Safety and Effects of the Rapid Maxillary Expander on Temporomandibular Joint in Subjects Affected by Juvenile Idiopathic Arthritis: A Retrospective Study

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Type of Participants and Inclusion Criteria
2.2. Cephalometric Analysis
2.3. Statistical Analysis
3. Results
3.1. Linear Measurements
3.2. Symmetry Indexes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Giancane, G.; Consolaro, A.; Lanni, S.; Davì, S.; Schiappapietra, B.; Ravelli, A. Juvenile Idiopathic Arthritis: Diagnosis and Treatment. Rheumatol. Ther. 2016, 3, 187–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ugolini, A.; Doldo, T.; Huanca Ghislanzoni, L.T.; Mapelli, A.; Giorgetti, R.; Sforza, C.; Fastuca, R.; Lorusso, P.; Lagravère, M.O.; Michelotti, A.; et al. Dentoskeletal outcomes of a rapid maxillary expander with differential opening in patients with bilateral cleft lip and palate: A prospective clinical trial. Am. J. Orthod. Dentofac. Orthop. 2017, 17, 1–7. [Google Scholar] [CrossRef]
- von Bremen, J.; Ruf, S. Orthodontic and dentofacial orthopedic management of juvenile idiopathic arthritis: A systematic review of the literature. Orthod. Craniofacial Res. 2011, 14, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Müller, L.; Kellenberger, C.J.; Cannizzaro, E.; Ettlin, D.; Schraner, T.; Bolt, I.B.; Peltomäki, T.; Saurenmann, R.K. Early diagnosis of temporomandibular joint involvement in juvenile idiopathic arthritis: A pilot study comparing clinical examination and ultrasound to magnetic resonance imaging. Rheumatology 2009. [Google Scholar] [CrossRef] [Green Version]
- Maspero, C.; Cavagnetto, D.; Abate, A.; Cressoni, P.; Farronato, M. Effects on the Facial Growth of Rapid Palatal Expansion in Growing Patients Affected by Juvenile Idiopathic Arthritis with Monolateral Involvement of the Temporomandibular Joints: A Case-Control Study on Posteroanterior and Lateral Cephalograms. J. Clin. Med. 2020, 9, 1159. [Google Scholar] [CrossRef]
- Billiau, A.D.; Hu, Y.; Verdonck, A.; Carels, C.; Wouters, C. Temporomandibular joint arthritis in juvenile idiopathic arthritis: Prevalence, clinical and radiological signs, and relation to dentofacial morphology. J. Rheumatol. 2007, 34, 1925–1933. [Google Scholar]
- De Carvalho, R.T.; Braga, F.S.F.F.; Brito, F.; Capelli Junior, J.; Figueredo, C.M.; Sztajnbok, F.R. Temporomandibular joint alterations and their orofacial complications in patients with juvenile idiopathic arthritis. Braz. J. Rheumatol. 2012, 52, 907–911. [Google Scholar]
- Hsieh, Y.J.; Darvann, T.A.; Hermann, N.V.; Larsen, P.; Liao, Y.F.; Bjoern-Joergensen, J.; Kreiborg, S. Facial morphology in children and adolescents with juvenile idiopathic arthritis and moderate to severe temporomandibular joint involvement. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 182–191. [Google Scholar] [CrossRef]
- Farronato, M.; Cavagnetto, D.; Abate, A.; Cressoni, P.; Fama, A.; Maspero, C. Assessment of condylar volume and ramus height in JIA patients with unilateral and bilateral TMJ involvement: Retrospective case-control study. Clin. Oral Investig. 2020, 24, 2635–2643. [Google Scholar] [CrossRef]
- Maspero, C.; Farronato, M.; Bellincioni, F.; Cavagnetto, D.; Abate, A. Assessing mandibular body changes in growing subjects: A comparison of CBCT and reconstructed lateral cephalogram measurements. Sci. Rep. 2020, 10, 1–12. [Google Scholar] [CrossRef]
- Ronchezel, M.V.; Hilario, M.O.E.; Goldenberg, J.; Lederman, H.M.; Faltin, K.; De Azevedo, M.F.; Naspitz, C.K. Temporomandibular joint and mandibular growth alterations in patients with juvenile rheumatoid arthritis. J. Rheumatol. 1995, 22, 1956–1961. [Google Scholar] [PubMed]
- Sidiropoulou-Chatzigianni, S.; Papadopoulos, M.A.; Kolokithas, G. Dentoskeletal morphology in children with juvenile idiopathic arthritis compared with healthy children. J. Orthod. 2001. [Google Scholar] [CrossRef] [PubMed]
- Lanteri, V.; Farronato, M.; Ugolini, A.; Cossellu, G.; Gaffuri, F.; Parisi, F.M.R.; Cavagnetto, D.; Abate, A.; Maspero, C. Volumetric Changes in the Upper Airways after Rapid and Slow Maxillary Expansion in Growing Patients: A Case-Control Study. Materials 2020, 13, 2239. [Google Scholar] [CrossRef] [PubMed]
- Maspero, C.; Farronato, M.; Bellincioni, F.; Annibale, A.; Machetti, J.; Abate, A.; Cavagnetto, D. Three-Dimensional Evaluation of Maxillary Sinus Changes in Growing Subjects: A Retrospective Cross-Sectional Study. Materials 2020, 13, 1007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quartier, P. Current treatments for juvenile idiopathic arthritis. Jt. Bone Spine 2010, 77, 511–516. [Google Scholar] [CrossRef]
- Te Veldhuis, E.C.; Te Veldhuis, A.H.; Koudstaal, M.J. Treatment Management of Children with Juvenile Idiopathic Arthritis with Temporomandibular Joint Involvement: A Systematic Review; Elsevier: Amsterdam, The Netherlands, 2014; Volume 117. [Google Scholar]
- Kjellberg, H. Juvenile chronic arthritis. Dentofacial morphology, growth, mandibular function and orthodontic treatment. Swed. Dent. J. Suppl. 1995, 109, 1–56. [Google Scholar]
- Stoustrup, P.; Twilt, M.; Spiegel, L.; Kristensen, K.D.; Koos, B.; Pedersen, T.K.; Küseler, A.; Cron, R.Q.; Abramowicz, S.; Verna, C.; et al. Clinical orofacial examination in juvenile idiopathic arthritis: International consensus-based recommendations for monitoring patients in clinical practice and research studies. J. Rheumatol. 2017, 44, 326–333. [Google Scholar] [CrossRef]
- Farronato, G.; Giannini, L.; Galbiati, G.; Maspero, C. A 5-year longitudinal study of survival rate and periodontal parameter changes at sites of dilacerated maxillary central incisors. Prog. Orthod. 2014, 15, 3. [Google Scholar] [CrossRef] [Green Version]
- Farronato, G.; Giannini, L.; Galbiati, G.; Cannalire, P.; Martinelli, G.; Tubertini, I.; Maspero, C. Oral tissues and orthodontic treatment: Common side effects. Minerva Stomatol. 2013, 62, 431–446. [Google Scholar]
- González, M.F.O.; Pedersen, T.K.; Dalstra, M.; Herlin, T.; Verna, C. 3D evaluation of mandibular skeletal changes in juvenile arthritis patients treated with a distraction splint: A retrospective follow-up. Angle Orthod. 2016, 86, 846–853. [Google Scholar] [CrossRef] [Green Version]
- Kjellberg, H.; Kiliaridis, S.; Thilander, B. Dentofacial growth in orthodontically treated and untreated children with juvenile chronic arthritis (JCA). A comparison with Angle Class II division 1 subjects. Eur. J. Orthod. 1995, 17, 357–373. [Google Scholar] [CrossRef] [PubMed]
- Stoustrup, P.; Pedersen, T.K.; Nørholt, S.E.; Resnick, C.M.; Abramowicz, S. Interdisciplinary Management of Dentofacial Deformity in Juvenile Idiopathic Arthritis. Oral Maxillofac. Surg. Clin. N. Am. 2020, 32, 117–134. [Google Scholar] [CrossRef] [PubMed]
- Macedo de Menezes, L.; Deon Rizzatto, S.M.; Martinelli Santayana de Lima, E.; Baccarin Matje, P.R.; Picarelli, M.M. Juvenile idiopatic arthritis in orthodontics: Case report with a 6-year follow-up. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 384–396. [Google Scholar] [CrossRef] [PubMed]
- Lanteri, V.; Cavagnetto, D.; Abate, A.; Mainardi, E.; Gaffuri, F.; Ugolini, A.; Maspero, C. Buccal Bone Changes Around First Permanent Molars and Second Primary Molars after Maxillary Expansion with a Low Compliance Ni-Ti Leaf Spring Expander. Int. J. Environ. Res. Public Health 2020, 17, 9104. [Google Scholar] [CrossRef]
- McNamara, J.A.; Brudon, W.L. Orthodontic and Orthopedic Treatment in the Mixed Dentition; Needham Press: Needham, MA, USA, 1993; ISBN 0963502212. [Google Scholar]
- Farronato, G.; Giannini, L.; Galbiati, G.; Maspero, C. Sagittal and vertical effects of rapid maxillary expansion in Class I, II, and III occlusions. Angle Orthod. 2011. [Google Scholar] [CrossRef] [PubMed]
- Ciancaglini, R.; Gherlone, E.F.; Redaelli, S.; Radaelli, G. The distribution of occlusal contacts in the intercuspal position and temporomandibular disorder. J. Oral Rehabil. 2002, 29, 1082–1090. [Google Scholar] [CrossRef]
- Ciancaglini, R.; Gherlone, E.F.; Radaelli, G. Unilateral temporomandibular disorder and asymmetry of occlusal contacts. J. Prosthet. Dent. 2003, 89, 180–185. [Google Scholar] [CrossRef]
- Wang, C.; Yin, X. Occlusal risk factors associated with temporomandibular disorders in young adults with normal occlusions. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2012, 114, 419–423. [Google Scholar] [CrossRef]
- Masi, M.; Lederman, H.M.; Yamashita, H.K.; de Arruda Aidar, L.A. Temporomandibular joint evaluation with magnetic resonance imaging in children with functional unilateral posterior crossbite, treated with rapid maxillary expansion. Am. J. Orthod. Dentofac. Orthop. 2009, 136, 207–217. [Google Scholar] [CrossRef]
- Arat, F.E.; Arat, Z.M.; Tompson, B.; Tanju, S. Muscular and condylar response to rapid maxillary expansion. Part 3: Magnetic resonance assessment of condyle-disc relationship. Am. J. Orthod. Dentofac. Orthop. 2008, 133, 830–836. [Google Scholar] [CrossRef]
- Leonardi, R.; Caltabiano, M.; Cavallini, C.; Sicurezza, E.; Barbato, E.; Spampinato, C.; Giordano, D. Condyle fossa relationship associated with functional posterior crossbite, before and after rapid maxillary expansion. Angle Orthod. 2012, 82, 1040–1046. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fama, A.; Cavagnetto, D.; Abate, A.; Mainardi, E.; De Filippis, A.; Esposito, L. Treatment of dental dilacerations. Narrative review. Dent. Cadmos 2020, in press. [Google Scholar]
- Baratieri, C.; Alves, M.; Bolognese, A.M.; Nojima, M.C.G.; Nojima, L.I. Changes in skeletal and dental relationship in Class II Division I malocclusion after rapid maxillary expansion: A prospective study. Dental Press J. Orthod. 2014, 19, 75–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maspero, C.; Fama, A.; Cavagnetto, D.; Abate, A.; Farronato, M. Treatment of dental dilacerations. J. Biol. Regul. Homeost. Agents 2019, 33, 1623–1627. [Google Scholar] [PubMed]
- Lima Filho, R.M.A.; Carlos, A.; Ruellas, O. Mandibular Behavior with Slow and Rapid Maxillary Expansion in Skeletal Class II Patients A Long-Term Study. Angle Orthod. 2007, 77. [Google Scholar] [CrossRef]
- Maspero, C.; Galbiati, G.; Del Rosso, E.; Farronato, M.; Giannini, L. RME: Effects on the nasal septum. A CBCT evaluation. Eur. J. Paediatr. Dent. 2019, 20, 123–126. [Google Scholar] [CrossRef]
- Abate, A.; Cavagnetto, D.; Fama, A.; Matarese, M.; Lucarelli, D.; Assandri, F. Short term effects of rapid maxillary expansion on breathing function assessed with spirometry: A case-control study. Saudi Dent. J. 2020. [Google Scholar] [CrossRef]
- Petty, R.E.; Southwood, T.R.; Manners, P.; Baum, J.; Glass, D.N.; Goldenberg, J.; He, X.; Maldonado-Cocco, J.; Orozco-Alcala, J.; Prieur, A.M.; et al. International League of Associations for Rheumatology Classification of Juvenile Idiopathic Arthritis: Second Revision, Edmonton, 2001. J. Rheumatol. 2004, 31, 390. [Google Scholar]
- Rongo, R.; Alstergren, P.; Ammendola, L.; Bucci, R.; Alessio, M.; D’Antò, V.; Michelotti, A. Temporomandibular joint damage in juvenile idiopathic arthritis: Diagnostic validity of diagnostic criteria for temporomandibular disorders. J. Oral Rehabil. 2019. [Google Scholar] [CrossRef]
- Cahill, A.M.; Baskin, K.M.; Kaye, R.D.; Arabshahi, B.; Cron, R.Q.; Dewitt, E.M.; Bilaniuk, L.; Towbin, R.B. CT-guided percutaneous steroid injection for management of inflammatory arthropathy of the temporomandibular joint in children. Am. J. Roentgenol. 2007, 188, 182–186. [Google Scholar] [CrossRef] [Green Version]
- Schiffman, E.L.; Ohrbach, R.; Truelove, E.L.; Tai, F.; Anderson, G.C.; Pan, W.; Gonzalez, Y.M.; John, M.T.; Sommers, E.; List, T.; et al. The Research Diagnostic Criteria for Temporomandibular Disorders. V: Methods used to establish and validate revised Axis I diagnostic algorithms. J. Orofac. Pain 2010, 24, 63–78. [Google Scholar] [PubMed]
- Caprioglio, A.; Bergamini, C.; Franchi, L.; Vercellini, N.; Zecca, P.A.; Nucera, R.; Fastuca, R. Prediction of Class II improvement after rapid maxillary expansion in early mixed dentition. Prog. Orthod. 2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lanteri, V.; Cossellu, G.; Gianolio, A.; Beretta, M.; Lanteri, C.; Cherchi, C.; Farronato, G. Comparison between RME, SME and Leaf Expander in growing patients: A retrospective postero-anterior cephalometric study. Eur. J. Paediatr. Dent. 2018. [Google Scholar] [CrossRef]
- Farronato, G.; Carletti, V.; Maspero, C.; Farronato, D.; Giannini, L.; Bellintani, C. Craniofacial Growth in Children Affected by Juvenile Idiopathic Arthritis Involving the Temporomandibular Joint: Functional Therapy Management. J. Clin. Pediatr. Dent. 2015. [Google Scholar] [CrossRef]
- Resnick, C.M.; Frid, P.; Norholt, S.E.; Stoustrup, P.; Peacock, Z.S.; Kaban, L.B.; Pedersen, T.K.; Abramowicz, S. An Algorithm for Management of Dentofacial Deformity Resulting From Juvenile Idiopathic Arthritis: Results of a Multinational Consensus Conference. J. Oral Maxillofac. Surg. 2019, 1–33. [Google Scholar] [CrossRef] [Green Version]
- Malandris, M.; Mahoney, E.K. Aetiology, diagnosis and treatment of posterior cross-bites in the primary dentition. Int. J. Paediatr. Dent. 2004, 14, 155–166. [Google Scholar]
- Brunetto, D.P.; Sant’Anna, E.F.; Machado, A.W.; Moon, W. Non-surgical treatment of transverse deficiency in adults using microimplant-assisted rapid palatal expansion (MARPE). Dental Press J. Orthod. 2017. [Google Scholar] [CrossRef] [Green Version]
- Maspero, C.; Abate, A.; Cavagnetto, D.; Fama, A.; Stabilini, A.; Farronato, G.; Farronato, M. Operculectomy and spontaneous eruption of impacted second molars: A retrospective study. J. Biol. Regul. Homeost. Agents 2019, 33, 1909–1912. [Google Scholar] [CrossRef]
- Abate, A.; Cavagnetto, D.; Fama, A.; Bellincioni, F.; Assandri, F. Efficacy of Operculectomy in the Treatment of 145 Cases with Unerupted Second Molars: A Retrospective Case–Control Study. Dent. J. 2020, 8, 65. [Google Scholar] [CrossRef]
- Sharma, D.S.; Srivastava, S.; Tandon, S. Preventive orthodontic approach for functional mandibular shift in early mixed dentition: A case report. J. Oral Biol. Craniofacial Res. 2019. [Google Scholar] [CrossRef]
- Abate, A.; Cavagnetto, D.; Fama, A.; Maspero, C.; Farronato, G. Relationship between Breastfeeding and Malocclusion: A Systematic Review of the Literature. Nutrients 2020, 12, 3688. [Google Scholar] [CrossRef] [PubMed]
- Wendling, L. Short-term Skeletal and Dental Effects of the Acrylic-splint Rapid Maxillary Expansion Appliance: A Thesis Submitted in Partial Fulfillment for the Degree of Master of Science in Orthodontics. Master’s Thesis, The University of Michigan, Ann Arbor, MI, USA, 1997. [Google Scholar]
- Alyessary, A.S.; Othman, S.A.; Yap, A.U.J.; Radzi, Z.; Rahman, M.T. Effects of non-surgical rapid maxillary expansion on nasal structures and breathing: A systematic review. Int. Orthod. 2019, 17, 12–19. [Google Scholar] [CrossRef]
- Galbiati, G.; Maspero, C.; Giannini, L.; Tagliatesta, C.; Farronato, G. Functional evaluation in young patients undergoing orthopedical interceptive treatment. Minerva Stomatol. 2016, 65, 276–283. [Google Scholar] [PubMed]
- McNamara, J.A.; Lione, R.; Franchi, L.; Angelieri, F.; Cevidanes, L.H.S.; Darendeliler, M.A.; Cozza, P. The role of rapid maxillary expansion in the promotion of oral and general health. Prog. Orthod. 2015, 16, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maspero, C.; Abate, A.; Bellincioni, F.; Cavagnetto, D.; Lanteri, V.; Costa, A.; Farronato, M. Comparison of a tridimensional cephalometric analysis performed on 3T-MRI compared with CBCT: A pilot study in adults. Prog. Orthod. 2019, 20, 40. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Abbreviation | Definition |
|---|---|
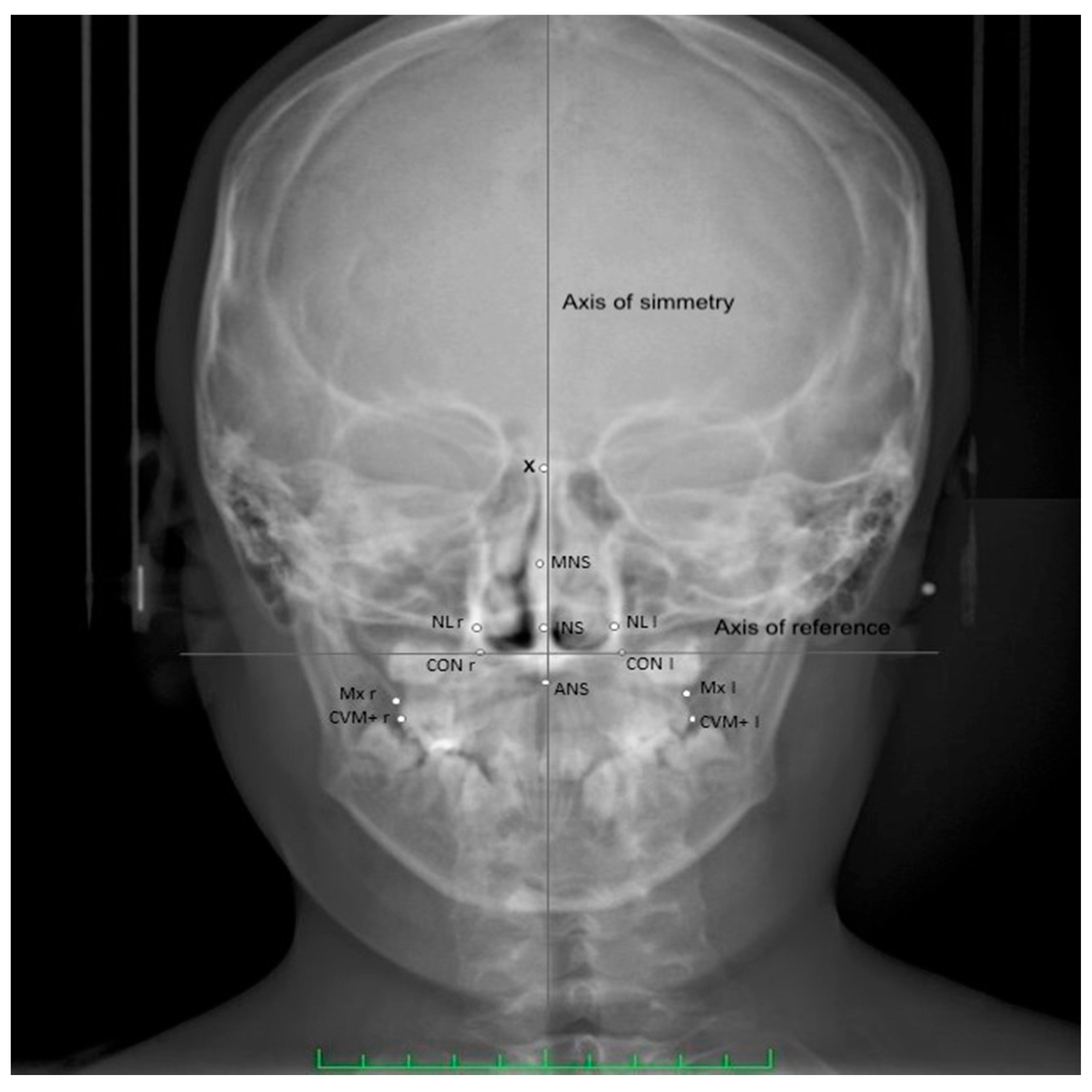
| CVM+ l/r | Most prominent point on the sagittal plane of the vestibular-mesial cuspid-upper left and upper right first permanent molar (left and right) |
| MNS | Middle Nasal Septum-middle point of the maximal diameter of the medium third of nasal septum, on the horizontal plane |
| INS | Inferior part of the Nasal Septum-middle point of the maximal diameter of the inferior third of nasal septum, on the horizontal plane |
| MID | Crossing point between the axis of symmetry and the horizontal straight line that connects the homolog cephalometric points |
| CON | Point of cephalometric congruence between the inferior condyle of the occipital bone and the contour of the great occipital foramen |
| Axis of reference | Axis passing through right and left CON |
| Axis of symmetry | Perpendicular to the reference axis, passing through the highest point of the occipital foramen |
| NL | External points at the maximal horizontal diameter of nasal cavity, left and right |
| X | Crossing point between the perpendicular plate of the ethmoid and the projection of the floor of the anterior cranial fossa floor |
| ANS | Anterior cephalometric nasal spine |
| Mx l/r | The intersection of the lateral contour of the maxillary alveolar process and the lower contour of the maxillozygomatic process of the maxilla (left and right) |
| Characteristics of JIA Group | |
|---|---|
| Sex | 10 men and 15 women |
| Age | Mean age 8.6 ± 1.8 |
| Follow up time | 6 ± 3 months |
| JIA Subtypes | 15 cases oligoarticular JIA, 10 polyarticular JIA |
| Severity of TMJ inflammation | All patients were in Age Grade 3 (Cahill grading system) |
| Disease onset | Mean age of 6.8 ± 1.1 years |
| TMJ involvement at baseline | Negative according to DC-TMD IIIA. All of them were in a quiescent phase of the disease |
| Measurements | TO (n = 25) Mean (SD) | T1 (n = 25) Mean (SD) | Δ T1-T0 | Significance |
|---|---|---|---|---|
| Mx r-l | 59.24 ± 3.03 | 62.31 ± 2.55 | 3.07 | 0.0023 |
| Cvm+ r-l | 56.31 ± 2.73 | 62.40 ± 2.88 | 6.08 | 0.0089 |
| NL r-l | 26.79 ± 3.41 | 29.71 ± 3.22 | 2.92 | 0.0095 |
| MNS-MID | 1.33 ± 0.26 | 0.14 ± 0.22 | −1.19 | 0.0074 |
| INS-MID | 0.88 ± 0.34 | 0.03 ± 0.18 | −0.85 | 0.0262 |
| X-MNS | 23.81 ± 0.91 | 25.17 ± 0.83 | 1.36 | 0.0464 |
| MNS-ANS | 23.91 ± 0.32 | 25.19 ± 0.24 | 1.28 | 0.0398 |
| CVM+ r-l- axis | 2.43 ± 0.20 | 1.16 ± 0.20 | −1.07 | 0.0413 |
| Measurements | TO (n = 25) Mean (SD) | T1 (n = 25) Mean (SD) | Δ T1-T0 | Significance |
|---|---|---|---|---|
| Mx r-l | 58.53 ± 2.92 | 61.47 ± 2.07 | 2.94 | 0.0092 |
| Cvm+ r-l | 56.31 ± 0.68 | 61.98 ± 0.78 | 5.67 | 0.0036 |
| NL r-l | 27.74 ± 2.91 | 31.03 ± 2.88 | 3.29 | 0.0071 |
| MNS-MID | 1.01 ± 0.2 | 0.15 ± 0.1 | −0.86 | 0.0264 |
| INS-MID | 1.01 ± 0.13 | 0.07 ± 0.09 | −0.94 | 0.0359 |
| X-MNS | 23.91 ± 1.14 | 24.97 ± 0.93 | 1.16 | 0.0178 |
| MNS-ANS | 23.93 ± 0.51 | 24.98 ± 0.67 | 1.05 | 0.0472 |
| CVM+ r-l- axis | 2.47 ± 0.17 | 1.21 ± 0.18 | −1.26 | 0.0403 |
| Measurements | JIA Δ T1-T0 (n = 25) Mean (SD) | Control Δ T1-T0 (n = 25) Mean (SD) | Δ JIA-Control | Effect Size (Cohen’s d) | Significance |
|---|---|---|---|---|---|
| Mx r-l | 3.07 ± 2.19 | 2.94 ± 1.84 | 0.13 | 0.092 | 0.835 |
| Cvm+ r-l | 6.08 ± 3.77 | 5.67 ± 2.86 | 0.41 | 0.23 | 0.181 |
| NL r-l | 2.92 ± 2.32 | 3.29 ± 2.21 | −0.37 | −0.25 | 0.594 |
| MNS-MID | −1.19 ± 0.11 | −0.86 ± 0.17 | −0.33 | −0.88 | 0.121 |
| INS-MID | −0.85 ± 0.12 | −0.94 ± 0.08 | 0.09 | 0.28 | 0.753 |
| X-MNS | 1.36 ± 0.87 | 1.16 ± 0.79 | 0.21 | 0.22 | 0.237 |
| MNS-ANS | 1.28 ± 0.71 | 1.05 ± 0.56 | 0.23 | 0.29 | 0.296 |
| CVM+ r-l- axis | −1.07 ± 0.21 | −1.26 ± 0.15 | 0.19 | 0.45 | 0.465 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abate, A.; Cavagnetto, D.; Rusconi, F.M.E.; Cressoni, P.; Esposito, L. Safety and Effects of the Rapid Maxillary Expander on Temporomandibular Joint in Subjects Affected by Juvenile Idiopathic Arthritis: A Retrospective Study. Children 2021, 8, 33. https://0-doi-org.brum.beds.ac.uk/10.3390/children8010033
Abate A, Cavagnetto D, Rusconi FME, Cressoni P, Esposito L. Safety and Effects of the Rapid Maxillary Expander on Temporomandibular Joint in Subjects Affected by Juvenile Idiopathic Arthritis: A Retrospective Study. Children. 2021; 8(1):33. https://0-doi-org.brum.beds.ac.uk/10.3390/children8010033
Chicago/Turabian StyleAbate, Andrea, Davide Cavagnetto, Francesca Maria Emilia Rusconi, Paolo Cressoni, and Luca Esposito. 2021. "Safety and Effects of the Rapid Maxillary Expander on Temporomandibular Joint in Subjects Affected by Juvenile Idiopathic Arthritis: A Retrospective Study" Children 8, no. 1: 33. https://0-doi-org.brum.beds.ac.uk/10.3390/children8010033