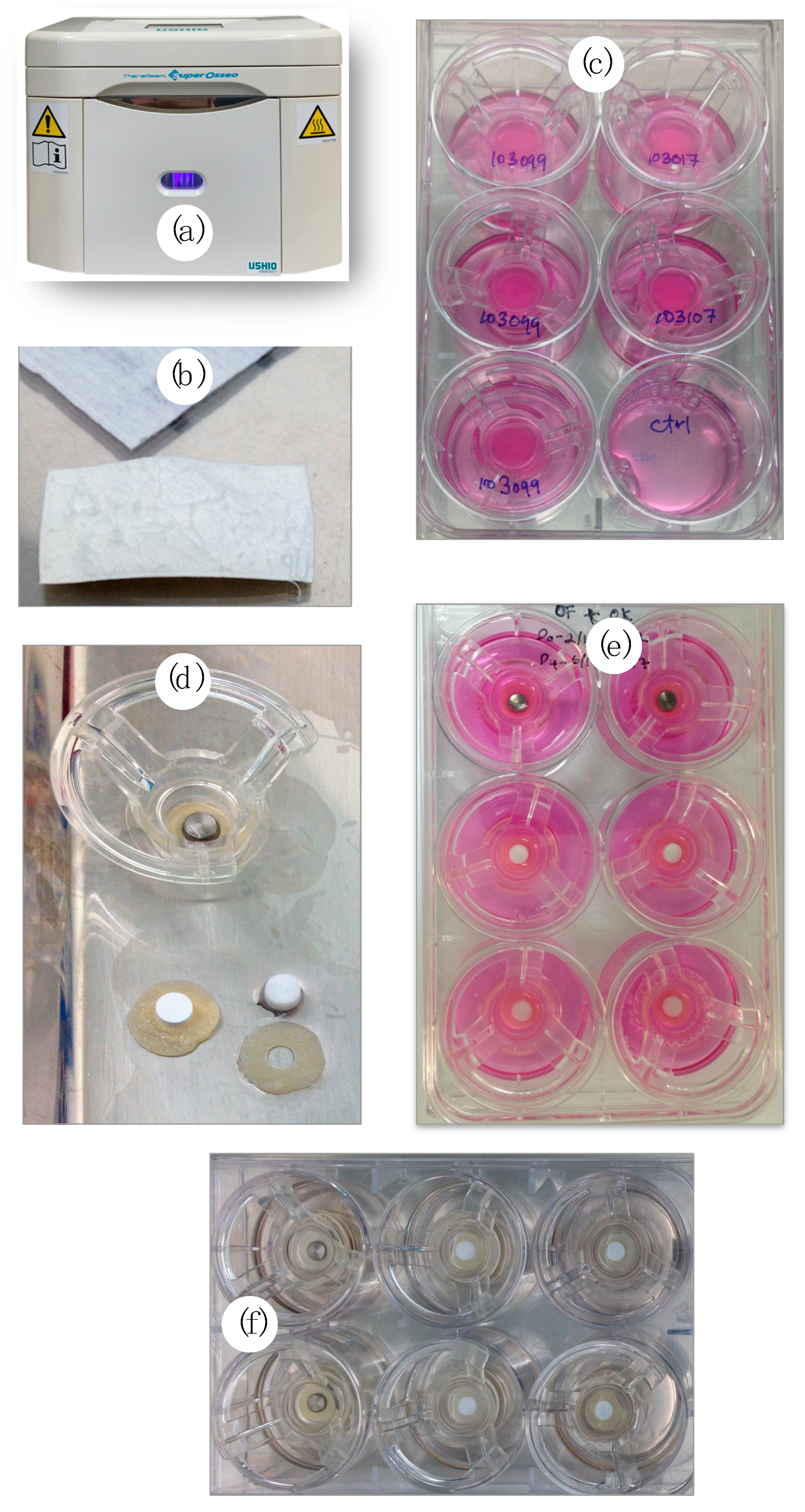
2.1. Preparation of Specimens
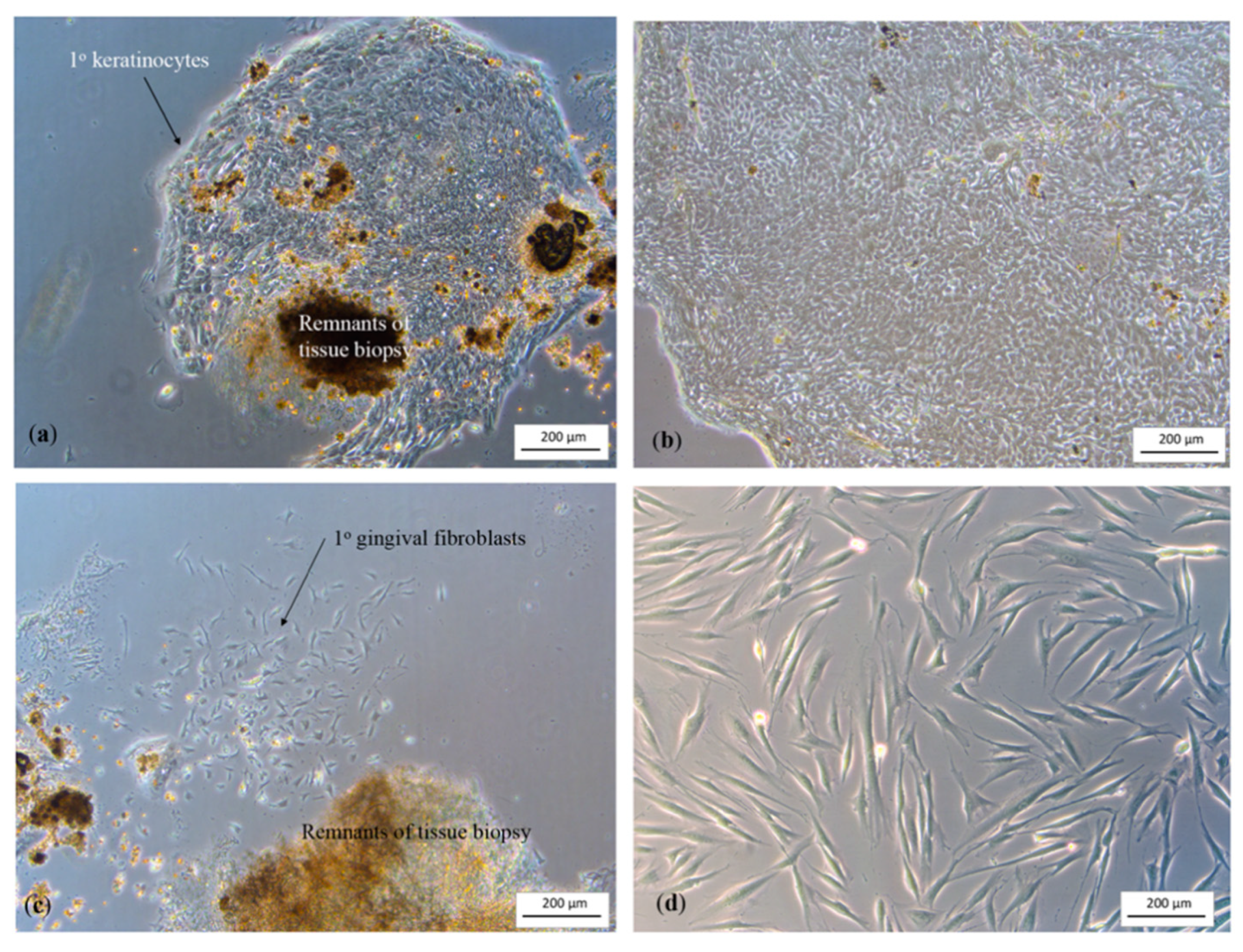
2.2. Cell Extraction
2.3. Three-Dimensional Peri-Implant Mucosal Model Development
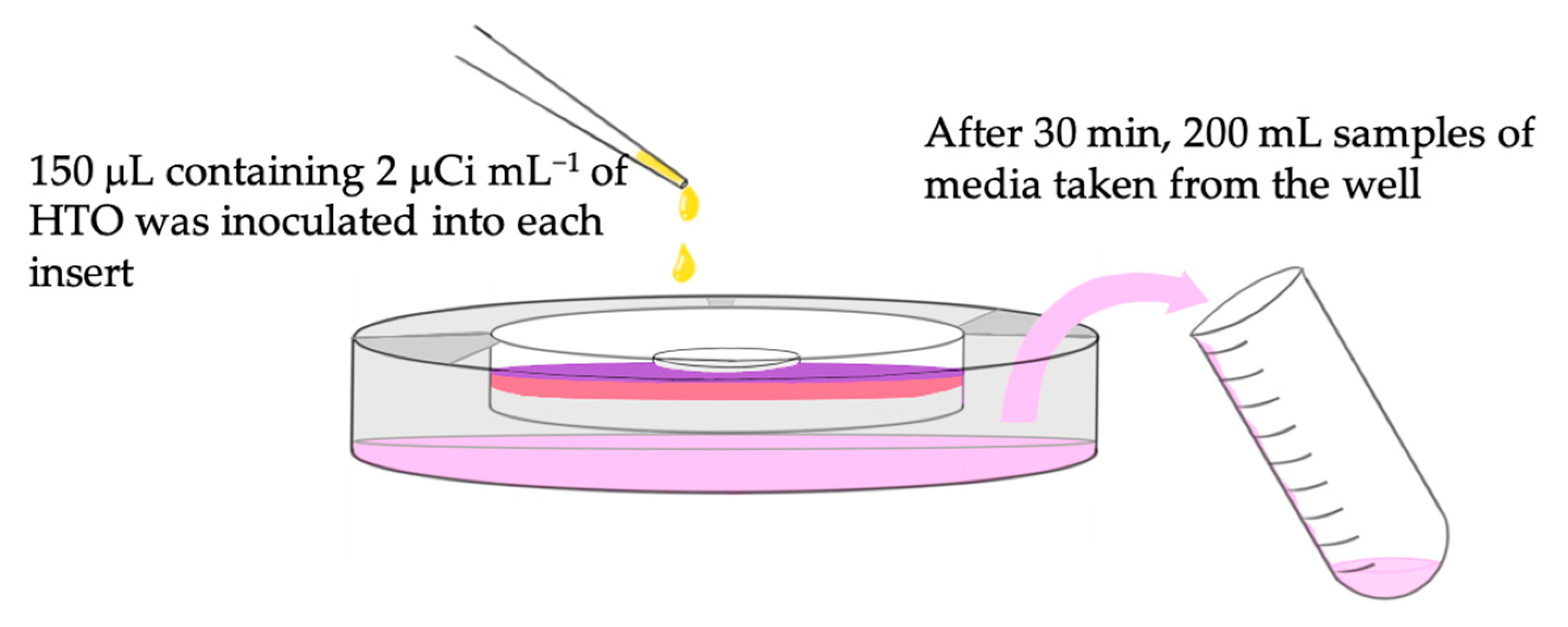
2.4. Permeability Test
2.5. Histological Preparation
2.6. Statistical Analysis
3. Results
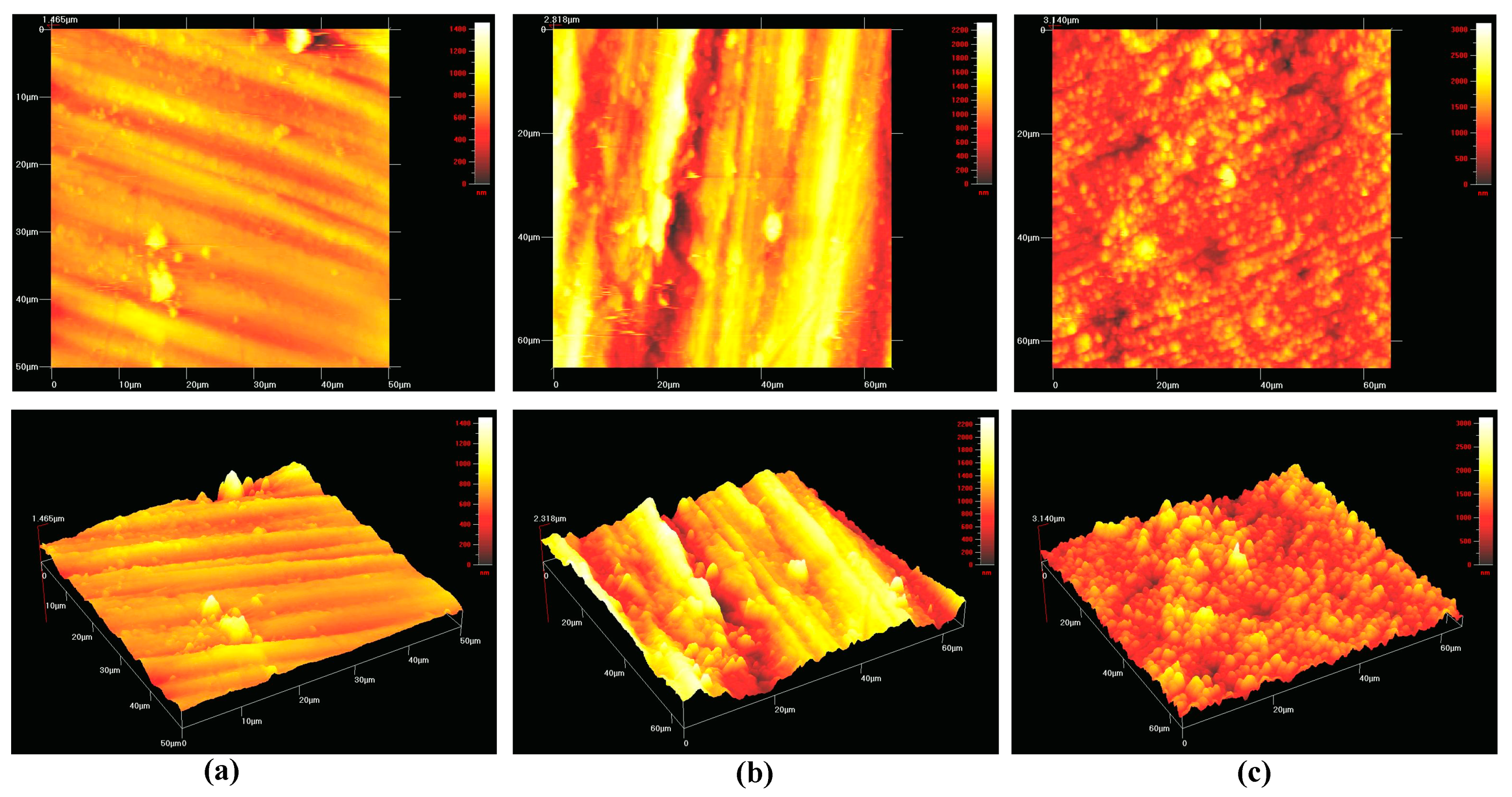
3.1. Composition and Surface Roughness
3.2. Cell Extraction and 3D Peri-Implant Mucosal Model
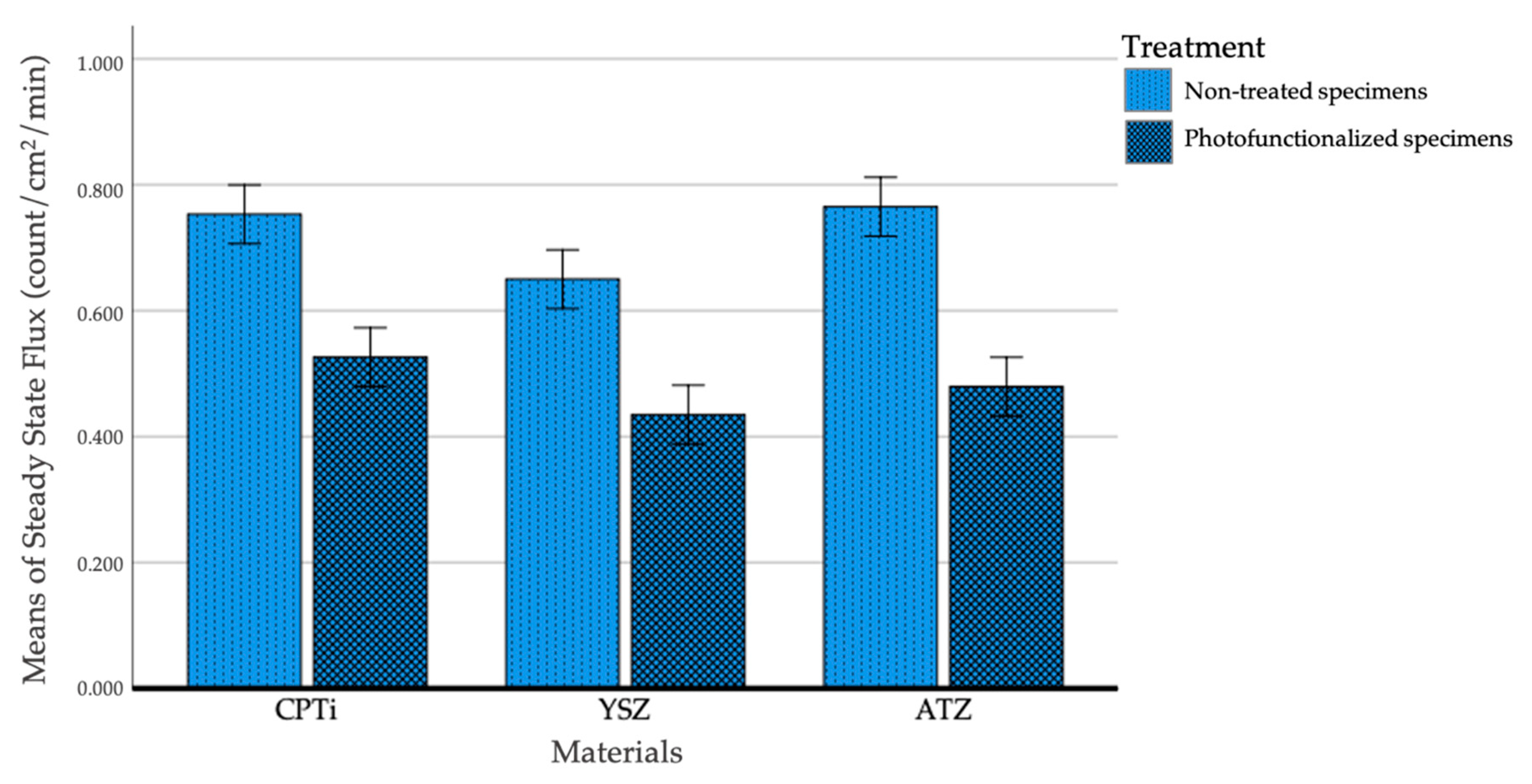
3.3. Permeability Test
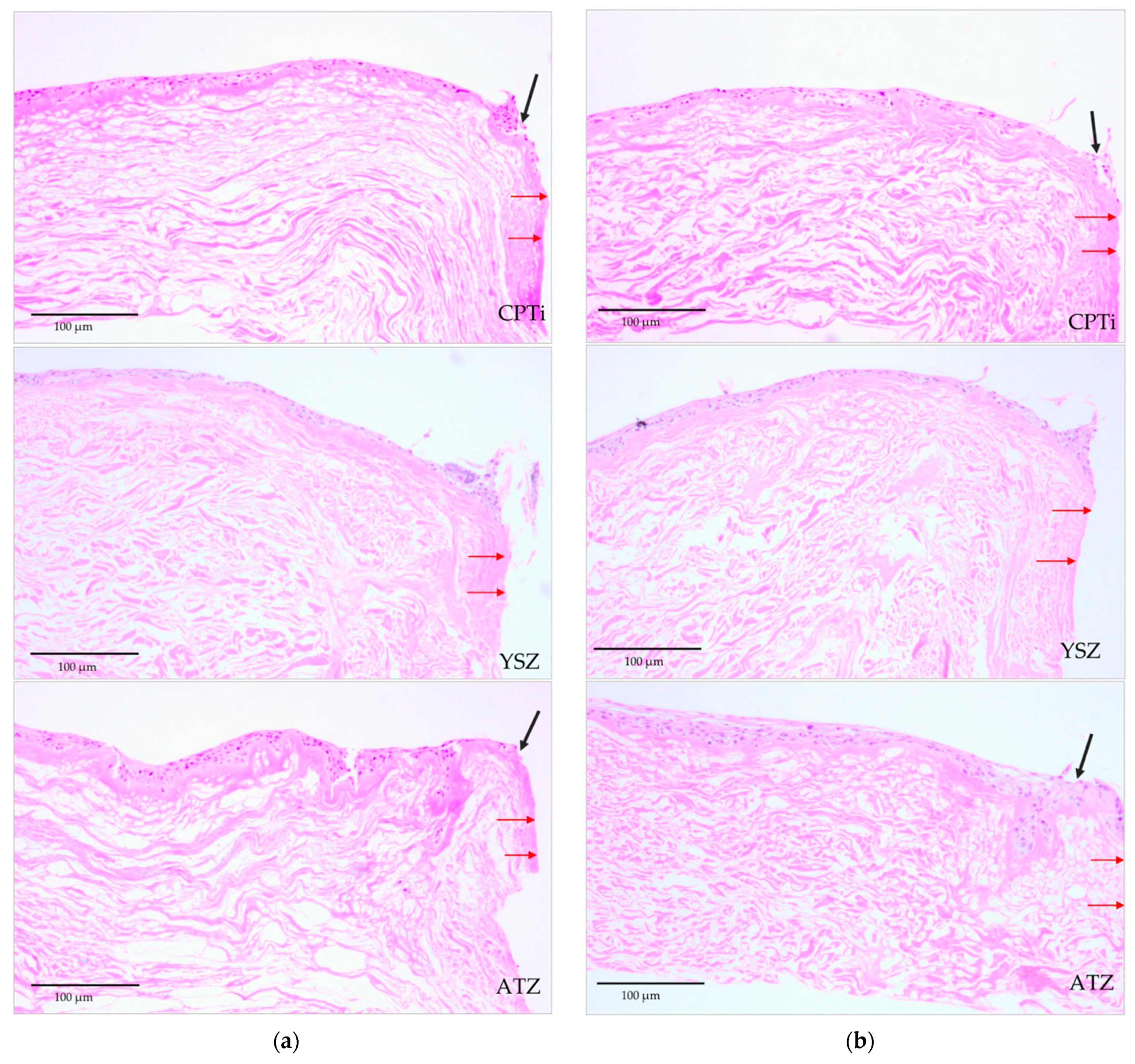
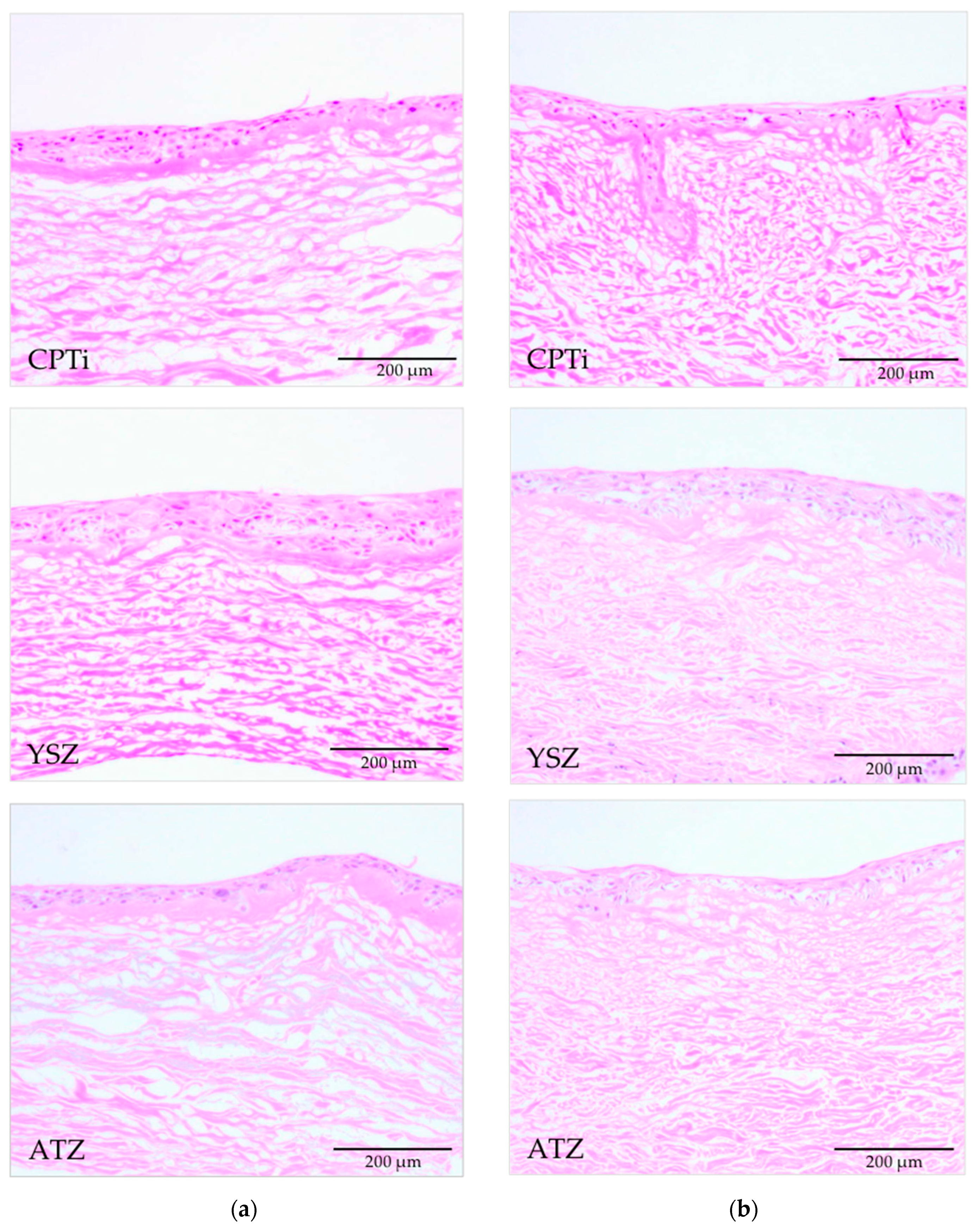
3.4. Histological Analyses
4. Discussions
5. Strengths and Limitations of the Study
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Howe, M.-S.; Keys, W.; Richards, D. Long-term (10-year) dental implant survival: A systematic review and sensitivity meta-analysis. J. Dent. 2019, 84, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Chrcanovic, B.; Kisch, J.; Albrektsson, T.; Wennerberg, A. A retrospective study on clinical and radiological outcomes of oral implants in patients followed up for a minimum of 20 years. Clin. Implant. Dent. Relat. Res. 2018, 20, 199–207. [Google Scholar] [CrossRef]
- Pettersson, M.; Kelk, P.; Belibasakis, G.N.; Bylund, D.; Thorén, M.M.; Johansson, A. Titanium ions form particles that activate and execute interleukin-1β release from lipopolysaccharide-primed macrophages. J. Periodontal Res. 2017, 52, 21–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hosoki, M.; Nishigawa, K.; Miyamoto, Y.; Ohe, G.; Matsuka, Y. Allergic contact dermatitis caused by titanium screws and dental implants. J. Prosthodont. Res. 2016, 60, 213–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siddiqi, A.; Payne, A.G.T.; De Silva, R.K.; Duncan, W. Titanium allergy: Could it affect dental implant integration? Clin. Oral Implant. Res. 2011, 22, 673–680. [Google Scholar] [CrossRef]
- Souza, J.G.S.; Oliveira, B.E.C.; Bertolini, M.; Lima, C.V.; Retamal-Valdes, B.; Faveri, M.; Feres, M.; Barão, V.A. Titanium particles and ions favor dysbiosis in oral biofilms. J. Periodontal Res. 2020, 55, 258–266. [Google Scholar] [CrossRef]
- Oliveira, M.N.; Schunemann, W.V.H.; Mathew, M.T.; Henriques, B.; Magini, R.S.; Teughels, W.; Souza, J.C.M. Can degradation products released from dental implants affect peri-implant tissues? J. Periodontal Res. 2018, 53, 1–11. [Google Scholar] [CrossRef]
- Chin, C.H.; Muchtar, A.; Azhari, C.H.; Razali, M.; Aboras, M. Influences of the processing method and sintering temperature on the translucency of polycrystalline yttria-stabilized tetragonal zirconia for dental applications. Ceram. Int. 2018, 44, 18641–18649. [Google Scholar] [CrossRef]
- Amat, N.F.; Muchtar, A.; Yew, H.Z.; Amril, M.S.; Muhamud, R.L. Machinability of a newly developed pre-sintered zirconia block for dental crown applications. Mater. Lett. 2020, 261. [Google Scholar] [CrossRef]
- Amat, N.F.; Muchtar, A.; Amril, M.S.; Ghazali, M.J.; Yahaya, N. Effect of sintering temperature on the aging resistance and mechanical properties of monolithic zirconia. J. Mater. Res. Technol. 2019, 8, 1092–1101. [Google Scholar] [CrossRef]
- Jemat, A.; Ghazali, M.; Razali, M.; Otsuka, Y.; Rajabi, A. Effects of TiO2 on microstructural, mechanical properties and in-vitro bioactivity of plasma sprayed yttria stabilised zirconia coatings for dental application. Ceram. Int. 2018, 44, 4271–4281. [Google Scholar] [CrossRef]
- Bagegni, A.; Abou-Ayash, S.; Rücker, G.; Algarny, A.; Att, W. The influence of prosthetic material on implant and prosthetic survival of implant-supported fixed complete dentures: A systematic review and meta-analysis. J. Prosthodont. Res. 2019, 63, 251–265. [Google Scholar] [CrossRef] [PubMed]
- Cai, H.; Chen, J.; Li, C.; Wang, J.; Wan, Q.; Liang, X. Quantitative discoloration assessment of peri-implant soft tissue around zirconia and other abutments with different colours: A systematic review and meta-analysis. J. Dent. 2018, 70, 110–117. [Google Scholar] [CrossRef] [PubMed]
- Aita, H.; Att, W.; Ueno, T.; Yamada, M.; Hori, N.; Iwasa, F.; Tsukimura, N.; Ogawa, T. Ultraviolet light-mediated photofunctionalization of titanium to promote human mesenchymal stem cell migration, attachment, proliferation and differentiation. Acta Biomater. 2009, 5, 3247–3257. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, T. Ultraviolet Photofunctionalization of Titanium Implants. Int. J. Oral Maxillofac. Implant. 2014, 29, e95–e102. [Google Scholar] [CrossRef] [Green Version]
- Yasuda, K.; Okazaki, Y.; Abe, Y.; Tsuga, K. Effective UV/Ozone irradiation method for decontamination of hydroxyapatite surfaces. Heliyon 2017, 3, e00372. [Google Scholar] [CrossRef] [Green Version]
- Att, W.; Ogawa, T. Biological aging of implant surfaces and their restoration with ultraviolet light treatment: A novel understanding of osseointegration. Int. J. Oral Maxillofac. Implant. 2012, 27, 753–761. [Google Scholar]
- Aita, H.; Hori, N.; Takeuchi, M.; Suzuki, T.; Yamada, M.; Anpo, M.; Ogawa, T. The effect of ultraviolet functionalization of titanium on integration with bone. Biomaterials 2009, 30, 1015–1025. [Google Scholar] [CrossRef]
- Sanchez-Perez, A.; Cachazo-Jiménez, C.; Sánchez-Matás, C.; Martín-De-Llano, J.J.; Davis, S.; Carda-Batalla, C. Effects of Ultraviolet Photoactivation on Osseointegration of Commercial Pure Titanium Dental Implant After 8 Weeks in a Rabbit Model. J. Oral Implant. 2020, 46, 101–107. [Google Scholar] [CrossRef]
- Dini, C.; Nagay, B.E.; Magno, M.B.; Maia, L.C.; Barão, V.A. Photofunctionalization as a suitable approach to improve the osseointegration of implants in animal models—A systematic review and meta-analysis. Clin. Oral Implant. Res. 2020, 31, 785–802. [Google Scholar] [CrossRef]
- Funato, A.; Ogawa, T. Photofunctionalized Dental Implants: A Case Series in Compromised Bone. Int. J. Oral Maxillofac. Implant. 2013, 28, 1589–1601. [Google Scholar] [CrossRef] [PubMed]
- Hirota, M.; Ozawa, T.; Iwai, T.; Ogawa, T.; Tohnai, I. Effect of Photofunctionalization on Early Implant Failure. Int. J. Oral Maxillofac. Implant. 2018, 33, 1098–1102. [Google Scholar] [CrossRef]
- Gionco, C.; Paganini, M.C.; Giamello, E.; Sacco, O.; Vaiano, V.; Sannino, D. Rare earth oxides in zirconium dioxide: How to turn a wide band gap metal oxide into a visible light active photocatalyst. J. Energy Chem. 2017, 26, 270–276. [Google Scholar] [CrossRef]
- Gionco, C.; Battiato, A.; Vittone, E.; Paganini, M.C.; Giamello, E. Structural and spectroscopic properties of high temperature prepared ZrO2–TiO2 mixed oxides. J. Solid State Chem. 2013, 201, 222–228. [Google Scholar] [CrossRef]
- Tuna, T.; Wein, M.; Swain, M.; Fischer, J.; Att, W. Influence of ultraviolet photofunctionalization on the surface characteristics of zirconia-based dental implant materials. Dent. Mater. 2015, 31, e14–e24. [Google Scholar] [CrossRef] [PubMed]
- Henningsen, A.; Smeets, R.; Heuberger, R.; Jung, O.T.; Hanken, H.; Heiland, M.; Cacaci, C.; Precht, C. Changes in surface characteristics of titanium and zirconia after surface treatment with ultraviolet light or non-thermal plasma. Eur. J. Oral Sci. 2018, 126, 126–134. [Google Scholar] [CrossRef]
- Smeets, R.; Henningsen, A.; Heuberger, R.; Hanisch, O.; Schwarz, F.; Precht, C. Influence of UV irradiation and cold atmospheric pressure plasma on zirconia surfaces: An in vitro study. Int. J. Oral Maxillofac. Implant. 2019, 34, 329–336. [Google Scholar] [CrossRef]
- Atsuta, I.; Ayukawa, Y.; Furuhashi, A.; Narimatsu, I.; Kondo, R.; Oshiro, W.; Koyano, K. Epithelial sealing effectiveness against titanium or zirconia implants surface. J. Biomed. Mater. Res. Part. A 2019, 107, 1379–1385. [Google Scholar] [CrossRef]
- Yang, Y.; Zheng, M.; Liao, Y.; Zhou, J.; Li, H.; Tan, J. Different behavior of human gingival fibroblasts on surface modified zirconia: A comparison between ultraviolet (UV) light and plasma. Dent. Mater. J. 2019, 38, 756–763. [Google Scholar] [CrossRef]
- Albrektsson, T.; Wennerberg, A. Oral implant surfaces: Part 1—Review focusing on topographic and chemical properties of different surfaces and in vivo responses to them. Int. J. Prosthodont. 2004, 17, 536–543. [Google Scholar]
- Chai, W.L.; Moharamzadeh, K.; Brook, I.M.; Emanuelsson, L.; Palmquist, A.; Van Noort, R. Development of a Novel Model for the Investigation of Implant–Soft Tissue Interface. J. Periodontol. 2010, 81, 1187–1195. [Google Scholar] [CrossRef] [PubMed]
- Korinth, G.; Schaller, K.H.; Drexler, H. Is the permeability coefficient Kp a reliable tool in percutaneous absorption studies? Arch. Toxicol. 2004, 79, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Chai, W.L.; Brook, I.M.; Palmquist, A.; Van Noort, R.; Moharamzadeh, K. The biological seal of the implant–soft tissue interface evaluated in a tissue-engineered oral mucosal model. J. R. Soc. Interface 2012, 9, 3528–3538. [Google Scholar] [CrossRef] [PubMed]
- Iglhaut, G.; Golubovic, V.; Becker, K.; Schliephake, H.; Mihatovic, I. The impact of dis-/reconnection of laser microgrooved and machined implant abutments on soft- and hard-tissue healing. Clin. Oral Implant. Res. 2012, 24, 391–397. [Google Scholar] [CrossRef] [PubMed]
- Farronato, D.; Santoro, G.; Canullo, L.; Botticelli, D.; Maiorana, C.; Lang, N.P. Establishment of the epithelial attachment and connective tissue adaptation to implants installed under the concept of “platform switching”: A histologic study in minipigs. Clin. Oral Implant. Res. 2011, 23, 90–94. [Google Scholar] [CrossRef]
- Rompen, E. The impact of the type and configuration of abutments and their (repeated) removal on the attachment level and marginal bone. Eur. J. Oral Implant. 2012, 5, 83–90. [Google Scholar]
- Razali, M.; Ngeow, W.C.; Omar, R.A.; Chai, W.L. An Integrated Overview of Ultraviolet Technology for Reversing Titanium Dental Implant Degradation: Mechanism of Reaction and Effectivity. Appl. Sci. 2020, 10, 1654. [Google Scholar] [CrossRef] [Green Version]
- Roy, M.; Pompella, A.; Kubacki, J.; Piosik, A.; Psiuk, B.; Klimontko, J.; Szade, J.; Roy, R.A.; Hedzelek, W. Photofunctionalization of dental zirconia oxide: Surface modification to improve bio-integration preserving crystal stability. Colloids Surfaces B Biointerfaces 2017, 156, 194–202. [Google Scholar] [CrossRef]
- Tuna, T.; Wein, M.; Altmann, B.; Steinberg, T.; Fischer, J.; Att, W. Effect of ultraviolet photofunctionalisation on the cell attractiveness of zirconia implant materials. Eur. Cells Mater. 2015, 29, 82–96. [Google Scholar] [CrossRef]
- Schwarz, F.; Messias, A.; Sanz-Sánchez, I.; De Albornoz, A.C.; Nicolau, P.; Taylor, T.; Beuer, F.; Schär, A.; Sader, R.; Guerra, F.; et al. Influence of implant neck and abutment characteristics on peri-implant tissue health and stability. Oral reconstruction foundation consensus report. Clin. Oral Implant. Res. 2019, 30, 588–593. [Google Scholar] [CrossRef] [Green Version]
- Sanz-Sanchez, I.; Sanz-Martín, I.; De Albornoz, A.C.; Figuero, E.; Sanz, M. Biological effect of the abutment material on the stability of peri-implant marginal bone levels: A systematic review and meta-analysis. Clin. Oral Implant. Res. 2018, 29, 124–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Furuhashi, K.; Akasaka, T.; Kitagawa, Y.; Watari, F. Evaluation of adhesion between materials and epithelium using a three-dimensional epidermal model. Nano Biomed. 2012, 4, 76–84. [Google Scholar]
- Moharamzadeh, K.; Brook, I.M.; Van Noort, R.; Scutt, A.M.; Smith, K.G.; Thornhill, M.H. Development, optimization and characterization of a full-thickness tissue engineered human oral mucosal model for biological assessment of dental biomaterials. J. Mater. Sci. Mater. Med. 2008, 19, 1793–1801. [Google Scholar] [CrossRef]
- Moharamzadeh, K.; Brook, I.; Van Noort, R.; Scutt, A.; Thornhill, M. Tissue-engineered Oral Mucosa: A Review of the Scientific Literature. J. Dent. Res. 2007, 86, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Berahim, Z.; Moharamzadeh, K.; Rawlinson, A.; Jowett, A.K. Biologic Interaction of Three-Dimensional Periodontal Fibroblast Spheroids with Collagen-Based and Synthetic Membranes. J. Periodontol. 2011, 82, 790–797. [Google Scholar] [CrossRef]
- Barker, E.; AlQobaly, L.; Shaikh, Z.; Franklin, K.; Moharamzadeh, K. Implant Soft-Tissue Attachment Using 3D Oral Mucosal Models—A Pilot Study. Dent. J. 2020, 8, 72. [Google Scholar] [CrossRef]
- Klausner, M.; Ayehunie, S.; Breyfogle, B.A.; Wertz, P.W.; Bacca, L.; Kubilus, J. Organotypic human oral tissue models for toxicological studies. Toxicol. Vitr. 2007, 21, 938–949. [Google Scholar] [CrossRef]
- Roffel, S.; Wu, G.; Nedeljkovic, I.; Meyer, M.; Razafiarison, T.; Gibbs, S. Evaluation of a novel oral mucosa in vitro implantation model for analysis of molecular interactions with dental abutment surfaces. Clin. Implant. Dent. Relat. Res. 2019, 21, 25–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jennings, L.R.; Colley, H.E.; Ong, J.; Panagakos, F.; Masters, J.G.; Trivedi, H.M.; Murdoch, C.; Whawell, S.A. Development and Characterization of In Vitro Human Oral Mucosal Equivalents Derived from Immortalized Oral Keratinocytes. Tissue Eng. Part C Methods 2016, 22, 1108–1117. [Google Scholar] [CrossRef]
- Dongari-Bagtzoglou, A.; Kashleva, H. Development of a novel three-dimensional in vitro model of oral Candida infection. Microb. Pathog. 2006, 40, 271–278. [Google Scholar] [CrossRef]
- Bierbaumer, L.; Schwarze, U.Y.; Gruber, R.; Neuhaus, W. Cell culture models of oral mucosal barriers: A review with a focus on applications, culture conditions and barrier properties. Tissue Barriers 2018, 6, 1–42. [Google Scholar] [CrossRef] [PubMed]
- Gibbs, S.; Roffel, S.; Meyer, M.; Gasser, A. Biology of soft tissue repair: Gingival epithelium in wound healing and attachment to the tooth and abutment surface. Eur. Cells Mater. 2019, 38, 63–78. [Google Scholar] [CrossRef] [PubMed]
- Beuer, F.; Schweiger, J.; Edelhoff, D. Digital dentistry: An overview of recent developments for CAD/CAM generated restorations. Br. Dent. J. 2008, 204, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Parpaiola, A.; Toia, M.; Norton, M.; Cecchinato, D.; Bressan, E.; Lops, D. CAD/CAM Implant Abutments: Peri-implant Hard and Soft Tissue Response with Up to 4 Years of Follow-up— A Retrospective Cohort Study Evaluation. Int. J. Periodontics Restor. Dent. 2020, 40, 193–201. [Google Scholar] [CrossRef]
- Alao, A.-R.; Stoll, R.; Song, X.-F.; Miyazaki, T.; Hotta, Y.; Shibata, Y.; Yin, L. Surface quality of yttria-stabilized tetragonal zirconia polycrystal in CAD/CAM milling, sintering, polishing and sandblasting processes. J. Mech. Behav. Biomed. Mater. 2017, 65, 102–116. [Google Scholar] [CrossRef]
- Bertolini, M.; Kempen, J.; Lourenço, E.J.V.; Telles, D. The use of CAD/CAM technology to fabricate a custom ceramic implant abutment: A clinical report. J. Prosthet. Dent. 2014, 111, 362–366. [Google Scholar] [CrossRef]
- Karl, M.; Irastorza-Landa, A. In Vitro Characterization of Original and Nonoriginal Implant Abutments. Int. J. Oral Maxillofac. Implant. 2018, 33, 1229–1239. [Google Scholar] [CrossRef]
- Gigandet, M.; Bigolin, G.; Faoro, F.; Bürgin, W.B.; Brägger, U. Implants with Original and Non-Original Abutment Connections. Clin. Implant. Dent. Relat. Res. 2014, 16, 303–311. [Google Scholar] [CrossRef]
- Kim, H.S.; Lee, J.I.; Yang, S.S.; Kim, B.S.; Kim, B.C.; Lee, J. The effect of alendronate soaking and ultraviolet treatment on bone-implant interface. Clin. Oral Implant. Res. 2016, 28, 1164–1172. [Google Scholar] [CrossRef]
- Lee, J.-B.; Jo, Y.-H.; Choi, J.Y.; Seol, Y.-J.; Lee, Y.-M.; Ku, Y.; Rhyu, I.-C.; Yeo, I.-S.L. The Effect of Ultraviolet Photofunctionalization on a Titanium Dental Implant with Machined Surface: An In Vitro and In Vivo Study. Materials 2019, 12, 2078. [Google Scholar] [CrossRef] [Green Version]
- Chai, W.L.; Moharamzadeh, K.; Van Noort, R.; Emanuelsson, L.; Palmquist, A.; Brook, I.M. Contour analysis of an implant-soft tissue interface. J. Periodontal Res. 2013, 48, 663–670. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Materials | Components and Composition by Weight% | Mean Surface Roughness (Sa Value ± SD) (nm) | p-Value |
|---|---|---|---|
| Commercially pure titanium (CPTi) | TiO2 | 212.05 ± 43.91 | 0.115 * |
| Yttria-stabilized zirconia (YSZ) | ZrO2/Y2O3 ≤94%/5.5% | 246.48 ± 27.04 | |
| Alumina-toughened zirconia (ATZ) | ZrO2/Al2O3/Y2O3 76%/20%/4% | 256.65 ± 35.59 |
| Materials | Mean Percentage of the Amount of Radioactivity that Passed through the Interface (% ± SD) | |
|---|---|---|
| Nontreated Surface (N-Tx) | UV-Treated Surface (UV-Tx) | |
| Commercially pure titanium (CPTi) | 1.866 ± 0.217 | 1.522 ± 0.201 |
| Yttria-stabilized zirconia (YSZ) | 1.660 ± 0.017 | 1.152 ± 0.007 |
| Alumina-toughened zirconia (ATZ) | 1.945 ± 0.0137 | 1.187 ± 0.005 |
| p value | 0.002 # | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Razali, M.; Ngeow, W.C.; Omar, R.A.; Chai, W.L. An In-Vitro Analysis of Peri-Implant Mucosal Seal Following Photofunctionalization of Zirconia Abutment Materials. Biomedicines 2021, 9, 78. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines9010078
Razali M, Ngeow WC, Omar RA, Chai WL. An In-Vitro Analysis of Peri-Implant Mucosal Seal Following Photofunctionalization of Zirconia Abutment Materials. Biomedicines. 2021; 9(1):78. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines9010078
Chicago/Turabian StyleRazali, Masfueh, Wei Cheong Ngeow, Ros Anita Omar, and Wen Lin Chai. 2021. "An In-Vitro Analysis of Peri-Implant Mucosal Seal Following Photofunctionalization of Zirconia Abutment Materials" Biomedicines 9, no. 1: 78. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines9010078