
Association of Infant Feeding Practices with Iron Status and Hematologic Parameters in 6-Month-Old Infants

 , and
, and
Abstract
:1. Background
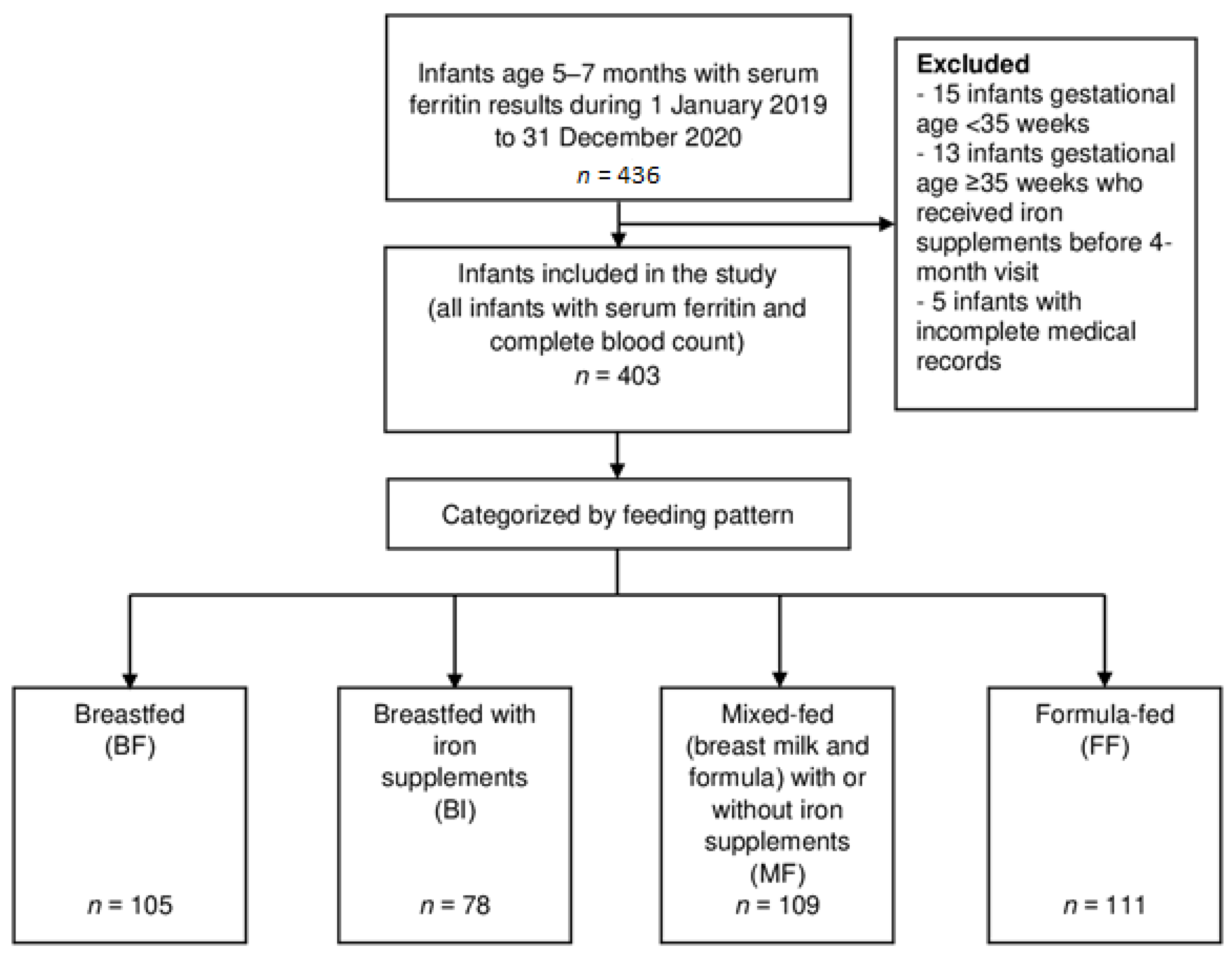
2. Methods
2.1. Biochemical Analyses
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| Hb | hemoglobin |
| HCT | hematocrit |
| ID | iron deficiency |
| IDA | iron deficiency anemia |
| MCH | mean corpuscular hemoglobin |
| MCHC | mean corpuscular hemoglobin concentration |
| MCV | mean corpuscular volume |
| RDW | red blood cell distribution width |
References
- Pasricha, S.R.; Tye-Din, J.; Muckenthaler, M.U.; Swinkels, D.W. Iron deficiency. Lancet 2021, 397, 233–248. [Google Scholar] [CrossRef]
- Kassebaum, N.J.; Jasrasaria, R.; Naghavi, M.; Wulf, S.K.; Johns, N.; Lozano, R.; Regan, M.; Weatherall, D.; Chou, D.P.; Eisele, T.P.; et al. A systematic analysis of global anemia burden from 1990 to 2010. Blood 2014, 123, 615–624. [Google Scholar] [CrossRef]
- Petry, N.; Olofin, I.; Hurrell, R.F.; Boy, E.; Wirth, J.P.; Moursi, M.; Donahue Angel, M.; Rohner, F. The proportion of anemia associated with iron deficiency in low, medium, and high Human Development Index countries: A systematic analysis of national surveys. Nutrients 2016, 8, 693. [Google Scholar] [CrossRef] [PubMed]
- Özdemir, N. Iron deficiency anemia from diagnosis to treatment in children. Türk Pediatri Arşivi 2015, 50, 11–19. [Google Scholar] [CrossRef]
- Lozoff, B.; Brittenham, G.M.; Wolf, A.W.; McClish, D.K.; Kuhnert, P.M.; Jimenez, E.; Jimenez, R.; Mora, L.A.; Gomez, I.; Krauskoph, D. Iron deficiency anemia and iron therapy effects on infant developmental test performance. Pediatrics 1987, 79, 981–995, Correction in Pediatrics 1988, 81, 683. [Google Scholar]
- Lozoff, B.; Beard, J.; Connor, J.; Barbara, F.; Georgieff, M.; Schallert, T. Long-lasting neural and behavioral effects of iron deficiency in infancy. Nutr. Rev. 2006, 64, S34–S91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO/UNICEF. Global Strategy for Infant and Young Child Feeding; World Health Organization: Geneva, Switzerland, 2003.
- Phuakpet, K. Chapter 14: Screening for anemia. In Guideline in Child Health Supervision; Noipayak, P., Piyasil, V., Ningsanon, W., Prasopsri, U., Eds.; Sappasan: Bangkok, Thailand, 2014; pp. 152–160. (In Thai) [Google Scholar]
- Bureau of Health Promotion, Department of Health, Ministry of Public Health. Mother and Child Health Handbook; Bureau of Health Promotion, Department of Health, Ministry of Public Health: Nonthaburi, Thailand, 2012; pp. 79–80.
- Pizzaro, F.; Yip, R.; Dallman, P.R.; Oliveres, M.; Hartrampf, E.; Walter, T. Iron status with different infant feeding regimens: Relevance to screening and prevention of iron deficiency. J. Pediatrics 1991, 118, 687–692. [Google Scholar] [CrossRef]
- Calvo, E.B.; Galindo, A.C.; Aspres, N.B. Iron status in exclusively breastfed infants. Pediatrics 1992, 90, 375–379. [Google Scholar]
- Krishnaswamy, S.; Bhattarai, D.; Bharti, B.; Bhatia, P.; Das, R.; Bansal, D. Iron deficiency and iron deficiency anemia in 3–5 months-old, breastfed healthy infants. Indian J. Pediatrics 2017, 84, 505–508. [Google Scholar] [CrossRef] [PubMed]
- Marques, R.F.; Taddei, J.A.; Lopez, F.A.; Braga, J.A. Breastfeeding exclusively and iron deficiency anemia during the first 6 months of age. Rev. Da Assoc. Médica Bras. 2014, 60, 18–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baker, R.D.; Greer, F.R.; Committee on Nutrition American Academy of Pediatrics. Diagnosis and prevention of iron deficiency and iron-deficiency anemia in infants and young children (0–3 years of age). Pediatrics 2010, 126, 1040–1050. [Google Scholar] [CrossRef] [Green Version]
- The Royal College of Pediatricians of Thailand & Pediatric Society of Thailand. Guidelines for Child Health Supervision from 0–18 Years Old. Updated 5 May 2020. Available online: http://www.thaipediatrics.org/Media/media-20180329072750.pdf (accessed on 10 September 2021). (In Thai).
- Chuansumrit, A.; Arnutti, P.; Apivanich, S. Iron status of one-year-old infants in a well baby clinic. J. Med. Assoc. Thail. 2002, 85 (Suppl. 4), S1081–S1088. [Google Scholar]
- Thaweekul, P.; Surapolchai, P.; Sinlapamongkolkul, P. Infant feeding practices in relation to iron status and other possible nutritional deficiencies in Pathumthani, Thailand. Asia Pac. J. Clin. Nutr. 2019, 28, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Tantracheewathorn, S.; Lohajaroensub, S. Incidence and risk factors of iron deficiency anemia in term infants. J. Med. Assoc. Thail. 2005, 88, 45–51. [Google Scholar]
- Suwannakeeree, P.; Jangmeonwai, P. The prevalence and risk factors of iron deficiency anemia in Thai infants by complete blood count at 9-month-old. J. Med. Assoc. Thail. 2020, 103, 891–896. [Google Scholar]
- World Health Organization. Iron Deficiency Anemia. Assessment, Prevention and Control. A Guide for Programme Managers; Con-tract No. WHO/NHD/01.3; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Rojroongwasinkul, N.; Kijboonchoo, K.; Wimonpeerapattana, W.; Purttiponthanee, S.; Yamborisut, U.; Boonpraderm, A.; Kunapan, P.; Thasanasuwan, W.; Khouw, I. SEANUTS: The nutritional status and dietary intakes of 0.5–12-year-old Thai children. Br. J. Nutr. 2013, 110 (Suppl. 3), S36–S44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, C.M.; Mu, S.C.; Shih, C.K.; Chen, Y.L.; Tsai, L.Y.; Kuo, Y.T.; Cheong, I.M.; Chang, M.L.; Chen, Y.C.; Li, S.C. Iron status of infants in the first year of life in northern Taiwan. Nutrients 2020, 12, 139. [Google Scholar] [CrossRef] [Green Version]
- Soh, P.; Ferguson, E.L.; McKenzie, J.E.; Homs, M.Y.; Gibson, R.S. Iron deficiency and risk factors for lower iron stores in 6-24-month-old New Zealanders. Eur. J. Clin. Nutr. 2004, 58, 71–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nanta, N.; Natesirinilkul, R.; Kittisakmontri, K.; Chimnuan, K.; Manowong, S.; Suanta, S.; Charoenkwan, P. Screening for iron deficiency anemia in infants in a thalassemia-endemic region. J. Pediatric Hematol. Oncol. 2021, 43, e11–e14. [Google Scholar] [CrossRef]
- Chaparro, C.M.; Suchdev, P.S. Anemia epidemiology, pathophysiology, and etiology in low- and middle-income countries. Ann. N. Y. Acad. Sci. 2019, 1450, 15–31. [Google Scholar] [CrossRef]
- Department of Health, Ministry of Public Health Thailand. Guidelines for the Control and Prevention of Iron Deficiency Anemia. Available online: https://www.nutrition.anamai.moph.go.th/images/file/filet001.pdf (accessed on 10 September 2021). (In Thai)
- Cai, C.; Granger, M.; Eck, P.; Friel, J. Effect of daily iron supplementation in healthy exclusively breastfed infants: A systematic review with meta-analysis. Breastfeed. Med. 2017, 12, 597–603. [Google Scholar] [CrossRef]
- Domellöf, M.; Cohen, R.J.; Dewey, K.G.; Hernell, O.; Rivera, L.L.; Lönnerdal, B. Iron supplementation of breast-fed Honduran and Swedish infants from 4 to 9 months of age. J. Pediatrics 2001, 138, 679–687. [Google Scholar] [CrossRef] [PubMed]
- Dumrongwongsiri, O.; Winichagoon, P.; Chongviriyaphan, N.; Suthutvoravut, U.; Grote, V.; Koletzko, B. Zinc and iron ade-quacy and relative importance of zinc/iron storage and intakes among breastfed infants. Matern. Child Nutr. 2021, e13268. [Google Scholar] [CrossRef] [PubMed]
- Qasem, W.; Fenton, T.; Friel, J. Age of introduction of first complementary feeding for infants: A systematic review. BMC Pediatrics 2015, 15, 107. [Google Scholar] [CrossRef] [Green Version]
- Kittisakmontri, K.; Fewtrell, M.; Roekworachai, K.; Phanpong, C.; Lanigan, J. Complementary feeding: Attitudes, knowledge and practices of urban families in northern Thailand. Nutr. Diet. 2019, 76, 57–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lönnerdal, B. Development of iron homeostasis in infants and young children. Am. J. Clin. Nutr. 2017, 106 (Suppl. 6), 1575S–1580S. [Google Scholar] [CrossRef] [Green Version]
- Pasricha, S.R.; Hayes, E.; Kalumba, K.; Biggs, B.A. Effect of daily iron supplementation on health in children aged 4–23 months: A systematic review and meta-analysis of randomised controlled trials. Lancet Glob. Health 2013, 1, e77–e86, Correction in Lancet Glob. Health 2014, 2, e144. [Google Scholar] [CrossRef] [Green Version]
- Kc, A.; Rana, N.; Målqvist, M.; Ranneberg, L.J.; Subedi, K.; Andersson, O. Effects of delayed umbilical cord clamping vs early clamping on anemia in infants at 8 and 12 months: A randomized clinical trial. JAMA Pediatrics 2017, 171, 264–270. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Breastfed (BF) (n = 105) | Breastfed with Iron Supplements (BI) (n = 78) | Mixed-Fed with or without Iron Supplements (MF) (n = 109) | Formula-Fed (FF) (n = 111) | p-Value |
|---|---|---|---|---|---|
| Male sex | 57 (54.3) | 37 (47.4) | 59 (54.1) | 52 (46.9) | 0.564 |
| Inborn | 43 (41.0) | 33 (42.3) | 49 (45.0) | 42 (37.8) | 0.757 |
| Gestational age (weeks) | 38 ± 1 | 38 ± 1 | 38 ± 1 | 38 ± 1 | 0.521 |
| Small for gestational age | 13 (12.4) | 18 (23.1) | 12 (11.0) | 15 (13.5) | 0.127 |
| Large for gestational age | 0 (0) | 3 (3.9) | 0 (0) | 5 (4.5) | 0.008 |
| At birth | |||||
| Weight (g) | 3103 ± 391 | 3105 ± 461 | 3120 ± 397 | 3195 ± 449 | 0.251 |
| Length (cm) | 49.5 ± 2.2 | 49.2 ± 2.1 | 49.6 ± 2.2 | 50.1 ± 2.2 | 0.971 |
| Head circumference (cm) | 33.6 ± 1.4 | 33.7 ± 1.4 | 33.7 ± 1.2 | 34.0 ± 1.4 | 0.411 |
| At 4-month visit | |||||
| Weight (g) | 6606 ± 813 | 6569 ± 905 | 6598 ± 895 | 6727 ± 842 | 0.699 |
| Length (cm) | 62.8 ± 2.2 | 62.7 ± 2.5 | 63.0 ± 2.3 | 63.4 ± 2.2 | 0.681 |
| Head circumference (cm) | 41.0 ± 1.2 | 40.8 ± 1.4 | 41.0 ± 1.4 | 40.9 ± 1.3 | 0.675 |
| At 6-month visit | |||||
| Weight (g) | 7468 ± 853 | 7475 ± 1065 | 7603 ± 1007 | 7730 ± 924 | 0.158 |
| Length (cm) | 66.1 ± 2.3 | 66.2 ± 2.6 | 66.8 ± 2.3 | 67.3 ± 2.4 | 0.523 |
| Head circumference (cm) | 42.7 ± 1.3 | 42.5 ± 1.4 | 42.7 ± 1.5 | 42.6 ± 1.2 | 0.327 |
| Complementary feeding before 6 months | 36 (34.3) | 41 (52.6) | 87 (79.8) | 95 (85.6) | <0.001 |
| Iron supplementation | 0 (0) | 78 (100.0) | 40 (36.7) | 0 (0) | <0.001 |
| Characteristics | Breastfed (BF) (n = 105) | Breastfed with Iron Supplements (BI) (n = 78) | Mixed-Fed with or without Iron Supplements (MF) (n = 109) | Formula-Fed (FF) (n = 111) | p-Value |
|---|---|---|---|---|---|
| Hb (g/dL) | 11.1 ± 1.0 a | 11.7 ± 1.0 | 11.8 ± 0.9 | 11.8 ± 0.9 | <0.001 |
| HCT (%) | 34.4 ± 2.9 b | 36.2 ± 3.0 | 36.2 ± 2.6 | 35.3 ± 2.6 | <0.001 |
| MCV (fL) | 69.8 ± 6.9 c | 71.8 ± 7.1 | 73.7 ± 6.5 | 74.3 ± 6.0 | <0.001 |
| MCH (pg) | 22.6 ± 2.5 c | 23.4 ± 2.7 e | 24.1 ± 2.4 | 24.8 ± 2.2 | <0.001 |
| MCHC (g/dL) | 32.3 ± 1.1 e | 32.5 ± 1.0 e | 32.7 ± 1.1 e | 33.3 ± 1.0 | <0.001 |
| RDW (%) | 14.6 ± 2.3 e | 14.5 ± 2.2 e | 14.0 ± 2.1 | 13.4 ± 1.9 | <0.001 |
| Serum ferritin (ng/mL) | 37.5 ± 43.4 a | 88.7 ± 84.1 | 74.8 ± 53.6 | 80.2 ± 47.6 | <0.001 |
| Anemia (Hb < 11 g/dL) | 40 (38.1) c,† | 17 (21.8) | 21 (19.3) | 18 (16.2) | <0.001 |
| ID (Serum ferritin < 12 ng/mL) | 30 (28.6) a,† | 3 (3.8) | 4 (3.7) | 1 (0.9) | <0.001 |
| IDA | 18 (17.1) a,† | 2 (2.6) | 1 (0.9) | 1 (0.9) | <0.001 |
| ID without anemia | 12 (11.4) d,† | 1 (1.3) | 3 (2.8) | 0 (0) | <0.001 |
| Anemia without ID | 22 (21.0) | 15 (19.2) | 20 (18.3) | 17 (15.3) | 0.754 |
| Variables | Crude OR | 95% CI | p-Value | Adjusted OR | 95% CI | p-Value |
|---|---|---|---|---|---|---|
| Gestational age | 0.586 | 0.392–0.875 | 0.009 | 0.819 | 0.464–1.447 | 0.819 |
| Birth weight | 0.998 | 0.997–0.999 | 0.003 | 0.997 | 0.995–0.999 | 0.002 |
| Male sex | 2.709 | 1.038–7.072 | 0.042 | 2.585 | 0.818–8.168 | 0.106 |
| Weight gain 0–6 months | 1.001 | 1.000–1.001 | 0.011 | 1.001 | 1.000–1.001 | 0.010 |
| Small for gestational age | 1.346 | 0.439–4.128 | 0.604 | |||
| Complementary feeding before 6 months | 0.651 | 0.274–1.546 | 0.331 | |||
| Feeding practices | ||||||
| BF | 1 (ref) | 1 (ref) | ||||
| BI | 0.127 | 0.029–0.566 | 0.007 | 0.096 | 0.020–0.466 | 0.004 |
| MF | 0.045 | 0.006–0.342 | 0.003 | 0.025 | 0.004–0.267 | <0.001 |
| FF | 0.044 | 0.006–0.336 | 0.003 | 0.031 | 0.003–0.218 | 0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruangkit, C.; Prachakittikul, N.; Hemprachitchai, N.; Dumrongwongsiri, O.; Soonsawad, S. Association of Infant Feeding Practices with Iron Status and Hematologic Parameters in 6-Month-Old Infants. Children 2021, 8, 1159. https://0-doi-org.brum.beds.ac.uk/10.3390/children8121159
Ruangkit C, Prachakittikul N, Hemprachitchai N, Dumrongwongsiri O, Soonsawad S. Association of Infant Feeding Practices with Iron Status and Hematologic Parameters in 6-Month-Old Infants. Children. 2021; 8(12):1159. https://0-doi-org.brum.beds.ac.uk/10.3390/children8121159
Chicago/Turabian StyleRuangkit, Chayatat, Nawapat Prachakittikul, Nutthida Hemprachitchai, Oraporn Dumrongwongsiri, and Sasivimon Soonsawad. 2021. "Association of Infant Feeding Practices with Iron Status and Hematologic Parameters in 6-Month-Old Infants" Children 8, no. 12: 1159. https://0-doi-org.brum.beds.ac.uk/10.3390/children8121159