Functional Disability in Adolescents with Chronic Pain: Comparing an Interdisciplinary Exposure Program to Usual Care

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
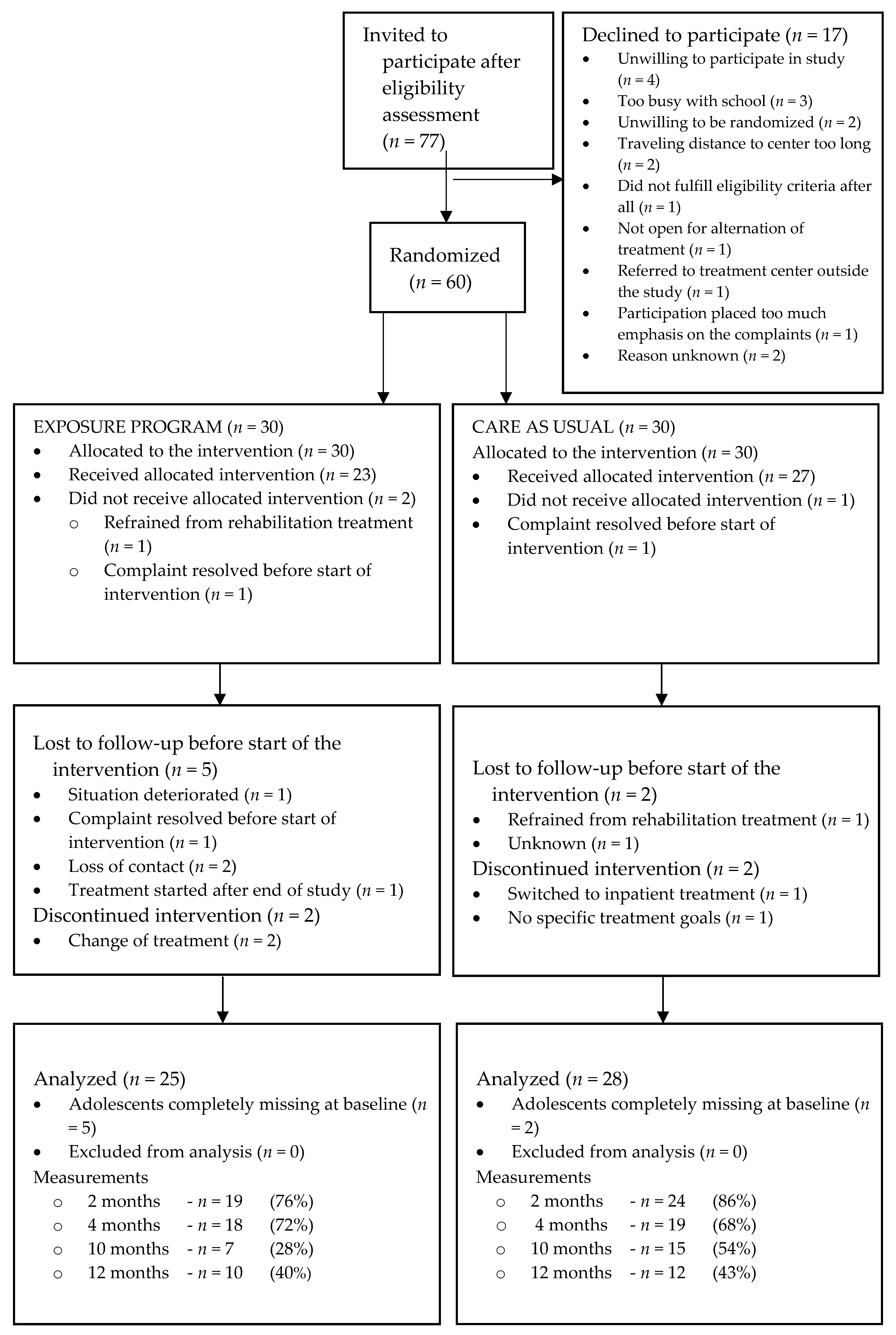
2.2. Sample and Procedure
2.3. Interventions
2.4. Measurement Points, Describing Baseline, and Outcome Measures for Treatment Effectiveness
2.5. Protocol Adherence and Contamination Check
2.6. Randomization, Allocation Concealment, and Blinding
2.7. Sample Size
2.8. Statistical Analysis
2.9. Analysis of Treatment Effectiveness
2.10. Analysis of Treatment Delivery
3. Results
3.1. Description of the Study Population
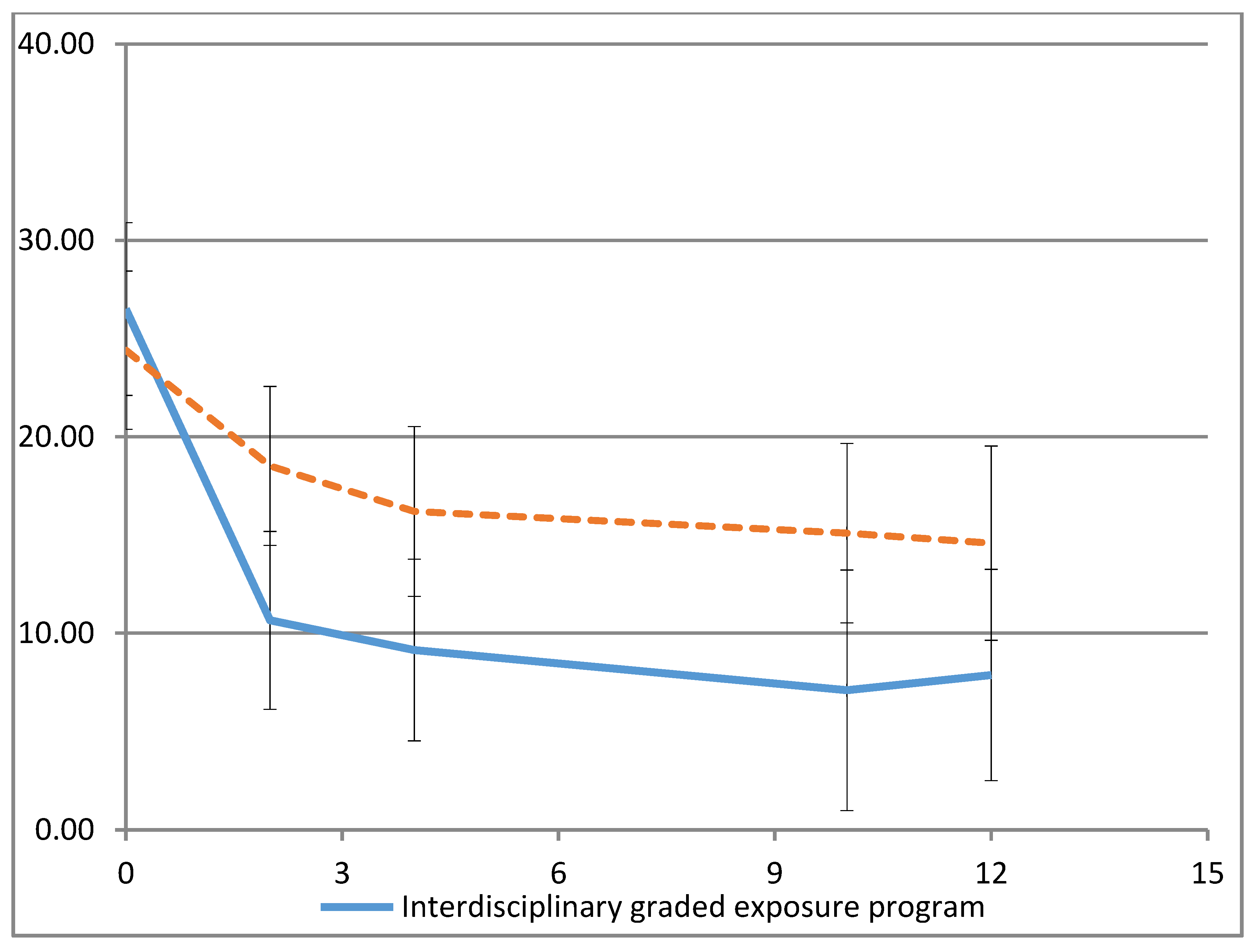
3.2. Effects of the Multimodal Rehabilitation Program
3.3. Health Care Utilization and School Support and Absenteeism
3.4. Protocol Adherence and Contamination
4. Discussions
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Perquin, C.W.; Hazebroek-Kampschreur, A.A.J.M.; Hunfeld, J.A.M.; Bohnen, A.M.; van Suijlekom-Smit, L.W.A.; Passchier, J.; van der Wouden, J.C. Pain in children and adolescents: A common experience. Pain 2000, 87, 51–58. [Google Scholar] [CrossRef]
- King, S.; Chambers, C.T.; Huguet, A.; MacNevin, R.C.; McGrath, P.J.; Parker, L.; MacDonald, A.J. The epidemiology of chronic pain in children and adolescents revisited: A systematic review. Pain 2011, 152, 2729–2738. [Google Scholar] [CrossRef] [PubMed]
- El-Metwally, A.; Salminen, J.J.; Auvinen, A.; Kautiainen, H.; Mikkelsson, M. Prognosis of non-specific musculoskeletal pain in preadolescents: A prospective 4-year follow-up study till adolescence. Pain 2004, 110, 550–559. [Google Scholar] [CrossRef] [PubMed]
- Fearon, P.; Hotopf, M. Relation between headache in childhood and physical and psychiatric symptoms in adulthood: National birth cohort study. BMJ 2001, 322, 1145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eccleston, C.; Palermo, T.M.; de CWilliams, A.C.; Holley, A.L.; Morley, S.; Fisher, E.; Law, E. Psychological therapies for the management of chronic and recurrent pain in children and adolescents. Cochrane Database Syst. Rev. 2012, 12, CD003968. [Google Scholar]
- Palermo, T.M.; Eccleston, C.; Lewandowski, A.S.; Williams, A.C.D.C.; Morley, S. Randomized controlled trials of psychological therapies for management of chronic pain in children and adolescents: An updated meta-analytic review. Pain 2010, 148, 387–397. [Google Scholar] [CrossRef] [Green Version]
- Hechler, T.; Kanstrup, M.; Holley, A.L.; Simons, L.E.; Wicksell, R.; Hirschfeld, G.; Zernikow, B. Systematic Review on Intensive Interdisciplinary Pain Treatment of Children with Chronic Pain. Pediatrics 2015, 136, 115–127. [Google Scholar] [CrossRef] [Green Version]
- Martin, A.L.; McGrath, P.A.; Brown, S.C.; Katz, J. Anxiety sensitivity, fear of pain and pain-related disability in children and adolescents with chronic pain. Pain Res. Manag. 2007, 12, 267–272. [Google Scholar] [CrossRef]
- de Jong, J.R.; Vlaeyen, J.W.; Onghena, P.; Cuypers, C.; den Hollander, M.; Ruijgrok, J. Reduction of pain-related fear in complex regional pain syndrome type I: The application of graded exposure in vivo. Pain 2005, 116, 264–275. [Google Scholar] [CrossRef]
- Leeuw, M.; Goossens, M.E.; van Breukelen, G.J.; de Jong, J.R.; Heuts, P.H.; Smeets, R.J.; Köke, A.J.; Vlaeyen, J.W. Exposure in vivo versus operant graded activity in chronic low back pain patients: Results of a randomized controlled trial. Pain 2008, 138, 192–207. [Google Scholar] [CrossRef]
- den Hollander, M.; Goossens, M.; de Jong, J.; Ruijgrok, J.; Oosterhof, J.; Onghena, P.; Smeets, R.; Vlaeyen, J.W. Expose or protect? A randomized controlled trial of exposure in vivo vs pain-contingent treatment as usual in patients with complex regional pain syndrome type 1. Pain 2016, 157, 2318–2329. [Google Scholar] [CrossRef] [PubMed]
- Vlaeyen, J.W.; Linton, S.J. Fear-avoidance and its consequences in chronic musculoskeletal pain: A state of the art. Pain 2000, 85, 317–332. [Google Scholar] [CrossRef] [Green Version]
- Caes, L.; Fisher, E.; Clinch, J.; Tobias, J.H.; Eccleston, C. The role of pain-related anxiety in adolescents’ disability and social impairment: ALSPAC data. Eur. J. Pain 2015, 19, 842–851. [Google Scholar] [CrossRef] [PubMed]
- Simons, L.E.; Kaczynski, K.J. The Fear Avoidance model of chronic pain: Examination for pediatric application. J. Pain 2012, 13, 827–835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simons, L.E.; Kaczynski, K.J.; Conroy, C.; Logan, D.E. Fear of pain in the context of intensive pain rehabilitation among children and adolescents with neuropathic pain: Associations with treatment response. J. Pain 2012, 13, 1151–1161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goubert, L.; Simons, L.E. Cognitive styles and processes in paediatric pain. In Oxford Textbook of Paediatric Pain; McGrath, P.A., Stevens, B.J., Walker, S.M., Zempsky, W.T., Eds.; Oxford University Press: Oxford, UK, 2012. [Google Scholar]
- Dekker, C.; Goossens, M.E.; Bastiaenen, C.H.; Verbunt, J.A. Study protocol for a multicentre randomized controlled trial on effectiveness of an outpatient multimodal rehabilitation program for adolescents with chronic musculoskeletal pain (2B Active). BMC Musculoskelet. Disord. 2016, 17, 317. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, D.; Lellouch, J. Explanatory and pragmatic attitudes in therapeutical trials. J. Clin. Epidemiol. 2009, 62, 499–505. [Google Scholar] [CrossRef]
- Engelbert, R.H.; Juul-Kristensen, B.; Pacey, V.; de Wandele, I.; Smeenk, S.; Woinarosky, N.; Sabo, S.; Scheper, M.C.; Russek, L.; Simmonds, J.V. The evidence-based rationale for physical therapy treatment of children, adolescents, and adults diagnosed with joint hypermobility syndrome/hypermobile Ehlers Danlos syndrome. Am. J. Med. Genet. C Semin. Med. Genet. 2017, 175, 158–167. [Google Scholar] [CrossRef] [Green Version]
- Keer, R.; Simmonds, J. Joint protection and physical rehabilitation of the adult with hypermobility syndrome. Curr. Opin. Rheumatol. 2011, 23, 131–136. [Google Scholar] [CrossRef]
- Dekker, C.; van Haastregt, J.C.M.; Verbunt, J.A.M.C.F.; De Jong, J.; van Meulenbroek, T.; Pernot, H.F.M.; van Velzen, A.D.; Bastiaenen, C.H.G.; Goossens, M.E.J.B. Pain-related fear in adolescents with chronic musculoskeletal pain: Process evaluation of an interdisciplinary graded exposure program. BMC Health Serv. Res. 2020, 20, 213. [Google Scholar] [CrossRef]
- Claar, R.L.; Walker, L.S. Functional assessment of pediatric pain patients: Psychometric properties of the functional disability inventory. Pain 2006, 121, 77–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walker, L.S.; Greene, J.W. The functional disability inventory: Measuring a neglected dimension of child health status. J. Pediatr. Psychol. 1991, 16, 39–58. [Google Scholar] [CrossRef] [PubMed]
- Simons, L.E.; Sieberg, C.B.; Carpino, E.; Logan, D.; Berde, C. The Fear of Pain Questionnaire (FOPQ): Assessment of Pain-Related Fear among Children and Adolescents with Chronic Pain. J. Pain 2011, 12, 677–686. [Google Scholar] [CrossRef] [PubMed]
- Dekker, C.; Bastiaenen, C.H.G.; de Vries, J.E.; Simons, L.E.; Goossens, M.; Verbunt, J. Dutch version of the Fear of Pain Questionnaire for adolescents with chronic pain. Disabil. Rehabil. 2017, 40, 1326–13324. [Google Scholar] [CrossRef] [Green Version]
- Verbunt, J.A.; Nijhuis, A.; Vikstrom, M.; Stevens, A.; Haga, N.; de Jong, J.; Goossens, M. The psychometric characteristics of an assessment instrument for perceived harmfulness in adolescents with musculoskeletal pain (PHODA-youth). Eur. J. Pain 2015, 19, 695–705. [Google Scholar] [CrossRef]
- Crombez, G.; Bijttebier, P.; Eccleston, C.; Mascagni, T.; Mertens, G.; Goubert, L.; Verstraeten, K. The child version of the pain catastrophizing scale (PCS-C): A preliminary validation. Pain 2003, 104, 639–646. [Google Scholar] [CrossRef]
- Roelofs, J.; Braet, C.; Rood, L.; Timbremont, B.; van Vlierberghe, L.; Goossens, L.; van Breukelen, G. Norms and screening utility of the Dutch version of the Children’s Depression Inventory in clinical and nonclinical youths. Psychol. Assess. 2010, 22, 866–877. [Google Scholar] [CrossRef] [Green Version]
- Stinson, J.N.; Kavanagh, T.; Yamada, J.; Gill, N.; Stevens, B. Systematic review of the psychometric properties, interpretability and feasibility of self-report pain intensity measures for use in clinical trials in children and adolescents. Pain 2006, 125, 143–157. [Google Scholar] [CrossRef]
- Merlijn, V.P.; Hunfeld, J.A.; van der Wouden, J.C.; Hazebroek-Kampschreur, A.A.; Passchier, J. Shortening a quality of life questionnaire for adolescents with chronic pain and its psychometric qualities. Psychol. Rep. 2002, 90 Pt 1, 753–759. [Google Scholar] [CrossRef]
- Leeuw, M.; Goossens, M.E.; de Vet, H.C.; Vlaeyen, J.W. The fidelity of treatment delivery can be assessed in treatment outcome studies: A successful illustration from behavioral medicine. J. Clin. Epidemiol. 2009, 62, 81–90. [Google Scholar] [CrossRef]
- Perepletchikova, F.; Kazdin, A. Treatment integrity and therapeutic change: Issues and research recommendations. Clin. Psychol. Sci. Pract. 2005, 12, 365–383. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sil, S.; Arnold, L.M.; Lynch-Jordan, A.; Ting, T.V.; Peugh, J.; Cunningham, N.; Powers, S.W.; Lovell, D.J.; Hashkes, P.J.; Passo, M.; et al. Identifying treatment responders and predictors of improvement after cognitive-behavioral therapy for juvenile fibromyalgia. Pain 2014, 155, 1206–1212. [Google Scholar] [CrossRef] [PubMed]
- Kashikar-Zuck, S.; Flowers, S.R.; Claar, R.L.; Guite, J.W.; Logan, D.E.; Lynch-Jordan, A.M.; Palermo, T.M.; Wilson, A.C. Clinical utility and validity of the Functional Disability Inventory among a multicenter sample of youth with chronic pain. Pain 2011, 152, 1600–1607. [Google Scholar] [CrossRef] [Green Version]
- Eccleston, C.; Malleson, P.N.; Clinch, J.; Connell, H.; Sourbut, C. Chronic pain in adolescents: Evaluation of a programme of interdisciplinary cognitive behaviour therapy. Arch. Dis. Child. 2003, 88, 881–885. [Google Scholar] [CrossRef] [Green Version]
- Kashikar-Zuck, S.; Swain, N.F.; Jones, B.A.; Graham, T.B. Efficacy of cognitive-behavioral intervention for juvenile primary fibromyalgia syndrome. J. Rheumatol. 2005, 32, 1594–1602. [Google Scholar]
- Hechler, T.; Dobe, M.; Kosfelder, J.; Damschen, U.; Hubner, B.; Blankenburg, M.; Sauer, C.; Zernikow, B. Effectiveness of a 3-week multimodal inpatient pain treatment for adolescents suffering from chronic pain: Statistical and clinical significance. Clin. J. Pain 2009, 25, 156–166. [Google Scholar] [CrossRef]
- Hechler, T.; Ruhe, A.K.; Schmidt, P.; Hirsch, J.; Wager, J.; Dobe, M.; Krummenauer, F.; Zernikow, B. Inpatient-based intensive interdisciplinary pain treatment for highly impaired children with severe chronic pain: Randomized controlled trial of efficacy and economic effects. Pain 2014, 155, 118–128. [Google Scholar] [CrossRef]
- Maynard, C.S.; Amari, A.; Wieczorek, B.; Christensen, J.R.; Slifer, K.J. Interdisciplinary behavioral rehabilitation of pediatric pain-associated disability: Retrospective review of an inpatient treatment protocol. J. Pediatr. Psychol. 2010, 35, 128–137. [Google Scholar] [CrossRef] [Green Version]
- Simons, L.E.; Sieberg, C.B.; Pielech, M.; Conroy, C.; Logan, D.E. What does it take? Comparing intensive rehabilitation to outpatient treatment for children with significant pain-related disability. J. Pediatr. Psychol. 2013, 38, 213–223. [Google Scholar] [CrossRef] [Green Version]
- Logan, D.E.; Simons, L.E.; Carpino, E.A. Too sick for school? Parent influences on school functioning among children with chronic pain. Pain 2012, 153, 437–443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patsopoulos, N.A. A pragmatic view on pragmatic trials. Dialogues Clin. Neurosci. 2011, 13, 217–224. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Exposure Program | Care as Usual (GA) | |
|---|---|---|
| Underlying paradigm | Classical conditioning; cognitive behavioral | Operant learning principles |
| Main treatment aim | Restore adolescents’ age-appropriate functional abilities by reducing pain-related fear through gradual exposure to fear-provoking activities | Increase adolescents’ age-appropriate functional abilities by encouraging desired behavior and time-contingent stepwise increase in activity levels |
| Therapists | Consultant in rehabilitation medicine, psychologist, physiotherapist or occupational therapist | Consultant in rehabilitation medicine, psychologist, physiotherapist or occupational therapist |
| Number of sessions | 1 intake with consultant in rehabilitation medicine + 14 sessions of 1 h. 3 sessions for parents | Variable, from 9 to 16 sessions |
| Treatment overview in phases | Phase 1: intake + PHODA-youth (1 h): cognitive behavioral analysis of complaints and consequences Phase 2: education (1 h) about treatment rationale, personal fear-avoidance model Phase 3: Exposure with behavioral experiments (12 × 1 h), exposure to fear-provoking activities and movements, generalization and relapse prevention | Phase 1: inventory of the problem Phase 2: problem analyses Phase 3: education Phase 4: choosing activities Phase 5: determining baseline (pain-contingent functioning) Phase 6: determining goal and scheme to increase activity Phase 7: executing scheme, time-contingent increase of activities, encouraging of successful behavior Phase 8: generalization and evaluation |
| Parent module | 3 sessions of 2 h: medical education and treatment rationale, the role of pain in the family system, generalization and relapse prevention | No separate parent program |
| Additional physical training + alternative treatment schedule | Adolescents with pain complaints related to hypermobility receive 16 (x2 h) physical training focusing on aerobic capacity, muscle strength, core stability, proprioception | No separate program for adolescents with pain complaints related to hypermobility |
| Exposure Program (n = 25) | Care as Usual (n = 28) | Total (n = 53) | |
|---|---|---|---|
| Age (years) − mean (SD) | 15.9 (1.99) | 16.2 (1.79) | 16.0 (1.87) |
| Sex (female) − n (%) | 24 (96) | 25 (89) | 49 (92) |
| Relative with pain complaints − n (% *) | 13 (62) (4 missing) | 15 (60) (3 missing) | 28 (61) |
| Other health issues − n (% *) | 8 (38) (4 missing) | 11 (44) (3 missing) | 19 (41) |
| Onset of current pain complaints − n (% *) | (4 missing) | (4 missing) | (8 missing) |
| <1 year ago | 5 (24) | 12 (50) | 17 (38) |
| 1–5 years ago | 14 (67) | 11 (46) | 25 (56) |
| >5 years ago | 2 (10) | 1 (4) | 3 (7) |
| Problems with sleep − n (%) | 14 (67) (4 missing) | 17 (68) (3 missing) | 31 (67) (7 missing) |
| Education − n (% *) | (3 missing) | (3 missing) | (6 missing) |
| Low | 11 (50) | 16 (64) | 27 (58) |
| Middle | 5 (23) | 6 (24) | 11 (23) |
| High | 6 (27) | 3 (12) | 9 (19) |
| Absence at school in the past year − n (% *) | (3 missing) | (3 missing) | (6 missing) |
| 0–14 days | 14 (64) | 15 (60) | 29 (62) |
| 15–30 days | 3 (14) | 1 (4) | 4 (9) |
| 1–3 months | 2 (9) | 6 (24) | 8 (17) |
| 4–6 months | 2 (9) | 1 (4) | 3 (6) |
| 7–12 months | 1 (4) | 2 (8) | 3 (6) |
| FDI (scored 0–60) − mean (SD) | 24.7 (10.3) | 23.1 (8.1) | 23.8 (9.1) |
| QLA-CP (scored 0–3) − mean (SD) | |||
| Domain Psychological Functioning | 1.57 (0.47) | 1.67 (0.51) | 1.62 (0.49) |
| Domain Functional Status | 1.74 (0.53) | 1.86 (0.44) | 1.80 (0.48) |
| Domain Physical Status | 1.81 (0.63) | 1.76 (0.64) | 1.78 (0.63) |
| Domain Social Functioning | 1.72 (0.60) | 1.81 (0.59) | 1.77 (0.59) |
| FOPQ (scored 0–96) − mean (SD) | 40.1 (16.7) | 38.7 (13.7) | 39.3 (15.0) |
| PCS-C (scored 0–52) − mean (SD) | 22.1 (11.0) | 20.3 (9.5) | 21.1 (10.2) |
| CDI (scored 0–54) − mean (SD) | 26.1 (2.55) | 25.7 (2.53) | 25.9 (2.51) |
| VAS (0–100) − mean (SD) | 53 (14) | 55 (22) | 54 (18) |
| PHODA-Youth (scored 0–510) − mean (SD) | 191 (121) | 180 (119) | 185 (119) |
| Credibility (CEQ, scored 3–27) − mean (SD) | 17.7 (5.1) | 18.3 (5.2) | 18.0 (5.0) |
| Expectancy (CEQ, scored 2–18) − mean (SD) | 13.2 (2.6) | 12.5 (3.5) | 12.8 (3.1) |
| Estimated Mean Difference * (95% CI); p-Value | ||||
|---|---|---|---|---|
| At 2 months (n = 43) | At 4 months (n = 37) | At 10 months (n = 22) | At 12 months (n = 22) | |
| FDI | −9.96 (−15.39 to −4.53); 0.000 | −9.16 (−14.79 to −3.52); 0.002 | −10.09 (−17.17 to −3.01); 0.006 | −8.81 (−15.59 to −2.044); 0.011 |
| FOPQ | −3.61 (−12.60 to 5.37); 0.427 | −8.00 (−17.26 to 1.26); 0.090 | −6.43 (−18.16 to 5.31); 0.280 | −8.08 (−19.21 to 3.044); 0.153 |
| PHODA-Youth | −82.19 (−131.06 to −33.32); 0.001 | −108.62 (−159.21 to −58.03); 0.000 | −134.32 (−203.17 to −65.46); 0.000 | −96.12 (−157.63 to −34.61); 0.002 |
| PCS-C | −5.86 (−11.42 to −0.30); 0.039 | −4.96 (−10.75 to 0.83); 0.092 | −4.89 (−12.15 to 2.37); 0.185 | −5.58 (−12.46 to 1.31); 0.112 |
| CDI | −1.57 (−5.04 to 1.90); 0.371 | −1.14 (−4.72 to 2.44); 0.530 | −6.16 (−10.70 to −1.62); 0.008 | −3.27 (−7.57 to 1.03); 0.135 |
| Pain intensity | −11.80 (−24.70 to 1.10); 0.073 | −14.88 (−28.08 to −1.67); 0.028 | −21.94 (−39.76 to −4.13); 0.016 | −10.74 (−26.79 to 5.30); 0.187 |
| QLA − Psychological Functioning | 5.55 (0.15 to 10.95); 0.044 | 3.90 (−1.71 to 9.51); 0.171 | 7.58 (0.49 to 14.66); 0.036 | 4.94 (−1.79 to 11.68); 0.149 |
| QLA − Functional Status | 3.96 (1.12 to 6.80); 0.007 | 3.63 (0.68 to 6.58); 0.016 | 3.71 (−0.01 to 7.43); 0.051 | 3.52 (−0.01 to 7.06); 0.051 |
| QLA − Physical Status | 0.62 (−1.51 to 2.75); 0.567 | 0.66 (−1.56 to 2.87); 0.559 | 0.77 (−2.01 to 3.55); 0.585 | 1.02 (−1.64 to 3.68); 0.448 |
| QLA − Social Functioning | −0.25 (−4.55 to 4.05); 0.909 | 2.88 (−1.30 to 7.07); 0.176 | 2.74 (−2.85 to 8.33); 0.334 | 1.97 (−3.37 to 7.31); 0.467 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dekker, C.; Goossens, M.; Winkens, B.; Remerie, S.; Bastiaenen, C.; Verbunt, J. Functional Disability in Adolescents with Chronic Pain: Comparing an Interdisciplinary Exposure Program to Usual Care. Children 2020, 7, 288. https://0-doi-org.brum.beds.ac.uk/10.3390/children7120288
Dekker C, Goossens M, Winkens B, Remerie S, Bastiaenen C, Verbunt J. Functional Disability in Adolescents with Chronic Pain: Comparing an Interdisciplinary Exposure Program to Usual Care. Children. 2020; 7(12):288. https://0-doi-org.brum.beds.ac.uk/10.3390/children7120288
Chicago/Turabian StyleDekker, Carolien, Mariëlle Goossens, Bjorn Winkens, Silvia Remerie, Caroline Bastiaenen, and Jeanine Verbunt. 2020. "Functional Disability in Adolescents with Chronic Pain: Comparing an Interdisciplinary Exposure Program to Usual Care" Children 7, no. 12: 288. https://0-doi-org.brum.beds.ac.uk/10.3390/children7120288