A Model for a Standardized and Sustainable Pediatric Anesthesia-Intensive Care Unit Hand-Off Process

Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting
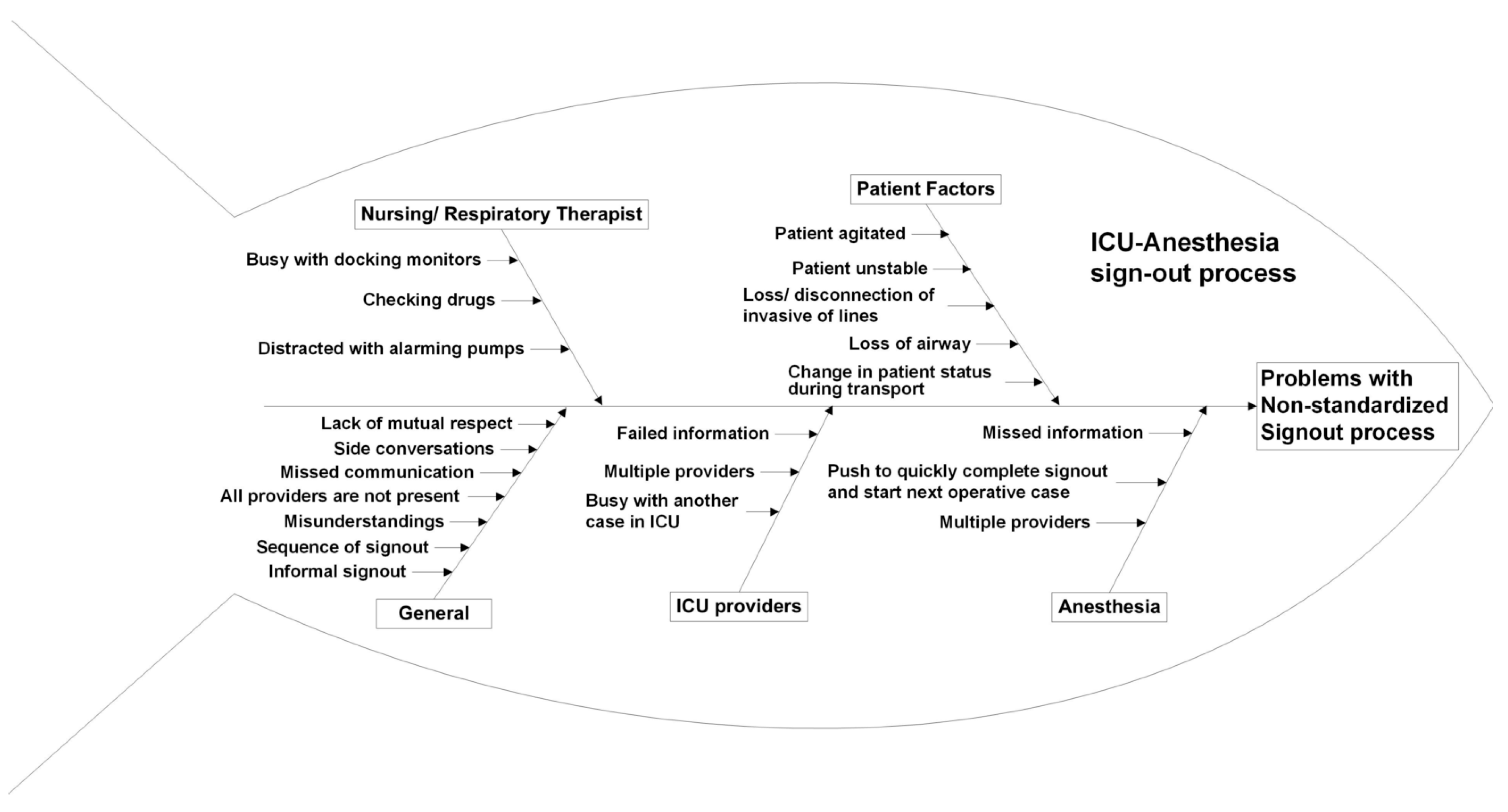
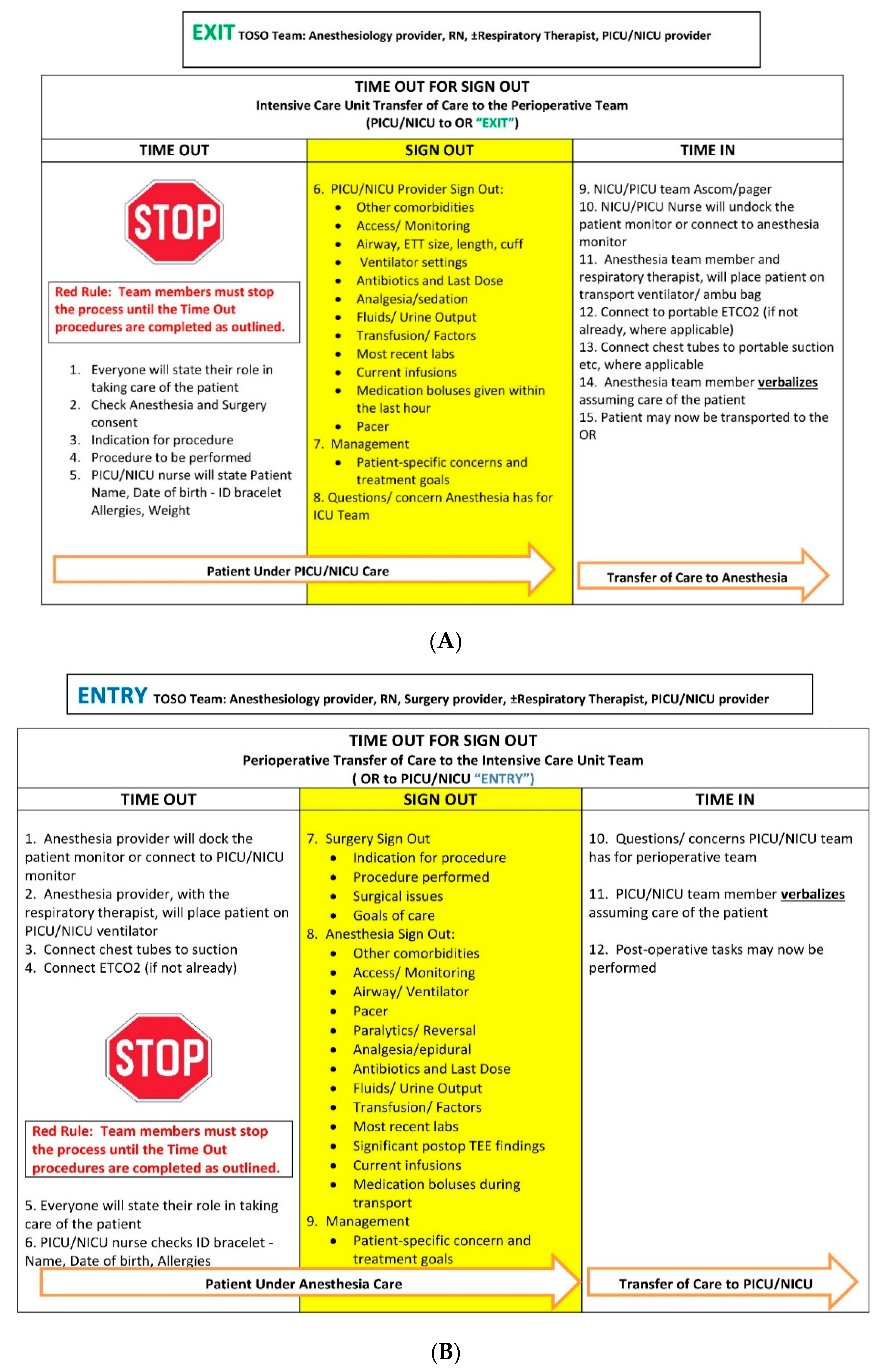
2.2. Planning the Intervention
2.3. Assessing the Intervention
2.3.1. Survey
- (1)
- What Unit do you work in?
- (2)
- What is your role?
- (3)
- How many years have you worked in your current unit?
- (4)
- The time out for sign out process provides the necessary information about the patient.
- (5)
- The sign out system makes it comfortable for you to ask question to the OR/ICU team members.
- (6)
- The sign out system is efficient and limits needless information about patient care.
- (7)
- At the end of the time out for sign out, do you feel like the sign out was a necessary and important part of patient care?
- (8)
- Do you feel the time out for sign out can be improved?
2.3.2. Audit
2.4. Statistical Analysis
3. Results
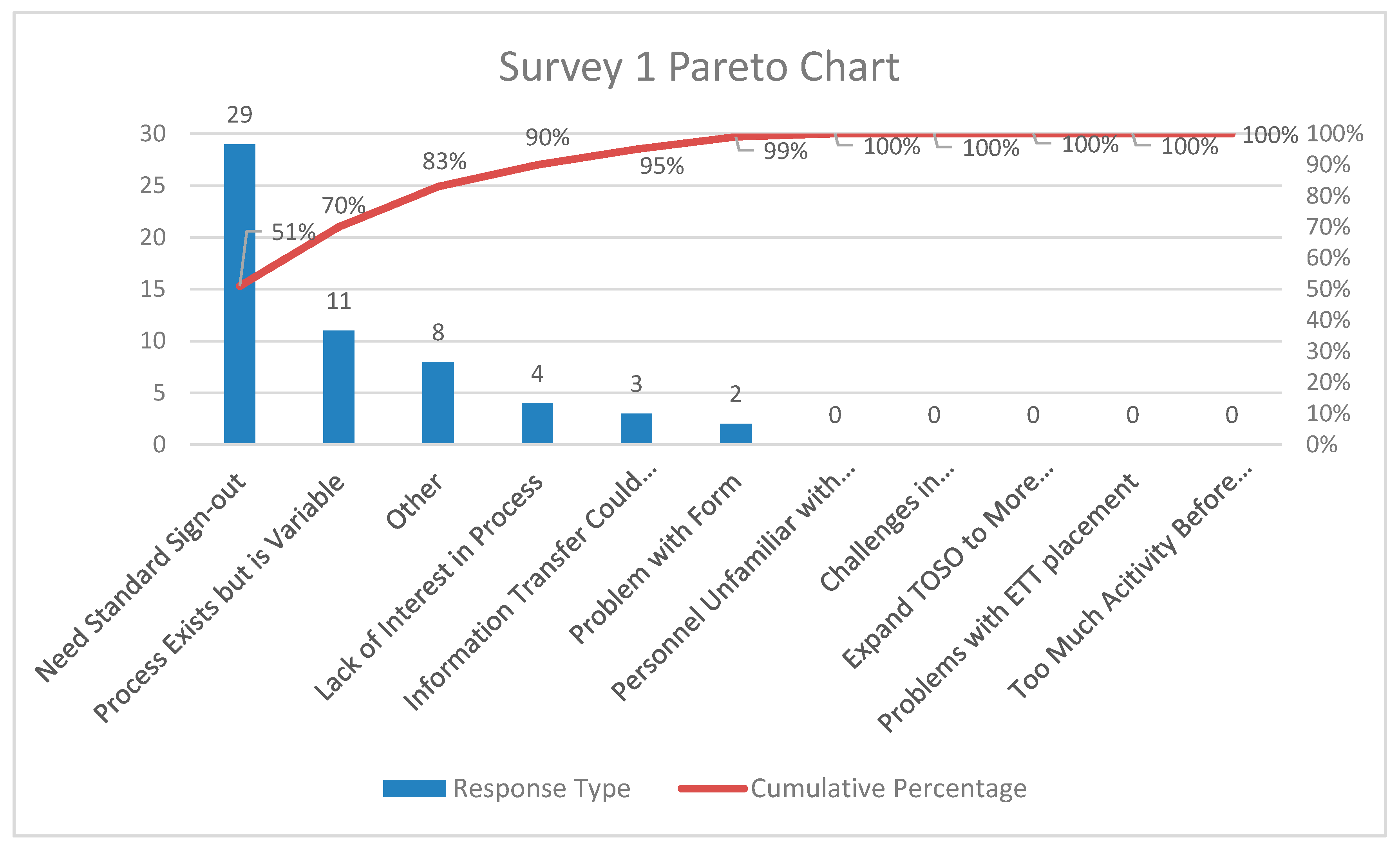
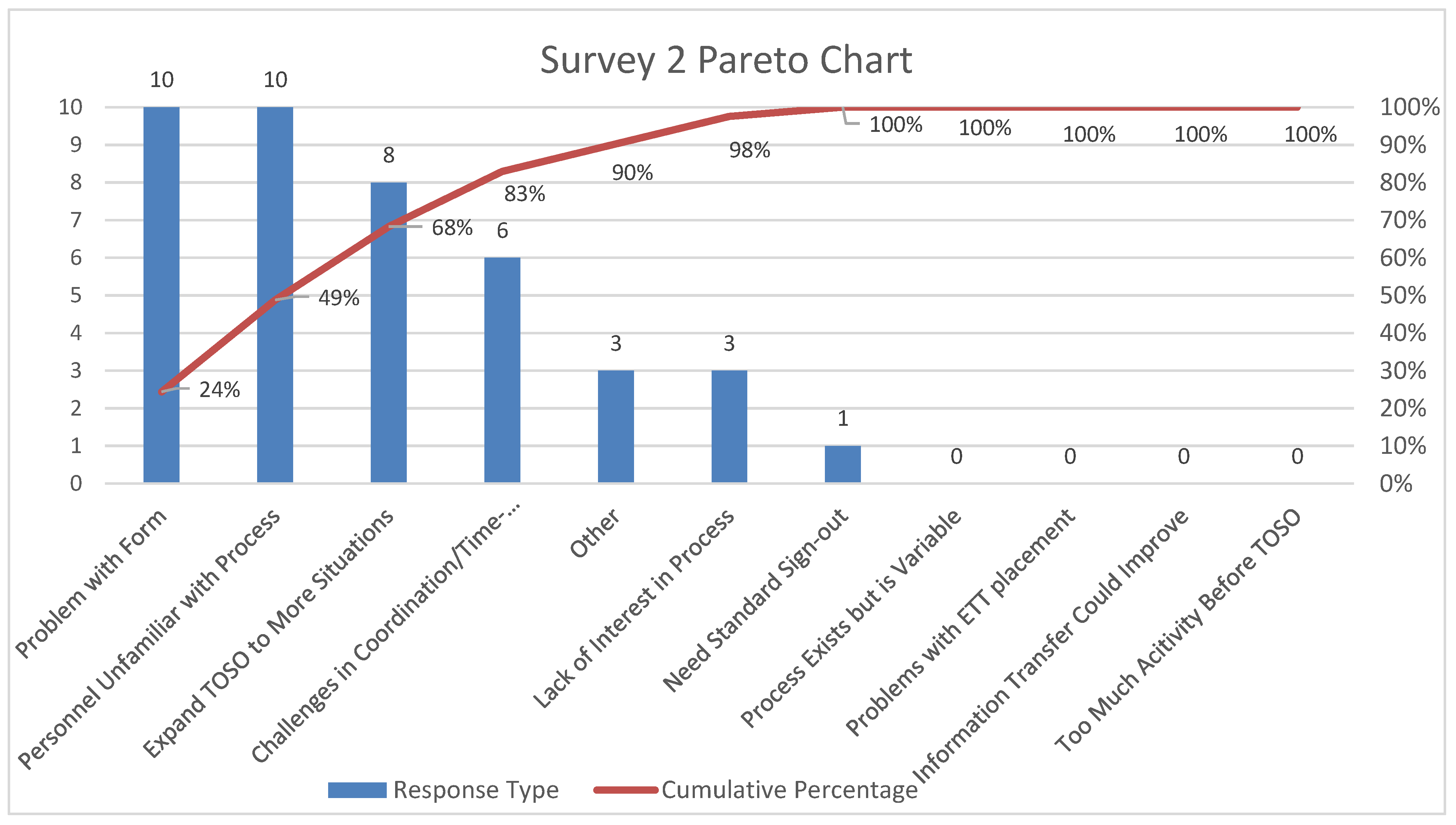
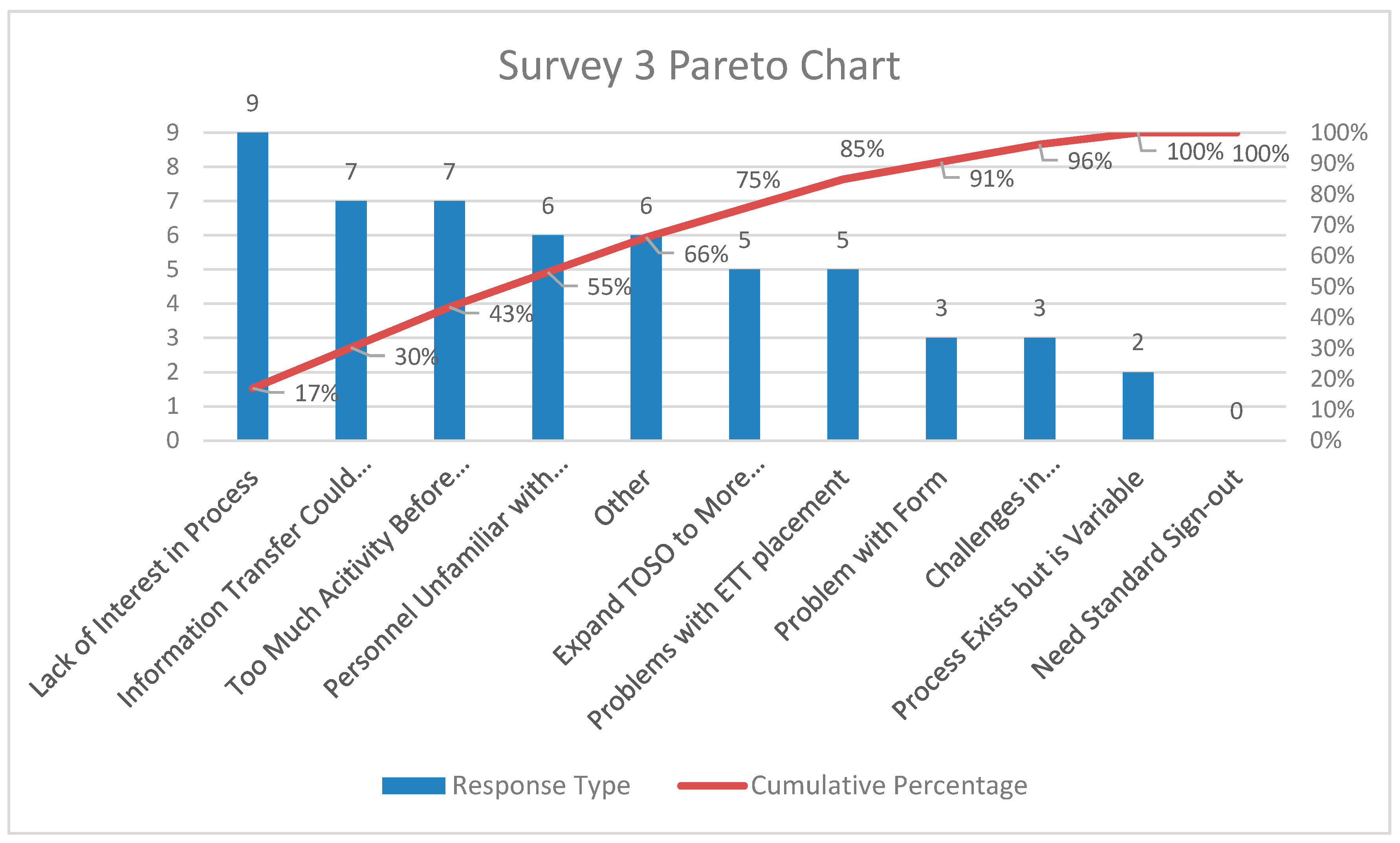
3.1. Survey Results
3.2. Audit Results
4. Discussion
Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
- Comorbidities
- Access—peripheral central venous arterial line
- ETT/tracheostomy-size length cuffed/uncuffed
- Ventilator settingsFiO2 Mode Paw TV PS PEEP
- IV infusions
- Medications due for Operating room
- Availability of blood/blood products
- Last set of labsHb/Hct Blood glucose
- Post-operative plan for ventilation
- Any issues/concernsICU attending, contact # ICU resident contact #
- Airway ETT size type length issues
- Recommended Ventilation settings, FiO2 Paw TV Ventilation mode PEEP
- New access established in OR
- Anesthetic agents used
- Last dose of narcotics, anesthetic agent, sedative or neuromuscular blocking agent
- Analgesics in OR—acetaminophen, narcotics, regional block and infiltration of surgical wound
- Reversal agents administered
- If epidural—plan, drug, infusion rate
- Antibiotics administered in OR, dose and time
- IV infusions—inotropes, dosage rate
- Total fluids administered
- Blood or blood products Estimated blood loss
- Intraoperative labs blood glucose
- CP bypass, times
- Any specific issues and concernsAttending Anesthesiologist contact # Anesthesia Resident contact #
References
- The Joint Commission. Handsoff Communications: Toolkit for Implementing the National Patient Safety Goal; Joint Commission Resources: Oak Brook, IL, USA, 2008; Volume 65. [Google Scholar]
- Horwitz, L.I.; Meredith, T.; Schuur, J.D.; Shah, N.R.; Kulkarni, R.G.; Jenq, G.Y. Dropping the baton: A qualitative analysis of failures during the transition from emergency department to inpatient care. Ann. Emerg. Med. 2009, 53, 701–710.e4. [Google Scholar] [CrossRef]
- Krimminger, D.; Sona, C.; Thomas-Horton, E.; Schallom, M. A Multidisciplinary QI Initiative to Improve OR-ICU Handovers. Am. J. Nurs. 2018, 118, 48–59. [Google Scholar] [CrossRef] [PubMed]
- Petrovic, M.A.; Aboumatar, H.; Baumgartner, W.A.; Ulatowski, J.A.; Moyer, J.; Chang, T.Y.; Camp, M.S.; Kowalski, J.; Senger, C.M.; Martinez, E.A. Pilot implementation of a perioperative protocol to guide operating room-to-intensive care unit patient handoffs. J. Cardiothorac. Vasc. Anesth. 2012, 26, 11–16. [Google Scholar] [CrossRef]
- Pickering, B.W.; Hurley, K.; Marsh, B. Identification of patient information corruption in the intensive care unit: Using a scoring tool to direct quality improvements in handover. Crit. Care Med. 2009, 37, 2905–2912. [Google Scholar] [CrossRef]
- Boat, A.C.; Spaeth, J.P. Handoff checklists improve the reliability of patient handoffs in the operating room and postanesthesia care unit. Paediatr. Anaesth. 2013, 23, 647–654. [Google Scholar] [CrossRef]
- Karamchandani, K.; Fitzgerald, K.; Carroll, D.; Trauger, M.E.; Ciccocioppo, L.A.; Hess, W.; Prozesky, J.; Armen, S.B. A Multidisciplinary Handoff Process to Standardize the Transfer of Care Between the Intensive Care Unit and the Operating Room. Qual. Manag. Health Care 2018, 27, 215–222. [Google Scholar] [CrossRef]
- Joint Commission Center for Transforming Healthcare Releases Targeted Solutions Tool for Hand-Off Communications. Joint Comm. Perspect. 2012, 32. Available online: https://www.jointcommission.org/-/media/deprecated-unorganized/imported-assets/tjc/system-folders/blogs/tst_hoc_persp_08_12pdf.pdf?db=web&hash=BA7C8CDB4910EF6633F013D0BC08CB1C (accessed on 2 September 2020).
- Petrovic, M.A.; Martinez, E.A.; Aboumatar, H. Implementing a perioperative handoff tool to improve postprocedural patient transfers. Jt. Comm. J. Qual. Patient Saf. 2012, 38, 135–142. [Google Scholar] [CrossRef]
- Catchpole, K.R.; de Leval, M.R.; McEwan, A.; Pigott, N.; Elliott, M.J.; McQuillan, A.; MacDonald, C.; Goldman, A.J. Patient handover from surgery to intensive care: Using Formula 1 pit-stop and aviation models to improve safety and quality. Paediatr. Anaesth. 2007, 17, 470–478. [Google Scholar] [CrossRef] [PubMed]
- Craig, R.; Moxey, L.; Young, D.; Spenceley, N.S.; Davidson, M.G. Strengthening handover communication in pediatric cardiac intensive care. Paediatr. Anaesth. 2012, 22, 393–399. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, G.C.; McGeorge, P.; Flin, R.H.; Glavin, R.J.; Maran, N.J. The role of non-technical skills in anaesthesia: A review of current literature. Br. J. Anaesth. 2002, 88, 418–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donchin, Y.; Gopher, D.; Olin, M.; Badihi, Y.; Biesky, M.; Sprung, C.L.; Pizov, R.; Cotev, S. A look into the nature and causes of human errors in the intensive care unit. 1995. Qual. Saf. Health Care 2003, 12, 143–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horwitz, L.I.; Moin, T.; Krumholz, H.M.; Wang, L.; Bradley, E.H. Consequences of inadequate sign-out for patient care. Arch. Intern. Med. 2008, 168, 1755–1760. [Google Scholar] [CrossRef] [PubMed]
- Chenault, K.; Moga, M.A.; Shin, M.; Petersen, E.; Backer, C.; De Oliveira, G.S., Jr.; Suresh, S. Sustainability of protocolized handover of pediatric cardiac surgery patients to the intensive care unit. Paediatr. Anaesth. 2016, 26, 488–494. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, H.S.; Saville, B.R.; Slayton, J.M.; Donahue, B.S.; Daves, S.; Christian, K.G.; Bichell, D.P.; Harris, Z.L. Standardized postoperative handover process improves outcomes in the intensive care unit: A model for operational sustainability and improved team performance. Crit. Care Med. 2012, 40, 2109–2115. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Survey Questions | Answer Options | Survey 1 Response % n = 113 | Survey 2 Response % n = 85 | Survey 3 Response % n = 135 | p-Value, Chi-Square Test |
|---|---|---|---|---|---|
| Question 1, Unit of the Provider | Anesthesia | 27 | 29 | 40 | p = 0.258 |
| NICU | 38 | 38 | 28 | ||
| Pediatric Surgery | 3 | 1 | 4 | ||
| PICU | 32 | 32 | 28 | ||
| Question 2, Provider role | Nurse | 40 | 53 | 23 | p < 0.001 |
| CRNP/PA | 6 | 7 | 8 | ||
| Attending Physician | 21 | 22 | 23 | ||
| CRNA | 4 | 1 | 11 | ||
| Resident/Fellow | 16 | 17 | 22 | ||
| Respiratory Therapist | 13 | 0 | 13 | ||
| Question 3, Provider Experience | <2 years | 19 | 29 | 26 | p = 0.43 |
| >2 years to <4 years | 30 | 21 | 31 | ||
| ≥4 years | 51 | 50 | 43 |
| Survey Question | Survey 1 n = 113 | Survey 2 n = 85 | Survey 3 n = 135 | p-Value, Chi Square Test |
|---|---|---|---|---|
| Question 4 (Provides Necessary Information), % | 40.5 | 90.5 | 89.5 | <0.001 |
| Question 5 (Comfortable to Ask Questions), % | 47.8 | 75.3 | 83.7 | <0.001 |
| Question 6 (Efficient and Limits Needless Information), % | 30.4 | 64.7 | 70.6 | <0.001 |
| Question 7 (Necessary and Important), % | 65.1 | 79.7 | 80.7 | 0.237 |
| Audit 1 (Pre-Implementation) n = 27 | Audit 2 (Six Months Post-Implementation) n = 55 | Audit 3 (>2 Years Post-Implementation) n = 38 | p-Value, Chi-Square Test | |
|---|---|---|---|---|
| Formal Hand-off Process Occurred, % | 88.8 | 91 | 94.7 | 0.08 |
| Full Completion of Hand-off, % | 44.4 | 87.2 | 81.5 | <0.001 |
| Items Missed during Hand-off, % | 22 | 9 | 5 | <0.001 |
| Laboratory Values Information Missed, n (%) | 10 (37) | 7 (12.5) | 6 (15.7) | 0.032 |
| Airway Ventilation Information Missed | 5 (18.5) | 5 (8.9) | 1 (2.6) | 0.09 |
| Medication Information Missed | 5 (18.5) | 5 (8.9) | 3 (7.8) | 0.339 |
| Time for Completion of Hand-off, Median, IQR; Minutes | 5 (3, 8) | 5 (3.75, 7) | 6 (5, 9.75) | 0.251 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dalal, P.G.; Cios, T.J.; DeMartini, T.K.M.; Prasad, A.A.; Whitley, M.C.; Clark, J.B.; Lin, L.; Mujsce, D.J.; Cilley, R.E. A Model for a Standardized and Sustainable Pediatric Anesthesia-Intensive Care Unit Hand-Off Process. Children 2020, 7, 123. https://0-doi-org.brum.beds.ac.uk/10.3390/children7090123
Dalal PG, Cios TJ, DeMartini TKM, Prasad AA, Whitley MC, Clark JB, Lin L, Mujsce DJ, Cilley RE. A Model for a Standardized and Sustainable Pediatric Anesthesia-Intensive Care Unit Hand-Off Process. Children. 2020; 7(9):123. https://0-doi-org.brum.beds.ac.uk/10.3390/children7090123
Chicago/Turabian StyleDalal, Priti G., Theodore J. Cios, Theodore K. M. DeMartini, Amit A. Prasad, Meghan C. Whitley, Joseph B. Clark, Leon Lin, Dennis J. Mujsce, and Robert E. Cilley. 2020. "A Model for a Standardized and Sustainable Pediatric Anesthesia-Intensive Care Unit Hand-Off Process" Children 7, no. 9: 123. https://0-doi-org.brum.beds.ac.uk/10.3390/children7090123