
Selective Bronchial Occlusion for Treatment of a Bronchopleural Fistula in an Extremely Preterm Infant

 , , , , ,
, , , , ,  ,
,
Abstract
:1. Introduction
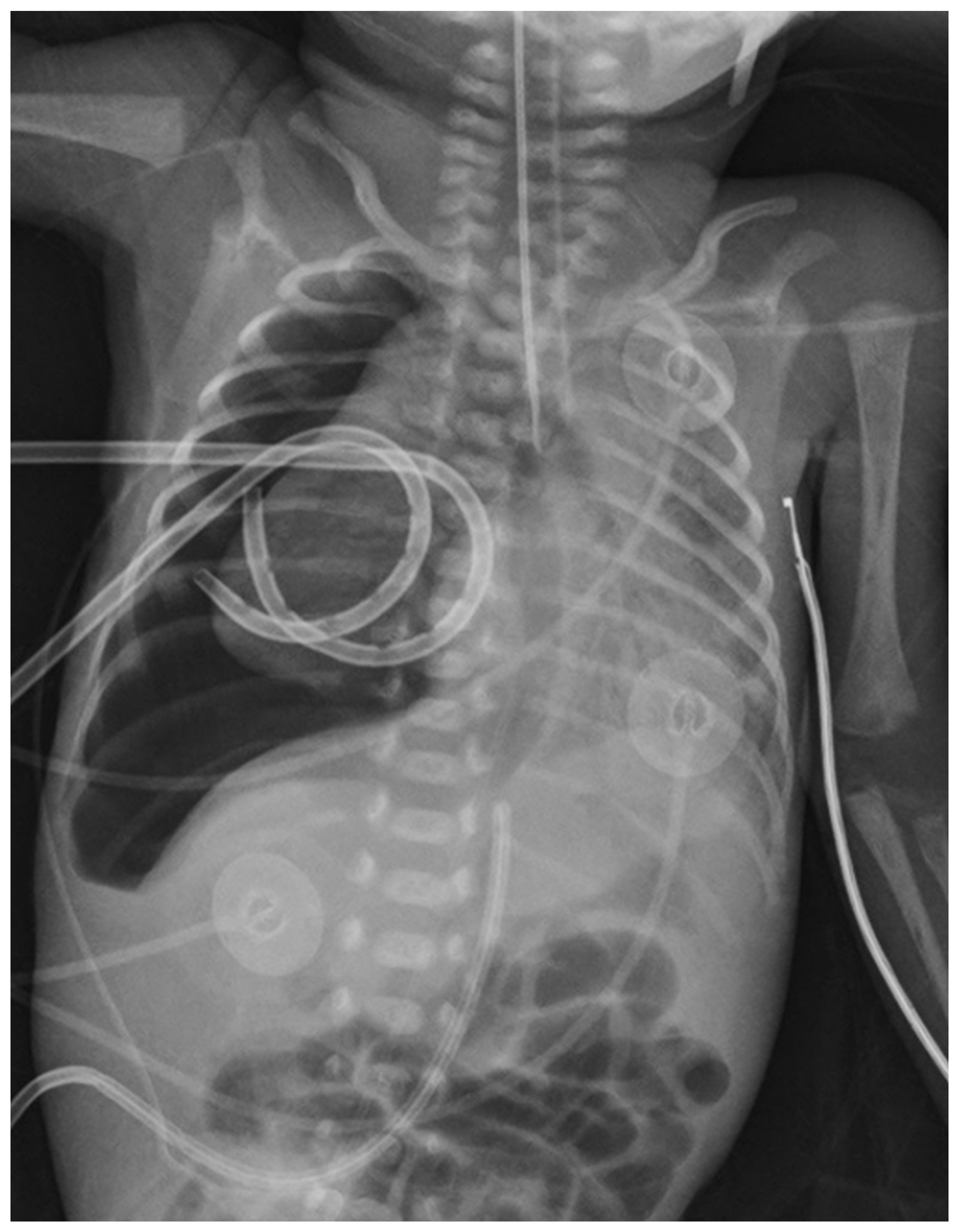
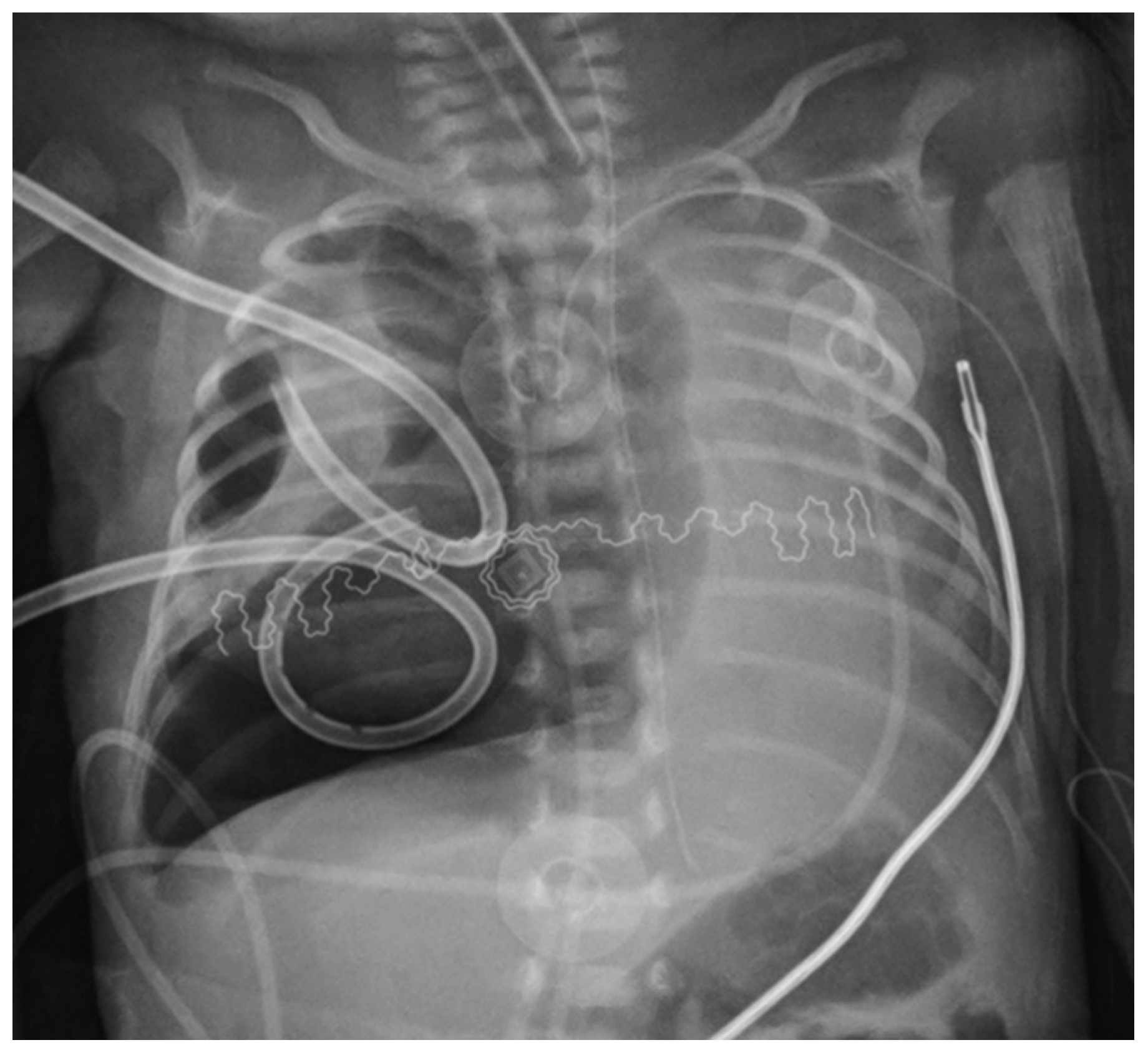
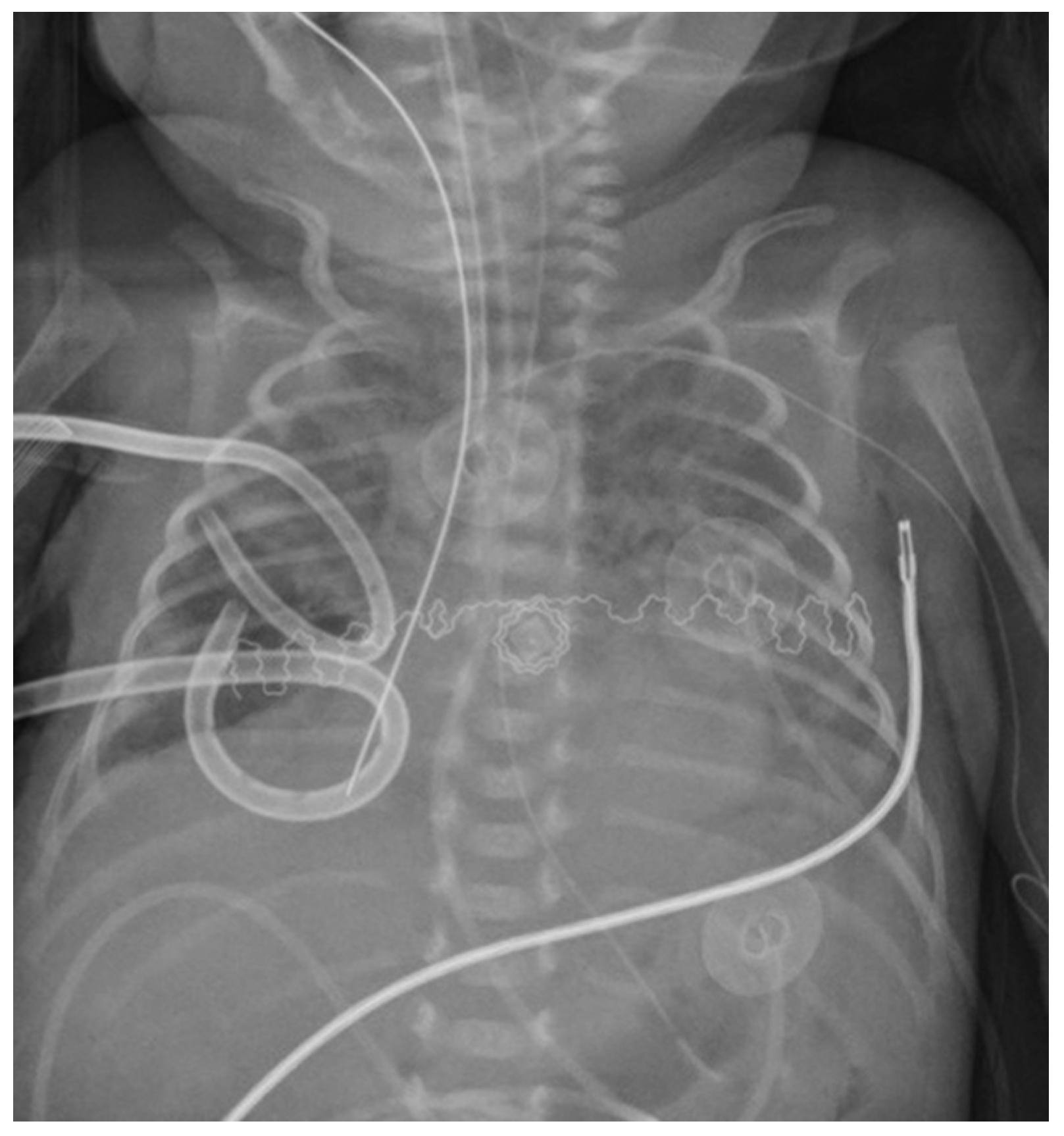
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Andreou, A.; Papouli, M.; Netskos, D.; Papadopoulou, F.; Rossiou, E. One-sided high-frequency oscillatory ventilation in the management of an acquired neonatal lobar emphysema. A case report and review. J. Perinatol. 2001, 21, 61–64. [Google Scholar] [CrossRef] [Green Version]
- Bruschettini, M.; Romantsik, O.; Zappettini, S.; O’Donnell, C.P.; Calevo, M.G. Needle aspiration versus intercostal tube drainage for pneumothorax in the newborn. Cochrane Database Syst Rev. 2019, 2, CD011724. [Google Scholar] [CrossRef] [PubMed]
- Kitsommart, R.; Martins, B.; Bottino, M.N. Expectant management of pneumothorax in preterm infants receiving assisted ventilation: Report of 4 cases and review of the literature. Respir Care 2012, 57, 789–793. [Google Scholar] [CrossRef] [PubMed]
- Mosca, F.; Lattanzio, M.; Colnaghi, M.; Pugliese, S. Bronchopleural fistula: Successful selective bronchial occlusion with a Fogarty’s catheter in a preterm infant. Acta Paediatr. 1995, 84, 1079–1082. [Google Scholar] [CrossRef] [PubMed]
- Aurilia, C.; Ricci, C.; Tana, M.; Tirone, C.; Lio, A.; Gambacorta, A.; Paladini, A.; Vento, G. Management of pneumothorax in hemodynamically stable preterm infants using high frequency oscillatory ventilation: Report of five cases. Ital. J. Pediatr. 2017, 43, 114. [Google Scholar] [CrossRef] [PubMed]
- Goussard, P.; Morrison, J.; Bekker, A.; Fourie, B. Acquired neonatal bronchial stenosis after selective intubation: Successful managed with balloon dilatation. Clin. Case Rep. 2019, 7, 917–919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glenski, J.A.; Thibeault, D.W.; Hall, F.K.; Hall, R.T.; Germann, D.R. Selective bronchial intubation in infants with lobar emphysema. Am. J. Perinatol. 1986, 3, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Hathorn, C.; Armitage, N.; Wensley, D.; Seear, M. Bronchial balloon occlusion in children with complex pulmonary air leaks. Arch. Dis. Child. 2013, 98, 136–140. [Google Scholar] [CrossRef] [PubMed]
- Rastogi, S.; Gupta, A.; Wung, J.-T.; Berdon, W.E. Treatment of giant pulmonary interstitial emphysema by ipsilateral bronchial occlusion with a swan-ganz catheter. Pediatr. Radiol. 2007, 37, 1130–1134. [Google Scholar] [CrossRef] [PubMed]
- Al-Alaiyan, S.; Katan, A. Pulmonary interstitial emphysema treated by selective bronchial obstruction and high-frequency oscillatory ventilation. Am. J. Perinatol. 1994, 11, 433–435. [Google Scholar] [CrossRef] [PubMed]
- Al Jishi, N.; Dyer, D.; Sharief, N.; Al-Alaiyan, S. Selective bronchial occlusion for treatment of bullous interstitial emphysema and bronchopleural fistula. J. Pediatr. Surg. 1994, 29, 1545–1547. [Google Scholar] [CrossRef]
- Weintraub, Z.; Oliven, A. Successful resolution of unilateral pulmonary interstitial emphysema in a premature infant by selective bronchial balloon catheterization. J. Pediatr. Surg. 1988, 23, 1005–1006. [Google Scholar] [CrossRef]
- Lewis, S.; Pelausa, E.; Ojah, C.; Paes, B. Pulmonary interstitial emphysema: Selective bronchial occlusion with a swan-ganz catheter. Arch. Dis. Child. 1988, 63, 313–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeWitte, D.B.; Batton, D.G.; Prudent, L.; Maisels, M.J. Endotracheal tube modification for therapy of right-sided pulmonary interstitial emphysema. Clin. Pediatr. 1986, 25, 626–628. [Google Scholar] [CrossRef] [PubMed]
- Auerbach, D.A.; Blackmon, L.R.; Filston, H.C.; Merten, D.F.; Kirks, D.R. Localized pulmonary interstitial emphysema: Treatment by bronchial occlusion. Am. J. Perinatol. 1983, 1, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Mathew, O.P.; Thach, B.T. Selective bronchial obstruction for treatment of bullous interstitial emphysema. J. Pediatr. 1980, 96, 475–477. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Author | GA (Weeks) | Weight (g) | Air Leak | Position | Unsuccessful Treatment | HFO | Instrumentation Used | Insertion | Occlusion Type | Length |
|---|---|---|---|---|---|---|---|---|---|---|
| Present study | 27 | 600 | PTX | Right | Chest drainage and postural therapy | Yes | Fogarty’s catheter 3 FR, inflated 0.2 mL | Direct laryngoscopy | Inflated 1 h/deflated 2 h | 72 h |
| Al alaiyan | 30 | 1500 | PIE | Right | Postural therapy and chest drainage | Yes | Balloon catheter inflated 0.3 mL | Direct laryngoscopy | Deflated for 5 min each hour | 48 h |
| Alijishi | 28 | 1240 | PIE | Right | Postural therapy, chest drainage, and selective left bronchial intubation | No | Balloon catheter inflated 0.35 mL | Direct laryngoscopy | Deflated for 5 min each hour | 60 h |
| Auerbach | 30 | 1620 | PIE | Left | Chest drainage and selective right bronchial intubation | No | Fogarty’s catheter 4 FR | Bronchoscopy | Continuous | 48 h |
| 32 | 1250 | PIE | Left | NA | No | Fogarty’s catheter 3 FR | Bronchoscopy | Inflated 4 h/deflated 4 h | 96 h | |
| Dewitte | 29 | 1340 | PIE | Right | Postural therapy | NA | ET 2.5 mm modified * | Direct laryngoscopy | Continuous | 72 h |
| 28 | 1120 | PIE | Right | Chest drainage | NA | ET 2.5 mm modified * | Direct laryngoscopy | Continuous | 48 h | |
| Hathorn | 33 | 2390 | PIE | Right | NA | NA | Balloon catheter 4 FR | Direct laryngoscopy | Continuous | 96 h |
| 27 | 1200 | PIE | Left | NA | NA | Balloon catheter 4 FR | Bronchoscopy with Fluoroscopic guidance | Continuous | 7 days | |
| Lewis | 26 | 760 | PIE | Right | Postural therapy, chest drainage, and selective left bronchial intubation | No | Swan-Ganz catheter 5 FR | Direct laryngoscopy | Deflated 5 min each hour | 72 h |
| Mathew | 29 | 950 | PIE and PTX | Right | Chest drainage and selective left bronchial intubation | No | Umbilical catheter modified °, inflated 0.7 mL | Direct laryngoscopy | Continuous | 48 + 72 h Ψ |
| Mosca | 26 | 1000 | PIE and PTX | Right | Postural therapy and chest drainage | No | Fogarty’s catheter 5 FR, inflated 0.3 mL | Direct laryngoscopy | Deflated 5 min each hour | 26 h |
| Weintraub | 28 | 1200 | PIE | Right | Postural therapy | No | Balloon catheter 4 FR, inflated 0.75 mL | Direct laryngoscopy | Continuous | NA |
| Rastoigi ⊥ | 25–32 | 600–1700 | 12 PIE/2 PTX | NA | Postural therapy | 3 yes/11 no | Swan-Ganz catheter 5 FR, inflated 0.6 mL | Direct laryngoscopy | Every hour at the hour | 24 h after the PIE resolution |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amelio, G.S.; Colnaghi, M.; Gulden, S.; Raffaeli, G.; Cortesi, V.; Amodeo, I.; Cavallaro, G.; Mosca, F.; Ghirardello, S. Selective Bronchial Occlusion for Treatment of a Bronchopleural Fistula in an Extremely Preterm Infant. Children 2021, 8, 1208. https://0-doi-org.brum.beds.ac.uk/10.3390/children8121208
Amelio GS, Colnaghi M, Gulden S, Raffaeli G, Cortesi V, Amodeo I, Cavallaro G, Mosca F, Ghirardello S. Selective Bronchial Occlusion for Treatment of a Bronchopleural Fistula in an Extremely Preterm Infant. Children. 2021; 8(12):1208. https://0-doi-org.brum.beds.ac.uk/10.3390/children8121208
Chicago/Turabian StyleAmelio, Giacomo Simeone, Mariarosa Colnaghi, Silvia Gulden, Genny Raffaeli, Valeria Cortesi, Ilaria Amodeo, Giacomo Cavallaro, Fabio Mosca, and Stefano Ghirardello. 2021. "Selective Bronchial Occlusion for Treatment of a Bronchopleural Fistula in an Extremely Preterm Infant" Children 8, no. 12: 1208. https://0-doi-org.brum.beds.ac.uk/10.3390/children8121208