
Outcomes in Establishing Individual Vessel Patency for Pediatric Pulmonary Vein Stenosis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Aims
2.2. Study Design
2.3. Outcomes and Data Collection
2.4. Statistical Analysis
2.5. Ethics Statement
3. Results
3.1. Patients
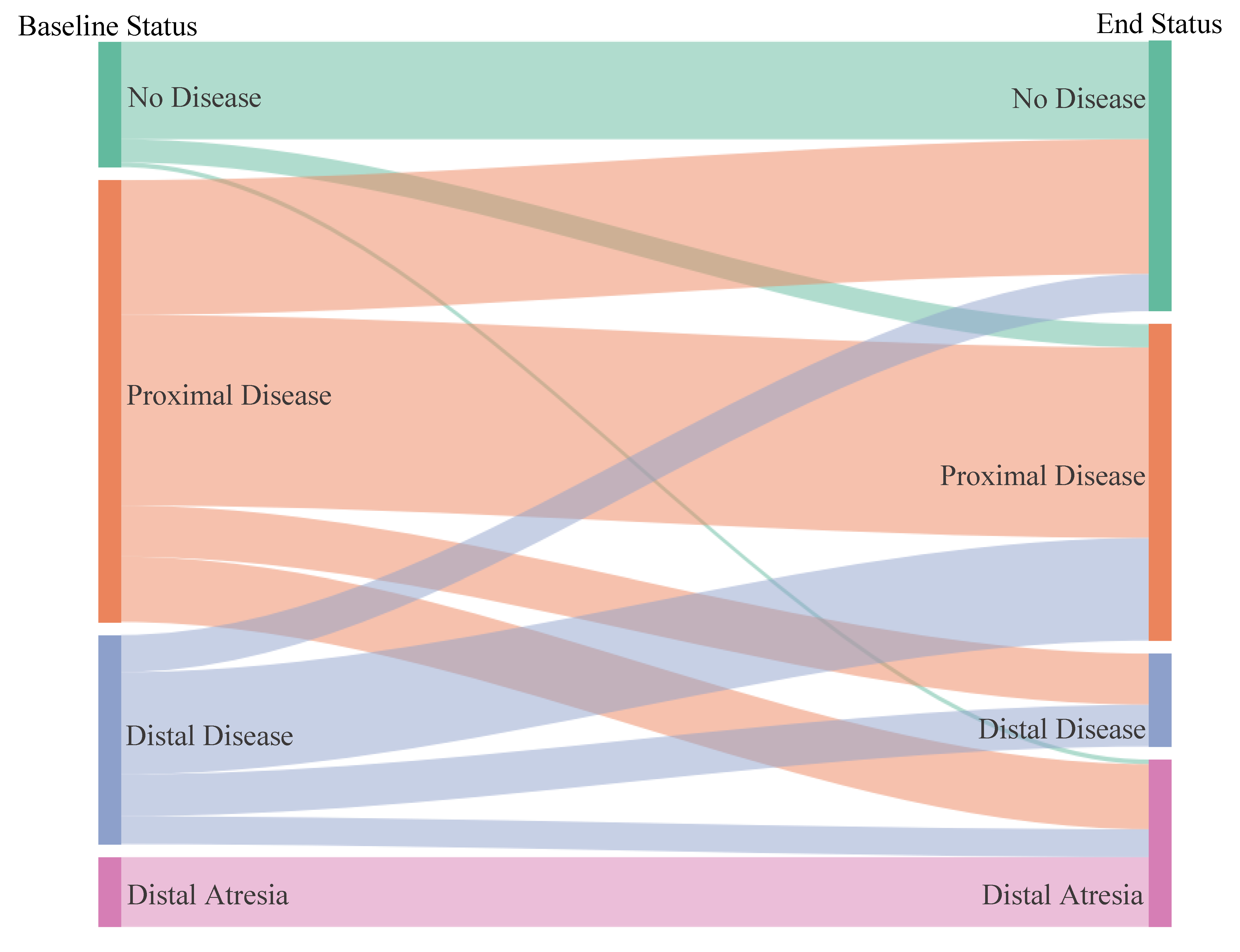
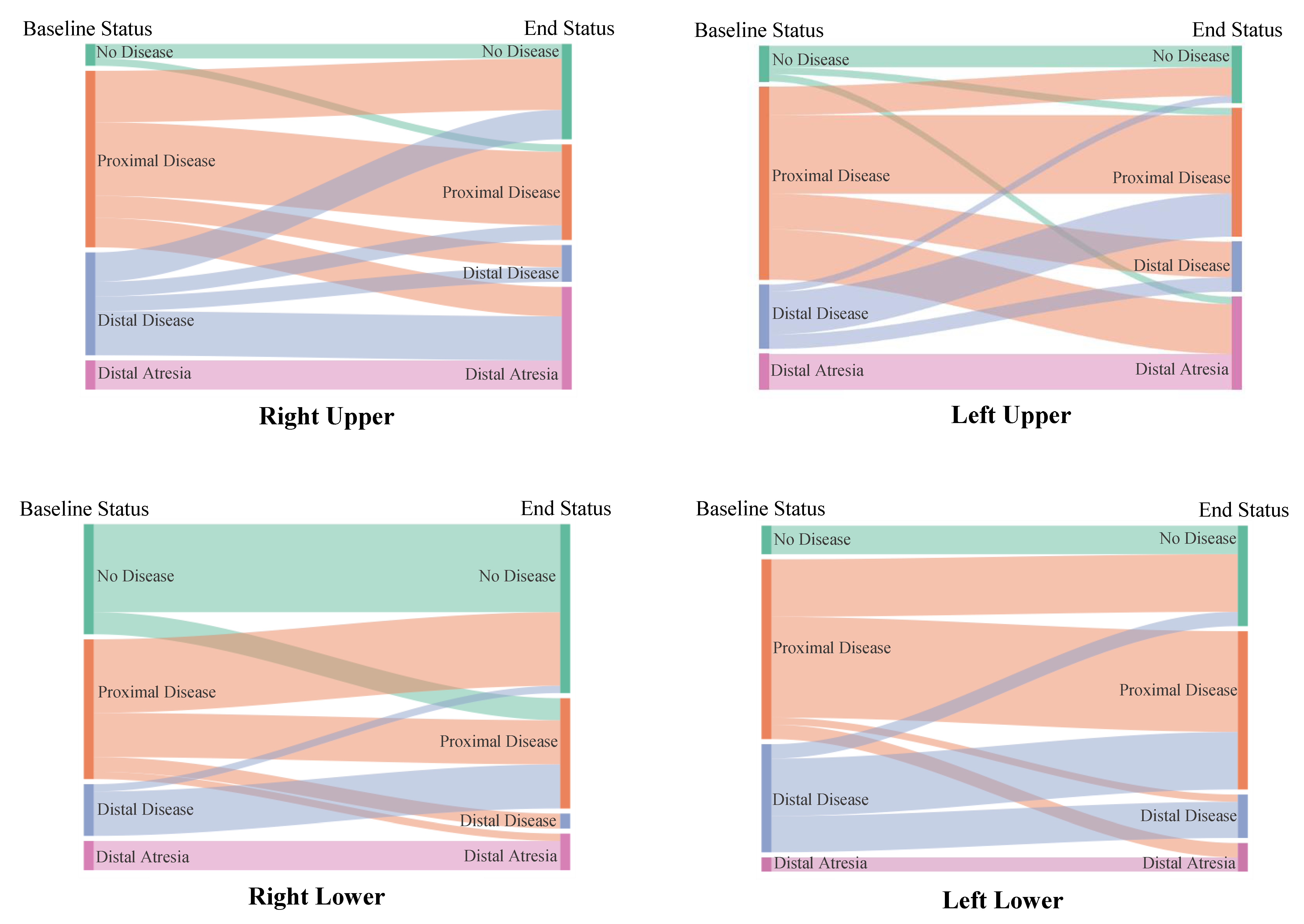
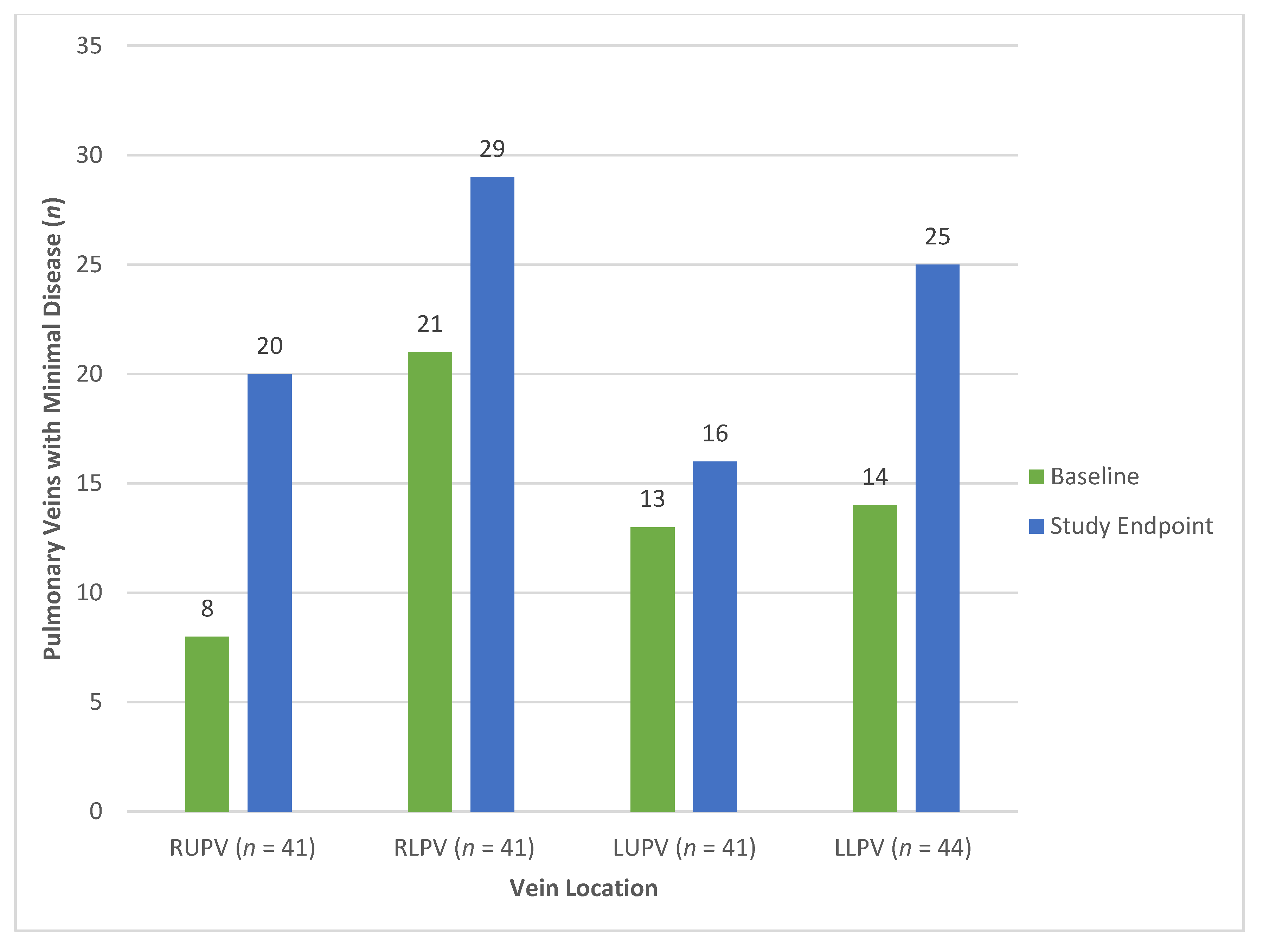
3.2. Vein Status
3.3. Primary Outcome
3.4. Secondary Outcome
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sadr, I.M.; Tan, P.E.; Kieran, M.W.; Jenkins, K.J. Mechanism of pulmonary vein stenosis in infants with normally connected veins. Am. J. Cardiol. 2000, 86, 577–579. [Google Scholar] [CrossRef]
- Riedlinger, W.F.J.; Juraszek, A.L.; Jenkins, K.J.; Nugent, A.W.; Balasubramanian, S.; Calicchio, M.L.; Kieran, M.W.; Collins, T. Pulmonary vein stenosis: Expression of receptor tyrosine kinases by lesional cells. Cardiovasc. Pathol. 2006, 15, 91–99. [Google Scholar] [CrossRef]
- Kovach, A.E.; Magcalas, P.M.; Ireland, C.; McEnany, K.; Oliveira, A.M.; Kieran, M.W.; Baird, C.W.; Jenkins, K.; Vargas, S.O. Paucicellular Fibrointimal Proliferation Characterizes Pediatric Pulmonary Vein Stenosis: Clinicopathologic Analysis of 213 Samples From 97 Patients. Am. J. Surg. Pathol. 2017, 41, 1198–1204. [Google Scholar] [CrossRef]
- Mahgoub, L.; Kaddoura, T.; Kameny, A.R.; Lopez Ortego, P.; Vanderlaan, R.D.; Kakadekar, A.; Dicke, F.; Rebeyka, I.; Calderone, C.A.; Redington, A.; et al. Pulmonary vein stenosis of ex-premature infants with pulmonary hypertension and bronchopulmonary dysplasia, epidemiology, and survival from a multicenter cohort. Pediatr. Pulmonol. 2017, 52, 1063–1070. [Google Scholar] [CrossRef]
- Balasubramanian, S.; Rehman, M.; Gauvreau, K.; Jenkins, K.J. Bilateral disease and early age at presentation are associated with shorter survival in patients with congenital heart disease and intraluminal pulmonary vein stenosis. Congenit. Heart Dis. 2012, 7, 378–386. [Google Scholar] [CrossRef]
- Rito, M.L.; Gazzaz, T.; Wilder, T.J.; Vanderlaan, R.D.; Van Arsdell, G.S.; Honjo, O.; Yoo, S.J.; Caldarone, C.A. Pulmonary vein stenosis: Severity and location predict survival after surgical repair. J. Thorac. Cardiovasc. Surg. 2016, 151, 657–666.e1-2. [Google Scholar] [CrossRef] [Green Version]
- Kalfa, D.; Belli, E.; Bacha, E.; Lambert, V.; di Carlo, D.; Kostolny, M.; Salminen, J.; Nosal, M.; Poncelet, A.; Horer, J.; et al. Primary Pulmonary Vein Stenosis: Outcomes, Risk Factors, and Severity Score in a Multicentric Study. Ann. Thorac. Surg. 2017, 104, 182–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sykes, M.C.; Ireland, C.; McSweeney, J.E.; Rosenholm, E.; Andren, K.G.; Kulik, T.J. The impact of right ventricular pressure and function on survival in patients with pulmonary vein stenosis. Pulm. Circ. 2018, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DiLorenzo, M.P.; Santo, A.; Rome, J.J.; Zhang, H.; Faerber, J.A.; Mercer-Rosa, L.; Hopper, R.K. Pulmonary Vein Stenosis: Outcomes in Children With Congenital Heart Disease and Prematurity. Semin. Thorac. Cardiovasc. Surg. 2019, 31, 266–273. [Google Scholar] [CrossRef]
- Peng, L.F.; Lock, J.E.; Nugent, A.W.; Jenkins, K.J.; McElhinney, D.B. Comparison of conventional and cutting balloon angioplasty for congenital and postoperative pulmonary vein stenosis in infants and young children. Catheter. Cardiovasc. Interv. 2010, 75, 1084–1090. [Google Scholar] [CrossRef]
- Quinonez, L.G.; Gauvreau, K.; Borisuk, M.; Ireland, C.; Marshall, A.M.; Mayer, J.E.; Jenkins, K.J.; Fynn-Thompson, F.E.; Baird, C.W. Outcomes of surgery for young children with multivessel pulmonary vein stenosis. J. Thorac. Cardiovasc. Surg. 2015, 150, 911–917. [Google Scholar] [CrossRef] [Green Version]
- Balasubramanian, S.; Marshall, A.C.; Gauvreau, K.; Peng, L.F.; Nugent, A.W.; Lock, J.E.; McElhinney, D.B. Outcomes after stent implantation for the treatment of congenital and postoperative pulmonary vein stenosis in children. Circ. Cardiovasc. Interv. 2012, 5, 109–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Callahan, R.; Kieran, M.W.; Baird, C.W.; Colan, S.D.; Gauvreau, K.; Ireland, C.M.; Marshall, A.C.; Sena, L.M.; Vargas, S.O.; Jenkins, K.J. Adjunct Targeted Biologic Inhibition Agents to Treat Aggressive Multivessel Intraluminal Pediatric Pulmonary Vein Stenosis. J. Pediatr. 2018, 198, 29–35.e5. [Google Scholar] [CrossRef] [PubMed]
- Pogoriler, J.E.; Kulik, T.J.; Casey, A.M.; Baird, C.W.; Mullen, M.P.; Jenkins, K.J.; Vargas, S.O. Lung Pathology in Pediatric Pulmonary Vein Stenosis. Pediatr. Dev. Pathol. 2016, 19, 219–229. [Google Scholar] [CrossRef] [PubMed]
- Rosenblum, J.M.; Altin, H.F.; Gillespie, S.E.; Bauser-Heaton, H.; Kanter, K.A.; Sinha, R.; Cory, M.; Alsoufi, B. Management outcomes of primary pulmonary vein stenosis. J. Thorac. Cardiovasc. Surg. 2020, 159, 1029–1036.e1. [Google Scholar] [CrossRef]
- Callahan, R.; Jenkins, K.J.; Gauthier, Z.; Gauvreau, K.; Porras, D. Preliminary findings on the use of intravascular ultrasound in the assessment of pediatric pulmonary vein stenosis. Catheter. Cardiovasc. Interv. 2020. [Google Scholar] [CrossRef]
- Drubach, L.A.; Jenkins, K.J.; Stamoulis, C.; Palmer, E.L.; Lee, E.Y. Evaluation of Primary Pulmonary Vein Stenosis in Children: Comparison of Radionuclide Perfusion Lung Scan and Angiography. Am. J. Roentgenol. 2015, 205, 873–877. [Google Scholar] [CrossRef]
- Ibrahim, A.R.; Eliasson, L.; Apperley, J.F.; Milojkovic, D.; Bua, M.; Szydlo, R.; Mahon, F.X.; Kozlowski, K.; Paliompeis, C.; Foroni, L.; et al. Poor adherence is the main reason for loss of CCyR and imatinib failure for chronic myeloid leukemia patients on long-term therapy. Blood 2011, 117, 3733–3736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noens, L.; Van Lierde, M.A.; De Bock, R.; Verhoef, G.; Zachée, P.; Berneman, Z.; Martiat, P.; Mineur, P.; Van Eygen, K.; MacDonald, K.; et al. Prevalence, determinants, and outcomes of nonadherence to imatinib therapy in patients with chronic myeloid leukemia: The ADAGIO study. Blood 2009, 113, 5401–5411. [Google Scholar] [CrossRef] [Green Version]
- Chiu, J.-J.; Chien, S. Effects of disturbed flow on vascular endothelium: Pathophysiological basis and clinical perspectives. Physiol. Rev. 2011, 91, 327–387. [Google Scholar] [CrossRef] [Green Version]
- Choi, C.; Gauvreau, K.; Levy, P.; Callahan, R.; Jenkins, K.J.; Chen, M. Longer Exposure to Left-to-Right Shunts Is a Risk Factor for Pulmonary Vein Stenosis in Patients with Trisomy 21. Children 2021, 8, 19. [Google Scholar] [CrossRef] [PubMed]
- Feins, E.N.; Ireland, C.M.; Chavez, M.; Gauvreau, K.; Callahan, R.; Jenkins, K.J.; Baird, C.W. Pulmonary Vein Stenosis Management & Outcomes—A Large Single Center Retrospective Review [Abstract]. In Proceedings of the 100th Annual Meeting of the American Association for Thoracic Surgery, Online, 22–23 May 2020. [Google Scholar]
- Lee, E.Y.; Jenkins, K.J.; Muneeb, M.; Marshall, A.C.; Tracy, D.A.; Zurakowski, D.; Boiselle, P.M. Proximal pulmonary vein stenosis detection in pediatric patients: Value of multiplanar and 3-D VR imaging evaluation. Pediatr. Radiol. 2013, 43, 929–936. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Category | Criteria |
|---|---|
| 1 | None: no narrowing of the luminal contour. |
| 2 | Mild proximal narrowing: mild (<50%) narrowing of the proximal (<5 mm) luminal contour. |
| 3 | Proximal atretic: complete obliteration of the luminal contour confined to the proximal (<5 mm) vessel segment (distal vasculature unaffected). |
| 4 | Significant proximal narrowing: significant (>50%) narrowing of the proximal (<5 mm) luminal contour. |
| 5 | Extensive narrowing: narrowing of the luminal contour confined to a defined portion of the vessel but extending > 5 mm beyond the left atrium. |
| 6 | Diffuse: narrowing of the entire luminal contour. |
| 7 | Distal atretic: complete obliteration of the luminal contour extending >5 mm within the vessel segment. |
| Patient Characteristics (n = 46) | N (%) or Median [Interquartile Range] (Range) |
|---|---|
| Age at drug start date (months) | 7 [5, 12] (1, 61) |
| Age at drug start date | |
| → <6 months | 17 (37%) |
| → 6–11 months | 19 (41%) |
| → ≥1 year | 10 (22%) |
| Sex female | 21 (46%) |
| Premature birth (<37 weeks gestation) | 18 (39%) |
| If premature, gestational age (week) | 32 [29, 35] (25, 36) |
| Diagnosis | |
| → CHD | 21 (46%) |
| → CHD/TAPVC | 13 (28%) |
| → CHD/PAPVC | 3 (7%) |
| → Primary PVS | 4 (9%) |
| → Isolated lung disease | 5 (11%) |
| Single ventricle physiology | 6 (13%) |
| Presence of lung disease | 17 (37%) |
| Genetic syndrome | 13 (28%) |
| Number of veins affected at baseline | |
| → 2 | 8 (17%) |
| → 3 | 13 (28%) |
| → 4 | 25 (54%) |
| Percent of eligible drug doses received (n = 44) | 0.86 [0.75, 0.92] (0.54, 0.99) |
| Surgery type prior to drug start | |
| → None | 4 (9%) |
| → Conventional sutureless | 19 (41%) |
| → Modified sutureless | 19 (41%) |
| → Other 1 | 4 (9%) |
| PVS Status at Study Endpoint | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| PVS Status at Baseline | n | 1 | 2 | 3 | 4 | 5 | 6 | 7 | |
| 1 | No disease | 27 | 21 (78) | 3 (11) | 0 (0) | 2 (7) | 0 (0) | 0 (0) | 1 (4) |
| 2 | Mild proximal narrowing | 29 | 11 (38) | 7 (24) | 0 (0) | 5 (17) | 3 (10) | 1 (3) | 2 (7) |
| 3 | Proximal atretic | 4 | 0 (0) | 1 (25) | 0 (0) | 1 (25) | 0 (0) | 1 (25) | 1 (25) |
| 4 | Significant proximal narrowing | 62 | 18 (29) | 16 (26) | 0 (0) | 11 (18) | 5 (8) | 1 (2) | 11 (18) |
| 5 | Extensive narrowing | 30 | 8 (27) | 3 (10) | 1 (3) | 9 (30) | 2 (7) | 4 (13) | 3 (10) |
| 6 | Diffuse | 15 | 0 (0) | 2 (13) | 3 (20) | 4 (27) | 0 (0) | 3 (20) | 3 (20) |
| 7 | Distal atretic | 15 | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 15 (100) |
| Total | 182 | 58 | 32 | 4 | 32 | 10 | 10 | 36 | |
| Minimal Disease 1 | More Than Minimal Disease 1 | Odds Ratio | 95% Confidence Interval | p Value | |
|---|---|---|---|---|---|
| (n = 90) | (n = 77) | ||||
| Patient Level | |||||
| Age at drug start date (months) | 9 (1, 61) | 6 (1, 45) | 1.07 | (1.01, 1.12) | 0.017 |
| Age at drug start date | |||||
| → <6 months | 24 (27%) | 37 (48%) | 1.00 | - | - |
| → 6 months to <1 year | 39 (43%) | 32 (42%) | 1.88 | (0.78, 4.51) | 0.16 |
| → ≥1 year | 27 (30%) | 8 (10%) | 5.20 | (2.00, 13.5) | 0.001 |
| Sex female | 45 (50%) | 32 (42%) | 1.41 | (0.63, 3.16) | 0.41 |
| Premature birth | 39 (43%) | 28 (36%) | 1.34 | (0.62, 2.90) | 0.46 |
| Diagnosis primary PVS | 4 (4%) | 12 (16%) | 0.25 | (0.06, 1.00) | 0.051 |
| Diagnosis anomalous vein | 27 (30%) | 24 (31%) | 0.95 | (0.42, 2.11) | 0.89 |
| Single ventricle physiology | 13 (14%) | 10 (13%) | 1.13 | (0.38, 3.34) | 0.82 |
| Presence of lung disease | 38 (42%) | 21 (27%) | 1.95 | (0.81, 4.69) | 0.14 |
| Percent of eligible drug doses received (↑5%) (n = 86, 73) | 0.87 (0.81, 0.93) | 0.85 (0.72, 0.90) | 1.08 | (0.94, 1.26) | 0.27 |
| Surgery type | |||||
| → Conventional sutureless | 37 (41%) | 35 (45%) | 1.00 | - | - |
| → Modified sutureless | 36 (40%) | 33 (43%) | 1.03 | (0.44, 2.41) | 0.94 |
| → None/Other | 17 (19%) | 9 (12%) | 1.79 | (0.54, 5.91) | 0.34 |
| Vein Level | |||||
| No distal disease at baseline | 77 (86%) | 45 (58%) | 4.21 | (1.86, 9.54) | 0.001 |
| No disease at baseline | 24 (27%) | 3 (4%) | 8.97 | (2.43, 33.0) | 0.001 |
| Location right upper | 20 (22%) | 21 (27%) | 0.76 | (0.41, 1.41) | 0.39 |
| Location right lower | 29 (32%) | 12 (16%) | 2.58 | (1.31, 5.05) | 0.006 |
| Location left upper | 16 (18%) | 25 (32%) | 0.45 | (0.24, 0.85) | 0.013 |
| Location left lower | 25 (28%) | 19 (25%) | 1.17 | (0.64, 2.14) | 0.60 |
| Vein part of common vein | 19 (21%) | 9 (12%) | 2.02 | (0.79, 5.20) | 0.14 |
| Odds Ratio | 95% Confidence Interval | p Value | |
|---|---|---|---|
| No disease at baseline | 6.15 | (1.69, 22.4) | 0.006 |
| No distal disease at baseline | 3.69 | (1.52, 8.94) | 0.004 |
| Location not left upper | 2.58 | (1.07, 6.19) | 0.034 |
| Age at drug start date | |||
| → <6 months | 1.00 | - | - |
| → 6 months to <1 year | 1.59 | (0.63, 4.01) | 0.33 |
| → ≥1 year | 5.59 | (1.81, 17.3) | 0.003 |
| Number of Reinterventions 1 | IRR 2 | 95% Confidence Interval | p Value | |||
|---|---|---|---|---|---|---|
| None (n = 85) | 1 (n = 25) | ≥2 (n = 57) | ||||
| Patient Level | ||||||
| Age at drug start date (months) | 9 (2, 61) | 6 (3, 45) | 6 (1, 45) | 0.96 | (0.89, 1.03) | 0.24 |
| Age at drug start date | ||||||
| → <6 months | 19 (22%) | 12 (48%) | 30 (53%) | 1.00 | - | - |
| → 6 months to <1 year | 45 (53%) | 5 (20%) | 21 (37%) | 0.40 | (0.20, 0.81) | 0.011 |
| → ≥1 year | 21 (25%) | 8 (32%) | 6 (11%) | 0.29 | (0.12, 0.71) | 0.007 |
| Sex female | 44 (52%) | 8 (32%) | 25 (44%) | 0.87 | (0.44, 1.74) | 0.70 |
| Premature birth | 33 (39%) | 9 (36%) | 25 (44%) | 1.48 | (0.73, 3.00) | 0.27 |
| Diagnosis primary PVS | 4 (5%) | 9 (36%) | 3 (5%) | 0.94 | (0.47, 1.88) | 0.86 |
| Diagnosis anomalous vein | 23 (27%) | 8 (32%) | 20 (35%) | 1.11 | (0.54, 2.32) | 0.77 |
| Single ventricle physiology | 13 (15%) | 3 (12%) | 7 (12%) | 0.73 | (0.29, 1.81) | 0.49 |
| Presence of lung disease | 28 (33%) | 7 (28%) | 24 (42%) | 1.50 | (0.75, 2.99) | 0.25 |
| Genetic syndrome | 16 (19%) | 8 (32%) | 21 (37%) | 1.13 | (0.59, 2.17) | 0.72 |
| Percent of eligible drug doses received (↑5%) (n = 79, 23, 57) | 0.90 (0.54, 0.99) | 0.89 (0.54, 0.98) | 0.81 (0.55, 0.92) | 0.78 | (0.68, 0.89) | <0.001 |
| Surgery type | ||||||
| → Conventional sutureless | 34 (40%) | 14 (56%) | 24 (42%) | 1.00 | - | - |
| → Modified sutureless | 35 (41%) | 11 (44%) | 23 (40%) | 0.78 | (0.36, 1.65) | 0.51 |
| → None/other | 16 (19%) | 0 (0%) | 10 (18%) | 0.74 | (0.27, 2.00) | 0.55 |
| Vein Level | ||||||
| Distal disease at baseline | 12 (14%) | 8 (32%) | 25 (44%) | 1.79 | (1.09, 2.96) | 0.022 |
| No disease at baseline | 24 (28%) | 2 (8%) | 1 (2%) | 0.19 | (0.04, 0.90) | 0.036 |
| Location right upper | 22 (26%) | 7 (28%) | 12 (21%) | 0.75 | (0.48, 1.19) | 0.22 |
| Location right lower | 24 (28%) | 7 (28%) | 10 (18%) | 0.80 | (0.57, 1.14) | 0.22 |
| Location left upper | 17 (20%) | 8 (32%) | 16 (28%) | 1.17 | (0.83, 1.66) | 0.37 |
| Location left lower | 22 (26%) | 3 (12%) | 19 (33%) | 1.31 | (0.96, 1.79) | 0.090 |
| Vessel part of common vein | 23 (27%) | 3 (12%) | 2 (4%) | 0.19 | (0.06, 0.63) | 0.007 |
| IRR | 95% Confidence Interval | p Value | |
|---|---|---|---|
| No disease at baseline | 0.18 | (0.05, 0.67) | 0.011 |
| Percent of eligible drug doses received (↑5%) | 0.76 | (0.68, 0.85) | <0.001 |
| Vessel part of common vein | 0.17 | (0.05, 0.55) | 0.003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Callahan, R.; Gauvreau, K.; Marshall, A.C.; Sena, L.M.; Baird, C.W.; Ireland, C.M.; McEnaney, K.; Bjornlund, E.C.; Mendonca, J.T.; Jenkins, K.J. Outcomes in Establishing Individual Vessel Patency for Pediatric Pulmonary Vein Stenosis. Children 2021, 8, 210. https://0-doi-org.brum.beds.ac.uk/10.3390/children8030210
Callahan R, Gauvreau K, Marshall AC, Sena LM, Baird CW, Ireland CM, McEnaney K, Bjornlund EC, Mendonca JT, Jenkins KJ. Outcomes in Establishing Individual Vessel Patency for Pediatric Pulmonary Vein Stenosis. Children. 2021; 8(3):210. https://0-doi-org.brum.beds.ac.uk/10.3390/children8030210
Chicago/Turabian StyleCallahan, Ryan, Kimberlee Gauvreau, Audrey C. Marshall, Laureen M. Sena, Christopher W. Baird, Christina M. Ireland, Kerry McEnaney, Elsa C. Bjornlund, Juliana T. Mendonca, and Kathy J. Jenkins. 2021. "Outcomes in Establishing Individual Vessel Patency for Pediatric Pulmonary Vein Stenosis" Children 8, no. 3: 210. https://0-doi-org.brum.beds.ac.uk/10.3390/children8030210