
Asthma Comorbidities: Frequency, Risk Factors, and Associated Burden in Children and Adolescents

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
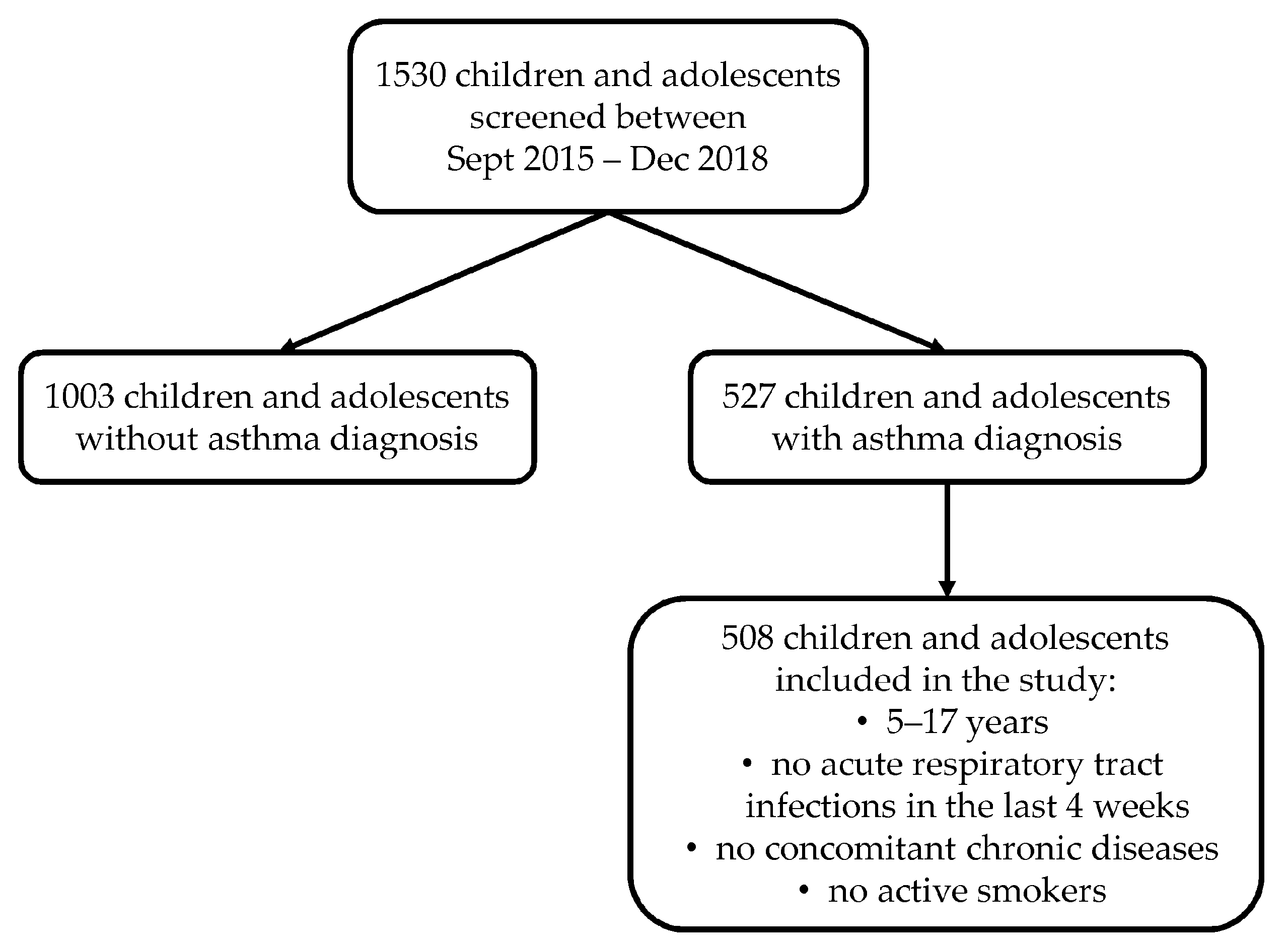
2.1. Study Design and Population
2.2. Assessments
2.3. Asthma Comorbidities
2.4. Host and Environmental Risk Factors
2.5. Visual Analog Scale
2.6. Childhood Asthma Control Test and Asthma Control Test
2.7. Pediatric Asthma Quality of Life Questionnaire
2.8. Pittsburgh Sleep Quality Index
2.9. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Karlstad, Ø.; Nafstad, P.; Tverdal, A.; Skurtveit, S.; Furu, K. Comorbidities in an asthma population 8–29 years old: A study from the Norwegian Prescription Database. Pharmacoepidemiol. Drug Saf. 2012, 21, 1045–1052. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinart, M.; Benet, M.; Annesi-Maesano, I.; von Berg, A.; Berdel, D.; Carlsen, K.C.; Carlsen, K.-H.; Bindslev-Jensen, C.; Eller, E.; Fantini, M.P.; et al. Comorbidity of eczema, rhinitis, and asthma in IgE-sensitised and non-IgE-sensitised children in MeDALL: A population-based cohort study. Lancet Respir. Med. 2014, 2, 131–140. [Google Scholar] [CrossRef] [Green Version]
- Cibella, F.; Ferrante, G.; Cuttitta, G.; Bucchieri, S.; Melis, M.R.; La Grutta, S.; Viegi, G. The burden of rhinitis and rhinoconjunctivitis in adolescents. Allergy Asthma Immunol. Res. 2015, 7, 44–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poddighe, D.; Brambilla, I.; Licari, A.; Marseglia, G.L. Pediatric rhinosinusitis and asthma. Respir. Med. 2018, 141, 94–99. [Google Scholar] [CrossRef]
- Cvejoska-Cholakovska, V.; Kocova, M.; Velikj-Stefanovska, V.; Vlashki, E. The association between asthma and obesity in children–inflammatory and mechanical factors. Open Access Maced. J. Med. Sci. 2019, 7, 1314. [Google Scholar] [CrossRef] [Green Version]
- Liu, P.-C.; Kieckhefer, G.M.; Gau, B.-S. A systematic review of the association between obesity and asthma in children. J. Adv. Nurs. 2013, 69, 1446–1465. [Google Scholar] [CrossRef] [Green Version]
- Gershon, A.S.; Wang, C.; Guan, J.; To, T. Burden of comorbidity in individuals with asthma. Thorax 2010, 65, 612–618. [Google Scholar] [CrossRef] [Green Version]
- Ballardini, N.; Kull, I.; Lind, T.; Hallner, E.; Almqvist, C.; Östblom, E.; Melén, E.; Pershagen, G.; Lilja, G.; Bergström, A.; et al. Development and comorbidity of eczema, asthma and rhinitis to age 12–data from the BAMSE birth cohort. Allergy 2012, 67, 537–544. [Google Scholar] [CrossRef] [Green Version]
- Sun, H.-L.; Yeh, C.-J.; Ku, M.-S.; Lue, K.-H. Coexistence of allergic diseases: Patterns and frequencies. Allergy Asthma Proc. 2012, 33, e1–e4. [Google Scholar] [CrossRef]
- Geraldini, M.; Chong Neto, H.J.; Riedi, C.A.; Rosário, N.A. Epidemiology of ocular allergy and co-morbidities in adolescents. J. Pediatr. 2013, 89, 354–360. [Google Scholar] [CrossRef] [Green Version]
- Beydon, N.; Delclaux, C. BMI as a comorbidity factor in childhood asthma. Expert Rev. Respir. Med. 2012, 6, 569–571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fedele, D.A.; Janicke, D.M.; Lim, C.S.; Abu-Hasan, M. An examination of comorbid asthma and obesity: Assessing differences in physical activity, sleep duration, health-related quality of life and parental distress. J. Asthma 2014, 51, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Ross, K.R.; Storfer-Isser, A.; Hart, M.A.; Kibler, A.M.V.; Rueschman, M.; Rosen, C.L.; Kercsmar, C.M.; Redline, S. Sleep-disordered breathing is associated with asthma severity in children. J. Pediatrics 2012, 160, 736–742. [Google Scholar] [CrossRef] [Green Version]
- Sigurdardottir, S.T.; Jonasson, K.; Clausen, M.; Lilja Bjornsdottir, K.; Sigurdardottir, S.E.; Roberts, G.; Grimshaw, K.; Papadopoulos, N.G.; Xepapadaki, P.; Fiandor, A.; et al. Prevalence and early-life risk factors of school-age allergic multimorbidity: The EuroPrevall-iFAAM birth cohort. Allergy 2021, 76, 2855–2865. [Google Scholar] [CrossRef] [PubMed]
- Nriagu, J.; Martin, J.; Smith, P.; Socier, D. Residential hazards, high asthma prevalence and multimorbidity among children in Saginaw, Michigan. Sci. Total Environ. 2012, 416, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Pyle, R.C.; Divekar, R.; May, S.M.; Narla, N.; Pianosi, P.T.; Hartz, M.F.; Ott, N.L.; Park, M.A.; McWilliams, D.B.; Green, J.A.; et al. Asthma-associated comorbidities in children with and without secondhand smoke exposure. Ann. Allergy Asthma Immunol. 2015, 115, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, I.L.; Li, J.T.; Bernstein, D.I.; Hamilton, R.; Spector, S.L.; Tan, R.; Sicherer, S.; Golden, D.B.; Khan, D.A.; Nicklas, R.A.; et al. Allergy diagnostic testing: An updated practice parameter. Ann. Allergy Asthma Immunol. 2008, 100, S1–S148. [Google Scholar] [CrossRef]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; van der Grinten, C.P.M.; Gustafsson, P.; et al. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [Green Version]
- Quanjer, P.H.; Stanojevic, S.; Cole, T.J.; Baur, X.; Hall, G.L.; Culver, B.H.; Enright, P.L.; Hankinson, J.L.; Ip, M.S.; Zheng, J.; et al. Multi-ethnic reference values for spirometry for the 3–95-yr age range: The global lung function 2012 equations. Eur. Respir. J. 2012, 40, 1324–1343. [Google Scholar] [CrossRef]
- American Thoracic Society; European Repiratory Society ATS/ERS recommendations for standardized procedures for the online and offline measurement of exhaled lower respiratory nitric oxide and nasal nitric oxide, 2005. Am. J. Respir. Crit. Care Med. 2005, 171, 912–930. [CrossRef] [Green Version]
- Renzoni, E.; Sestini, P.; Corbo, G.; Biggeri, A.; Viegi, G.; Forastiere, F. Asthma and respiratory symptoms in 6–7 yr old Italian children: Gender, latitude, urbanization and socioeconomic factors SIDRIA (Italian Studies on Respiratory Disorders in Childhood and the Environment). Eur. Respir. J 1997, 10, 1780–1786. [Google Scholar]
- Bousquet, P.; Combescure, C.; Neukirch, F.; Klossek, J.; Mechin, H.; Daures, J.-P.; Bousquet, J. Visual analog scales can assess the severity of rhinitis graded according to ARIA guidelines. Allergy 2007, 62, 367–372. [Google Scholar] [CrossRef] [PubMed]
- Liu, A.H.; Zeiger, R.; Sorkness, C.; Mahr, T.; Ostrom, N.; Burgess, S.; Rosenzweig, J.C.; Manjunath, R. Development and cross-sectional validation of the Childhood Asthma Control Test. J. Allergy Clin. Immunol. 2007, 119, 817–825. [Google Scholar] [CrossRef] [PubMed]
- Nathan, R.A.; Sorkness, C.A.; Kosinski, M.; Schatz, M.; Li, J.T.; Marcus, P.; Murray, J.J.; Pendergraft, T.B. Development of the asthma control test: A survey for assessing asthma control. J. Allergy Clin. Immunol. 2004, 113, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Ricci, G.; Dondi, A.; Baldi, E.; Bendandi, B.; Giannetti, A.; Masi, M. Use of the Italian version of the Pediatric Asthma Quality of Life Questionnaire in the daily practice: Results of a prospective study. BMC Pediatrics 2009, 9, 30. [Google Scholar] [CrossRef] [Green Version]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Chowdhury, N.U.; Guntur, V.P.; Newcomb, D.C.; Wechsler, M.E. Sex and gender in asthma. Eur. Respir. Rev. 2021, 30, 210067. [Google Scholar] [CrossRef]
- Rosário, C.S.; Cardozo, C.A.; Neto, H.J.C.; Rosário Filho, N.A. Do gender and puberty influence allergic diseases? Allergol. Immunopathol. 2021, 49, 122–125. [Google Scholar] [CrossRef] [PubMed]
- Manivannan, S.; Chandrasekaran, V.; Subramanian, N. A comparative study of clinical profile and symptom control in overweight and normal weight school-age children with mild persistent asthma. Health Sci. Rep. 2021, 4, e224. [Google Scholar] [CrossRef]
- Ross, K.R.; Hart, M.A.; Storfer-Isser, A.; Kibler, A.M.V.; Johnson, N.L.; Rosen, C.L.; Kercsmar, C.M.; Redline, S. Obesity and obesity related co-morbidities in a referral population of children with asthma. Pediatric Pulmonol. 2009, 44, 877–884. [Google Scholar] [CrossRef] [Green Version]
- Palmer, L.; Knuiman, M.; Divitini, M.; Burton, P.; James, A.; Bartholomew, H.; Ryan, G.; Musk, A. Familial aggregation and heritability of adult lung function: Results from the Busselton Health Study. Eur. Respir. J. 2001, 17, 696–702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmad, K.; Kabir, E.; Ormsby, G.M.; Khanam, R. Clustering of asthma and related comorbidities and their association with maternal health during pregnancy: Evidence from an Australian birth cohort. BMC Public Health 2021, 21, 1952. [Google Scholar] [CrossRef] [PubMed]
- Martel, M.; Rey, E.; Beauchesne, M.; Malo, J.; Perreault, S.; Forget, A.; Blais, L. Control and severity of asthma during pregnancy are associated with asthma incidence in offspring: Two-stage case–control study. Eur. Respir. J. 2009, 34, 579–587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gough, H.; Grabenhenrich, L.; Reich, A.; Eckers, N.; Nitsche, O.; Schramm, D.; Beschorner, J.; Hoffmann, U.; Schuster, A.; Bauer, C.-P.; et al. Allergic multimorbidity of asthma, rhinitis and eczema over 20 years in the German birth cohort MAS. Pediatric Allergy Immunol. 2015, 26, 431–437. [Google Scholar] [CrossRef]
- Lodge, C.J.; Tan, D.; Lau, M.; Dai, X.; Tham, R.; Lowe, A.J.; Bowatte, G.; Allen, K.; Dharmage, S.C. Breastfeeding and asthma and allergies: A systematic review and meta-analysis. Acta Paediatr. 2015, 104, 38–53. [Google Scholar] [CrossRef]
- Victora, C.G.; Bahl, R.; Barros, A.J.; França, G.V.; Horton, S.; Krasevec, J.; Murch, S.; Sankar, M.J.; Walker, N.; Rollins, N.C.; et al. Breastfeeding in the 21st century: Epidemiology, mechanisms, and lifelong effect. Lancet 2016, 387, 475–490. [Google Scholar] [CrossRef] [Green Version]
- Guilbert, T.W.; Stern, D.A.; Morgan, W.J.; Martinez, F.D.; Wright, A.L. Effect of breastfeeding on lung function in childhood and modulation by maternal asthma and atopy. Am. J. Respir. Crit. Care Med. 2007, 176, 843–848. [Google Scholar] [CrossRef] [Green Version]
- Azalim, S.P.; Camargos, P.; Alves, A.L.; Senna, M.I.B.; Sakurai, E.; Schwabe Keller, W. Exposure to environmental factors and relationship to allergic rhinitis and/or asthma. Ann. Agric. Environ. Med. 2014, 21, 59–63. [Google Scholar]
- Cibella, F.; Cuttitta, G.; La Grutta, S.; Melis, M.R.; Lospalluti, M.L.; Uasuf, C.G.; Bucchieri, S.; Viegi, G. Proportional Venn diagram and determinants of allergic respiratory diseases in Italian adolescents. Pediatric Allergy Immunol. 2011, 22, 60–68. [Google Scholar] [CrossRef] [Green Version]
- Baldacci, S.; Modena, P.; Carrozzi, L.; Pedreschi, M.; Vellutini, M.; Biavati, P.; Simoni, M.; Sapigni, T.; Viegi, G.; Paoletti, P.; et al. Skin prick test reactivity to common aeroallergens in relation to total IgE, respiratory symptoms, and smoking in a general population sample of northern Italy. Allergy 1996, 51, 149–156. [Google Scholar] [CrossRef]
- Sears, M.; Burrows, B.; Flannery, E.; Herbison, G.; Holdaway, M. Atopy in childhood. I. Gender and allergen related risks for development of hay fever and asthma. Clin. Exp. Allergy 1993, 23, 941–948. [Google Scholar] [CrossRef] [PubMed]
- Boulet, L. Influence of comorbid conditions on asthma. Eur. Respir. J. 2009, 33, 897–906. [Google Scholar] [CrossRef] [PubMed]
- Dixon, A.E.; Kaminsky, D.A.; Holbrook, J.T.; Wise, R.A.; Shade, D.M.; Irvin, C.G. Allergic rhinitis and sinusitis in asthma: Differential effects on symptoms and pulmonary function. Chest 2006, 130, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, M.; Yoshida, K.; Adachi, Y.; Furukawa, M.; Itazawa, T.; Odajima, H.; Saito, H.; Akasawa, A. Factors associated with asthma control in children: Findings from a national Web-based survey. Pediatric Allergy Immunol. 2014, 25, 804–809. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Reference Group | |
|---|---|
| A | asthma only |
| Comorbidity Group | |
| AR | asthma AND (rhinitis OR sinusitis OR snoring) |
| AER | asthma AND (food allergy OR gastroesophageal reflux OR eczema OR urticaria OR angioedema OR anaphylaxis) |
| ARER | asthma AND (rhinitis OR sinusitis OR snoring) AND (food allergy OR gastroesophageal reflux OR eczema OR urticaria OR angioedema OR anaphylaxis) |
| Overall n = 508 (100%) | A n = 68 (13%) | AR n = 188 (37%) | AER n = 50 (10%) | ARER n = 202 (40%) | p-Value | |
|---|---|---|---|---|---|---|
| Host Factors | ||||||
| Female gender | 181 (36) | 17 (25) | 61 (32) | 26 (52) | 77 (38) | 0.014 |
| Age, years | 8.6 (2.8) | 8.1 (2.9) | 9.0 (2.8) | 8.3 (2.6) | 8.6 (2.8) | 0.064 |
| Body mass index, kg/m2 | 19.4 (4.3) 1 | 18.9 (4.5) | 20.0 (4.4) | 18.1 (4.1) | 19.4 (4.2) | 0.014 |
| Asthma duration, years | 3.8 (2.3) | 3.5 (1.9) | 3.7 (2.6) | 3.7 (1.5) | 4.0 (2.3) | 0.041 |
| Allergic sensitization | 0.036 | |||||
| Non-sensitized | 123 (24) | 25 (37) | 39 (21) | 11 (22) | 48 (24) | |
| Mono-sensitized | 143 (28) | 18 (26) | 50 (27) | 21 (42) | 54 (27) | |
| Poly-sensitized | 242 (48) | 25 (37) | 99 (53) | 18 (36) | 100 (50) | |
| Parent education ≥ eight years | 447 (88) | 57 (84) | 168 (89) | 42 (84) | 180 (89) | 0.485 |
| Maternal history of asthma | 107 (21) | 6 (9) | 42 (22) | 7 (14) | 52 (26) | 0.015 |
| Maternal history of allergies | 185 (36) | 17 (25) | 74 (39) | 15 (30) | 79 (39) | 0.109 |
| Cesarean delivery | 285 (56) | 38 (56) | 110 (59) | 32 (64) | 105 (52) | 0.376 |
| Preterm birth | 57 (11) | 7 (10) | 28 (15) | 3 (6) | 19 (9) | 0.200 |
| Breastfeeding ≥ three months | 331 (65) | 35 (51) | 119 (63) | 36 (72) | 141 (70) | 0.031 |
| Environmental Factors | ||||||
| Early pet exposure | 58 (11) | 3 (4) | 27 (14) | 4 (8) | 24 (12) | 0.137 |
| Current pet exposure | 104 (20) | 12 (18) | 46 (24) | 9 (18) | 37 (18) | 0.401 |
| Early mold exposure | 126 (25) | 10 (15) | 54 (29) | 8 (16) | 54 (27) | 0.052 |
| Current mold exposure | 102 (20) | 11 (16) | 35 (19) | 7 (14) | 49 (24) | 0.236 |
| ETS exposure during pregnancy | 199 (39) | 25 (37) | 76 (40) | 15 (30) | 83 (41) | 0.500 |
| Early ETS exposure | 189 (37) | 26 (38) | 71 (38) | 15 (30) | 77 (38) | 0.744 |
| Current ETS exposure | 210 (41) | 21 (31) | 85 (45) | 18 (36) | 86 (43) | 0.176 |
| Current traffic exposure | 151 (30) | 15 (22) | 59 (31) | 12 (24) | 65 (32) | 0.317 |
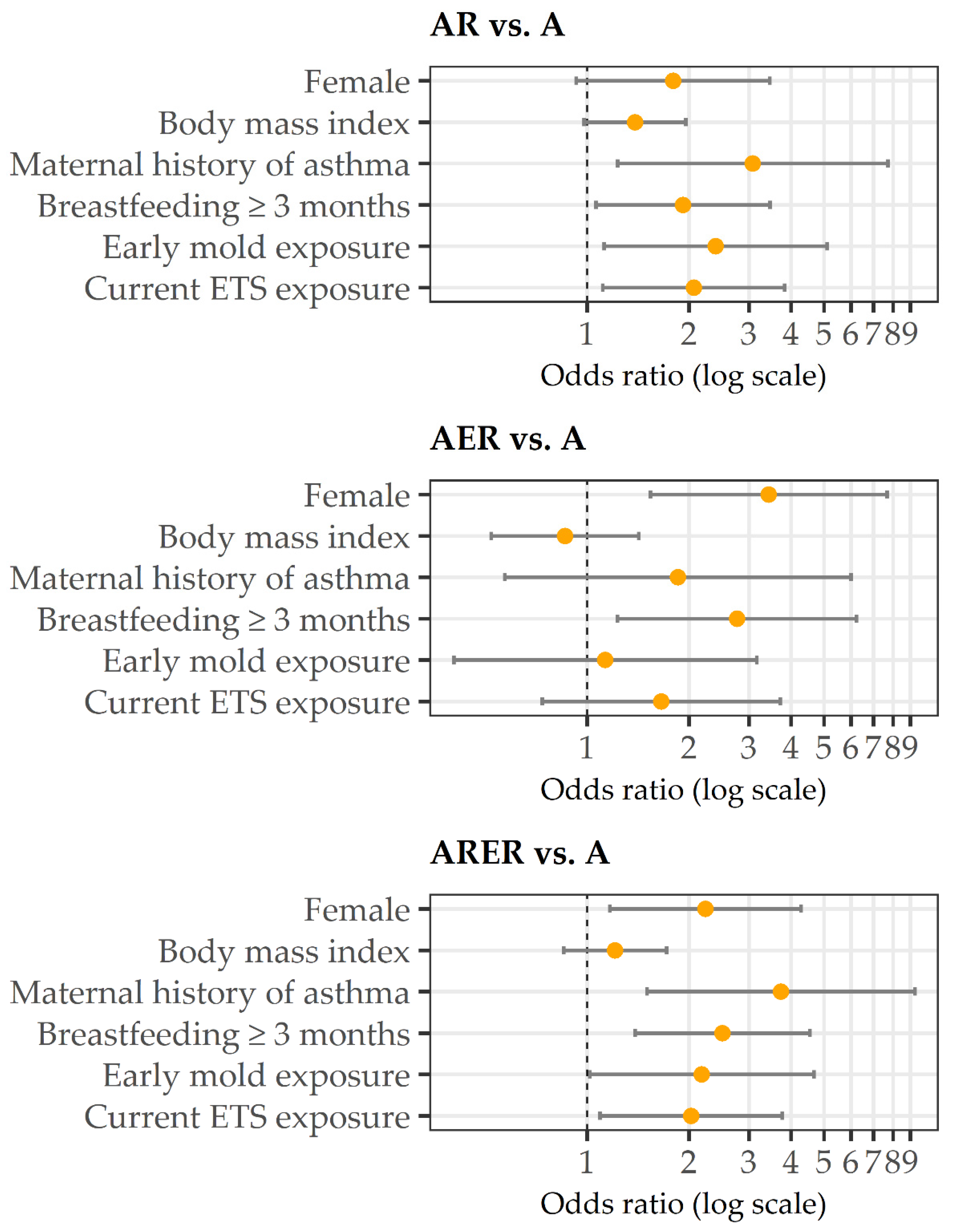
| AR vs. A | AER vs. A | ARER vs. A | ||||
|---|---|---|---|---|---|---|
| OR (p-Value) | 95% CI | OR (p-Value) | 95% CI | OR (p-Value) | 95% CI | |
| Female | 1.79 (0.083) | 0.93–3.46 | 3.43 (0.003) | 1.54–7.68 | 2.23 (0.015) | 1.17–4.28 |
| Body mass index (five-unit increase) | 1.38 (0.066) | 0.98–1.95 | 0.86 (0.558) | 0.52–1.42 | 1.21 (0.288) | 0.85–1.71 |
| Maternal history of asthma | 3.08 (0.016) | 1.23–7.72 | 1.85 (0.305) | 0.57–6.00 | 3.73 (0.005) | 1.50–9.27 |
| Breastfeeding ≥ three months | 1.92 (0.031) | 1.06–3.46 | 2.77 (0.014) | 1.23–6.22 | 2.50 (0.002) | 1.38–4.54 |
| Early mold exposure | 2.39 (0.024) | 1.12–5.11 | 1.13 (0.816) | 0.40–3.17 | 2.18 (0.045) | 1.02–4.66 |
| Current ETS exposure | 2.06 (0.022) | 1.11–3.83 | 1.65 (0.224) | 0.74–3.71 | 2.03 (0.025) | 1.09–3.76 |
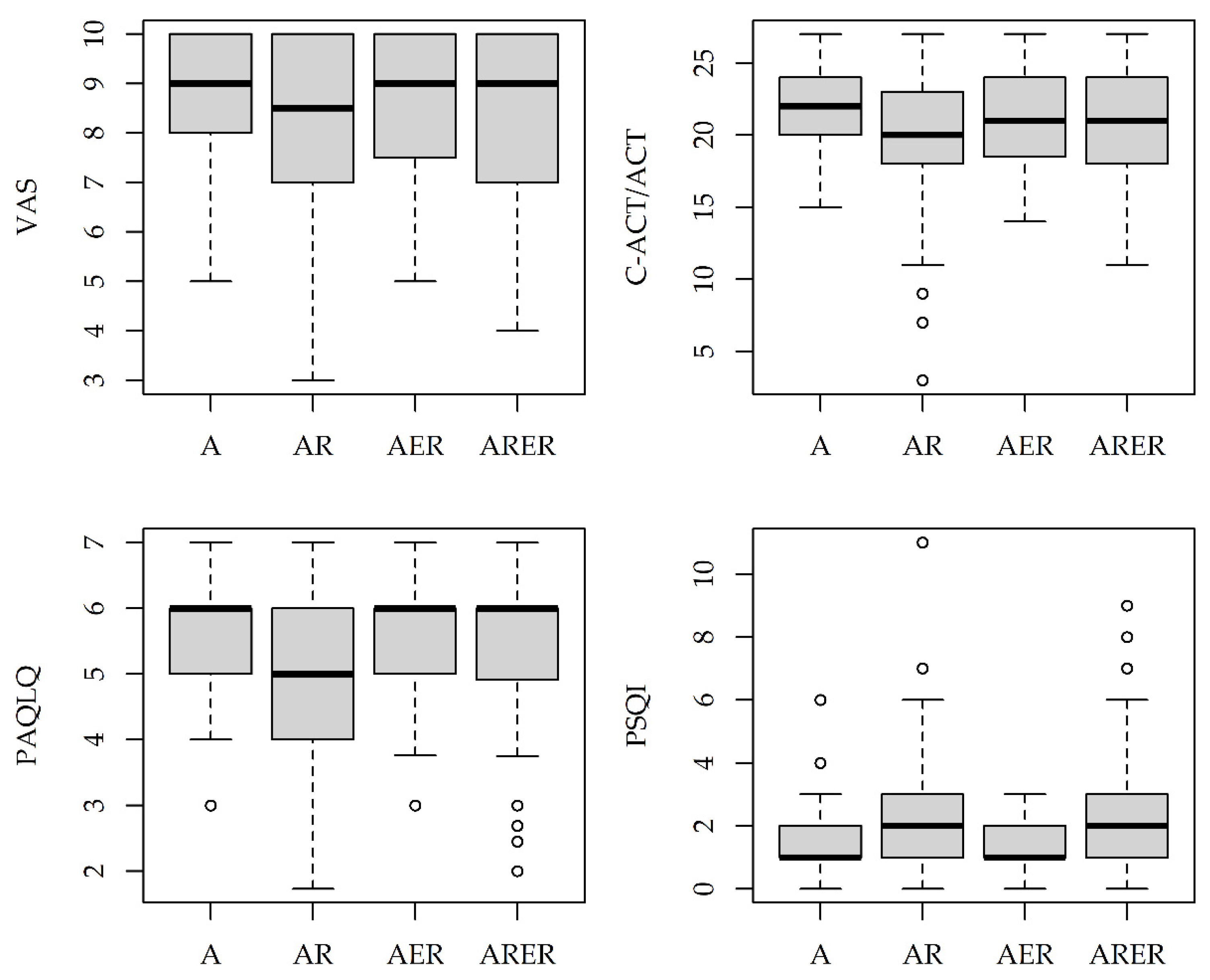
| Overall n = 508 (100%) | A n = 68 (13%) | AR n = 188 (37%) | AER n = 50 (10%) | ARER n = 202 (40%) | p-Value | |
|---|---|---|---|---|---|---|
| Asthma severity | 0.666 | |||||
| Intermittent | 246 (48) | 32 (47) | 93 (49) | 25 (50) | 96 (48) | |
| Mild persistent | 170 (33) | 27 (40) | 65 (35) | 15 (30) | 63 (31) | |
| Moderate/severe persistent | 92 (18) | 9 (13) | 30 (16) | 10 (20) | 43 (21) | |
| Asthma control | 0.220 | |||||
| Well controlled | 195 (38) | 34 (50) | 64 (34) | 21 (42) | 76 (38) | |
| Partly controlled | 107 (21) | 8 (12) | 46 (24) | 8 (16) | 45 (22) | |
| Uncontrolled | 206 (41) | 26 (38) | 78 (41) | 21 (42) | 81 (40) | |
| Exacerbations last 12 months | 2.6 (3.4) | 2.0 (3.2) | 3.0 (3.4) | 2.2 (3.4) | 2.6 (3.3) | 0.009 |
| FEV1 % predicted | 96.5 (13.2) | 95.9 (14.6) | 96.2 (12.0) | 93.8 (13.3) | 97.8 (13.7) | 0.193 |
| eNO, ppb | 13.2 (10.1) | 13.0 (8.9) | 14.9 (11.9) | 11.5 (7.4) | 12.2 (9.1) | 0.185 |
| C-ACT/ACT 1 | 20.6 (4.1) | 21.8 (2.7) | 19.7 (4.8) | 20.9 (3.7) | 20.8 (3.8) | 0.215 |
| PSQI 1 | 2.1 (1.9) | 1.5 (1.3) | 2.3 (1.8) | 1.4 (0.8) | 2.3 (2.2) | 0.034 |
| PAQLQ 1 | 5.3 (1.2) | 5.5 (1.0) | 5.2 (1.2) | 5.4 (1.1) | 5.4 (1.2) | 0.635 |
| VAS 1 | 8.3 (1.8) | 8.7 (1.5) | 8.1 (1.9) | 8.5 (1.8) | 8.2 (1.7) | 0.404 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fasola, S.; Ferrante, G.; Cilluffo, G.; Malizia, V.; Alfano, P.; Montalbano, L.; Cuttitta, G.; La Grutta, S. Asthma Comorbidities: Frequency, Risk Factors, and Associated Burden in Children and Adolescents. Children 2022, 9, 1001. https://0-doi-org.brum.beds.ac.uk/10.3390/children9071001
Fasola S, Ferrante G, Cilluffo G, Malizia V, Alfano P, Montalbano L, Cuttitta G, La Grutta S. Asthma Comorbidities: Frequency, Risk Factors, and Associated Burden in Children and Adolescents. Children. 2022; 9(7):1001. https://0-doi-org.brum.beds.ac.uk/10.3390/children9071001
Chicago/Turabian StyleFasola, Salvatore, Giuliana Ferrante, Giovanna Cilluffo, Velia Malizia, Pietro Alfano, Laura Montalbano, Giuseppina Cuttitta, and Stefania La Grutta. 2022. "Asthma Comorbidities: Frequency, Risk Factors, and Associated Burden in Children and Adolescents" Children 9, no. 7: 1001. https://0-doi-org.brum.beds.ac.uk/10.3390/children9071001