Short- and Long-Term Neurodevelopmental Outcomes of Very Preterm Infants with Neonatal Sepsis: A Systematic Review and Meta-Analysis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search Strategy
2.2. Study Selection Criteria
2.3. Data Extraction
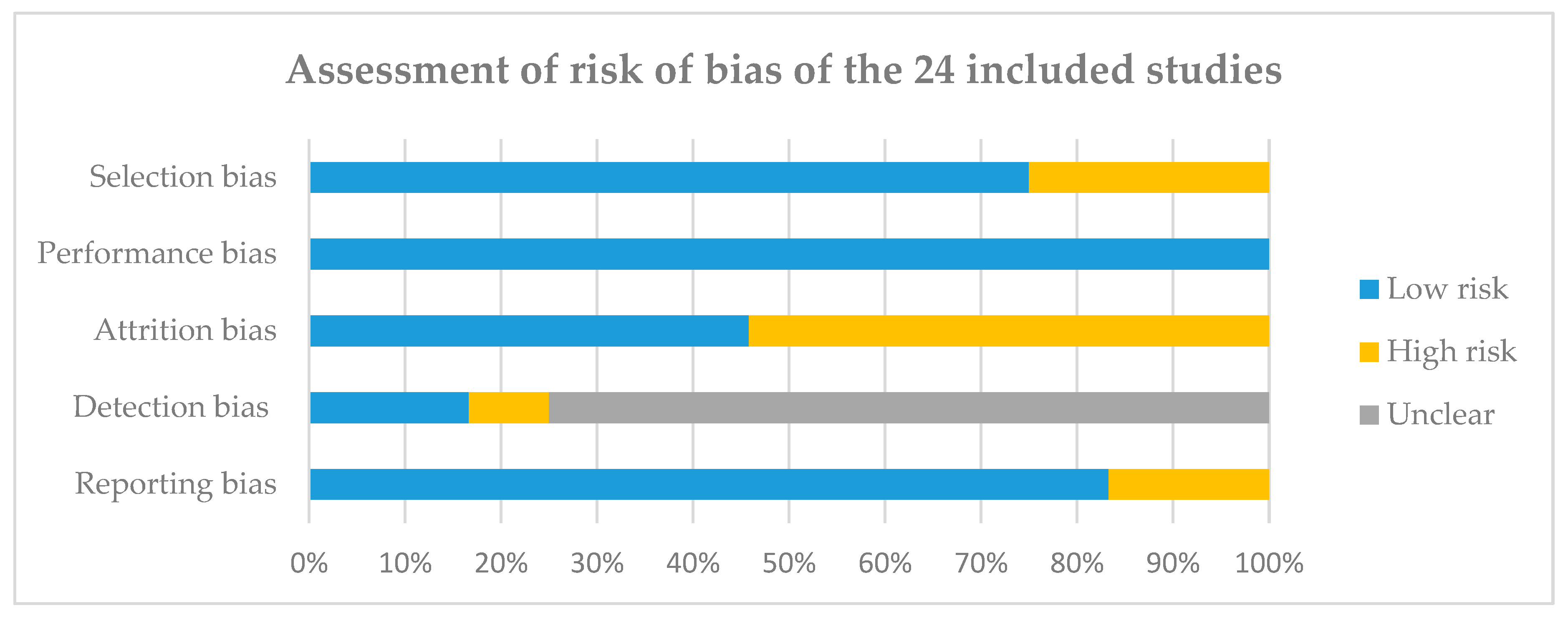
2.4. Assess Risk of Bias in Individual Studies
2.5. Data Synthesis and Analysis
3. Results
3.1. Study Selection
3.2. Study Characteristics
3.3. Risk of Bias within Studies
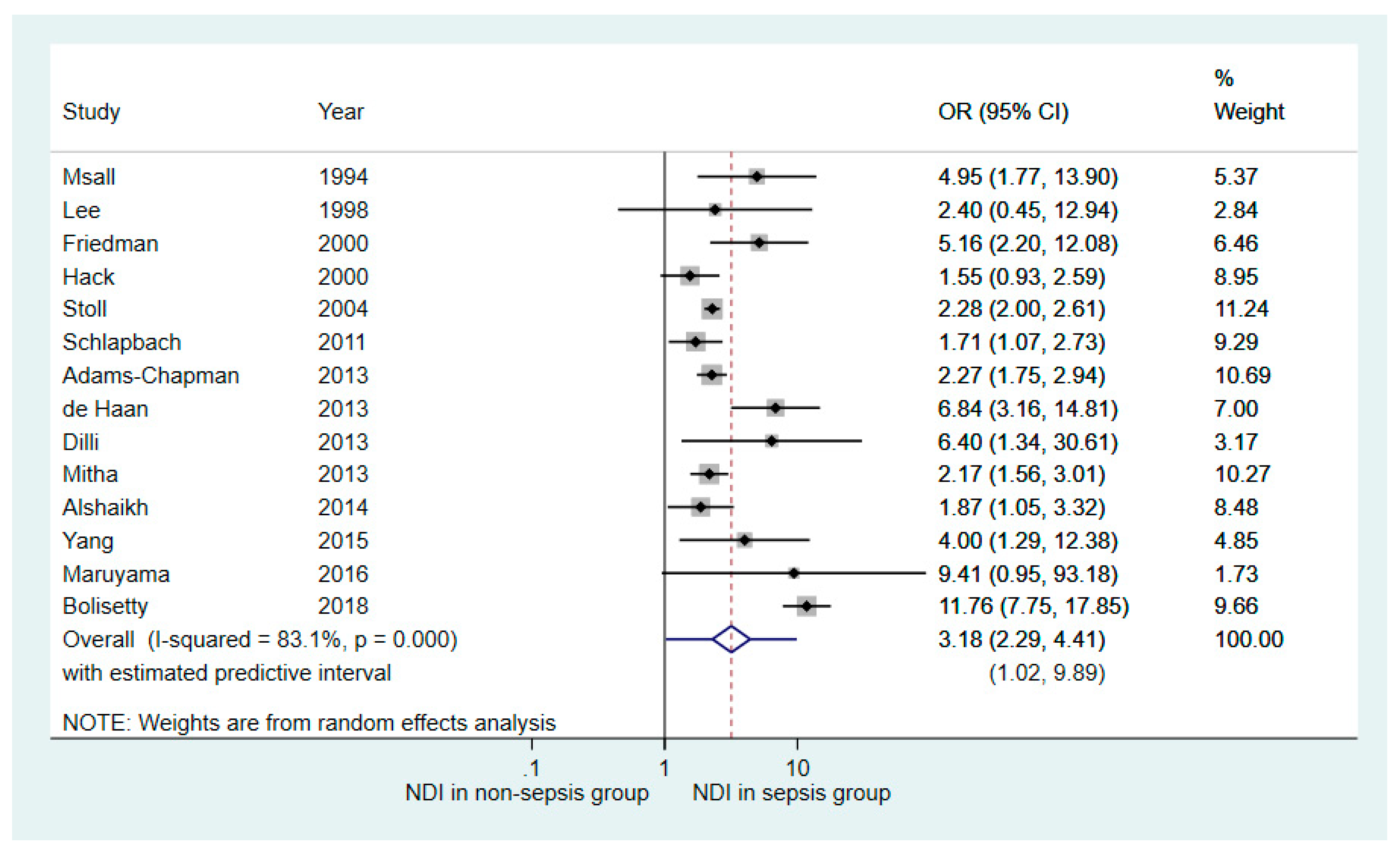
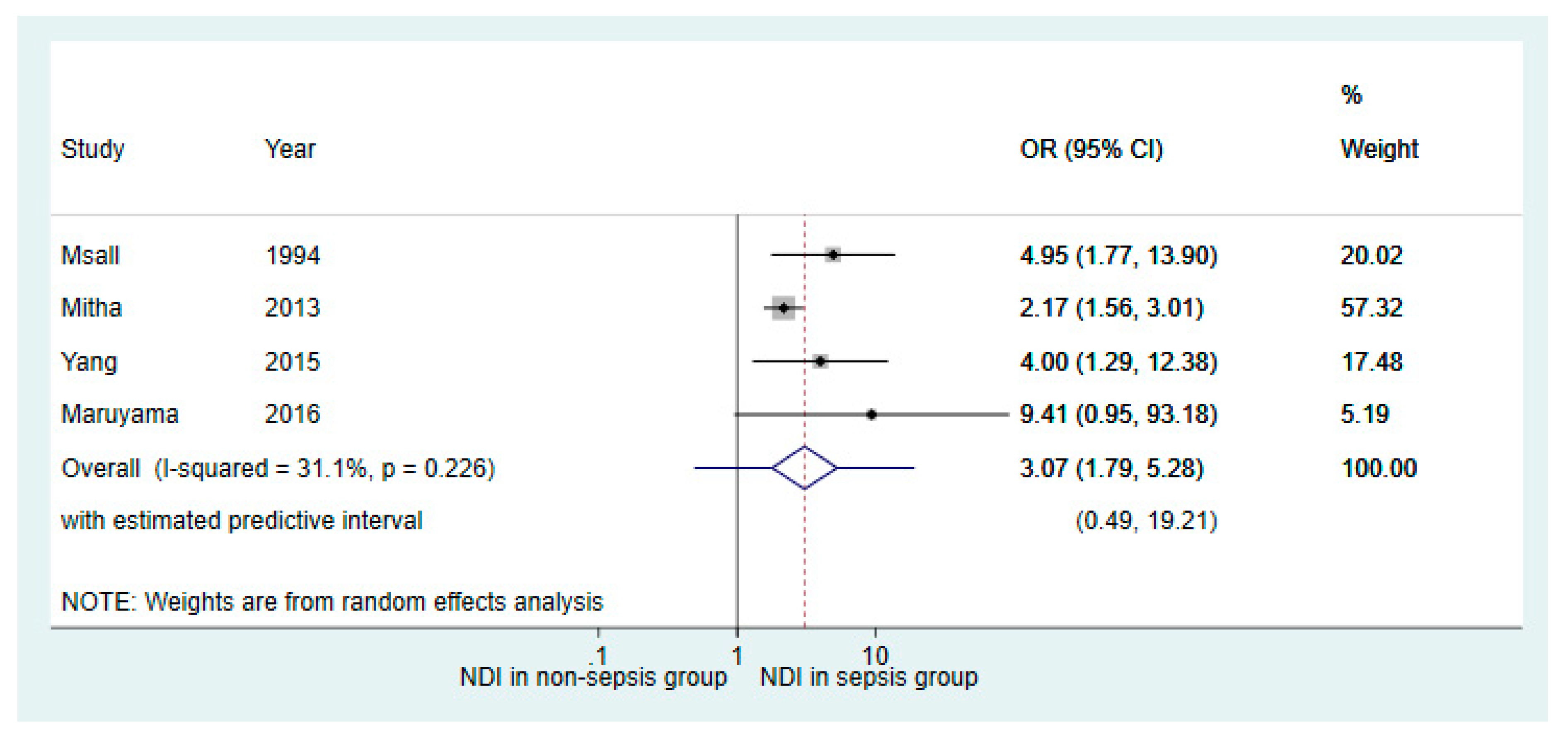
3.4. Quantitative Synthesis
3.5. Qualitative Synthesis
3.5.1. Studies Reporting Dichotomised Outcomes
3.5.2. Studies Reporting Continuous Outcomes
4. Discussion
4.1. Study Designs
4.2. Population
4.3. Assessment of Sepsis
4.4. Assessment of Outcomes
4.5. Review Limitations
4.6. Recommendations for Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Shane, A.L.; Sanchez, P.J.; Stoll, B.J. Neonatal sepsis. Lancet 2017, 390, 1770–1780. [Google Scholar] [CrossRef]
- Shah, B.A.; Padbury, J.F. Neonatal sepsis: An old problem with new insights. Virulence 2014, 5, 170–178. [Google Scholar] [CrossRef] [PubMed]
- McCormick, M.C. The contribution of low birth weight to infant mortality and childhood morbidity. N. Engl. J. Med. 1985, 312, 82–90. [Google Scholar] [CrossRef] [PubMed]
- Wynn, J.L. Defining neonatal sepsis. Curr. Opin. Pediatr. 2016, 28, 135–140. [Google Scholar] [CrossRef]
- Boghossian, N.S.; Page, G.P.; Bell, E.F.; Stoll, B.J.; Murray, J.C.; Cotten, C.M.; Shankaran, S.; Walsh, M.C.; Laptook, A.R.; Newman, N.S.; et al. Late-onset sepsis in very low birth weight infants from singleton and multiple-gestation births. J. Pediatr. 2013, 162, 1120–1124. [Google Scholar] [CrossRef] [PubMed]
- Regev, R.H.; Arnon, S.; Litmanovitz, I.; Bauer-Rusek, S.; Boyko, V.; Lerner-Geva, L.; Reichman, B.; Israel Neonatal, N. Association between neonatal morbidities and head growth from birth until discharge in very-low-birthweight infants born preterm: A population-based study. Dev. Med. Child Neurol. 2016, 58, 1159–1166. [Google Scholar] [CrossRef]
- Adams-Chapman, I.; Stoll, B.J. Neonatal infection and long-term neurodevelopmental outcome in the preterm infant. Curr. Opin. Infect. Dis. 2006, 19, 290–297. [Google Scholar] [CrossRef]
- Khwaja, O.; Volpe, J.J. Pathogenesis of cerebral white matter injury of prematurity. Arch. Dis. Child. Fetal Neonatal Ed. 2008, 93, F153–F161. [Google Scholar] [CrossRef]
- Volpe, J.J. Postnatal sepsis, necrotizing entercolitis, and the critical role of systemic inflammation in white matter injury in premature infants. J. Pediatr. 2008, 153, 160–163. [Google Scholar] [CrossRef]
- Alshaikh, B.; Yusuf, K.; Sauve, R. Neurodevelopmental outcomes of very low birth weight infants with neonatal sepsis: Systematic review and meta-analysis. J. Perinatol. 2013, 33, 558–564. [Google Scholar] [CrossRef]
- Cochrane Handbook for Systematic Reviews of Interventions. Available online: www.handbook.cochrane.org (accessed on 10 November 2019).
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Kontopantelis, E.; Reeves, D. metaan: Random-effects meta-analysis. Stata J. 2010, 10, 395–407. [Google Scholar] [CrossRef]
- Chaimani, A.; Mavridis, D.; Salanti, G. A hands-on practical tutorial on performing meta-analysis with Stata. Evid. Based Ment. Health 2014, 17, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Mantel, N.; Haenszel, W. Statistical aspects of the analysis of data from retrospective studies of disease. J. Natl. Cancer Inst. 1959, 22, 719–748. [Google Scholar]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. Br. Med. J. 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Riley, R.D.; Higgins, J.P.; Deeks, J.J. Interpretation of random effects meta-analyses. Br. Med. J. 2011, 342, d549. [Google Scholar] [CrossRef]
- Peters, J.L.; Sutton, A.J.; Jones, D.R.; Abrams, K.R.; Rushton, L. Contour-enhanced meta-analysis funnel plots help distinguish publication bias from other causes of asymmetry. J. Clin. Epidemiol. 2008, 61, 991–996. [Google Scholar] [CrossRef]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. Br. Med. J. 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Paul, V.K.; Radhika, S.; Deorari, A.K.; Singh, M. Neurodevelopmental outcome of ‘at risk’ nursery graduates. Indian J. Pediatr. 1998, 65, 857–862. [Google Scholar] [CrossRef]
- Wheater, M.; Rennie, J.M. Perinatal infection is an important risk factor for cerebral palsy in very-low-birthweight infants. Dev. Med. Child Neurol. 2000, 42, 364–367. [Google Scholar] [CrossRef]
- McGrath, M.; Sullivan, M. Birth weight, neonatal morbidities, and school age outcomes in full-term and preterm infants. Issues Compr. Pediatr. Nurs. 2002, 25, 231–254. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, D.K., Jr.; Stoll, B.J.; Fanaroff, A.A.; McDonald, S.A.; Oh, W.; Higgins, R.D.; Duara, S.; Poole, K.; Laptook, A.; Goldberg, R.; et al. Neonatal candidiasis among extremely low birth weight infants: Risk factors, mortality rates, and neurodevelopmental outcomes at 18 to 22 months. Pediatrics 2006, 117, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Addison, K.; Griffin, M.P.; Moorman, J.R.; Lake, D.E.; O’Shea, T.M. Heart rate characteristics and neurodevelopmental outcome in very low birth weight infants. J. Perinatol. 2009, 29, 750–756. [Google Scholar] [CrossRef] [PubMed]
- Kiechl-Kohlendorfer, U.; Ralser, E.; Pupp Peglow, U.; Reiter, G.; Trawoger, R. Adverse neurodevelopmental outcome in preterm infants: Risk factor profiles for different gestational ages. Acta Paediatr. 2009, 98, 792–796. [Google Scholar] [CrossRef]
- Mercier, C.E.; Dunn, M.S.; Ferrelli, K.R.; Howard, D.B.; Soll, R.F. Neurodevelopmental outcome of extremely low birth weight infants from the vermont oxford network: 1998–2003 and the Vermont Oxford Network ELBW infant follow-up study group. Neonatology 2010, 97, 329–338. [Google Scholar] [CrossRef]
- Gocer, C.; Kavuncuoglu, S.; Arslan, G.; Ertem, L.; Ozbek, S.; Ozturegen, E.; Akin, M.A.; Baysoy, N. Neurodevelopmental problems of very low birth weight premature infants and factors affecting neurological morbidity. Turk. Arch. Pediatr. 2011, 46, 207–214. [Google Scholar] [CrossRef]
- Schlapbach, L.J.; Adams, M.; Proietti, E.; Aebischer, M.; Grunt, S.; Borradori-Tolsa, C.; Bickle-Graz, M.; Bucher, H.U.; Latal, B.; Natalucci, G. Outcome at two years of age in a Swiss national cohort of extremely preterm infants born between 2000 and 2008. BMC Pediatr. 2012, 12. [Google Scholar] [CrossRef]
- Barton, M.; O’Brien, K.; Robinson, J.L.; Davies, D.H.; Simpson, K.; Asztalos, E.; Langley, J.M.; Le Saux, N.; Sauve, R.; Synnes, A.; et al. Invasive candidiasis in low birth weight preterm infants: Risk factors, clinical course and outcome in a prospective multicenter study of cases and their matched controls. BMC Infect. Dis. 2014, 14, 327. [Google Scholar] [CrossRef]
- Fairchild, K.D.; Sinkin, R.A.; Davalian, F.; Blackman, A.E.; Swanson, J.R.; Matsumoto, J.A.; Lake, D.E.; Moorman, J.R.; Blackman, J.A. Abnormal heart rate characteristics are associated with abnormal neuroimaging and outcomes in extremely low birth weight infants. J. Perinatol. 2014, 34, 375–379. [Google Scholar] [CrossRef]
- Ferreira, R.C.; Mello, R.R.; Silva, K.S. Neonatal sepsis as a risk factor for neurodevelopmental changes in preterm infants with very low birth weight. J. Pediatr. (Rio J.) 2014, 90, 293–299. [Google Scholar] [CrossRef]
- Chattopadhyay, N.; Mitra, K. Neurodevelopmental outcome of high risk newborns discharged from special care baby units in a rural district in India. J. Public Health Res. 2015, 4, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Picciolini, O.; Montirosso, R.; Porro, M.; Gianni, M.L.; Mosca, F. Neurofunctional assessment at term equivalent age can predict 3-year neurodevelopmental outcomes in very low birth weight infants. Acta Paediatr. 2016, 105, e47–e53. [Google Scholar] [CrossRef] [PubMed]
- Shany, E.; Inder, T.E.; Goshen, S.; Lee, I.; Neil, J.J.; Smyser, C.D.; Doyle, L.W.; Anderson, P.J.; Shimony, J.S. Diffusion Tensor Tractography of the Cerebellar Peduncles in Prematurely Born 7-Year-Old Children. Cerebellum 2017, 16, 314–325. [Google Scholar] [CrossRef] [Green Version]
- Abolfotouh, M.A.; Al Saif, S.; Altwaijri, W.A.; Al Rowaily, M.A. Prospective study of early and late outcomes of extremely low birthweight in Central Saudi Arabia. BMC Pediatr. 2018, 18. [Google Scholar] [CrossRef] [PubMed]
- Adams-Chapman, I.; Heyne, R.J.; DeMauro, S.B.; Duncan, A.F.; Hintz, S.R.; Pappas, A.; Vohr, B.R.; McDonald, S.A.; Das, A.; Newman, J.E.; et al. Neurodevelopmental Impairment Among Extremely Preterm Infants in the Neonatal Research Network. Pediatrics 2018, 141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, J.H.; Hsu, C.H.; Tsou, K.I.; Jim, W.T. Outcomes and related factors in a cohort of infants born in Taiwan over a period of five years (2007–2011) with borderline viability. J. Formos. Med. Assoc. 2018, 117, 365–373. [Google Scholar] [CrossRef] [PubMed]
- Pawar, S.J.; Oleti, T.; Bharathi, S.; Tipparaju, S.; Mustafa, E. Growth and Neurodevelopmental Outcome in Preterm LBW Infants with Sepsis in India: A Prospective Cohort. Int. J. Pediatr. 2018, 2018, 5735632. [Google Scholar] [CrossRef] [Green Version]
- Savioli, K.; Rouse, C.; Susi, A.; Gorman, G.; Hisle-Gorman, E. Suspected or known neonatal sepsis and neurodevelopmental delay by 5 years. J. Perinatol. 2018, 38, 1573–1580. [Google Scholar] [CrossRef]
- Singh, L.; Das, S.; Bhat, V.B.; Plakkal, N. Early Neurodevelopmental Outcome of Very Low Birthweight Neonates with Culture-positive Blood Stream Infection: A Prospective Cohort Study. Cureus 2018, 10, e3492. [Google Scholar] [CrossRef] [Green Version]
- Smilga, A.S.; Garfinkle, J.; Ng, P.; Andersen, J.; Buckley, D.; Fehlings, D.; Kirton, A.; Wood, E.; van Rensburg, E.; Shevell, M.; et al. Neonatal Infection in Children With Cerebral Palsy: A Registry-Based Cohort Study. Pediatr. Neurol. 2018, 80, 77–83. [Google Scholar] [CrossRef]
- Rand, K.M.; Austin, N.C.; Inder, T.E.; Bora, S.; Woodward, L.J. Neonatal Infection and Later Neurodevelopmental Risk in the Very Preterm Infant. J. Pediatr. 2016, 170, 97–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stoll, B.J.; Hansen, N.I.; Adams-Chapman, I.; Fanaroff, A.A.; Hintz, S.R.; Vohr, B.; Higgins, R.D.; National Institute of Child Health; Human Development Neonatal Research Network. Neurodevelopmental and growth impairment among extremely low-birth-weight infants with neonatal infection. J. Am. Med. Assoc. 2004, 292, 2357–2365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kono, Y.; Mishina, J.; Yonemoto, N.; Kusuda, S.; Fujimura, M.; Nicu Network, J. Neonatal correlates of adverse outcomes in very low-birthweight infants in the NICU Network. Pediatr. Int. 2011, 53, 930–935. [Google Scholar] [CrossRef] [PubMed]
- Schlapbach, L.J.; Aebischer, M.; Adams, M.; Natalucci, G.; Bonhoeffer, J.; Latzin, P.; Nelle, M.; Bucher, H.U.; Latal, B.; Swiss Neonatal, N.; et al. Impact of sepsis on neurodevelopmental outcome in a Swiss National Cohort of extremely premature infants. Pediatrics 2011, 128, e348–e357. [Google Scholar] [CrossRef] [PubMed]
- Adams-Chapman, I.; Bann, C.M.; Das, A.; Goldberg, R.N.; Stoll, B.J.; Walsh, M.C.; Sanchez, P.J.; Higgins, R.D.; Shankaran, S.; Watterberg, K.L.; et al. Neurodevelopmental outcome of extremely low birth weight infants with Candida infection. J. Pediatr. 2013, 163, 961–967. [Google Scholar] [CrossRef]
- Mitha, A.; Foix-L’Helias, L.; Arnaud, C.; Marret, S.; Vieux, R.; Aujard, Y.; Thiriez, G.; Larroque, B.; Cambonie, G.; Burguet, A.; et al. Neonatal infection and 5-year neurodevelopmental outcome of very preterm infants. Pediatrics 2013, 132, e372–e380. [Google Scholar] [CrossRef] [Green Version]
- Synnes, A.; Luu, T.M.; Moddemann, D.; Church, P.; Lee, D.; Vincer, M.; Ballantyne, M.; Majnemer, A.; Creighton, D.; Yang, J.; et al. Determinants of developmental outcomes in a very preterm Canadian cohort. Arch. Dis. Child. 2016, 6. [Google Scholar] [CrossRef]
- Bright, H.R.; Babata, K.; Allred, E.N.; Erdei, C.; Kuban, K.C.K.; Joseph, R.M.; O’Shea, T.M.; Leviton, A.; Dammann, O.; Investigators, E.S. Neurocognitive Outcomes at 10 Years of Age in Extremely Preterm Newborns with Late-Onset Bacteremia. J. Pediatr. 2017, 187, 43–49. [Google Scholar] [CrossRef]
- Bolisetty, S.; Tiwari, M.; Schindler, T.; Bowen, J.; Bajuk, B.; Carlisle, H.; Kent, A.; Smith, J.; Craven, P.; Glover, R.; et al. Neurodevelopmental outcomes of extremely preterm infants in New South Wales and the Australian Capital Territory. J. Paediatr. Child Health 2018. [Google Scholar] [CrossRef]
- Msall, M.E.; Buck, G.M.; Rogers, B.T.; Merke, D.P.; Wan, C.C.; Catanzaro, N.L.; Zorn, W.A. Multivariate risks among extremely premature infants. J. Perinatol. 1994, 14, 41–47. [Google Scholar]
- Friedman, S.; Richardson, S.E.; Jacobs, S.E.; O’Brien, K. Systemic Candida infection in extremely low birth weight infants: Short term morbidity and long term neurodevelopmental outcome. Pediatr. Infect. Dis. J. 2000, 19, 499–504. [Google Scholar] [CrossRef] [PubMed]
- Hack, M.; Wilson-Costello, D.; Friedman, H.; Taylor, G.H.; Schluchter, M.; Fanaroff, A.A. Neurodevelopment and predictors of outcomes of children with birth weights of less than 1000 g: 1992–1995. Arch. Pediatr. Adolesc. Med. 2000, 154, 725–731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoekstra, R.E.; Ferrara, T.B.; Couser, R.J.; Payne, N.R.; Connett, J.E. Survival and long-term neurodevelopmental outcome of extremely premature infants born at 23–26 weeks’ gestational age at a tertiary center. Pediatrics 2004, 113, e1–e6. [Google Scholar] [CrossRef] [Green Version]
- Shah, D.K.; Doyle, L.W.; Anderson, P.J.; Bear, M.; Daley, A.J.; Hunt, R.W.; Inder, T.E. Adverse neurodevelopment in preterm infants with postnatal sepsis or necrotizing enterocolitis is mediated by white matter abnormalities on magnetic resonance imaging at term. J. Pediatr. 2008, 153, 170–175. [Google Scholar] [CrossRef] [PubMed]
- Jang, D.H.; Sung, I.Y.; Jeon, J.Y.; Moon, H.J.; Kim, K.S.; Kim, E.A.R.; Lee, B.S. Neurodevelopmental outcomes in very low-birth-weight infants in Korea: 1998–2007 vs. 1989–1997. J. Child Neurol. 2011, 26, 1405–1410. [Google Scholar] [CrossRef] [PubMed]
- Alshaikh, B.; Yee, W.; Lodha, A.; Henderson, E.; Yusuf, K.; Sauve, R. Coagulase-negative staphylococcus sepsis in preterm infants and long-term neurodevelopmental outcome. J. Perinatol. 2014, 34, 125–129. [Google Scholar] [CrossRef] [Green Version]
- Hentges, C.R.; Silveira, R.C.; Procianoy, R.S.; Carvalho, C.G.; Filipouski, G.R.; Fuentefria, R.N.; Marquezotti, F.; Terrazan, A.C. Association of late-onset neonatal sepsis with late neurodevelopment in the first two years of life of preterm infants with very low birth weight. J. Pediatr. (Rio J.) 2014, 90, 50–57. [Google Scholar] [CrossRef] [Green Version]
- Yang, P.; Chen, Y.H.; Yen, C.F.; Chen, H.L. Psychiatric diagnoses, emotional-behavioral symptoms and functional outcomes in adolescents born preterm with very low birth weights. Child Psychiatry Hum. Dev. 2015, 46, 358–366. [Google Scholar] [CrossRef]
- Maruyama, H.; Nakata, Y.; Kanazawa, A.; Kikkawa, K. Survival and Neurodevelopmental Outcomes of Very Low Birth Weight Infants in a Regional Core Hospital in Kochi, Japan. Acta Med. Okayama 2016, 70, 345–352. [Google Scholar]
- Young, J.M.; Morgan, B.R.; Powell, T.L.; Moore, A.M.; Whyte, H.E.A.; Smith, M.L.; Taylor, M.J. Associations of Perinatal Clinical and Magnetic Resonance Imaging Measures with Developmental Outcomes in Children Born Very Preterm. J. Pediatr. 2016, 170, 90–96. [Google Scholar] [CrossRef]
- Zonnenberg, I.A.; van Dijk-Lokkart, E.M.; van den Dungen, F.A.M.; Vermeulen, R.J.; van Weissenbruch, M.M. Neurodevelopmental outcome at 2 years of age in preterm infants with late-onset sepsis. Eur. J. Pediatr. 2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, B.E.; Cheung, P.Y.; Robinson, J.L.; Evanochko, C.; Robertson, C.M. Comparative study of mortality and morbidity in premature infants (birth weight, <1250 g) with candidemia or candidal meningitis. Clin. Infect. Dis. 1998, 27, 559–565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van der Ree, M.; Tanis, J.C.; Van Braeckel, K.N.; Bos, A.F.; Roze, E. Functional impairments at school age of preterm born children with late-onset sepsis. Early Hum. Dev. 2011, 87, 821–826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Haan, T.R.; Beckers, L.; de Jonge, R.C.; Spanjaard, L.; van Toledo, L.; Pajkrt, D.; van Wassenaer-Leemhuis, A.G.; van der Lee, J.H. Neonatal gram negative and Candida sepsis survival and neurodevelopmental outcome at the corrected age of 24 months. PLoS ONE 2013, 8, e59214. [Google Scholar] [CrossRef] [Green Version]
- Dilli, D.; Eras, Z.; Dilmen, U.; Sakrucu, E.D. Neurodevelopmental evaluation of very low birth weight infants with sepsis at 18 to 24 months corrected age. Indian Pediatr. 2013, 50, 327–330. [Google Scholar] [CrossRef]
- Tin, W.; Fritz, S.; Wariyar, U.; Hey, E. Outcome of very preterm birth: Children reviewed with ease at 2 years differ from those followed up with difficulty. Arch. Dis. Child. Fetal Neonatal Ed. 1998, 79, F83–F87. [Google Scholar] [CrossRef]
- Callanan, C.; Doyle, L.; Rickards, A.; Kelly, E.; Ford, G.; Davis, N. Children followed with difficulty: How do they differ? J. Paediatr. Child Health 2001, 37, 152–156. [Google Scholar] [CrossRef]
- Wynn, J.L.; Wong, H.R.; Shanley, T.P.; Bizzarro, M.J.; Saiman, L.; Polin, R.A. Time for a neonatal-specific consensus definition for sepsis. Pediatr. Crit. Care Med. 2014, 15, 523–528. [Google Scholar] [CrossRef] [Green Version]
- Anderson, P.J.; De Luca, C.R.; Hutchinson, E.; Roberts, G.; Doyle, L.W.; Victorian Infant Collaborative, G. Underestimation of developmental delay by the new Bayley-III Scale. Arch. Pediatr. Adolesc. Med. 2010, 164, 352–356. [Google Scholar] [CrossRef] [Green Version]
- Moore, T.; Johnson, S.; Haider, S.; Hennessy, E.; Marlow, N. Relationship between test scores using the second and third editions of the Bayley Scales in extremely preterm children. J. Pediatr. 2012, 160, 553–558. [Google Scholar] [CrossRef]
- Luttikhuizen dos Santos, E.S.; de Kieviet, J.F.; Konigs, M.; van Elburg, R.M.; Oosterlaan, J. Predictive value of the Bayley scales of infant development on development of very preterm/very low birth weight children: A meta-analysis. Early Hum. Dev. 2013, 89, 487–496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Study Design | Population | Birth Year | No. of Survivors at Follow-Up | Follow-Up Rate | Total No. Followed Up | No. of Confirmed Sepsis | No. of Non-sepsis Comparators | Organism Isolated | Age at Assessment (Months) | Blinding of Outcome Assessors |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Msall [51] | 1994 | SC, cohort | GA 23–28 | 1983–1986 | 153 | 97% | 149 | 18 | 131 | NS | 52–62 | Yes |
| Lee [63] | 1998 | SC, case control | BW < 1250 | 1990–1995 | 35 | N/A | N/A | 14 | 21 | Candida | 9–50 | NS |
| Friedman [52] | 2000 | SC, cohort | ELBW | 1988–1996 | 334 | 90% | 299 | 27 | 272 | Candida | 21–24 | NS |
| Hack [53] | 2000 | SC, cohort | ELBW | 1992–1995 | 241 | 92% | 221 | 109 | 112 | NS | 20 | NS |
| Hoekstra [54] | 2004 | SC, cohort | GA 23–26 | 1986–2000 | 778 | 87% | 675 | NS | NS | NS | 36–60 | No |
| Stoll [43] | 2004 | MC, cohort | ELBW | 1993–2001 | 7892 | 80% | 6314 | 1922 | 2161 | Shows breakdown | 18–22 | NS |
| Shah [55] | 2008 | SC, cohort | GA < 30 | 2001–2003 | 204 | 94% | 192 | 64 | 119 | NS | 24 | NS |
| Kono [44] | 2011 | MC, cohort | VLBW | 2003–2004 | 2847 | 64% | 1826 | 113 | 1714 | NS | 36–42 | NS |
| Jang [56] | 2011 | SC, cohort | VLBW | 1989–2007 | 967 | N/A | N/A | NS | NS | NS | 18–24 | NS |
| Schlapbach [45] | 2011 | MC, cohort | GA 24–27 | 2000–2007 | 482 | 77% | 372 | 136 | 236 | Shows breakdown | 18–24 | NS |
| Van der Ree [64] | 2011 | SC, case-control | GA < 32 or VLBW | 2000–2001 | 50 | N/A | N/A | 32 | 18 | Shows breakdown | 72–108 | NS |
| Adams-Chapman [46] | 2013 | MC, cohort | ELBW | 2004–2007 | 1966 | 71% | 1391 | 474 | 917 | Candida and other | 18–22 | NS |
| De Haan [65] | 2013 | SC, case-control | GA < 30 | 1997–2007 | 168 | 90% | 152 | 50 | 102 | GN and Candida | 24 | NS |
| Dilli [66] | 2013 | SC, case control | VLBW | 2008–2009 | 33 | N/A | N/A | 13 | 20 | NS | 18–24 | NS |
| Mitha [47] | 2013 | MC, cohort | GA 22–32 | 1997 | 2277 | 78% | 1769 | 688 | 1081 | NS | 60 | NS |
| Alshaikh [57] | 2014 | SC, cohort | GA < 29 | 1995–2008 | 383 | 87% | 332 | 105 | 227 | CONS | 30–42 | Yes |
| Hentges [58] | 2014 | SC, cohort | GA < 32 or VLBW | 2003–2010 | 291 | 78% | 226 | 62 | 164 | Shows breakdown | 18–24 | Yes |
| Yang [59] | 2015 | SC, cohort | VLBW | 1996–1999 | 111 | 55% | 61 | 26 | 35 | NS | 144–180 | NS |
| Maruyama [60] | 2016 | SC, cohort | VLBW | 2005–2012 | 200 | 78% | 155 | N/A | N/A | NS | 36–42 | NS |
| Synnes [48] | 2016 | MC, cohort | GA < 29 | 2009–2011 | 2340 | 80% | 1870 | NS | NS | NS | 18–21 | NS |
| Young [61] | 2016 | SC, cohort | GA < 32 | 2008–2010 | 100 | N/A | N/A | 17 | 33 | NS | 24, 48 | NS |
| Bright [49] | 2017 | MC, cohort | GA < 28 | 2002–2004 | 966 | 92% | 889 | 223 | 532 | NS | 120 | Yes |
| Bolisetty [50] | 2018 | MC, cohort | GA 23–28 | 2007–2012 | 1897 | 80% | 1514 | 526 | 988 | NS | 24–36 | NS |
| Zonnenberg [62] | 2019 | SC, cohort | GA < 32 or VLBW | 2008–2014 | 104 | 87% | 90 | 68 | 22 | Shows breakdown | 24 | Yes |
| Study | Scale Used | NDI Definitions |
|---|---|---|
| Studies Which Reported Dichotomised Outcomes | ||
| Msall [51] | McCarthy Scales of Children’s Abilities, Cattell Infant Intelligence Test or the Clinical Linguistic Auditory Milestone Scale (for children with a mental age < 30 months) | One or more of the following:
|
| Lee [63] | BSID-II (<24 months), Stanford–Binet Intelligence Scale, Peabody Developmental Motor Scales | One or more of the following:
|
| Friedman [52] | BSID-II | Mild-moderate: mild-moderate CP, moderate cognitive delay (MDI 70–82) Severe: severe CP (not sitting by 2 years of age, non-ambulatory), bilateral blindness, aided sensorineural hearing loss, severe cognitive delay (MDI < 70), shunted hydrocephalus |
| Hack [53] | BSID-II | One or more of the following:
|
| Hoekstra [54] | BSID-II (<36 mo) | Mild–moderate: isolated muscle tone abnormalities, unilateral blindness, hyperactivity, scores 1–2 SD below mean Severe: spasticity, severe hypotonia, blindness, deafness, scores >2 SD below mean |
| 3–6 years: Denver Developmental Screening Test, Early Language Milestone Scale, Zimmerman Preschool Articulation Test | Mild–moderate: minor abnormalities, developmental assessments 6–12 months below chronological age Severe: severe physical and neurologic examinations, developmental assessments >1 year below chronological age | |
| School children: University of Vermont Achenbach Child Behaviour Checklist and the Teacher’s Report form | Mild–moderate: below grade average in >1 subject, but not far below in >1 subject, or had below-normal Achenbach scores Severe: spasticity, severe hypotonia, blindness, hearing loss, repeated a grade, require special education, far below grade average in >1 subject or Achenbach scores far below normal | |
| Stoll [43] | BSID-II | One or more of the following:
|
| Kono [44] | KPSD | One or more of the following:
|
| Jang [56] | BSID or Denver Developmental Screening Test | One or more of the following:
|
| Schlapbach [45] | BSID-II, GMFCS | One or more of the following:
|
| Adams-Chapman [46] | BSID-II, BSID-III, GMFCS | BSID-II (Epoch 1)
|
| De Haan [65] | BSID-II-NL | One or more of the following:
|
| Dilli [66] | BSID-II, GMFCS | One or more of the following:
|
| Mitha [47] | Kaufman Assessment Battery for Children |
|
| Alshaikh [57] | BSID-II, WPPSI-Revised, Stanford–Binet IV | One or more of the following:
|
| Yang [59] | CBCL, “Current Status Survey”, WISC-IV, MINI-KID (for ADHD, anxiety/mood disorders), DSM-IV-TR (for ASD) | “Disabled” = when parents disclosed that the child received a handicap status as issued by the Ministry of the Interior of Taiwan. Handicap is defined as disadvantaged condition, deriving from impairment or disability limiting a person performing a role considered normal in respect of their age, sex and social and cultural factors. |
| Maruyama [60] | KPSD | One or more of the following:
|
| Synnes [48] | BSID-III, GMFCS | Severe NDI
|
| Bright [49] | GMFCS, DAS-II, OWLS, NEPSY-II, WIAT-III, Manual Ability Classification Test |
|
| Bolisetty [50] | BSID-III, GMFCS | Moderate
|
| Studies Which Reported Continuous Outcomes | ||
| Shah [55] | BSID-II | N/A |
| Van der Ree [64] | Bax’ criteria, GMFCS, Movement ABC, WISC-III-NL, NEPSY-II, AVLT, TEA-Ch, ADHD questionnaire, BRIEF, CBCL | N/A |
| Hentges [58] | BSID-II | N/A |
| Young [61] | At 2 years: BSID-III At 4 years: WPPI-III, CLEF-2, Beery-Buktenica Test of Visual Motor Integration, the Behaviour Assessment System for Children Parent Rating Scales, Behavioural Rating Inventory of Executive Functioning-Preschool | N/A |
| Zonnenberg [62] | BSID-II, Lexilijst (lexical development questionnaire), CBCL | N/A |
| Number of Infants with NDI | ||||
|---|---|---|---|---|
| Study | Sepsis Group | No Sepsis Group | Attrition Rate | Comments |
| Msall [51] | 9/18 (50%) | 22/131 (17%) | 3% | N/A |
| Lee [63] | 4/14 (29%) | 3/21 (14%) | N/A | N/A |
| Friedman [52] | 11/27 (41%) | 32/272 (12%) | 10% | N/A |
| Hack [53] | 43/93 (46%) | 62/112 (55%) | 8% | N/A |
| Hoekstra [54] # | NS | NS | 13% | At 47.5 months (range 36–60), there was no statistically significant association between primary or secondary sepsis and NDI. |
| Stoll [43] | 861/1778 (48%) | 576/1976 (29%) | 20% | N/A |
| Kono [44] # | NS | NS | 36% | At 36–42 months, there was an association between sepsis and cerebral palsy or death (OR 2.6, 95% CI 1.4–4.8) as well as sepsis and NDI or death (OR 2.8, 95% CI 1.6–4.8). |
| Jang [56] # | NS | NS | N/A | At 18–24 months, univariate analysis showed weak association between sepsis and cerebral palsy (OR 1.653, 95% CI 0.849–3.215). |
| Schlapbach [45] | 46/134 (34%) | 55/235 (23%) | 23% | N/A |
| Adams-Chapman [46] | 148/474 (31%) | 153/917 (17%) | 16% | N/A |
| De Haan [65] | 28/50 (56%) | 16/102 (17%) | 10% | N/A |
| Dilli [66] | 8/13 (62%) | 4/20 (20%) | N/A | N/A |
| Mitha [47] | 84/643 (14%) | 73/1126 (6%) | 22% | N/A |
| Alshaikh [57] | 26/105 (25%) | 34/227 (15%) | 13% | N/A |
| Yang [59] | 13/26 (50%) | 7/35 (20%) | 45% | N/A |
| Maruyama [60] | 3/4 (75%) | 37/153 (24%) | 28% | N/A |
| Synnes [48] # | NS | NS | 20% | At 18–21 months, there was significant association between sepsis and significant NDI (OR 1.50, 95% CI 1.05–1.86), but no information was reported on association between sepsis and NDI. |
| Bright [49] # | NS | NS | 8% | At 10 years of age, children who had confirmed bacteraemia were associated with lower z-scores in verbal and nonverbal IQ, oral expression, academic achievement, executive function and visual impairment. They were also more likely to have visual and auditory impairment but not motor deficits. After adjusting for IQ, many of these associations were lost. |
| Bolisetty [50] | 138/526 (26%) | 29/988 (3%) | 20% | N/A |
| Total | 1422/3905 (36%) | 1103/6315 (17%) | Median: 18% | |
| Study | Assessment Tool | Sepsis Group | Non-sepsis Group | Attrition Rate | Comments |
|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | ||||
| Shah [55] | MDI (BSID-II) | 79.7 (21.2) | 86.5 (18.7) | 6% | N/A |
| PDI (BSID-II) | 84.2 (21.4) | 89.9 (14.5) | |||
| Van der Ree [64] | Movement ABC Total (M-ABC2)—raw score | 13 (10) | 8 (6) | N/A | N/A |
| Total intelligence (WISC-II)—IQ | 89 (13) | 98 (8) | |||
| Total behavioural problems (CBCL)—t-scores | 53 (12) | 56 (9) | |||
| Hentges [58] | MDI (BSID-II) | 85.9 (10.8) | 86.1 (11.59) | 22% | N/A |
| PDI (BSID-II) | 89.8 (13.3) | 91.7 (14.02) | |||
| Young [61] # | At 2 years: BSID-III | NS | NS | N/A | Sepsis was not significant with 2-year or 4-year cognitive measures, but significant with 4-year behavioural measures. |
| At 4 years: WPPI-III, CLEF-2, Beery–Buktenica Test of Visual Motor Integration, the Behaviour Assessment System for Children Parent Rating Scales, Behavioural Rating Inventory of Executive Functioning – Preschool | |||||
| Zonnenberg [62] | MDI (BSID-II) | 100 (9.0) | 98 (13.9) | 23% | N/A |
| PDI (BSID-II) | 100 (9.4) | 99 (12.3) | |||
| Lexiquotient (Lexilijst) | 91 (16.1) | 88 (18.2) | |||
| Total behavioural score (CBCL) | 26 (14.9) | 30 (21.2) | |||
| Total internalising score (CBCL) | 5 (4.3) | 8 (7.9) | |||
| Total externalising score (CBCL) | 12 (7.5) | 12 (7.6) | |||
| Median: 22% |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cai, S.; Thompson, D.K.; Anderson, P.J.; Yang, J.Y.-M. Short- and Long-Term Neurodevelopmental Outcomes of Very Preterm Infants with Neonatal Sepsis: A Systematic Review and Meta-Analysis. Children 2019, 6, 131. https://0-doi-org.brum.beds.ac.uk/10.3390/children6120131
Cai S, Thompson DK, Anderson PJ, Yang JY-M. Short- and Long-Term Neurodevelopmental Outcomes of Very Preterm Infants with Neonatal Sepsis: A Systematic Review and Meta-Analysis. Children. 2019; 6(12):131. https://0-doi-org.brum.beds.ac.uk/10.3390/children6120131
Chicago/Turabian StyleCai, Shirley, Deanne K. Thompson, Peter J. Anderson, and Joseph Yuan-Mou Yang. 2019. "Short- and Long-Term Neurodevelopmental Outcomes of Very Preterm Infants with Neonatal Sepsis: A Systematic Review and Meta-Analysis" Children 6, no. 12: 131. https://0-doi-org.brum.beds.ac.uk/10.3390/children6120131