
A Review of Experiential School-Based Culinary Interventions for 5–12-Year-Old Children

 , and
, and
Abstract
:1. Introduction
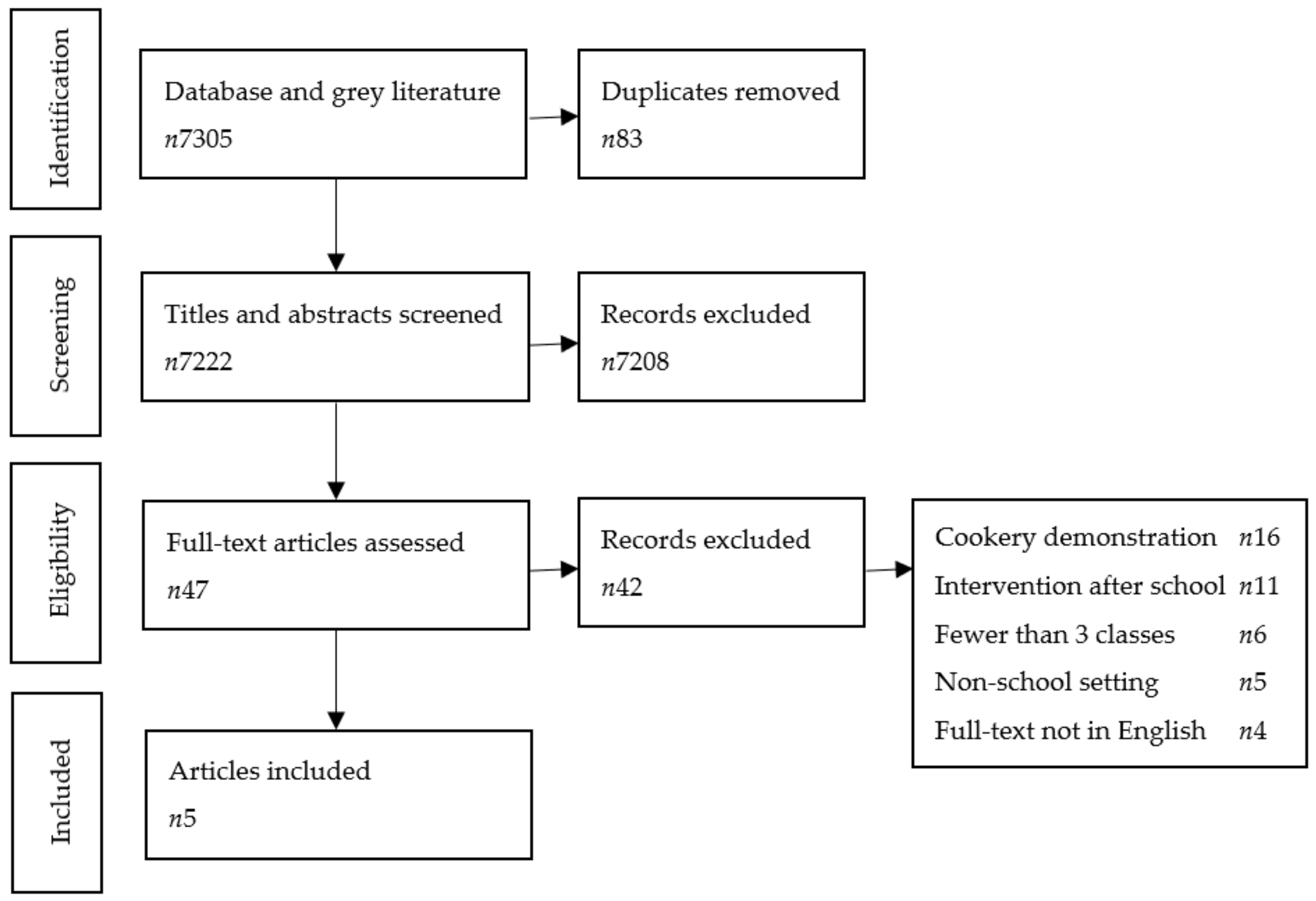
2. Materials and Methods
- ‘cooking’/exp AND (‘education’/exp OR ‘nutrition education’/exp OR ‘nutritional science’/exp OR ‘feeding behavior’/exp OR ‘nutrition’/exp)
- ((Cookery OR cooking OR cook OR food OR feeding OR eat* OR nutrition) NEAR/3 (educat* OR instruct* OR teach* OR demo? OR demonstration* OR skill* OR technique* OR learn* OR program* OR classes)):ti,ab
- #1 OR #2
- (‘school child’/exp OR ‘school’/de OR ‘kindergarten’/exp OR ‘primary school’/exp)
- (child* OR teenager* OR adolescen* OR kid? OR pupil* OR student* OR school*):ti,ab
- #4 OR #5
- #3 AND #6
3. Results
3.1. Overview of Studies
3.2. Intervention Aims and Content
3.3. Approach to Intervention Delivery
3.4. Evaluation and Outcomes
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Manzano-Carrasco, S.; Felipe, J.L.; Sanchez-Sanchez, J.; Hernandez-Martin, A.; Gallardo, L.; Garcia-Unanue, J. Weight Status, Adherence to the Mediterranean Diet, and Physical Fitness in Spanish Children and Adolescents: The Active Health Study. Nutrients 2020, 12, 1680. [Google Scholar] [CrossRef]
- O’Neil, A.; Quirk, S.E.; Housden, S.; Brennan, S.L.; Williams, L.J.; Pasco, J.A.; Berk, M.; Jacka, F.N. Relationship Between Diet and Mental Health in Children and Adolescents: A Systematic Review. Am. J. Public Health 2014, 104, e31–e42. [Google Scholar] [CrossRef] [PubMed]
- Pont, S.J.; Puhl, R.; Cook, S.R.; Slusser, W. Stigma Experienced by Children and Adolescents With Obesity. Pediatrics 2017, 140, e20173034. [Google Scholar] [CrossRef] [Green Version]
- Irish Universities Nutrition Alliance (IUNA). National Children’s Food Survey II; Irish Universities Nutrition Alliance (IUNA): Cork, Ireland, 2019; p. 37. [Google Scholar]
- Dunford, E.K.; Popkin, B.M.; Ng, S.W. Recent Trends in Junk Food Intake in U.S. Children and Adolescents, 2003–2016. Am. J. Prev. Med. 2020, 59, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Steele, E.M.; Popkin, B.M.; Swinburn, B.; Monteiro, C.A. The share of ultra-processed foods and the overall nutritional quality of diets in the US: Evidence from a nationally representative cross-sectional study. Popul. Health Metr. 2017, 15, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Vandevijvere, S.; De Ridder, K.; Fiolet, T.; Bel, S.; Tafforeau, J. Consumption of ultra-processed food products and diet quality among children, adolescents and adults in Belgium. Eur. J. Nutr. 2018, 58, 3267–3278. [Google Scholar] [CrossRef] [PubMed]
- Machado, P.P.; Steele, E.M.; Levy, R.B.; Sui, Z.; Rangan, A.; Woods, J.; Gill, T.; Scrinis, G.; Monteiro, C. Ultra-processed foods and recommended intake levels of nutrients linked to non-communicable diseases in Australia: Evidence from a nationally representative cross-sectional study. BMJ Open 2019, 9, e029544. [Google Scholar] [CrossRef] [Green Version]
- Department of Health. A Healthy Weight for Ireland: Obesity Policy and Action Plan; Government Publications; Department of Health: Dublin, Ireland, 2016; pp. 35–55. [Google Scholar]
- Lee, E.Y.; Yoon, K.-H. Epidemic obesity in children and adolescents: Risk factors and prevention. Front. Med. 2018, 12, 658–666. [Google Scholar] [CrossRef] [PubMed]
- Chung, S.T.; Onuzuruike, A.U.; Magge, S.N. Cardiometabolic risk in obese children. Ann. N.Y. Acad. Sci. 2018, 1411, 166–183. [Google Scholar] [CrossRef]
- Lavelle, F.; Spence, M.; Hollywood, L.; McGowan, L.; Surgenor, D.; McCloat, A.; Mooney, E.; Caraher, M.; Raats, M.; Dean, M. Learning cooking skills at different ages: A cross-sectional study. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Lavelle, F.; Bucher, T.; Dean, M.; Brown, H.M.; Rollo, M.E.; Collins, C.E. Diet quality is more strongly related to food skills rather than cooking skills confidence: Results from a national cross-sectional survey. Nutr. Diet. 2019, 77, 112–120. [Google Scholar] [CrossRef] [PubMed]
- Muzaffar, H.; Metcalfe, J.J.; Fiese, B. Narrative Review of Culinary Interventions with Children in Schools to Promote Healthy Eating: Directions for Future Research and Practice. Curr. Dev. Nutr. 2018, 2, nzy016. [Google Scholar] [CrossRef] [PubMed]
- Pearson, M.; Chilton, R.; Woods, H.B.; Wyatt, K.; Ford, T.; Abraham, C.; Anderson, R. Implementing health promotion in schools: Protocol for a realist systematic review of research and expe-rience in the United Kingdom (UK). Syst. Rev. 2012, 1, 48. [Google Scholar] [CrossRef] [Green Version]
- Lazarowicz, A.; O’Hara, R.L.; Broder, J.C.; Grunberg, D.M.S.; Gasevic, D. Gender differences in barriers to participation in after-school physical activities and related factors in Australian schoolchildren: A cross-sectional study. Health Promot. J. Aust. 2020, 32, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Pelcher, A.; Rajan, S. After-School Program Implementation in Urban Environments: Increasing Engagement Among Adolescent Youth. J. Sch. Health 2016, 86, 585–594. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, J.P. Significance of After-School Programming for Immigrant Children during Middle Childhood: Opportunities for School Social Work. Soc. Work 2014, 59, 243–251. [Google Scholar] [CrossRef] [PubMed]
- Bennett, A.E.; Cunningham, C.; Molloy, C.J. An evaluation of factors which can affect the implementation of a health promotion programme under the Schools for Health in Europe framework. Eval. Program Plan. 2016, 57, 50–54. [Google Scholar] [CrossRef] [Green Version]
- Day, R.E.; Sahota, P.; Christian, M.S. Effective implementation of primary school-based healthy lifestyle programmes: A qualitative study of views of school staff. BMC Public Health 2019, 19, 1–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ingemarson, M.; Rubenson, B.; Bodin, M.; Guldbrandsson, K. Implementation of a school-wide prevention programme-teachers’ and headmasters’ perceptions of organizational capacity. Eval. Program Plan. 2014, 43, 48–54. [Google Scholar] [CrossRef]
- Sutton, A.; Clowes, M.; Preston, L.; Booth, A. Meeting the review family: Exploring review types and associated information retrieval requirements. Health Inf. Libr. J. 2019, 36, 202–222. [Google Scholar] [CrossRef]
- Bai, Y.; Kim, Y.-H.; Han, Y.-H.; Hyun, T. Impact of a school-based culinary nutrition education program on vegetable consumption behavior, intention, and personal factors among Korean second-graders. Nutr. Res. Pract. 2018, 12, 527–534. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.N.; Pérez, A.; Asigbee, F.M.; Landry, M.J.; Vandyousefi, S.; Ghaddar, R.; Hoover, A.; Jeans, M.; Nikah, K.; Fischer, B.; et al. School-based gardening, cooking and nutrition intervention increased vegetable intake but did not reduce BMI: Texas sprouts - a cluster randomized controlled trial. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 1–14. [Google Scholar] [CrossRef]
- Cunningham-Sabo, L.; Lohse, B. Cooking with KidsPositively Affects Fourth Graders’ Vegetable Preferences and Attitudes and Self-Efficacy for Food and Cooking. Child. Obes. 2013, 9, 549–556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liquori, T.; Koch, P.D.; Contento, I.R.; Castle, J. The Cookshop Program: Outcome evaluation of a nutrition education program linking lunchroom food ex-periences with classroom cooking experiences. J. Nutr. Educ. 1998, 30, 302–313. [Google Scholar] [CrossRef]
- Ensaff, H.; Crawford, R.; Russell, J.; Barker, M. Preparing and sharing food: A quantitative analysis of a primary school-based food intervention. J. Public Health 2016, 39, 567–573. [Google Scholar] [CrossRef]
- Handjieva-Darlenska, T.; Blajeva, M.; Handjiev, S. Evaluation of diet and physical activity in school-age population in Bulgaria (the ephe project). Ann. Nutr. Metab. 2013, 63, 742. [Google Scholar]
- Lohse, B.; Cunningham-Sabo, L.; Walters, L.M.; Stacey, J.E. Valid and Reliable Measures of Cognitive Behaviors toward Fruits and Vegetables for Children Aged 9 to 11 Years. J. Nutr. Educ. Behav. 2011, 43, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Charlton, K.; Comerford, T.; Deavin, N.; Walton, K. Characteristics of successful primary school-based experiential nutrition programmes: A systematic literature review. Public Health Nutr. 2020, 24, 1–21. [Google Scholar] [CrossRef]
- Jung, T.; Huang, J.; Eagan, L.; Oldenburg, D. Influence of school-based nutrition education program on healthy eating literacy and healthy food choice among primary school children. Int. J. Health Promot. Educ. 2019, 57, 67–81. [Google Scholar] [CrossRef]
- Evans, A.; Ranjit, N.; Rutledge, R.; Medina, J.; Jennings, R.; Smiley, A.; Stigler, M.; Hoelscher, D. Exposure to Multiple Components of a Garden-Based Intervention for Middle School Students Increases Fruit and Vegetable Consumption. Health Promot. Pract. 2012, 13, 608–616. [Google Scholar] [CrossRef]
- Prelip, M.; Kinsler, J.; Thai, C.L.; Erausquin, J.T.; Slusser, W. Evaluation of a school-based multicomponent nutrition education program to improve young children’s fruit and vegetable consumption. J. Nutr. Educ. Behav. 2012, 44, 310–318. [Google Scholar] [CrossRef] [PubMed]
- Ensaff, H.; Canavon, C.; Crawford, R.; Barker, M. A qualitative study of a food intervention in a primary school: Pupils as agents of change. Appetite 2015, 95, 455–465. [Google Scholar] [CrossRef]
- Kien, C.; Grillich, L.; Nussbaumer-Streit, B.; Schoberberger, R. Pathways leading to success and non-success: A process evaluation of a cluster randomized physical activity health promotion program applying fuzzy-set qualitative comparative analysis. BMC Public Health 2018, 18, 1386. [Google Scholar] [CrossRef] [PubMed]
- Nixon, C.A.; Moore, H.J.; Douthwaite, W.; Gibson, E.L.; Vogele, C.; Kreichauf, S.; Wildgruber, A.; Manios, Y.; Summerbell, C.D. ToyBox-study group Identifying effective behavioural models and behaviour change strategies underpinning preschool- and school-based obesity prevention interventions aimed at 4-6-year-olds: A systematic review. Obes. Rev. 2012, 13, 106–117. [Google Scholar] [CrossRef] [PubMed]
- Hingle, M.D.; O’Connor, T.M.; Dave, J.M.; Baranowski, T. Parental involvement in interventions to improve child dietary intake: A systematic review. Prev. Med. 2010, 51, 103–111. [Google Scholar] [CrossRef] [Green Version]
- Larson, N.I.; Perry, C.L.; Story, M.; Neumark-Sztainer, D. Food Preparation by Young Adults Is Associated with Better Diet Quality. J. Am. Diet. Assoc. 2006, 106, 2001–2007. [Google Scholar] [CrossRef]
- Laska, M.N.; Larson, N.; Neumark-Sztainer, D.; Story, M. Does involvement in food preparation track from adolescence to young adulthood and is it associated with better dietary quality? Findings from a 10-year longitudinal study. Public Health Nutr. 2011, 15, 1150–1158. [Google Scholar] [CrossRef] [Green Version]
- Storfer-Isser, A.; Musher-Eizenman, D. Measuring Parent Time Scarcity and Fatigue as Barriers to Meal Planning and Preparation: Quantitative Scale Development. J. Nutr. Educ. Behav. 2013, 45, 176–182. [Google Scholar] [CrossRef]
- Lavelle, F.; McGowan, L.; Hollywood, L.; Surgenor, D.; McCloat, A.; Mooney, E.; Caraher, M.; Raats, M.; Dean, M. The development and validation of measures to assess cooking skills and food skills. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 118. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| First Author | Bai et al. [23] | Cunningham-Sabo et al. [25] | Davis et al. [24] | Ensaff et al. [27] | Liquori et al. [26] |
|---|---|---|---|---|---|
| Program name | Veggiecation | Cooking with Kids | Texas Sprouts | Jamie Oliver’s Kitchen Garden Project | Cookshop Program |
| Year | 2018 | 2013 | 2021 | 2016 | 1998 |
| Country | South Korea | U.S.A. | U.S.A. | U.K. | U.S.A. |
| Age range (years) | 7–8 | 9–10 | 8–11 | 7–9 | 5–12 |
| Total n | 71 | 257 | 3135 | 338 | 590 |
| Intervention n | 35 | 137 | 1412 | 164 | 4 class groups |
| Total no. sessions | 4 | 6 | 18 | NS † | 20 |
| No. cookery sessions | 4 | 3 | 11 | NS † | 9 |
| Length of sessions | 40 min | 120 min | 60 min | 90 min | 90–120 min |
| Interval | Weekly | 1–2 weeks | Approx. fortnightly | Fortnightly | Weekly |
| Duration | One month | One semester | One academic year | One academic year | One academic year |
| Study design | Quasi-experimental | RCT | Cluster RCT | Longitudinal comparative | Quasi-experimental |
| Theory | NS | NS | Social ecological-transactional | Social cognitive | Social cognitive |
| Content | 10 min theory lessons 30 min cookery lessons | 3 cookery sessions 3 tasting sessions | 11 cookery sessions 7 tasting sessions | Cookery sessions † | 9 cookery sessions 17 garden trips 10 classroom lessons |
| Facilitators | Nutrition teacher Teaching assistants | Food educator Classroom teacher Nutrition graduate | Nutrition educator Garden educator | Classroom teachers | Classroom teachers Parents University students |
| Included parents * | No | No | Yes | No | Yes |
| Evaluation method | Pre-post survey | 35-item pre-post survey | Pre-post data included Demographic survey SPAN dietary screener Weight Waist circumference Body composition Blood pressure % attendance | Pre-post survey | Visual estimate of plate waste (pre-post) K–3rd grade 38-item survey (post) 4th–6th grade 67-item survey (post) |
| Bai et al. [23] | Compared to the control group, the Veggiecation intervention led to the following: + Higher (p < 0.001) self-reported scores for behavior and intention in relation to vegetables. + Higher (p < 0.001) self-reported scores for attitude about, and preference for, vegetables. + Higher (p < 0.01) self-efficacy scores in relation to vegetables. + A total of 43.3% of parents reported trying the recipes at home. |
| Cunningham-Sabo et al. [25] | Compared to the control group, the Cooking with Kids intervention led to the following: + Higher (p = 0.007) vegetable preference scores. + More positive (p = 0.029) attitude toward food and cooking. + Positive (p < 0.001) change in food and cooking self-efficacy. - Higher (but not statistically significant, p ≤ 0.087) fruit preference scores. |
| Davis et al. [24] | Compared to the control group, the Texas Sprouts intervention led to: + Higher (p = 0.02, CCA) frequency of vegetable intake. - No significant change to frequency of fruit (p = 0.77) and SSB (p = 0.15) intake. - No significant change in CCA for BMI (p = 0.84), BMI z-score (p = 0.36), or BMI percentile (p = 0.39). - No significant change in CCA for waist circumference (p = 0.31) or percentage body fat (p = 0.47). - No significant change in CCA for systolic (p = 0.81) and diastolic (p = 0.28) blood pressure. |
| Ensaff et al. [27] | Compared to the control group, Jamie Oliver’s Kitchen Garden Project led to the following: + Higher scores (p = 0.004) for liking cooking. + Increased likelihood (p = 0.034) of helping with cooking at home. + Higher (p = 0.004) taste description score. + Higher (p = 0.02) scores from parents for children liking cooking. - No significant change (p = 0.493) in the food neophobia and fussiness score. |
| Liquori et al. [26] | Compared to the control group, the Cookshop Program led to the following: + Higher (p ≤ 0.001) mean preference scores for plant foods. + Positive (p ≤ 0.001) impact on knowledge. + Positive (p ≤ 0.05) impact on self-efficacy in cooking. + Positive (p ≤ 0.10) effects found for plate waste, i.e., increased consumption of targeted foods. + Higher (but not statistically significant) scores for intentions to eat plant foods. - No statistically significant change in attitudes to health, cooking, and cooperation. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bennett, A.E.; Mockler, D.; Cunningham, C.; Glennon-Slattery, C.; Johnston Molloy, C. A Review of Experiential School-Based Culinary Interventions for 5–12-Year-Old Children. Children 2021, 8, 1080. https://0-doi-org.brum.beds.ac.uk/10.3390/children8121080
Bennett AE, Mockler D, Cunningham C, Glennon-Slattery C, Johnston Molloy C. A Review of Experiential School-Based Culinary Interventions for 5–12-Year-Old Children. Children. 2021; 8(12):1080. https://0-doi-org.brum.beds.ac.uk/10.3390/children8121080
Chicago/Turabian StyleBennett, Annemarie E., David Mockler, Cara Cunningham, Corina Glennon-Slattery, and Charlotte Johnston Molloy. 2021. "A Review of Experiential School-Based Culinary Interventions for 5–12-Year-Old Children" Children 8, no. 12: 1080. https://0-doi-org.brum.beds.ac.uk/10.3390/children8121080