Social Functioning of Childhood Cancer Survivors after Computerized Cognitive Training: A Randomized Controlled Trial

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Measures
2.4. Statistical Analyses
3. Results
3.1. Participants
3.2. Prior Cognitive Findings
3.3. Baseline Social Functioning
3.4. Post-Intervention Acute Change in Social Functioning
3.5. Post-Intervention Maintenance of Change in Social Functioning
3.6. Patterns of Social Functioning by Acute Lymphoblastic Leukemia vs. Brain Tumor Diagnoses
4. Discussion
4.1. Study Limitations
4.2. Clinical Implications
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed]
- Krull, K.R.; Hardy, K.K.; Kahalley, L.S.; Schuitema, I.; Kesler, S.R. Neurocognitive outcomes and interventions in long-term survivors of childhood cancer. J. Clin. Oncol. 2018, 36, 2181–2189. [Google Scholar] [CrossRef] [PubMed]
- Kahalley, L.S.; Conklin, H.M.; Tyc, V.L.; Hudson, M.M.; Wilson, S.J.; Wu, S.; Xiong, X.; Hinds, P.S. Slower processing speed after treatment for pediatric brain tumor and acute lymphoblastic leukemia. Psychooncology 2013, 22, 1979–1986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conklin, H.M.; Ashford, J.M.; Howarth, R.A.; Merchant, T.E.; Ogg, R.J.; Santana, V.M.; Reddick, W.E.; Wu, S.; Xiong, X. Working memory performance among childhood brain tumor survivors. J. Int. Neuropsychol. Soc. 2012, 18, 996–1005. [Google Scholar] [CrossRef] [PubMed]
- Maddrey, A.M.; Bergeron, J.A.; Lombardo, E.R.; McDonald, N.K.; Mulne, A.F.; Barenberg, P.D.; Bowers, D.C. Neuropsychological performance and quality of life of 10 year survivors of childhood medulloblastoma. J. Neurooncol. 2005, 72, 245–253. [Google Scholar] [CrossRef] [PubMed]
- Schulte, F.; Barrera, M. Social competence in childhood brain tumor survivors: A comprehensive review. Support. Care Cancer 2010, 18, 1499–1513. [Google Scholar] [CrossRef] [PubMed]
- Hocking, M.C.; McCurdy, M.; Turner, E.; Kazak, A.E.; Noll, R.B.; Phillips, P.; Barakat, L.P. Social competence in pediatric brain tumor survivors: Application of a model from social neuroscience and developmental psychology. Pediatr. Blood Cancer 2015, 62, 375–384. [Google Scholar] [CrossRef]
- Armstrong, G.T.; Liu, Q.; Yasui, Y.; Huang, S.; Ness, K.K.; Leisenring, W.; Hudson, M.M.; Donaldson, S.S.; King, A.A.; Stovall, M.; et al. Long-term outcomes among adult survivors of childhood central nervous system malignancies in the childhood cancer survivor study. J. Natl. Cancer Inst. 2009, 101, 946–958. [Google Scholar] [CrossRef]
- Gurney, J.G.; Krull, K.R.; Kadan-Lottick, N.; Nicholson, H.S.; Nathan, P.C.; Zebrack, B.; Tersak, J.M.; Ness, K.K. Social outcomes in the childhood cancer survivor study cohort. J. Clin. Oncol. 2009, 27, 2390–2395. [Google Scholar] [CrossRef]
- Brinkman, T.M.; Krasin, M.J.; Liu, W.; Armstrong, G.T.; Ojha, R.P.; Sadighi, Z.S.; Gupta, P.; Kimberg, C.; Srivastava, D.; Merchant, T.E.; et al. Long-term neurocognitive functioning and social attainment in adult survivors of pediatric CNS tumors: Results from the St Jude lifetime cohort study. J. Clin. Oncol. 2016, 34, 1358–1367. [Google Scholar] [CrossRef]
- Tremolada, M.; Bonichini, S.; Taverna, L.; Basso, G.; Pillon, M. Self-esteem and academic difficulties in preadolescents and adolescents healed from paediatric leukaemia. Cancers 2017, 9, 55. [Google Scholar] [CrossRef] [PubMed]
- Sleurs, C.; Lemiere, J.; Vercruysse, T.; Nolf, N.; Van Calster, B.; Deprez, S.; Renard, M.; Vandecruys, E.; Benoit, Y.; Uyttebroeck, A. Intellectual development of childhood ALL patients: A multicenter longitudinal study. Psychooncology 2017, 26, 508–514. [Google Scholar] [CrossRef] [PubMed]
- Duffner, P.K. Risk factors for cognitive decline in children treated for brain tumors. Eur. J. Paediatr. Neurol. 2010, 14, 106–115. [Google Scholar] [CrossRef] [PubMed]
- Ellenberg, L.; Liu, Q.; Gioia, G.; Yasui, Y.; Packer, R.J.; Mertens, A.; Donaldson, S.S.; Stovall, M.; Kadan-Lottick, N.; Armstrong, G.; et al. Neurocognitive status in long-term survivors of childhood CNS malignancies: A report from the childhood cancer survivor study. Neuropsychology 2009, 23, 705–717. [Google Scholar] [CrossRef] [PubMed]
- Moore, B.D. Neurocognitive outcomes in survivors of childhood cancer. J. Pediatr. Psychol. 2005, 30, 51–63. [Google Scholar] [CrossRef] [PubMed]
- Anderson, F.S.; Kunin-Batson, A.S. Neurocognitive late effects of chemotherapy in children: The past 10 years of research on brain structure and function. Pediatr. Blood Cancer 2009, 52, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Iyer, N.S.; Balsamo, L.M.; Bracken, M.B.; Kadan-Lottick, N.S. Chemotherapy-only treatment effects on long-term neurocognitive functioning in childhood ALL survivors: A review and meta-analysis. Blood 2015, 126, 346–353. [Google Scholar] [CrossRef]
- Mabbott, D.J.; Spiegler, B.J.; Greenberg, M.L.; Rutka, J.T.; Hyder, D.J.; Bouffet, E. Serial evaluation of academic and behavioral outcome after treatment with cranial radiation in childhood. J. Clin. Oncol. 2005, 23, 2256–2263. [Google Scholar] [CrossRef]
- Castellino, S.M.; Ullrich, N.J.; Whelen, M.J.; Lange, B.J. Developing interventions for cancer-related cognitive dysfunction in childhood cancer survivors. J. Natl. Cancer Inst. 2014, 106, dju186. [Google Scholar] [CrossRef]
- Vannatta, K.; Gerhardt, C.A.; Wells, R.J.; Noll, R.B. Intensity of CNS treatment for pediatric cancer: Prediction of social outcomes in survivors. Pediatr. Blood Cancer 2007, 49, 716–722. [Google Scholar] [CrossRef]
- Aukema, E.J.; Caan, M.W.; Oudhuis, N.; Majoie, C.B.; Vos, F.M.; Reneman, L.; Last, B.F.; Grootenhuis, M.A.; Schouten-van Meeteren, A.Y.N. White matter fractional anisotropy correlates with speed of processing and motor speed in young childhood cancer survivors. Int. J. Radiat. Oncol. Biol. Phys. 2009, 74, 837–843. [Google Scholar] [CrossRef]
- Reddick, W.E.; White, H.A.; Glass, J.O.; Wheeler, G.C.; Thompson, S.J.; Gajjar, A.; Leigh, L.; Mulhern, R.K. Developmental model relating white matter volume to neurocognitive deficits in pediatric brain tumor survivors. Cancer 2003, 97, 2512–2519. [Google Scholar] [CrossRef]
- Tonning, O.; Perrin, S.; Lundgren, J.; Hjorth, L.; Johanson, A. Long-term cognitive sequelae after pediatric brain tumor related to medical risk factors, age, and sex. Pediatr. Neurol. 2014, 51, 515–521. [Google Scholar] [CrossRef]
- Emond, A.; Edwards, L.; Peacock, S.; Norman, C.; Evangeli, M. Social competence in children and young people treated for a brain tumour. Support. Care Cancer 2016, 24, 4587–4595. [Google Scholar] [CrossRef]
- Kok, T.B.; Post, W.J.; Tucha, O.L.; de Bont, E.S.; Kamps, W.A.; Kingma, A. Social competence in children with brain disorders: A meta-analytic review. Neuropsychol. Rev. 2014, 24, 219–235. [Google Scholar] [CrossRef]
- Moyer, K.H.; Willard, V.W.; Gross, A.M.; Netson, K.L.; Ashford, J.M.; Kahalley, L.S.; Wu, S.; Xiong, X.; Conklin, H.M. The impact of attention on social functioning in survivors of pediatric acute lymphoblastic leukemia and brain tumors. Pediatr. Blood Cancer 2012, 59, 1290–1295. [Google Scholar] [CrossRef] [Green Version]
- Bonner, M.J.; Hardy, K.K.; Willard, V.W.; Anthony, K.K.; Hood, M.; Gururangan, S. Social functioning and facial expression recognition in survivors of pediatric brain tumors. J. Pediatr. Psychol. 2008, 33, 1142–1152. [Google Scholar] [CrossRef]
- Willard, V.W.; Allen, T.M.; Hardy, K.K.; Bonner, M.J. Social functioning in survivors of pediatric brain tumors: Contribution of neurocognitive and social-cognitive skills. Child Health Care 2017, 46, 181–195. [Google Scholar] [CrossRef]
- Riggs, N.R.; Jahromi, L.B.; Razza, R.P.; Dillworth-Bart, J.E.; Mueller, U. Executive function and the promotion of social–emotional competence. J. Appl. Dev. Psychol. 2006, 27, 300–309. [Google Scholar] [CrossRef]
- Willard, V.W. Social skills interventions for survivors of pediatric brain tumors: A review and reformulation. Pediatr. Blood Cancer 2018, 65, e27434. [Google Scholar] [CrossRef]
- Conklin, H.M.; Reddick, W.E.; Ashford, J.; Ogg, S.; Howard, S.C.; Morris, E.B.; Brown, R.; Bonner, M.; Christensen, R.; Wu, S.; et al. Long-Term efficacy of methylphenidate in enhancing attention regulation, social skills, and academic abilities of childhood cancer survivors. J. Clin. Oncol. 2010, 28, 4465–4472. [Google Scholar] [CrossRef]
- Conklin, H.M.; Ashford, J.M.; Clark, K.N.; Martin-Elbahesh, K.; Hardy, K.K.; Merchant, T.E.; Ogg, R.J.; Jeha, S.; Huang, L.; Zhang, H. Long-term efficacy of computerized cognitive training among survivors of childhood cancer: A single-blind randomized controlled trial. J. Pediatr. Psychol. 2016, 42, 220–231. [Google Scholar] [CrossRef]
- Klingberg, T.; Fernell, E.; Olesen, P.J.; Johnson, M.; Gustafsson, P.; Dahlström, K.; Gillberg, C.G.; Forssberg, H.; Westerberg, H. Computerized training of working memory in children with ADHD-a randomized, controlled trial. J. Am. Acad. Child Adolesc. Psychiatry 2005, 44, 177–186. [Google Scholar] [CrossRef]
- Weicker, J.; Villringer, A.; Thöne-Otto, A.; Brown, G.G. Can impaired working memory functioning be improved by training? A meta-analysis with a special focus on brain injured patients. Neuropsychology 2016, 30, 190. [Google Scholar] [CrossRef]
- Hardy, K.K.; Willard, V.W.; Allen, T.M.; Bonner, M.J. Working memory training in survivors of pediatric cancer: A randomized pilot study. Psychooncology 2013, 22, 1856–1865. [Google Scholar] [CrossRef]
- Cox, L.E.; Ashford, J.M.; Clark, K.N.; Martin-Elbahesh, K.; Hardy, K.K.; Merchant, T.E.; Ogg, R.J.; Jeha, S.; Willard, V.W.; Huang, L.; et al. Feasibility and acceptability of a remotely administered computerized intervention to address cognitive late effects among childhood cancer survivors. Neurooncol. Pract. 2015, 2, 78–87. [Google Scholar] [CrossRef] [Green Version]
- Conklin, H.M.; Ogg, R.J.; Ashford, J.M.; Scoggins, M.A.; Zou, P.; Clark, K.N.; Martin-Elbahesh, K.; Merchant, T.E.; Jeha, S.; Huang, L.; et al. Computerized cognitive training for amelioration of cognitive late effects among childhood cancer survivors: A randomized controlled trial. J. Clin. Oncol. 2015, 33, 3894–3902. [Google Scholar] [CrossRef]
- Wechsler, D. Wechsler Intelligence Scale for Children, 4th ed.; Pearson Corporation: San Antonio, TX, USA, 2004. [Google Scholar]
- Wechsler, D. Wechsler Abbreviated Scale of Intelligence; Harcourt Assessment: San Antonio, TX, USA, 1999. [Google Scholar]
- Conners, C.K. Conners’ Rating Scales, 3rd ed.; Multi-Health Systems, Incorporated: Toronto, ON, Canada, 2008. [Google Scholar]
- Noll, R.B.; Bukowski, W.B. Commentary: Social competence in children with chronic illness: The devil is in the details. J. Pediatr. Psychol. 2012, 37, 959–966. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Intervention n = 34 | Control n = 34 | p | |||
|---|---|---|---|---|---|
| Demographic | Gender | Female | 16 (47%) | 16 (47%) | 1.00 |
| Male | 18 (53%) | 18 (53%) | |||
| Race/Ethnicity | African American | 1 (3%) | 5 (15%) | 0.39 | |
| Asian/Pacific Islander | 1 (3%) | 1 (3%) | |||
| Caucasian | 27 (79%) | 26 (76%) | |||
| Hispanic | 2 (6%) | 1 (3%) | |||
| Other/Multiple Races | 3 (9%) | 1 (3%) | |||
| SES (BSMSS) 1 | 39.68 ± 15.37 | 40.46 ± 12.20 | 0.82 | ||
| Clinical | ALL 2 | 23 (68%) | 24 (71%) | 1.00 | |
| Brain Tumor | 11 (32%) | 10 (29%) | 0.33 | ||
| Ependymoma | 1 (9%) | 3 (30%) | |||
| Glioma | 2 (18%) | 0 (0%) | |||
| Medulloblastoma/PNET | 8 (73%) | 7 (70%) | |||
| Age at Diagnosis (years) | 5.15 ± 2.92 | 4.62 ± 2.68 | 0.43 | ||
| Age at Testing (years) | 12.21 ± 2.47 | 11.82 ± 2.42 | 0.51 | ||
| Time since Treatment (years) | 4.97 ± 3.02 | 5.04 ± 2.41 | 0.91 | ||
| Treatment Group | Chemo 3 Only | 20 (59%) | 22 (65%) | 0.95 | |
| CSI 4 w/or w/o Chemo 3 | 8 (24%) | 7 (21%) | |||
| CRT 5 w/or w/o Chemo 3 | 3 (9%) | 3 (9%) | |||
| Chemo 3 + BMT 6 w/or w/o TBI 7 | 3 (9%) | 2 (6%) | |||
| WASI IQ 8 (Standard Score) | 106.90 ± 15.74 | 99.85 ± 14.01 | 0.06 |
| Mean ± SEM 1 | ||||||
|---|---|---|---|---|---|---|
| Intervention | Control | |||||
| Cognitive Outcome | Baseline | Immediate Post | Six-Months Post | Baseline | Immediate Post | Six-Months Post |
| WISC-IV 2 Digit Span Forward 5 | 9.00 ± 0.46 | 9.93 ± 0.53 | 10.23 ± 0.56 | 8.11 ± 0.54 | 8.95 ± 0.54 | 8.84 ± 0.55 |
| WISC-IV 2 Digit Span Backward 5 | 8.97 ± 0.51 | 11.17 ± 0.56 | 10.53 ± 0.54 | 8.58 ± 0.52 | 9.21 ± 0.52 | 9.37 ± 0.53 |
| WISC-IV 2 WMI 3,5 | 95.33 ± 2.32 | 104.50 ± 2.25 | 103.37 ± 2.39 | 92.50 ± 2.52 | 96.47 ± 2.85 | 95.97 ± 2.40 |
| WISC-IV 2 Spatial Span Forward 5 | 9.83 ± 0.61 | 13.13 ± 0.64 | 11.63 ± 0.57 | 8.56 ± 0.55 | 9.81 ± 0.55 | 9.97 ± 0.56 |
| WISC-IV 2 Spatial Span Backward 5 | 9.50 ± 0.61 | 12.63 ± 0.55 | 12.60 ± 0.51 | 10.03 ± 0.49 | 10.789 ± 0.49 | 10.81 ± 0.50 |
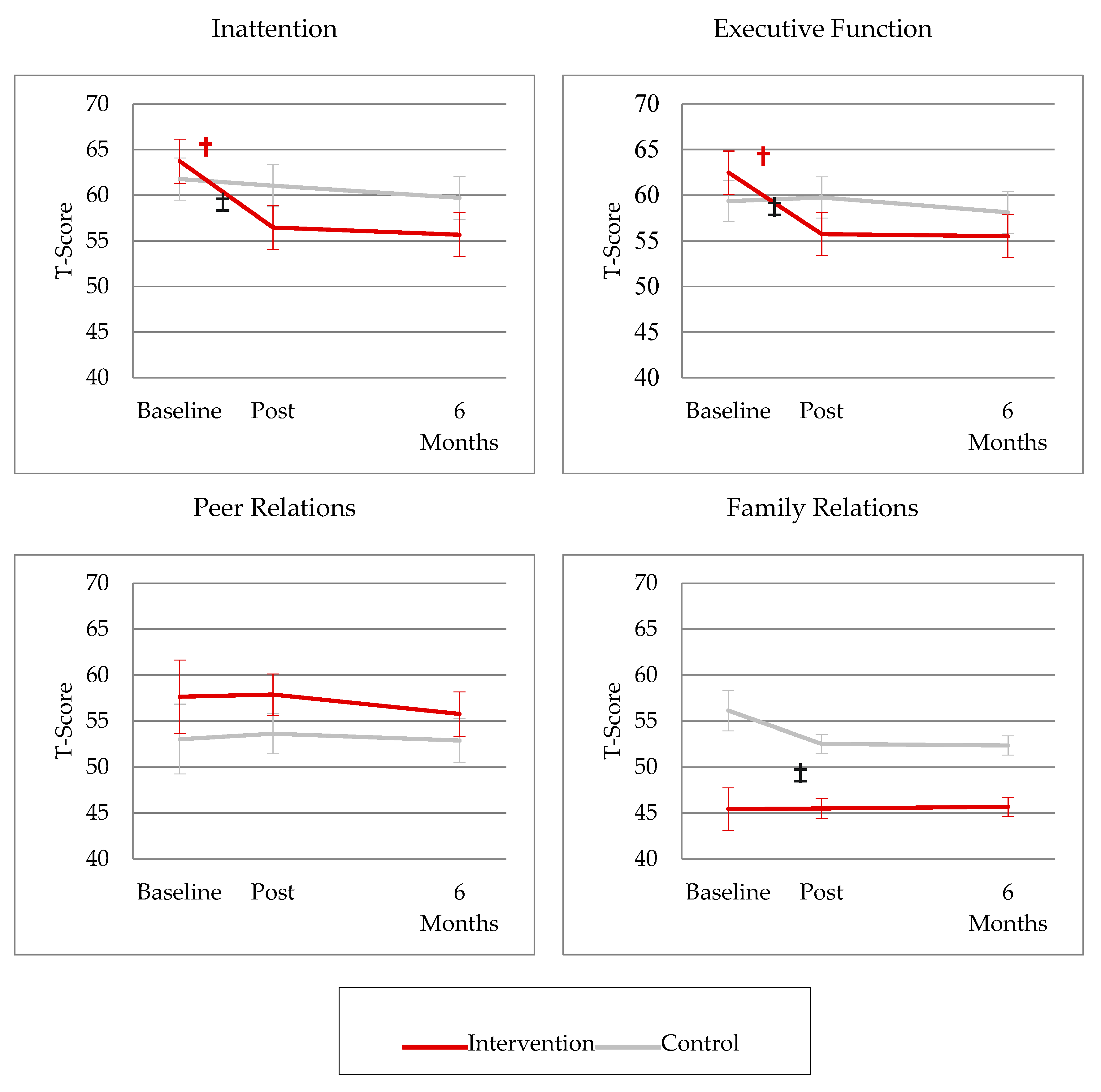
| Conners 3 Parent—Inattention 6 | 63.73 ± 2.53 | 59.47 ± 1.39 | 55.67 ± 2.42 | 61.77 ± 2.32 | 61.05 ± 2.32 | 59.72 ± 2.35 |
| Conners 3 Parent—EF 4,6 | 62.47 ± 2.43 | 55.73 ± 1.57 | 55.50 ± 2.36 | 59.33 ± 2.26 | 59.74 ± 2.26 | 58.12 ± 2.29 |
| Social Functioning Outcome | Baseline | Immediate Post | Six-Months | Baseline | Immediate Post | Six-Months Post |
| Conners 3 Parent—Peer Relations 6 | 57.63 ± 4.00 | 57.87 ± 2.27 | 55.77 ± 2.39 | 53.04 ± 3.79 | 53.61 ± 2.18 | 52.90 ± 2.40 |
| Conners 3 Self—Family Relations 6 | 45.43 ± 2.31 | 45.50 ± 1.10 | 45.68 ± 1.05 | 56.13 ± 2.18 | 52.53 ± 1.06 | 52.36 ± 1.05 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mendoza, L.K.; Ashford, J.M.; Willard, V.W.; Clark, K.N.; Martin-Elbahesh, K.; Hardy, K.K.; Merchant, T.E.; Jeha, S.; Wang, F.; Zhang, H.; et al. Social Functioning of Childhood Cancer Survivors after Computerized Cognitive Training: A Randomized Controlled Trial. Children 2019, 6, 105. https://0-doi-org.brum.beds.ac.uk/10.3390/children6100105
Mendoza LK, Ashford JM, Willard VW, Clark KN, Martin-Elbahesh K, Hardy KK, Merchant TE, Jeha S, Wang F, Zhang H, et al. Social Functioning of Childhood Cancer Survivors after Computerized Cognitive Training: A Randomized Controlled Trial. Children. 2019; 6(10):105. https://0-doi-org.brum.beds.ac.uk/10.3390/children6100105
Chicago/Turabian StyleMendoza, Leanne K., Jason M. Ashford, Victoria W. Willard, Kellie N. Clark, Karen Martin-Elbahesh, Kristina K. Hardy, Thomas E. Merchant, Sima Jeha, Fang Wang, Hui Zhang, and et al. 2019. "Social Functioning of Childhood Cancer Survivors after Computerized Cognitive Training: A Randomized Controlled Trial" Children 6, no. 10: 105. https://0-doi-org.brum.beds.ac.uk/10.3390/children6100105