Mathematical Model Based on the Shape of Pulse Waves Measured at a Single Spot for the Non-Invasive Prediction of Blood Pressure


Abstract
:1. Introduction
2. Methods
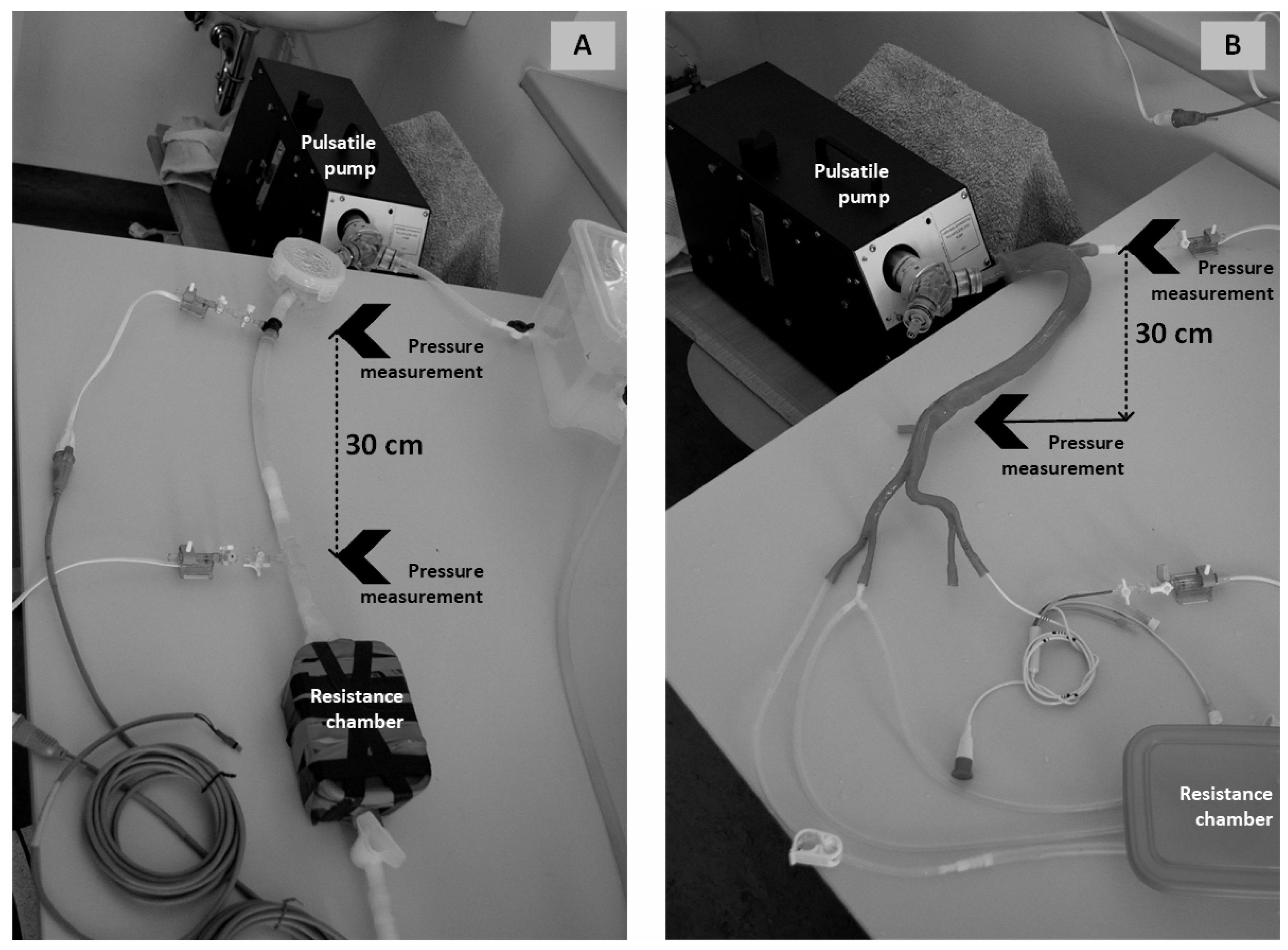
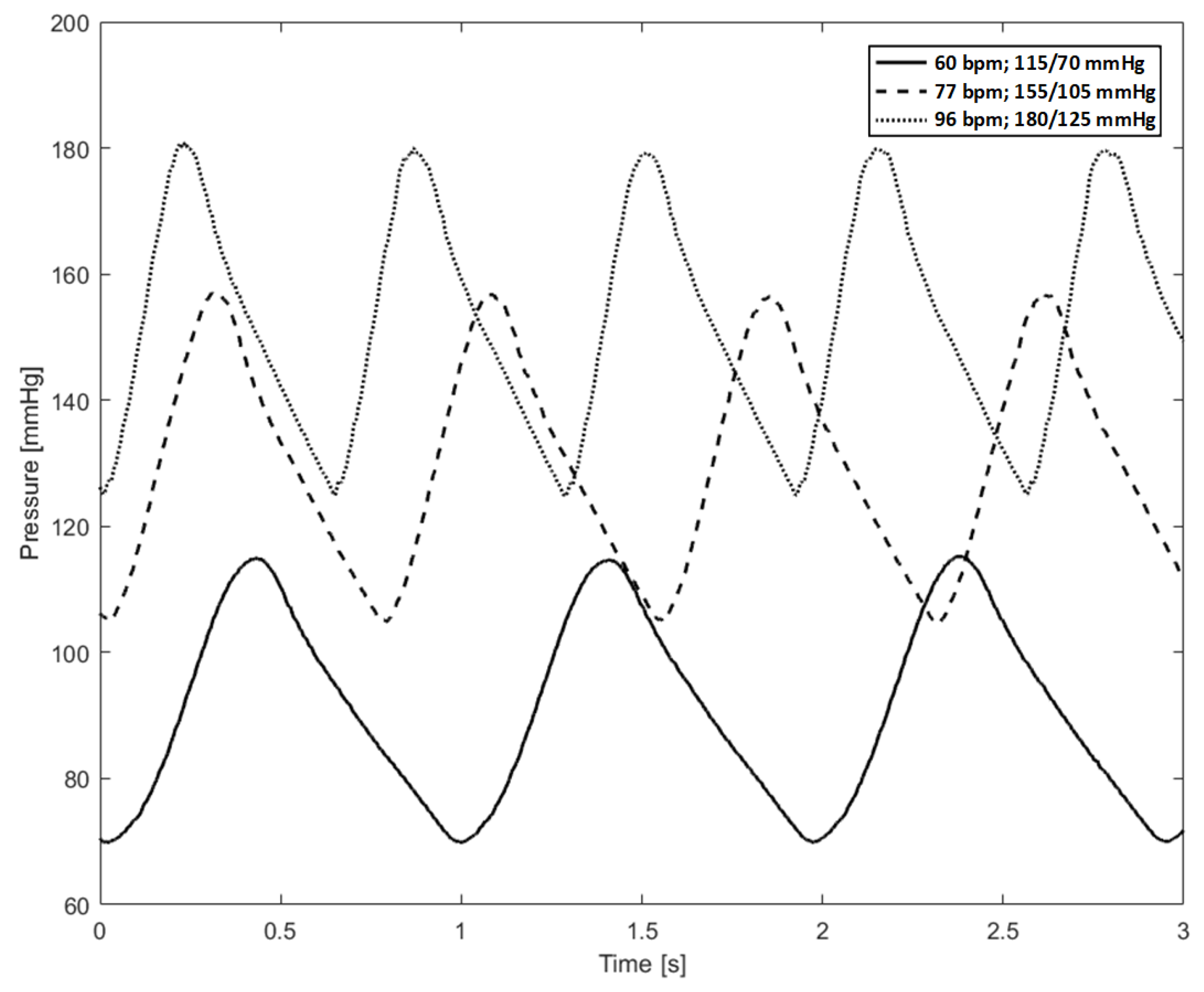
2.1. Experimental Model Setup
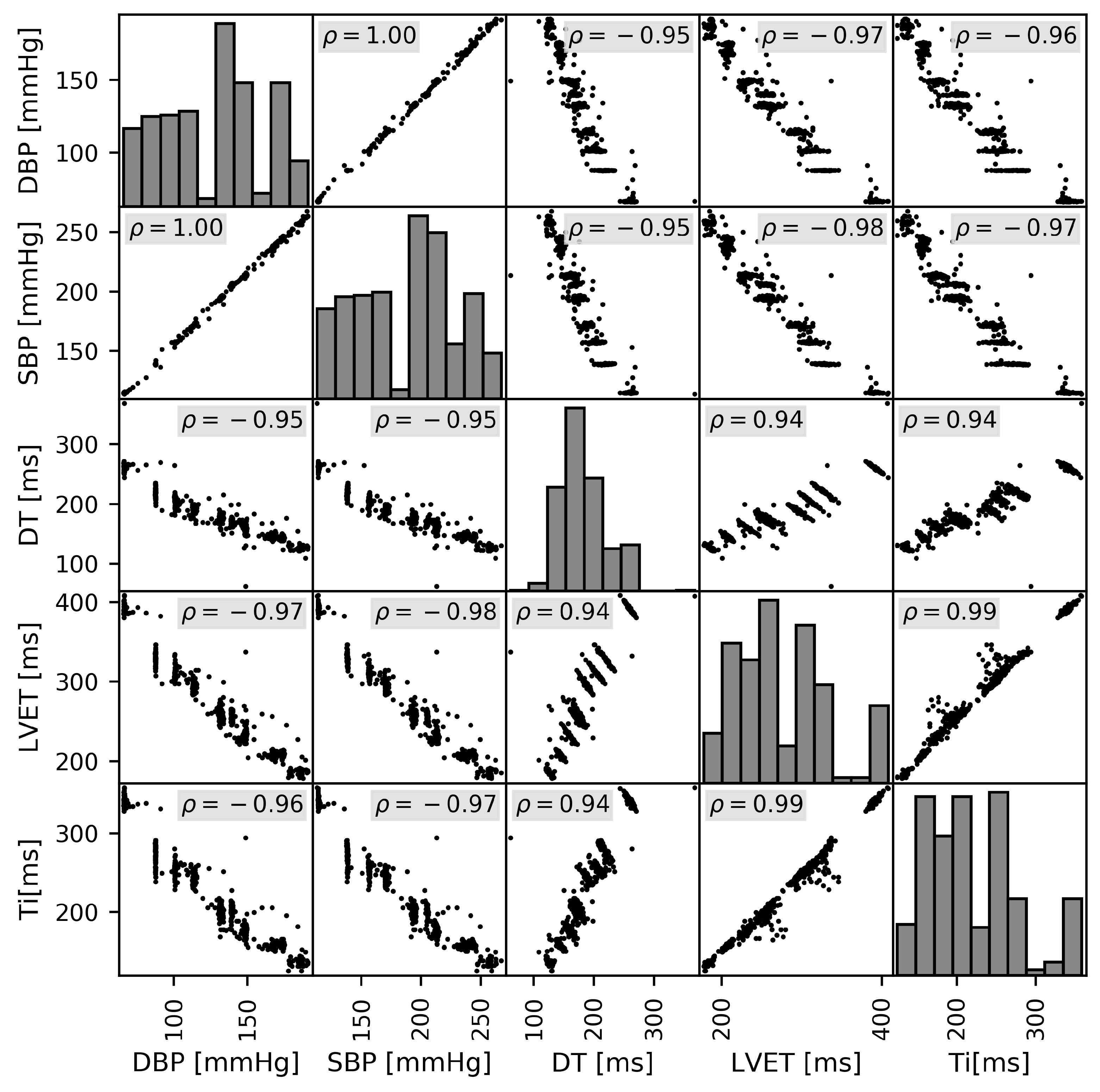
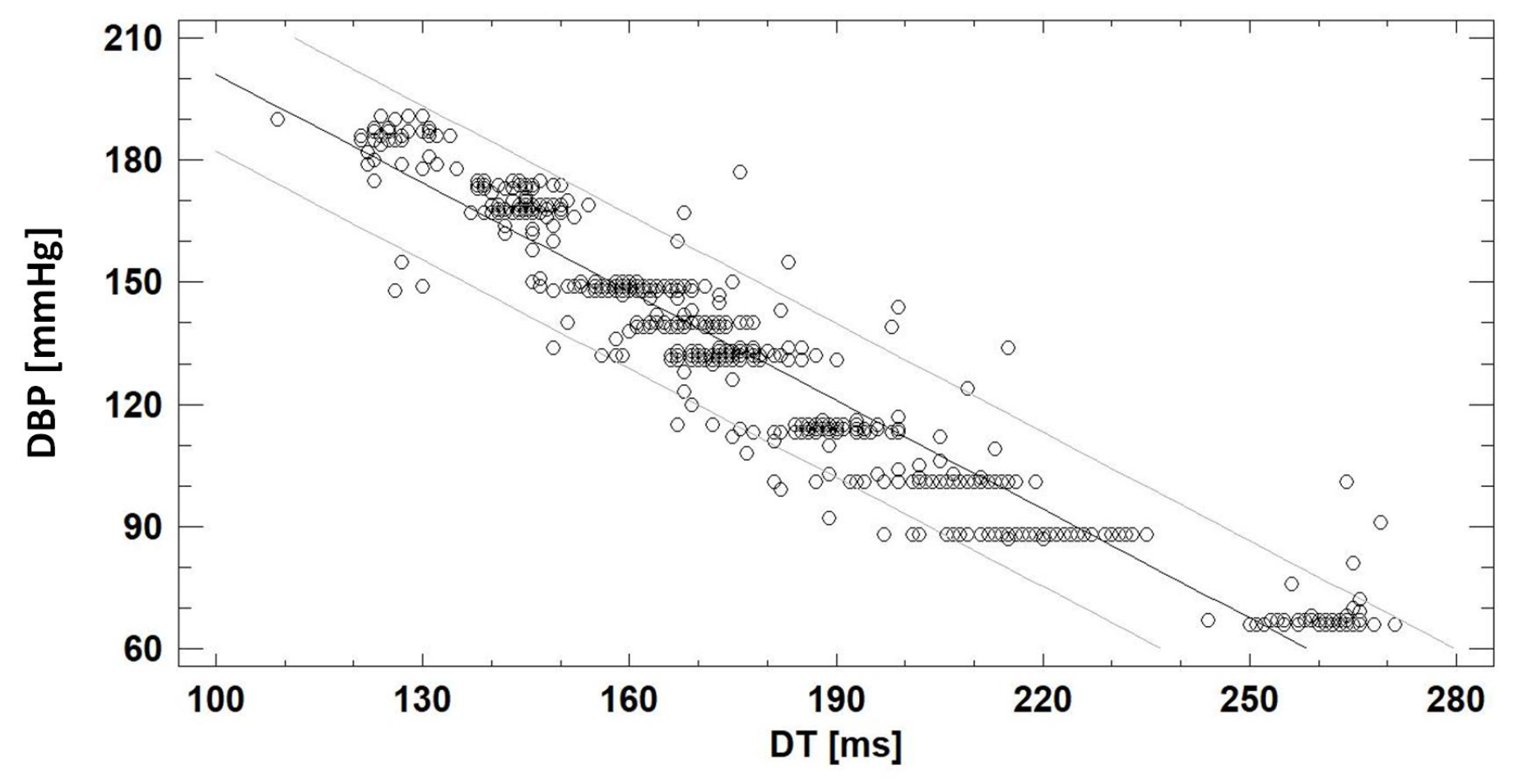
2.2. Correlation Analysis
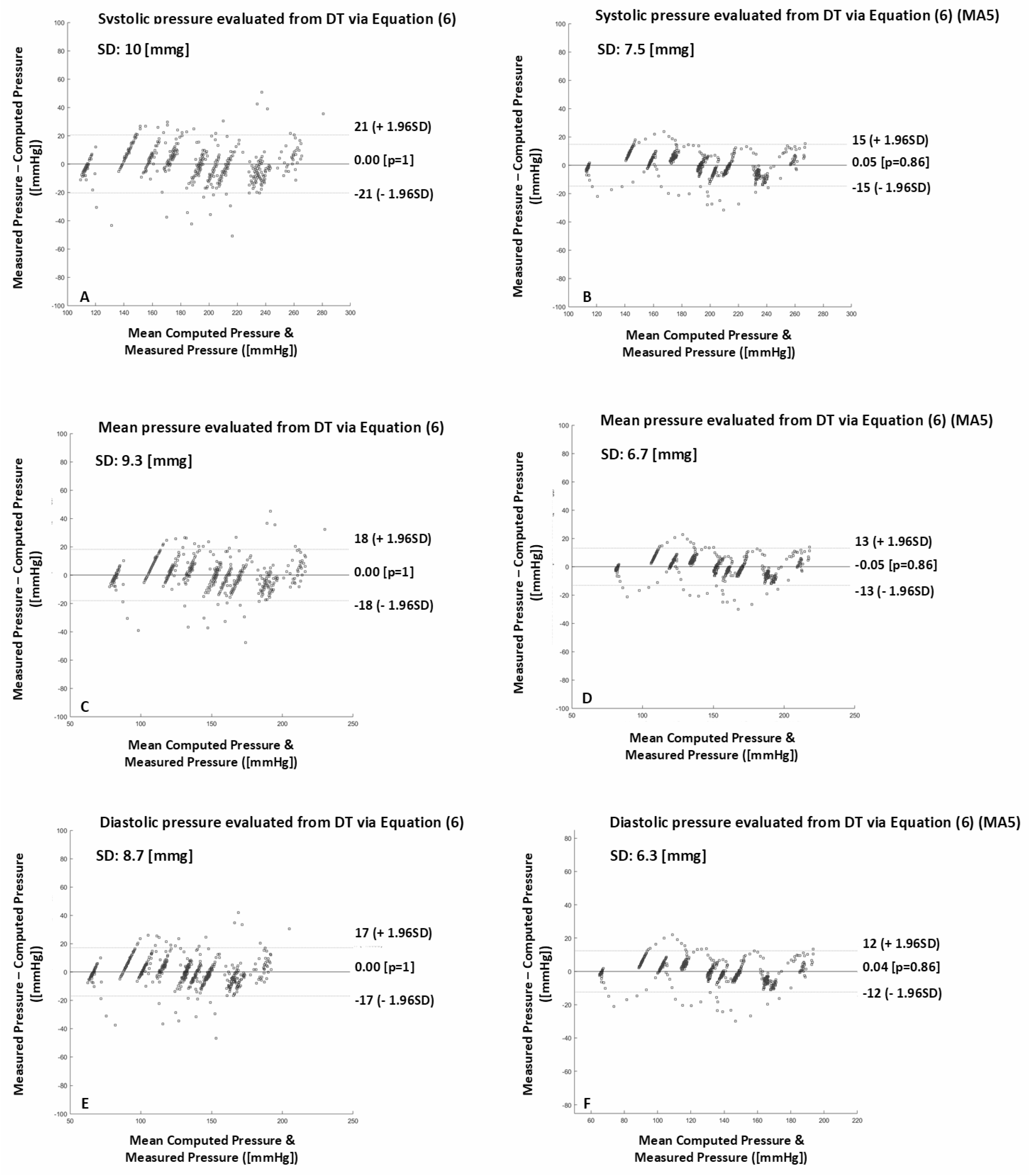
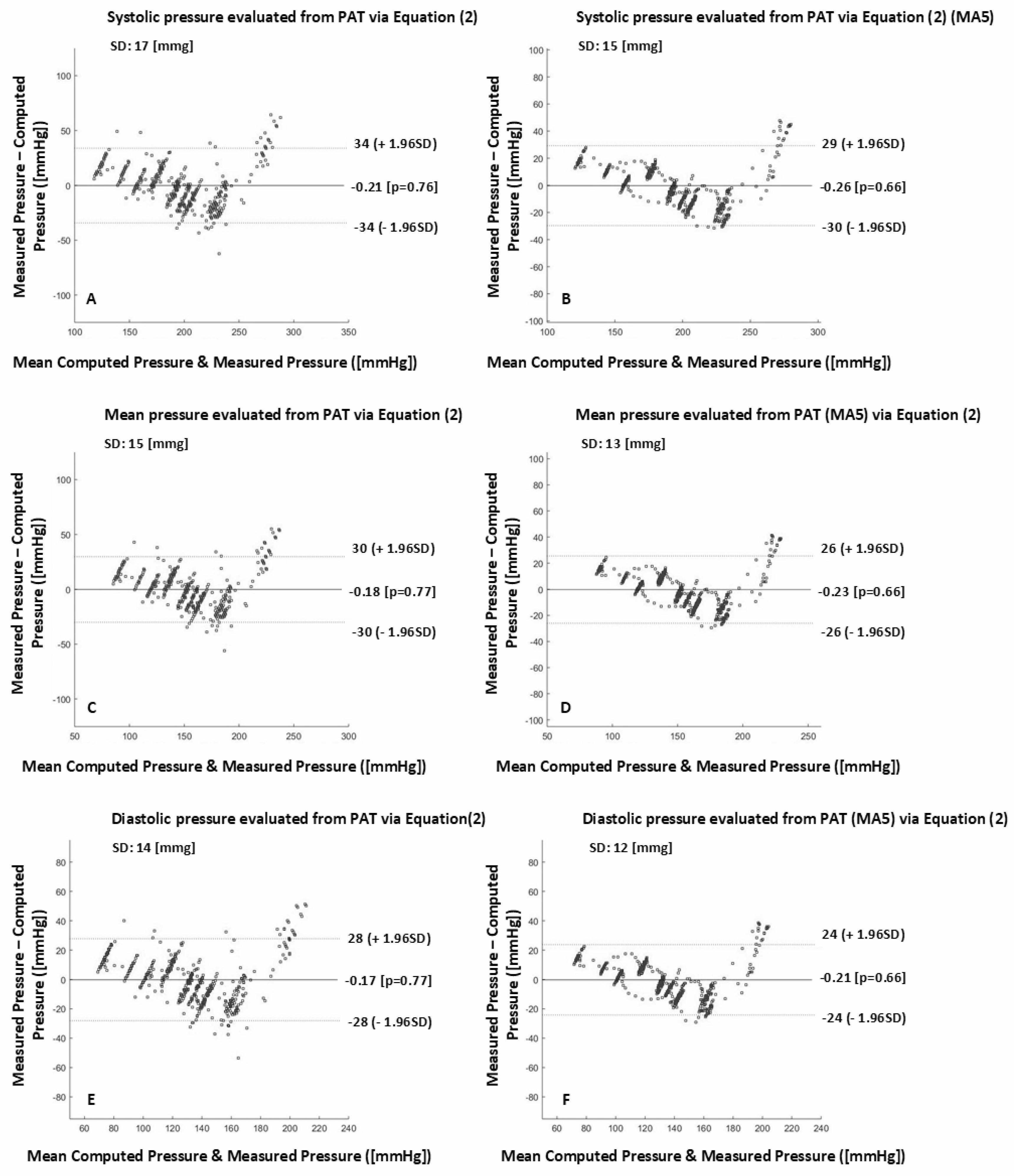
2.3. Validation Analysis
3. Results
3.1. Correlation Analysis
3.2. Validation Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| BP | Blood Pressure |
| DBP | Diastolic Blood Pressure |
| SBP | Systolic Blood Pressure |
| MAP | Mean Arterial Pressure |
| DT | Diastolic Time |
| LVET | left ventricular ejection time |
| PTT | Pulse Transit Time |
| PAT | Pulse Arrival Time |
References
- Wagner, J.Y.; Negulescu, I.; Schöfthaler, M.; Hapfelmeier, A.; Meidert, A.S.; Huber, W.; MSchmid, R.M.; Saugel, B. Continuous noninvasive arterial pressure measurement using the volume clamp method: An evaluation of the CNAP device in intensive care unit patients. J. Clin. Monit. Comput. 2015, 29, 807–813. [Google Scholar] [CrossRef] [PubMed]
- Berkelmans, G.F.N.; Kuipers, S.; Westerhof, B.E.; Spoelstra-de Man, A.M.E.; Smulders, Y.M. Comparing volume-clamp method and intra-arterial blood pressure measurements in patients with atrial fibrillation admitted to the intensive or medium care unit. J. Clin. Monit. Comput. 2018, 32, 439–446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacMahon, S.; Peto, R.; Collins, R.; Godwin, J.; Cutler, J.; Sorlie, P.; Stamler, J. Blood pressure, stroke, and coronary heart disease: Part 1, prolonged differences in blood pressure: Prospective observational studies corrected for the regression dilution bias. Lancet 1990, 335, 765–774. [Google Scholar] [CrossRef]
- Levy, D.; Larson, M.G.; Vasan, R.S.; Kannel, W.B.; Ho, K.K. The progression from hypertension to congestive heart failure. ACC Curr. J. Rev. 1997, 2, 37. [Google Scholar]
- Hirsch, A.T.; Criqui, M.H.; Treat-Jacobson, D.; Regensteiner, J.G.; Creager, M.A.; Olin, J.W. Peripheral arterial disease detection, awareness, and treatment in primary care. JAMA 2001, 286, 1317–1324. [Google Scholar] [CrossRef]
- Kario, K.; Ishikawa, J.; Pickering, T.G.; Hoshide, S.; Eguchi, K.; Morinari, M.; Hoshide, Y.; Kuroda, T.; Shimada, K. Morning hypertension: The strongest independent risk factor for stroke in elderly hypertensive patients. Hypertens. Res. 2006, 29, 581. [Google Scholar] [CrossRef] [Green Version]
- Rothwell, P.M.; Howard, S.C.; Dolan, E.; O’Brien, E.; Dobson, J.E.; Dahlöf, B.; Poulter, N.R.; Poulter, N.R. Prognostic significance of visit-to-visit variability, maximum systolic blood pressure, and episodic hypertension. Lancet 2010, 375, 895–905. [Google Scholar] [CrossRef]
- Kario, K.; Matsui, Y.; Shibasaki, S.; Eguchi, K.; Ishikawa, J.; Hoshide, S.; Shimada, K. An α-adrenergic blocker titrated by self-measured blood pressure recordings lowered blood pressure and microalbuminuria in patients with morning hypertension: The Japan Morning Surge-1 Study. J. Hypertens. 2008, 26, 1257–1265. [Google Scholar] [CrossRef]
- Hoshide, S.; Yano, Y.; Haimoto, H.; Yamagiwa, K.; Uchiba, K.; Nagasaka, S.; Ishikawa, J.; Matsui, Y.; Nakamura, A.; Fukutomi, M.; et al. Morning and evening home blood pressure and risks of incident stroke and coronary artery disease in the Japanese general practice population: The Japan Morning Surge-Home Blood Pressure Study. Hypertension 2016, 68, 54–61. [Google Scholar] [CrossRef] [Green Version]
- Clark, C.E.; Taylor, R.S.; Butcher, I.; Stewart, M.C.; Price, J.; Fowkes, F.G.R.; Campbell, J.L. Inter-arm blood pressure difference and mortality: A cohort study in an asymptomatic primary care population at elevated cardiovascular risk. Br. J. Gen. Pract. 2016, 66, e297–e308. [Google Scholar] [CrossRef]
- Peter, L.; Noury, N.; Cerny, M. A review of methods for non-invasive and continuous blood pressure monitoring: Pulse transit time method is promising? IRBM 2014, 35, 271–282. [Google Scholar] [CrossRef]
- CAROS, J.S.I.; Brunner, J.X.; Farrario, D.; Adler, A. Method and Apparatus for the Non-Invasive Measurement of Pulse Transit Times (PTT). U.S. Patent No 9,999,357, 19 June 2018. [Google Scholar]
- Geddes, L.A.; Voelz, M.H.; Babbs, C.F.; Bourl, J.D.; Tacker, W.A. Pulse transit time as an indicator of arterial blood pressure. Psychophysiology 1981, 18, 71–74. [Google Scholar] [CrossRef] [PubMed]
- Proença, J.; Muehlsteff, J.; Aubert, X.; Carvalho, P. Is pulse transit time a good indicator of blood pressure changes during short physical exercise in a young population? In Proceedings of the 2010 Annual International Conference of the IEEE Engineering in Medicine and Biology, Buenos Aires, Argentina, 31 August–4 September 2010; pp. 598–601. [Google Scholar]
- Sharma, M.; Barbosa, K.; Ho, V.; Griggs, D.; Ghirmai, T.; Krishnan, S.K.; Hsiai, T.K.; Chiao, J.-C.; Cao, H. Cuff-less and continuous blood pressure monitoring: A methodological review. Technologies 2017, 5, 21. [Google Scholar] [CrossRef] [Green Version]
- Chen, W.; Kobayashi, T.; Ichikawa, S.; Takeuchi, Y.; Togawa, T. Continuous estimation of systolic blood pressure using the pulse arrival time and intermittent calibration. Med Biol. Eng. Comput. 2000, 38, 569–574. [Google Scholar] [CrossRef]
- Baek, H.J.; Kim, K.K.; Kim, J.S.; Lee, B.; Park, K.S. Enhancing the estimation of blood pressure using pulse arrival time and two confounding factors. Physiol. Meas. 2009, 31, 145. [Google Scholar] [CrossRef]
- Proença, M.; Falhi, A.; Ferrario, D.; Grossenbacher, O.; Porchet, J.A.; Krauss, J.; Sola, J. Continuous non-occlusive blood pressure monitoring at the sternum. Biomed. Eng. Tech. 2012, 57, 2–5. [Google Scholar] [CrossRef]
- Ruiz-Rodríguez, J.C.; Ruiz-Sanmartín, A.; Ribas, V.; Caballero, J.; García-Roche, A.; Riera, J.; Nuvials, S.; de Nadal, M.; de Sola-Morales, O.; Serra, J.; et al. Innovative continuous non-invasive cuffless blood pressure monitoring based on photoplethysmography technology. Intensive Care Med. 2013, 39, 1618–1625. [Google Scholar] [CrossRef]
- Hughes, D.J.; Babbs, C.F.; Geddes, L.A.; Bourl, J.D. Measurements of Young’s modulus of elasticity of the canine aorta with ultrasound. Ultrasonic Imaging 1979, 1, 356–367. [Google Scholar] [CrossRef] [Green Version]
- Vlachopoulos, C.; O’Rourke, M.; Nichols, W.W. McDonald’s Blood Flow in Arteries: Theoretical, Experimental and Clinical Principles; CRC Press: Boca Raton, FL, USA, 2011. [Google Scholar]
- Peter, L.; Noury, N.; Cerny, M. Proposal of Physical Model of Cardiovascular System; Improvement of Mock Circulatory Loop. In World Congress on Medical Physics and Biomedical Engineering; Springer: Singapore, 2019; pp. 505–508. [Google Scholar]
- Vermeersch, S.J.; Rietzschel, E.R.; De Buyzere, M.L.; De Bacquer, D.; De Backer, G.; Van Bortel, L.M.; Gillebert, T.C.; Verdonck, P.R.; Segers, P. Determining carotid artery pressure from scaled diameter waveforms: Comparison and validation of calibration techniques in 2026 subjects. Physiol. Meas. 2008, 29, 1267. [Google Scholar] [CrossRef]
- Peter, L.; Noury, N.; Cerny, M.; Nykl, I. Comparison of methods for the evaluation of NIBP from pulse transit time. In Proceedings of the 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; pp. 4244–4247. [Google Scholar]
- Salvi, P. Pulse waves. In How Vascular Hemodynamics Affects Blood Pressure; Springer: Berlin, Germany, 2012. [Google Scholar]
- Van Bortel, L.M.; Balkestein, E.J.; van der Heijden-Spek, J.J.; Vanmolkot, F.H.; Staessen, J.A.; Kragten, J.A. Non-invasive assessment of local arterial pulse pressure: Comparison of applanation tonometry and echo-tracking. J. Hypertens. 2001, 19, 1037–1044. [Google Scholar] [CrossRef] [Green Version]
- Choi, Y.; Zhang, Q.; Ko, S. Noninvasive cuffless blood pressure estimation using pulse transit time and Hilbert-Huang transform. Comput. Electr. Eng. 2013, 39, 103–111. [Google Scholar] [CrossRef]
- Magder, S. Bench-to-bedside review: An approach to hemodynamic monitoring-Guyton at the bedside. Crit. Care 2012, 16, 236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sola, J.; Proença, M.; Ferrario, D.; Porchet, J.A.; Falhi, A.; Grossenbacher, O.; Allemann, Y.; Rimoldi, S.F.; Sartori, C. Noninvasive and nonocclusive blood pressure estimation via a chest sensor. IEEE Trans. Biomed. Eng. 2013, 60, 3505–3513. [Google Scholar] [CrossRef] [PubMed] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
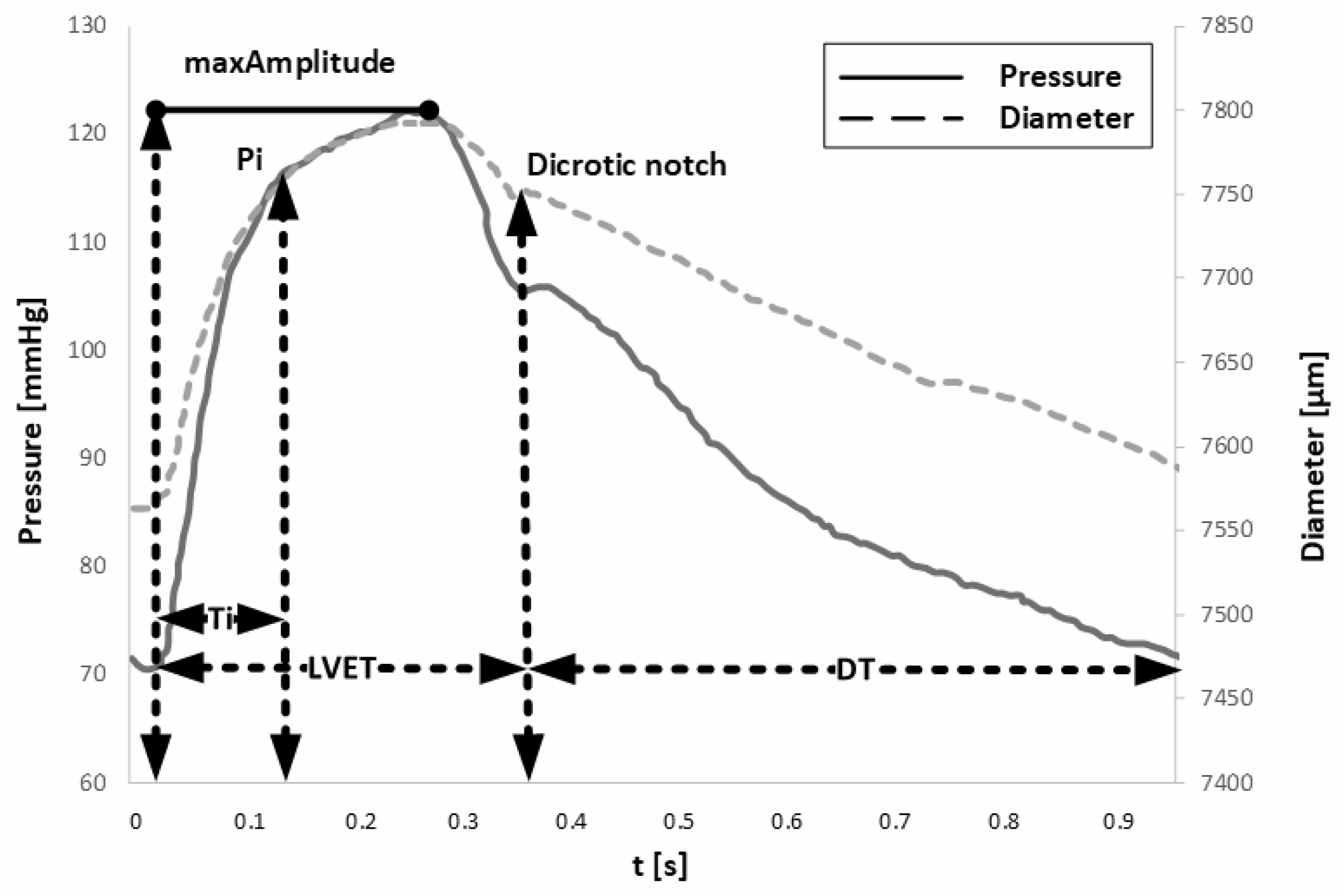
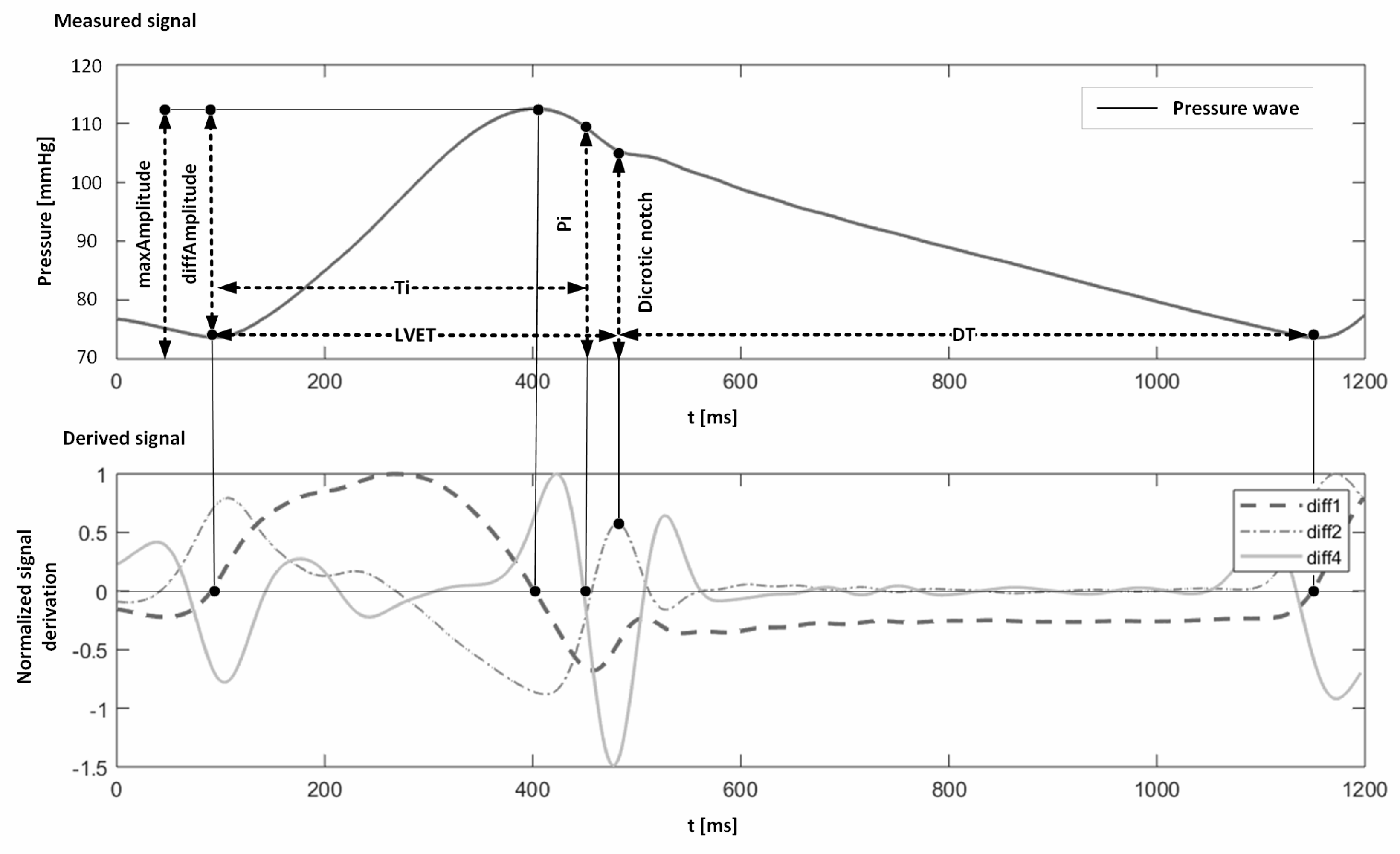
| Parameter | [Unit] | Definition |
|---|---|---|
| minAmplitude | [V] | The lowest amplitude of the signal recorded in the pulse wave |
| Pi | [V] | The amplitude of the pulse wave corresponding to the point where the backward wave starts superimposing onto the forward wave |
| maxAmplitude | [V] | The maximum amplitude of the signal in systole |
| LVET | [ms] | Duration of the systolic phase, left ventricular ejection time |
| Ti | [ms] | Travel time of the reflected wave, the time delay of the backward waveform |
| DT | [ms] | Diastolic time, the time of the diastolic phase, from the dicrotic notch to the end of diastole |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peter, L.; Kracik, J.; Cerny, M.; Noury, N.; Polzer, S. Mathematical Model Based on the Shape of Pulse Waves Measured at a Single Spot for the Non-Invasive Prediction of Blood Pressure. Processes 2020, 8, 442. https://0-doi-org.brum.beds.ac.uk/10.3390/pr8040442
Peter L, Kracik J, Cerny M, Noury N, Polzer S. Mathematical Model Based on the Shape of Pulse Waves Measured at a Single Spot for the Non-Invasive Prediction of Blood Pressure. Processes. 2020; 8(4):442. https://0-doi-org.brum.beds.ac.uk/10.3390/pr8040442
Chicago/Turabian StylePeter, Lukas, Jan Kracik, Martin Cerny, Norbert Noury, and Stanislav Polzer. 2020. "Mathematical Model Based on the Shape of Pulse Waves Measured at a Single Spot for the Non-Invasive Prediction of Blood Pressure" Processes 8, no. 4: 442. https://0-doi-org.brum.beds.ac.uk/10.3390/pr8040442