
Factors to Consider to Study Preductal Oxygen Saturation Targets in Neonatal Pulmonary Hypertension

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
1.1. Rationale for Higher (95–99%) SpO2 in PH
- a.
- Acidosis: Infants with aPH often have associated respiratory and metabolic acidosis that can exacerbate hypoxic pulmonary vasoconstriction [4]. Maintaining a higher SpO2 target (95–99%) may limit hypoxic pulmonary vasoconstriction when pH is <7.2.
- b.
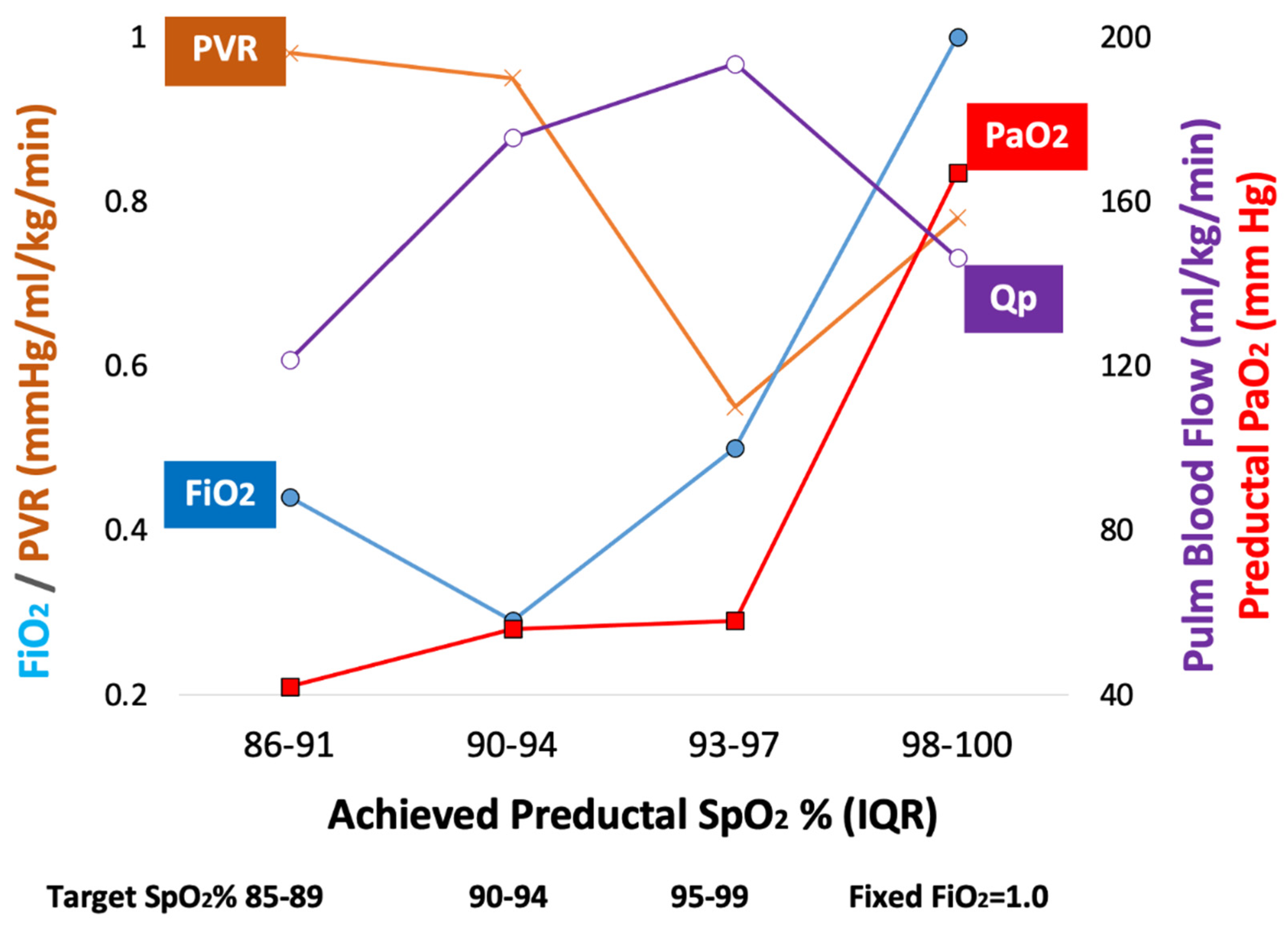
- Optimal FiO2: We have previously shown in the lamb model of asphyxia, MAS and PH, that targeting 95–99% SpO2 (achieving a median of 97%) resulted in lower PVR compared to the 90–94% target (achieving a median of 92%—Figure 1). This reduction in PVR was not associated with a statistically significant difference in preductal PaO2 (56 ± 11 mmHg with 90–94% target and 58 ± 19 mmHg with 95–99% target SpO2—Figure 1). However, the mean FiO2 to achieve 95–99% SpO2 was significantly higher than the 90–94% group (0.5 ± 0.21 vs. 0.29 ± 0.17) [10]. Given the importance of alveolar PAO2 in mitigating hypoxic pulmonary vasoconstriction [17], we speculate that FiO2 (in addition to SpO2 or PaO2) plays an important role in pulmonary vasodilation in PH.
- c.
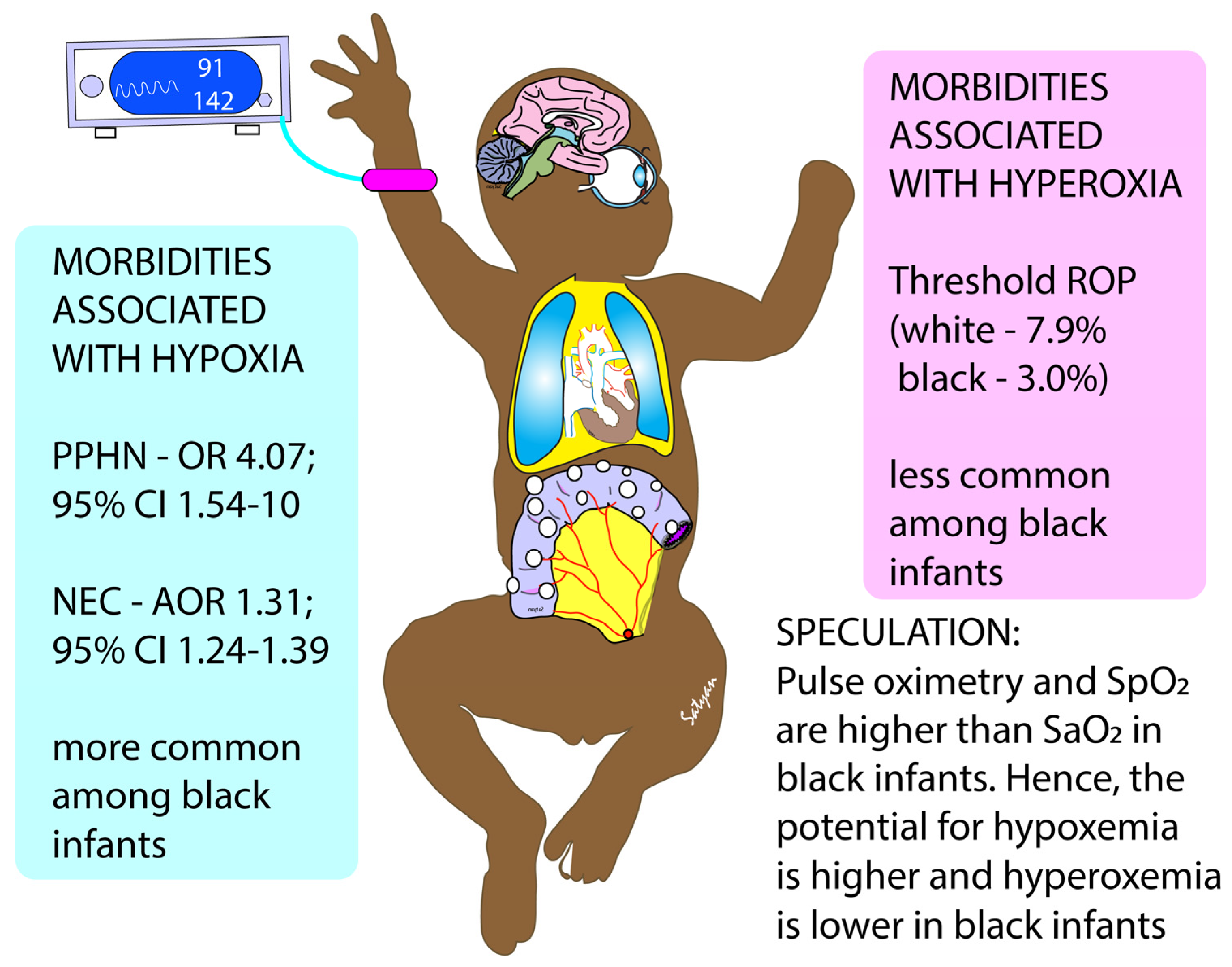
- Skin pigmentation, race and SpO2: Skin pigmentation can underestimate hypoxemia by pulse oximetry [18,19]. In neonates the discrepancy between arterial saturation (SaO2) and pulse oximetry (SpO2) is higher in Black infants compared to white infants, especially when SpO2 is below 95%. The incidence of occult hypoxemia (defined as SaO2 < 85% when SpO2 is ≥90%) is more common in Black infants (9.2% of samples) compared to white infants (7.7%) [19]. Targeting SpO2 in the low 90s might increase the risk of occult hypoxemia in infants with darker skin. Interestingly, conditions exacerbated by hypoxemia (such as necrotizing enterocolitis—NEC) and aPH are more common in Black infants, and conditions exacerbated by hyperoxia (such as ROP) are more common among white infants (Figure 2) [20,21,22,23].
- d.
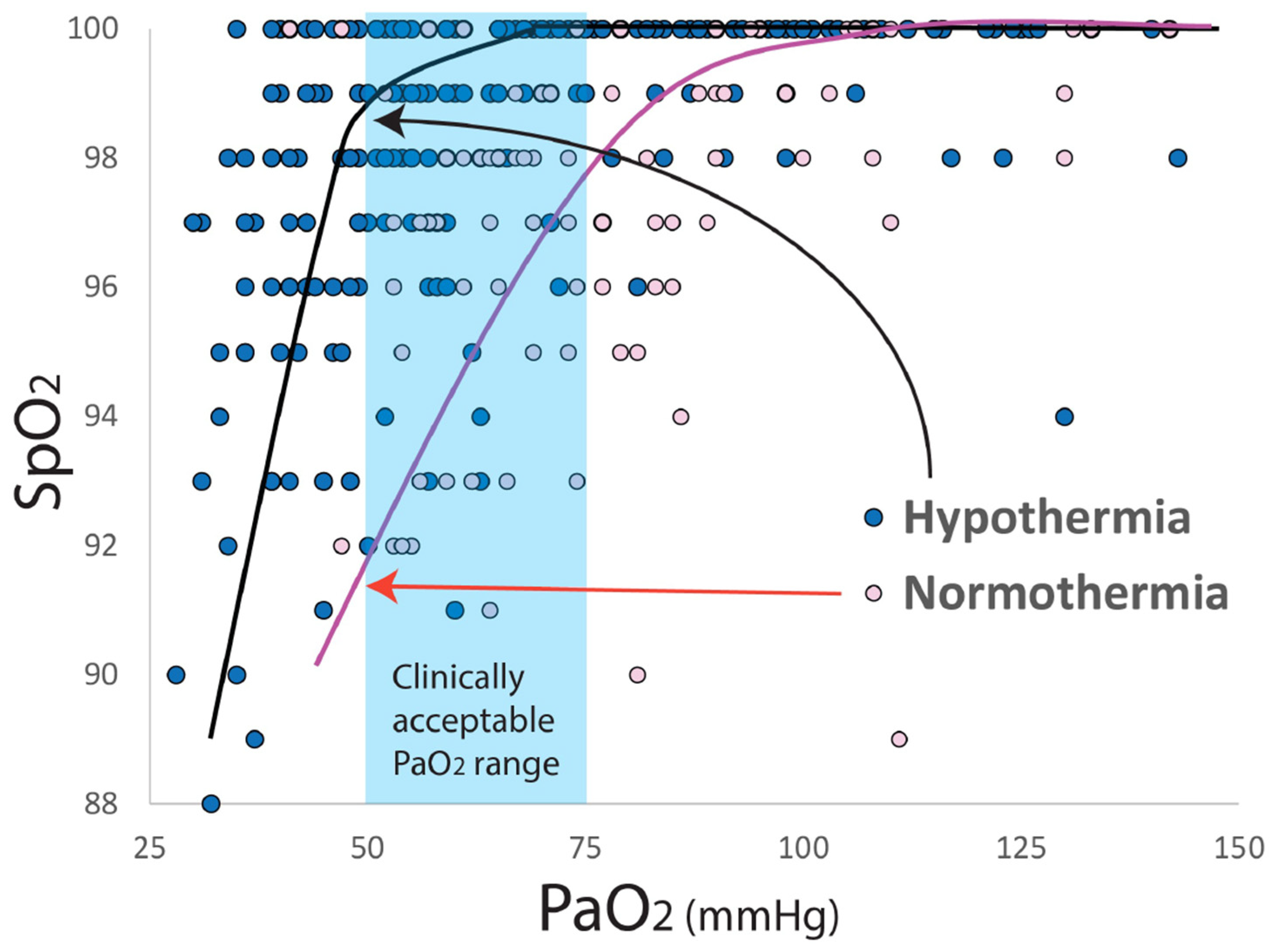
- Therapeutic hypothermia: Infants with moderate to severe hypoxic ischemic encephalopathy (HIE) undergoing therapeutic hypothermia exhibit features of aPH (~25% of neonates cooled down to a core temperature of 33.5 °C and ~34% of neonates cooled to 32 °C received iNO) [24]. Konduri et al. conducted a trial on iNO use in aPH prior to the advent of therapeutic hypothermia for HIE. Among all term neonates with aPH, 34/299 (11.4%) needed ECMO. Low Apgar scores (<3 at 1 min) were present in 26.1% of these patients with aPH, and perinatal aspiration syndrome (44%) was the leading cause of aPH [25]. In a study by Shankaran et al., 22/105 infants with HIE on iNO for aPH needed ECLS (21%), suggesting that the response to iNO might be impaired in HIE and hypothermia. HIE is often associated with left ventricular dysfunction, which can lead to pulmonary vascular congestion from increased left atrial and pulmonary venous pressure resulting in a poor response to iNO [26,27,28]. In addition, during whole body hypothermia, the hemoglobin–oxygen dissociation curve shifts to the left (Figure 3), resulting in higher SpO2 values for the same PaO2 range. Targeting 91–95% preductal SpO2 might lead to hypoxemia (lower PaO2), increased PVR and increased need for ECLS. Finally, the use of IV vasodilators such as milrinone may be associated with severe systemic hypotension during hypothermia, and may contribute to an increased need for ECLS [29]. The optimal target SpO2, physiologic basis of hemodynamic and oxygenation response to iNO, sildenafil and milrinone, during whole-body hypothermia are not known.
1.2. Rationale for Standard (91–95%) SpO2 Range in PH
- a.
- Response to pulmonary vasodilators and target SpO2: The target SpO2 that results in optimal vasodilation in response to iNO, sildenafil or milrinone is not known. Nitric oxide reacts with superoxide anions to form toxic peroxynitrite (Figure 4). The bioavailability of iNO is determined by local concentration of superoxide anions [30]. Ventilation with 100% oxygen increases superoxide anion production in pulmonary arterial smooth muscle cells and impairs response to iNO in lambs [5,31]. Gitto et al. ventilated 60 term neonates with aPH with an initial FiO2 of 0.45 or 0.8. All infants received iNO. Serum IL-6, IL-8 and TNF-α levels were measured over 72 h. Infants in the 0.45 FiO2 group showed progressive decrease in these inflammatory markers. Infants in the 0.8 FiO2 group saw an increase in serum IL-6, IL-8 and TNF-α levels [32]. The reduction in oxygenation index (mean airway pressure × FiO2 × 100 ÷ PaO2) was similar between both groups. These findings suggest a combination of high FiO2 and iNO can trigger inflammatory cytokines but does not alter improvement in oxygenation [32].
- b.
- Oxygen toxicity: Use of 100% inspired oxygen is associated with free radical formation in animal models and is associated with reduced response to pulmonary vasodilators such as iNO. The combination of iNO with high FiO2 is proinflammatory due to oxidant injury. However, iNO can exhibit anti-inflammatory and antioxidant effects when FiO2 is low. There are no studies evaluating different target SpO2 ranges with response to iNO.
2. Materials and Methods
2.1. Objectives/Specific Aims
2.2. Study Design
2.3. Screening and Eligibility
2.4. Criteria for Exit from the Trial Intervention
- Weaned to nasal cannula oxygen with FiO2 = 0.21 and flow < 2 LPM;
- Significant deterioration with OI > 35 or preparation for ECLS cannulation;
- Hospital discharge;
- Parental decision to withdraw from the study;
- Provider (attending physician) decision to withdraw from the study;
- Death.
2.5. Randomization
2.6. Intervention
2.7. Blinding
2.8. Outcomes
2.9. Sample Size
2.10. Data Monitoring Committee
2.11. Anticipated Challenges and Limitations
3. Conclusions
4. Trial Status
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Lakshminrusimha, S.; Steinhorn, R.H. Pulmonary vascular biology during neonatal transition. Clin. Perinatol. 1999, 26, 601–619. [Google Scholar] [CrossRef]
- Lakshminrusimha, S. The pulmonary circulation in neonatal respiratory failure. Clin. Perinatol. 2012, 39, 655–683. [Google Scholar] [CrossRef] [Green Version]
- Lakshminrusimha, S.; Keszler, M. Persistent pulmonary hypertension of the newborn. Neoreviews 2015, 16, e680–e694. [Google Scholar] [CrossRef] [Green Version]
- Rudolph, A.M.; Yuan, S. Response of the Pulmonary Vasculature to Hypoxia and H+ Ion Concentration Changes. J. Clin. Investig. 1966, 45, 399–411. [Google Scholar] [CrossRef]
- Lakshminrusimha, S.; Swartz, D.D.; Gugino, S.F.; Ma, C.-X.; Wynn, K.A.; Ryan, R.M.; Russell, J.A.; Steinhorn, R.H. Oxygen Concentration and Pulmonary Hemodynamics in Newborn Lambs with Pulmonary Hypertension. Pediatr. Res. 2009, 66, 539–544. [Google Scholar] [CrossRef] [Green Version]
- Lakshminrusimha, S.; Russell, J.A.; Wedgwood, S.; Gugino, S.F.; Kazzaz, J.A.; Davis, J.M.; Steinhorn, R.H. Superoxide Dismutase Improves Oxygenation and Reduces Oxidation in Neonatal Pulmonary Hypertension. Am. J. Respir. Crit. Care Med. 2012, 174, 1370–1377. [Google Scholar] [CrossRef]
- Lakshminrusimha, S.; Russell, J.A.; Steinhorn, R.H.; Ryan, R.M.; Gugino, S.F.; Morin, F.C.; Swartz, D.D.; Kumar, V.H. Pulmonary Arterial Contractility in Neonatal Lambs Increases with 100% Oxygen Resuscitation. Pediatr. Res. 2006, 59, 137–141. [Google Scholar] [CrossRef] [Green Version]
- Abman, S.H.; Hansmann, G.; Archer, S.L.; Ivy, D.D.; Adatia, I.; Chung, W.K.; Hanna, B.D.; Rosenzweig, E.B.; Raj, J.U.; Cornfield, D.; et al. Pediatric Pulmonary Hypertension:Guidelines from the American Heart Association and American Thoracic Society. Circulation 2015, 132, 2037–2099. [Google Scholar] [CrossRef]
- Hansmann, G.; Koestenberger, M.; Alastalo, T.P.; Apitz, C.; Austin, E.D.; Bonnet, D.; Budts, W.; D’Alto, M.; Gatzoulis, M.A.; Hasan, B.S.; et al. 2019 updated consensus statement on the diagnosis and treatment of pediatric pulmonary hypertension: The European Pediatric Pulmonary Vascular Disease Network (EPPVDN), endorsed by AEPC, ESPR and ISHLT. J. Heart Lung Transpl. 2019, 38, 879–901. [Google Scholar] [CrossRef] [Green Version]
- Rawat, M.; Chandrasekharan, P.; Gugino, S.F.; Koenigsknecht, C.; Nielsen, L.; Wedgwood, S.; Mathew, B.; Nair, J.; Steinhorn, R.; Lakshminrusimha, S. Optimal Oxygen Targets in Term Lambs with Meconium Aspiration Syndrome and Pulmonary Hypertension. Am. J. Respir. Cell Mol. Biol. 2020, 63, 510–518. [Google Scholar] [CrossRef]
- Manja, V.; Saugstad, O.D.; Lakshminrusimha, S. Oxygen saturation targets in preterm infants and outcomes at 18–24 months: A systematic review. Pediatrics 2017, 139, e20161609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manja, V.; Lakshminrusimha, S.; Cook, D.J. Oxygen Saturation Target Range for Extremely Preterm Infants: A Systematic Review and Meta-analysis. JAMA Pediatr. 2015, 169, 332–340. [Google Scholar] [CrossRef] [PubMed]
- Askie, L.M.; Darlow, B.A.; Finer, N.; Schmidt, B.; Stenson, B.; Tarnow-Mordi, W.; Davis, P.G.; Carlo, W.A.; Brocklehurst, P.; Davies, L.C.; et al. Association between Oxygen Saturation Targeting and Death or Disability in Extremely Preterm Infants in the Neonatal Oxygenation Prospective Meta-Analysis Collaboration. JAMA 2018, 319, 2190–2201. [Google Scholar] [CrossRef] [PubMed]
- Askie, L.M.; Henderson-Smart, D.J.; Irwig, L.; Simpson, J.M. Oxygen-Saturation Targets and Outcomes in Extremely Preterm Infants. N. Engl. J. Med. 2003, 349, 959–967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puligandla, P.S.; Skarsgard, E.D. The Canadian Pediatric Surgery Network Congenital Diaphragmatic Hernia Evidence Review Project: Developing national guidelines for care. Paediatr. Child Health 2016, 21, 183–186. [Google Scholar] [CrossRef] [Green Version]
- Alapati, D.; Jassar, R.; Shaffer, T.H. Management of Supplemental Oxygen for Infants with Persistent Pulmonary Hypertension of Newborn: A Survey. Am. J. Perinatol. 2017, 34, 276–282. [Google Scholar] [CrossRef] [Green Version]
- Moudgil, R.; Michelakis, E.D.; Archer, S.L. Hypoxic pulmonary vasoconstriction. J. Appl. Physiol. 2005, 98, 390–403. [Google Scholar] [CrossRef]
- Sjoding, M.W.; Dickson, R.P.; Iwashyna, T.J.; Gay, S.E.; Valley, T.S. Racial Bias in Pulse Oximetry Measurement. N. Engl. J. Med. 2020, 383, 2477–2478. [Google Scholar] [CrossRef]
- Vesoulis, Z.; Tims, A.; Lodhi, H.; Lalos, N.; Whitehead, H. Racial discrepancy in pulse oximeter accuracy in preterm infants. J. Perinatol. 2022, 42, 79–85. [Google Scholar] [CrossRef]
- Ong, M.S.; Abman, S.; Austin, E.D.; Feinstein, J.A.; Hopper, R.K.; Krishnan, U.S.; Mullen, M.P.; Natter, M.D.; Raj, J.U.; Rosenzweig, E.B.; et al. Racial and Ethnic Differences in Pediatric Pulmonary Hypertension: An Analysis of the Pediatric Pulmonary Hypertension Network Registry. J. Pediatr. 2019, 211, 63–71. [Google Scholar] [CrossRef]
- Jammeh, M.L.; Adibe, O.O.; Tracy, E.T.; Rice, H.E.; Clark, R.H.; Smith, P.B.; Greenberg, R.G. Racial/ethnic differences in necrotizing enterocolitis incidence and outcomes in premature very low birth weight infants. J. Perinatol. 2018, 38, 1386–1390. [Google Scholar] [CrossRef] [PubMed]
- Saunders, R.A.; Donahue, M.L.; Christmatm, L.M.; Pakalnis, A.I.V.; Tung, B.; Hardy, R.J.; Phelps, D.L. Racial variation in retinopathy of prematurity. Arch. Ophthalmol. 1997, 115, 604–608. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, J.D.; Hardy, R.J.; Kennedy, K.A.; Spencer, R.; Van Heuven, W.A.J.; Fielder, A.R. Lack of efficacy of light reduction in preventing retinopathy of prematurity. N. Engl. J. Med. 1998, 338, 1572–1576. [Google Scholar] [CrossRef] [PubMed]
- Shankaran, S.; Laptook, A.R.; Pappas, A.; Mcdonald, S.A.; Das, A.; Tyson, J.E.; Poindexter, B.B.; Schibler, K.; Bell, E.F.; Heyne, R.J.; et al. Effect of depth and duration of cooling on deaths in the NICU among neonates with hypoxic ischemic encephalopathy: A randomized clinical trial. JAMA 2014, 312, 2629–2639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Konduri, G.G.; Solimano, A.; Sokol, G.M.; Singer, J.; Ehrenkranz, R.A.; Singhal, N.; Wright, L.L.; Van Meurs, K.; Stork, E.; Kirpalani, H.; et al. A Randomized Trial of Early Versus Standard Inhaled Nitric Oxide Therapy in Term and Near-Term Newborn Infants with Hypoxic Respiratory Failure. Pediatrics 2004, 113, 559–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chandrasekharan, P.; Lakshminrusimha, S.; Abman, S.H. When to say no to inhaled nitric oxide in neonates? Semin. Fetal Neonatal Med. 2021, 26, 101200. [Google Scholar] [CrossRef]
- Lapointe, A.; Barrington, K. Pulmonary hypertension and the asphyxiated newborn. J. Pediatr. 2011, 158, e19–e24. [Google Scholar] [CrossRef]
- Rios, D.; Lapointe, A.; Schmolzer, G.; Mohammad, K.; VanMeurs, K.; Keller, R.; Seghal, A.; Lakshminrusimha, S.; Giesinger, R.E. Hemodynamic optimization for neonates with neonatal encephalopathy caused by hypoxic ischemic event: Physiological and therapeutic considerations. Semin. Fetal Neonatal Med. 2021, 26, 101277. [Google Scholar] [CrossRef]
- Bischoff, A.R.; Habib, S.; McNamara, P.J.; Giesinger, R.E. Hemodynamic response to milrinone for refractory hypoxemia during therapeutic hypothermia for neonatal hypoxic ischemic encephalopathy. J. Perinatol. 2021, 41, 2345–2354. [Google Scholar] [CrossRef]
- Faraci, F.M.; Didion, S.P. Vascular protection: Superoxide dismutase isoforms in the vessel wall. Arterioscler. Thromb. Vasc. Biol. 2004, 24, 1367–1373. [Google Scholar] [CrossRef] [Green Version]
- Lakshminrusimha, S.; Steinhorn, R.H.; Wedgwood, S.; Savorgnan, F.; Nair, J.; Mathew, B.; Gugino, S.F.; Russell, J.A.; Swartz, D.D. Pulmonary hemodynamics and vascular reactivity in asphyxiated term lambs resuscitated with 21 and 100% oxygen. J. Appl. Physiol. 2011, 111, 1441–1447. [Google Scholar] [CrossRef] [PubMed]
- Gitto, E.; Pellegrino, S.; Aversa, S.; Romeo, C.; Trimarchi, G.; Barberi, I.; Calabró, M.P.; Salpietro, C.D.; Reiter, R.J. Oxidative stress and persistent pulmonary hypertension of the newborn treated with inhaled nitric oxide and different oxygen concentrations. J. Matern.-Fetal Neonatal Med. 2012, 25, 1723–1726. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, B.; Roberts, R.S.; Whyte, R.K.; Asztalos, E.V.; Poets, C.; Rabi, Y.; Solimano, A.; Nelson, H.; Canadian Oxygen Trial Group. Impact of study oximeter masking algorithm on titration of oxygen therapy in the Canadian oxygen trial. J. Pediatr. 2014, 165, 666–671. [Google Scholar] [CrossRef] [PubMed]
- Donner, A.; Eliasziw, M. Sample size requirements for reliability studies. Stat. Med. 1987, 6, 441–448. [Google Scholar] [CrossRef] [PubMed]








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Siefkes, H.; Sunderji, S.; Vaughn, J.; Sankaran, D.; Vali, P.; Vadlaputi, P.; Timberline, S.; Bhatt, A.; Tancredi, D.; Lakshminrusimha, S. Factors to Consider to Study Preductal Oxygen Saturation Targets in Neonatal Pulmonary Hypertension. Children 2022, 9, 396. https://0-doi-org.brum.beds.ac.uk/10.3390/children9030396
Siefkes H, Sunderji S, Vaughn J, Sankaran D, Vali P, Vadlaputi P, Timberline S, Bhatt A, Tancredi D, Lakshminrusimha S. Factors to Consider to Study Preductal Oxygen Saturation Targets in Neonatal Pulmonary Hypertension. Children. 2022; 9(3):396. https://0-doi-org.brum.beds.ac.uk/10.3390/children9030396
Chicago/Turabian StyleSiefkes, Heather, Sherzana Sunderji, Jessica Vaughn, Deepika Sankaran, Payam Vali, Pranjali Vadlaputi, Sage Timberline, Avni Bhatt, Daniel Tancredi, and Satyan Lakshminrusimha. 2022. "Factors to Consider to Study Preductal Oxygen Saturation Targets in Neonatal Pulmonary Hypertension" Children 9, no. 3: 396. https://0-doi-org.brum.beds.ac.uk/10.3390/children9030396