
Bladder Substitution: The Role of Tissue Engineering and Biomaterials



1
Department of Surgery, Oncology and Gastroenterology, Giustiniani 2, 35128 Padua, Italy
2
L.i.f.e.L.a.b. Program, WP 14, Consorzio per la Ricerca Sanitaria (CORIS), Veneto Region, Via N. Giustiniani 2, 35128 Padua, Italy
*
Author to whom correspondence should be addressed.
Processes 2021, 9(9), 1643; https://0-doi-org.brum.beds.ac.uk/10.3390/pr9091643
Submission received: 10 August 2021
/
Revised: 6 September 2021
/
Accepted: 8 September 2021
/
Published: 13 September 2021
(This article belongs to the Section Biological Processes and Systems)
{kind=link}
Abstract
:Tissue engineering could play a major role in the setting of urinary diversion. Several conditions cause the functional or anatomic loss of urinary bladder, requiring reconstructive procedures on the urinary tract. Three main approaches are possible: (i) incontinent cutaneous diversion, such as ureterocutaneostomy, colonic or ileal conduit, (ii) continent pouch created using different segments of the gastrointestinal system and a cutaneous stoma, and (iii) orthotopic urinary diversion with an intestinal segment with spherical configuration and anastomosis to the urethra (neobladder, orthotopic bladder substitution). However, urinary diversions are associated with numerous complications, such as mucus production, electrolyte imbalances and increased malignant transformation potential. In this context, tissue engineering would have the fundamental role of creating a suitable material for urinary diversion, avoiding the use of bowel segments, and reducing complications. Materials used for the purpose of urinary substitution are biological in case of acellular tissue matrices and naturally derived materials, or artificial in case of synthetic polymers. However, only limited success has been achieved so far. The aim of this review is to present the ideal properties of a urinary tissue engineered scaffold and to examine the results achieved so far. The most promising studies have been highlighted in order to guide the choice of scaffolds and cells type for further evolutions.
1. Introduction: Clinical Context
Urinary bladder can lose its functional ability to store and empty effectively due to numerous conditions such as infection, cancer, trauma, inflammation or iatrogenic injury. Congenital or neurological disorders such as a spinal cord injury and spina bifida, can lead to a progressive bladder functionality loss with a concomitant urinary incontinence or renal impairment.
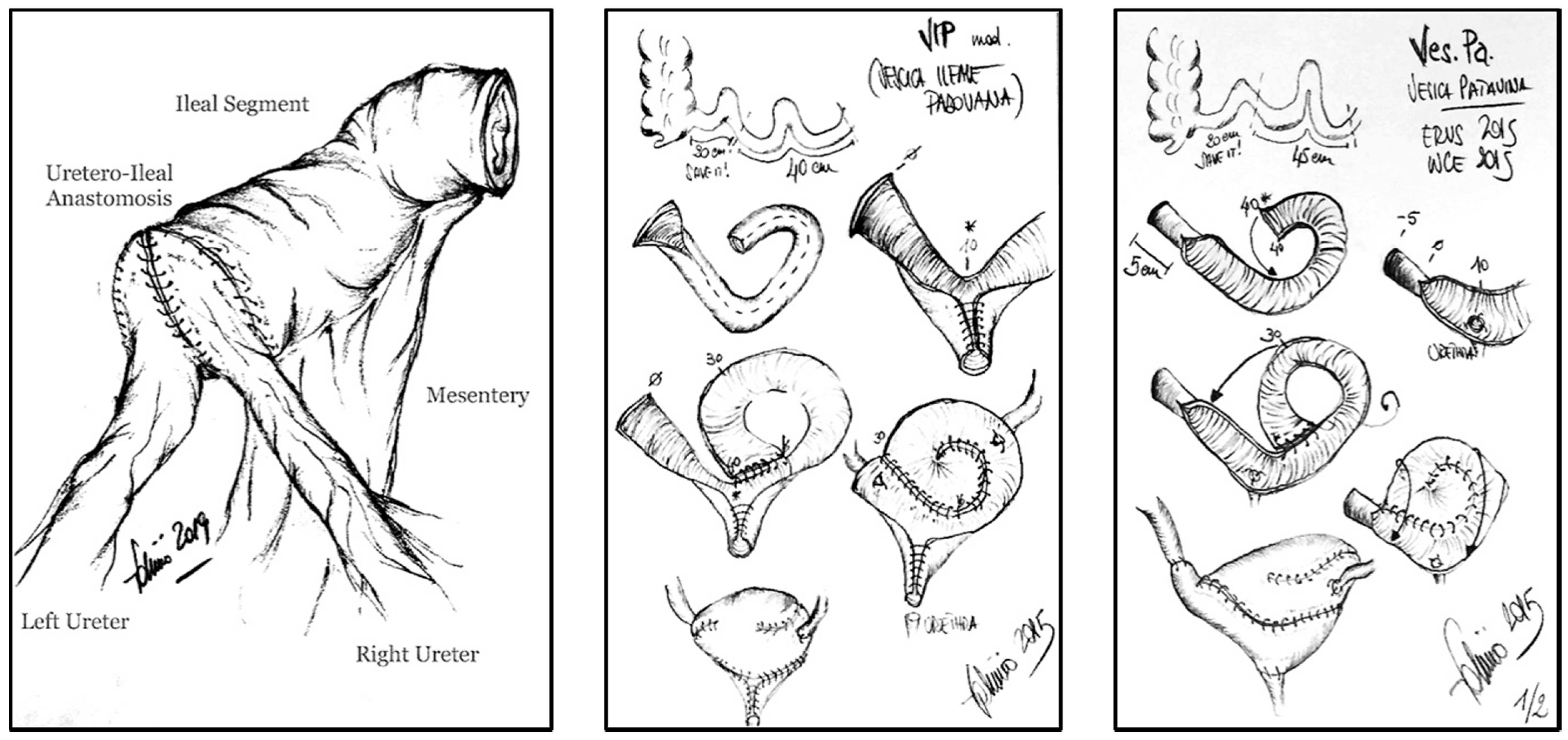
On the other hand, bladder cancer is one of the most frequent causes for bladder removal through radical cystectomy, the gold standard treatment for localized muscle-invasive bladder cancer, when conservative treatments such as chemo- and radiotherapies are not effective. In the European Union, the incidence of bladder cancer is in the sixth place and the age-standardized incidence rate of bladder cancer is 19.1 for men and 4.0 for women [1,2]. Unluckily, radical cystectomy is one of the more morbid urologic operations, with 80% of complications [3]. In men, this procedure involves the removal of the prostate, seminal vesicles, distal ureters and regional lymph nodes, while in women, the entire urethra and adjacent vagina, uterus, distal ureters and regional lymph nodes are excised. After radical cystectomy, three kind of urinary diversions are possible: (i) abdominal diversion, such as ureterocutaneostomy, colonic or ileal conduit, (ii) various forms of a continent pouch created using different segments of the gastrointestinal system and a cutaneous stoma, and (iii) orthotopic urinary diversion using an intestinal segment with reconfiguration and anastomosis to the ureters and urethra (neobladder, orthotopic bladder substitution) (Figure 1) [1].
Urinary diversions are associated with numerous complications, such as mucus production, electrolyte imbalances and increased malignant transformation potential. Mortality is reported as 1.2–3.2% at 30 days after surgery, and 2.3–8.0% after 90 days, while early complications occur in 58% of patients within 3 months after surgery and morbidity is linked to the type of urinary diversion. Diurnal (8–10%) and nocturnal (20–30%) incontinence, ureterointestinal stenosis (3–18%), metabolic disorders and vitamin B12 deficiency are reported [1,2].
The most conservative treatments typically do not produce a significant response in severe cases of bladder failure, seriously affecting the patient’s quality of life. In this case, an enterocystoplasty is performed. This procedure consists of a surgical bladder enlargement using intestinal tissue in order to increase its capacity and compliance, with a consequent improvement of incontinence and reduction of intravesical storage pressure with the aim of protecting the upper urinary tract. However, this surgical procedure fails in the restoration of the emptying function and may be cause of numerous complications especially related to the gastrointestinal tract, including persistent nausea, a need for nasogastric tube placement, partial or complete ileus/small intestinal obstructions, peritonitis, stenosis, gastrointestinal bleeding, a need for total parenteral nutrition, diarrhea and infections [3,4].
2. Tissue Engineering in Urology
Tissue engineering consists in a multidisciplinary approach with the aim of solving the problem of tissues and organs substitution or restoration in case of traditional transplants, circumventing the issues of biocompatibility and low availability of tissue and organs. The advantage of tissue engineering consists in the possibility to choose between biological and/or artificial materials substitutes, which may become practical solution for future tissue and organ regeneration.
In the urologic context, tissue engineering may allow the future fabrication of man-made constructs with the purpose of sparing the autologous gastro-intestinal tract which is currently used for urinary diversions, while preventing invasive surgery and potential complications [5].
Depending on the tissue type and the function needed, scaffolds need to have specific characteristics. In case of ureteral conduits, the ideal material should be easily accessible, impermeable to urine, non-immunogenic, amenable to remodeling and should possess appropriate conditions for cell growth and migration [6,7]. The major hindrances with regards to ureter regeneration are inappropriate blood supply, necrosis and urine toxicity. The main consequence for patients is obstruction of the urine passage that can cause severe complications, frequently associated with renal damage, leading to the patient’s debility, need of nephrectomy and even death. In case of urine leakage, inflammation of surrounding tissues ensues, leading to tissue fibrosis that causes ureter stenosis inhibiting urine transport to the bladder with subsequent renal damage [7]. With urine leakage from the kidney, ureter, bladder or urethra, there is the possibility of urinoma formation, which further enhances fibrosis, and a subsequent compression of the retroperitoneal structures, including ureters, impeding peristaltic wave formation. This may result in urine transport disorder even when the ureter is not damaged and its lumen is patent [6,7]. Several types of materials have been tested for ureter regeneration purposes ranging from synthetic polymers to natural and hybrid materials, but not all types of tested materials were suitable in terms of inadequate mechanical properties. Proper flexibility is needed for ureter regeneration, but also the formation of epithelium and muscular layer layers are required for this application. The epithelium has the aim to protect scaffold from the toxic urine environment, while the muscular layer provides correct peristaltic activity, causing physiologic urine transport. In case of proper muscle regeneration, an adequate blood supply to the regenerated tissue can be provided, but in case of improper fibrotic tissue formation, poor blood supply would be present, preventing the proper function of the graft [7].
When urinary bladder substitution is concerned, the scaffold should support a function of adequate dynamic mechanical and chemical resistance during filling and emptying phases. Engineered bladders have to support urine storage keeping contractile properties to allow physiologic voiding and need to reconstruct a compliant muscular wall with a highly specialized urothelium [1]. In fact, the main functions of the urinary bladder consist in storing large volumes of urine at low pressures to enable controlled micturition and to maintain a proper chemical gradient between urine and blood. For these reasons, to replicate this organ, special attention needs to be put towards biomechanical features. Both biological matrices derived from donor tissues (e.g., bladder acellular matrix (BAM) and small intestinal submucosa (SIS)) and different polymers have been tested in order to reconstruct urinary bladder. Moreover, scaffolds have been implanted either unseeded or seeded in order to promote tissue integration and mimic the histological, biomechanical and physiological features of native bladder wall [6,8]. In case of urinary bladder, it is needed an appropriate formation of smooth muscle layer and urothelium, including innervation and vascularization, in order to achieve the proper biomechanical and functional properties [8].
3. Tissue Engineered Urinary Scaffolds
The major aim of tissue engineering is to use biomaterials that can replicate the biological and mechanical functions of the extracellular matrix (ECM) found in the body. An artificial ECM forms a tri-dimensional (3D) surface, which provides structural integrity and a provisional support for cells to regenerate the tissue.
In the current state of the art, the major efforts to produce a tissue engineered urinary substitute are concentrated on the development of acellular or seeded scaffolds. An ideal scaffold should allow adequate cell proliferation and organization through appropriate vascularization and regulation of growth factors release and immune response. However, the main issue consists in the need to have a sufficient scaffold porosity to promote cell ingrowth, without compromising mechanical strength and barrier function against urine, which is toxic for surrounding tissues. Therefore, it is critical to directly control cell positioning and function within the scaffold, as cells need anchorage points without which they cannot survive and regenerate the tissue [9,10].
Materials used for the purpose of urinary substitution belong mainly to two categories: biological materials divided into acellular tissue matrices (e.g., SIS [11,12,13,14] and decellularized bladder matrix [15,16]) both allogeneic and xenogeneic, and naturally derived materials (e.g., collagen [17,18,19,20], hyaluronic acid, silk [21,22] and alginate [23]), as well as artificial materials which include synthetic polymers (e.g., polyglycolic acid, polylactic acid and polylactic-glycolic acid [24,25,26,27,28]).
Both types of materials show advantages and disadvantages which should be considered based on the specific application.
3.1. Acellular Tissue Matrices
Acellular tissue matrices are obtained through a decellularization process whose aim is the cellular removal while maintaining of natural histological microstructure of the original tissue. The final scaffold is rich in extracellular matrix proteins such as collagen, elastin and laminin in addition to growth factors, that give a three-dimensional structural support for cell growth and organization while enhancing cellular migration and differentiation. Such acellular matrices slowly degrade after implantation being subsequently replaced and remodeled through the deposition of novel ECM synthesized by cells. However, the main limitation of these materials resides in their variable mechanical properties, depending on the used decellularization and sterilization protocol, and the ability to completely remove remnant DNA fragments from the matrix, which could otherwise trigger an inflammatory reaction against the scaffold.
In many cases, decellularized tissues are preferred to enhance tissue regeneration after implantation for the aforementioned reasons, but there are some important issues to take in consideration.
Firstly, decellularization methods must be effective in the removal of cells and DNA fragments in order to prevent immune rejection in vivo, but the original morphology must not be negatively affecting in order to foster tissue regeneration. Many methodological approaches have been investigated, starting from different agents (chemicals such as acid/bases, detergents, alcohols and other solvents, biologicals, such as enzymes and non-enzymatic agents, physical and miscellaneous agents such as temperature, force/pressure and non-thermal irreversible electroporation), techniques to apply the agents (perfusion, pressure gradient, supercritical fluids, immersion and agitation) and sterilization protocols (incubation in acids or solvents, ethylene oxide exposure, gamma radiation and electron beam irradiation) [29]. Each method presents advantages and disadvantages in the preservation of tissue composition or morphology and in the removal of residual cellular material (e.g., acids and bases disrupt nucleic acids, but may denature proteins; hypotonic and hypertonic solutions effectively lyse cells, but do not effectively remove cellular residues; freezing and thawing can cause ice formation that disrupt ECM), therefore they must be investigated for the specific application. In fact, the optimal application of decellularization agents depends on tissue features, including thickness and density, the agents used and the clinical application. Before proceeding with tissue decellularization, undesirable excess of tissue may be removed in order to facilitate tissue decellularization which has to guarantee the retention of main ECM components. For example, for thin tissues like urinary bladder, intestine, pericardium and amnion, the most commonly used decellularization techniques are freezing and thawing, mechanical removal of undesirable layers and brief exposure to easily-removed detergents or acids, while, on the contrary, in case of thicker tissues like dermis, more extensive biochemical exposure and longer rinse times are needed. For these reasons, the complexity and the durations of the decellularization process depends on the degree of geometric and biologic conservation desired [29].
However, decellularization techniques in some cases cannot completely remove cellular material and it is still possible to detect cell components, such as dsDNA, mitochondria or membrane-associated molecules such as phospholipids. Crapo et al. proposed the minimal criteria that every decellularization protocol must guarantee: <50 ng dsDNA per mg ECM (dry weight), <200 bp DNA fragment length and lack of visible nuclear material in tissue sections stained with DAPI or H&E [29].
Xenogeneic DNA residues within decellularized scaffold materials often cause inflammatory reactions following implantation [30]. Only the most rigorous decellularization methods can ensure the complete removal of all cells and cell products in dense tissues. DNA residues are typically small fragments: the smaller the residue length, the lower the possibility to enhance an inflammatory response after transplantation (DNA fragments of less than 200 bp in length are not of concern) [31]. DNA residues are subjected to degradation fate via enzymatic breakdown.
Moreover, following organ xenotransplantation, hyperacute rejection can be caused by not completely removed cell membrane antigens such as α-Gal epitope since it is found in high density in most species, except for humans and Old World monkeys. These primates do not express the α-Gal epitope and produce large amounts of anti-Gal antibodies, including IgG, IgM and IgA, caused by the constant exposure to intestinal bacteria that carry the Gal epitope. Treatment of xenogeneic tissues with galactosidase can minimize potential adverse responses to the graft materials [32]. The length of time that a host is exposed to foreign antigens affects the type of immune response that will be elicited. When not chemically cross-linked, biological scaffold materials are rapidly degraded and any pro-inflammatory remnant is degraded as well [33]. Furthermore, degradation of ECM scaffold contributes to the overall remodeling process since chemo-attraction by degradation products contributes to the recruitment of host cells and to site-specific tissue remodeling [32].
Several acellular tissues have been used to create tissue engineered urinary substitutes. In case of urinary diversions, SIS has been used in a rat model, either unseeded and seeded with 3T3 fibroblasts [11]. All animals survived the observation period, though an inflammatory reaction was seen within the peritoneal cavity in both groups. Patent conduits were observed in half the animals at the end of the follow-up (two cell-seeded and one acellular conduit were completely occluded after 2 and 4 weeks) and no differences in cell layer regeneration were observed between the two groups. The acellular matrices induced less severe inflammatory responses and after one month, neovascularization could be observed. A multi-layered epithelium covered the conduit lumen near the distal anastomosis of the acellular conduit, and small islet-forming epithelial layer was observed after one month.
In rabbit model, a tissue engineered bladder acellular matrix (BAM) tubular graft has been used for urinary diversion after radical cystectomy [16,34]. The seeded scaffolds with urothelial cells (UCs, n = 24) resulted in coverage of conduit lumen with a multi-layered urothelium, less fibrosis and obstruction, demonstrating that pre-seeding with UCs re-established a blood-urine barrier, which allowed successful regeneration to occur in the absence of toxic metabolites present in urine. All the animals of the seeded group survived, and no severe complications were observed. In the unseeded group, four animals died one month before the end of the follow-up and the two remaining animals had fistulas and lack of urothelium regeneration.
Recently, a novel biomaterial has been investigated in order to find an alternative to commonly used materials to obtain a flexible, patent and impermeable urinary conduit. The marine biomaterial has been obtained by the decellularization of a squid mantle which has been chosen for its polarized structure and natural external polysaccharide layer that has been shown to protect urothelial and smooth muscle cells derived from porcine urinary bladder from urine [35].
On the other hand, in case of urethral replacement, several acellular scaffolds have been tested. Acellular dermis has been used for urethral reconstruction, seeded in vitro with human oral fibroblasts and oral keratinocytes, showing positive mechanical and biological properties. In fact, histologically scaffolds closely resembled native tissue and the MTT assay showed a good keratinocytes migration. Serial histologies showed a gradual remodeling by the fibroblasts from day 1 to day 14. For these reasons, it was reported the suitability of the tested cultured scaffolds for clinical use in substitution urethroplasty [36].
Acellular bladder collagen matrix has been used for the correction of 1.5 cm defect in the penile urethra mucosa in a rabbit model. At 6 months after implantation of the grafts, none of the treated animals developed strictures and fistulae. Analysis revealed a traditional epidermal arrangement rather than a transitional cell epithelium and a demarcated margin between the graft and the host tissue was clearly visible, suggesting incomplete integration of the graft within the original urethra [37].
Similar results in urethral reconstruction have been obtained using autologous oral keratinocytes seeded BAM grafts to replace a segment previously injured with a ventral defect [38]. At 6 months after implantation, none of the animals developed complications and structures, and the margins of the graft were not identifiable macroscopically. Microscopically, a stratified squamous epithelium like the native oral mucosa was found rather than an urothelium-like transitional epithelium, a clear demarcation margin between the graft and the urethral tissue and no inflammation, suggesting an incomplete integration of the graft into the native tissue.
Another group performed tubularized urethral replacement in rabbit model with unseeded matrices of various lengths. Acellular tubular patches could promote normal tissue regeneration only for short defects (0.5 cm), whereas for longer defects (1, 2 and 3 cm) the analysis revealed fibrosis and stenosis. Based on these results, they concluded that seeded patches are needed to successfully correct circumferential urethral defects longer than 5 mm [39].
Urethral reconstruction was also performed with a 3D porous scaffold derived from porcine decellularized bladder submucosa seeded with human bladder cells. In 3D dynamic culture, cells formed multiple layers on the surface of matrix. Cells also penetrated deeper into the lamina propria of the matrix compared to untreated matrix. Immunocytochemical staining indicated that the grafted bladder cells expressed urothelial and smooth muscle specific markers, both in vitro and in vivo [15].
The reconstruction of neo-urethra was performed also using porcine acellular corporal spongiosum matrices seeded with lingual keratinocytes and corporal smooth muscle cells (SMCs) by static-dynamic seeding method. The SMCs seeded scaffolds enhanced the growth of the epidermal layer, improved the vascularity, and promoted the infiltration of SMCs into the biomaterial with a net improvement in the graft biomechanical properties [40].
A tissue engineered urethra was realized using a modified 3D porous SIS scaffold seeded with human urine-derived stem cells (UDSCs) differentiated into urothelial cells and SMCs. Considering histological and immunohistochemical analysis, the grafts were comparable to the control tissues obtained by seeding urothelial cells and SMCs derived from native ureter on to SIS scaffolds. Considering the type of culture, dynamic culture provided superior infiltration of cells into the SIS and development of a multi-layered mucosa similar to that of native urethra, in comparison to static culture [13].
Urethra has also been reconstructed with in vitro epithelial-differentiated adipose-derived stem cells (ADSCs) seeded bladder acellular matrix grafts to correct a 2 cm urethral defect in rabbit model. The scaffolds seeded with this procedure showed better functional results in comparison with unseeded scaffolds and scaffolds seeded with undifferentiated ADSCs (control groups). In vivo were shown wider neo-urethra caliber, less postoperative complications and less strictures and fistulas, while ex vivo less fibrosis and growth of a multi-layered epithelium in the neo-urethra [41].
On the other hand, in case of bladder reconstruction, bovine pericardium (Supple Peri-Guard®) was tested in a case of entero-vesical fistula [42], but also porcine SIS and Urinary Bladder Matrix (UBM) seeded with human urothelial cells [43], where the luminal and abluminal surfaces of the UBM demonstrated significantly greater cell viability and cell proliferative activity compared with those of SIS.
In another study, bladder augmentation was performed using acellular collagen matrix in five patients presenting poor bladder capacity and compliance [44]. Surgeons used 4-layered SIS membrane (Surgisis®) covered by soft perivesical tissue or by omentum flap was used for the augmentation procedure. Bladder capacity and compliance increased at 6 months from the surgical procedure and remained stable at 18 months. At 6 months, there was no evidence of SIS remnants, while normal transitional mucosa and sero-muscular layer containing smooth muscle fascicles were found, small nerve trunks and vessels within abundant type III collagen. After 3 years of follow-up, no kidney damage or bladder diverticular stones were observed. Nonetheless, muscle regeneration was poor and continence was not achieved.
3.2. Naturally Derived Polymers
Similarly, naturally derived polymers are both highly biocompatible and biodegradable over time allowing in the meanwhile for tissue regeneration. Natural materials, such as collagen, provide natural adhesive ligands that promote cell attachment. In fact, collagen is the major component of the ECM and connective tissues and can be easily purified from both animal and human tissues. It provides the structural integrity to help in cellular growth and tissue development, with a concomitant minimal inflammatory response. Moreover, it has been approved by FDA for many medical applications.
Collagen has been tested also in combination with other materials. It has been used to reconstruct a tissue engineered tubular construct for urinary diversion in a pig model in combination with a propylene mesh (Vypro) with and without UCs seeding obtained from bladder’s biopsy [45]. In all cases, obstructions and hydronephrosis were present and no benefits were found for the pre-seeding of the scaffold.
The same material-based scaffolds were used to realize tubular constructs in pig model through standard freezing, lyophilization and cross-linking techniques [46]. The animals were divided into three groups: untreated scaffolds, SMCs seeded scaffolds and grafts formed by subcutaneously pre-implantation of a basic construct. After 1 month, pre-implantation of the basic construct resulted in improved drainage and vascularization compared with seeded and unseeded scaffolds. The outcome was favorable when compared to the other conduits.
Collagen has been used also for urethral replacement seeded with autologous bladder cells in a rabbit model [47] for 1-cm urethral defects. Unseeded scaffolds uniformly collapsed and formed strictions, whereas the seeded ones did not, maintaining patency and normal urethral architecture. Histological and immunocytochemical examination of the patches showed complete urethral structure at 1 month after implantation in the seeded scaffolds, whereas unseeded ones demonstrated extensive scarring with limited or absence of urothelium. Compared with controls, seeded patches contained organized muscle bundles able to contract in response to cholinergic, adrenergic and electrical input.
Using a canine model [48], researchers have demonstrated the superiority of a VEGF-bound collagen scaffold over the same unconjugated scaffold to correct a 5 cm defect in the anterior urethra, showing a better urethral regeneration in terms of thicker epithelial layer, higher density of blood vessels and SMCs and less inflammation, and in terms of functional parameters (larger neo-urethra diameter and lower neo-urethra contracture) at 6 months after the procedure.
The successful urethral regeneration of 2 cm defect using a double-layered acellular high density collagen tube in rabbit model has been obtained [19]. In 60% of the treated animals, no complications were reported. At 9 months after the procedure, histological and immunohistochemical analyses of the graft demonstrated complete stratification of the urothelium, with submucosal muscle bundles and progressive degradation and remodeling of the graft collagen.
3.3. Synthetic Scaffolds
The matrix porosity is crucial for ECM deposition and cell adhesion and engraftment. Matrix should be porous enough to promote cell and nutrient diffusion, but this feature might negatively affect the material’s mechanical strength.
The advantage of synthetic materials consists in the possibility to have defined and reliable mechanical features even if the usual disadvantage is given by the limited biocompatibility and the easier ability to provoke a foreign body reaction. Synthetic polyesters like PGA, PLA and PLGA, are biodegradable, non-toxic and are widely used in regenerative medicine and already approved by FDA. They are biodegradable and biocompatible since the degradation products are non-toxic, natural metabolites that are eventually eliminated from the body in the form of carbon dioxide and water. They consists of thermoplastic polymers that can be easily formed into a 3D scaffold with the desired microstructure, shape and dimensions using several techniques including molding, extrusion, solvent casting, phase separation, gas foaming and electrospinning that permits to control pore size and density [9,10,49].
Synthetic materials have been used both for urinary bladder reconstruction and urinary conduits creation. In case of urinary diversions, scaffolds have been made in PGA and PLGA [50] both unseeded and seeded with smooth muscle cells (SMCs) derived from bladder, adipose tissue and blood. It has been found that the use of SMCs led to regeneration of a native bladder-like neo-organ composed of urothelium and smooth muscle layers. On the contrary, the acellular scaffold has been lead to a fibrotic tissue formation with a smaller number of SMCs.
An observational study was performed on five patients needing urethral reconstruction using synthetic tubular scaffolds that were seeded in vitro with autologous muscle and epithelial cells. After 71 months from implantation, the reconstructed urethras remained patent and biopsies confirmed normal urethral tissue formation [51].
Another group performed the evaluation of the antifibrotic activity of the WNT pathway inhibitor ICG-001 delivering collagen/PLLA scaffold in vitro and in vivo. Compared to non-drug treated scaffolds seeded with epithelial cells, scaffolds treated with ICG-001 for the correction of 2 cm length urethral defect in male New Zealand rabbits were not associated to surgical complications in terms of fistulas and strictures and better histological outcomes in terms of multi-layered epithelium, lower collagen deposition and increased number of SMCs in submucosa [52].
The same author used a 3D bio-printed urethra in rabbit model using three types of cartridges: one loaded with a synthetic polymer blend and two with hydrogels loaded with either UCs or SMCs. The constructs presented similar mechanical properties to native tissue, but the main limitations consisted of the difficulty to print smaller scaffolds, the limited available bio-inks, the inability to produce complex tissues and the slow processing time [53].
In case of bladder reconstruction, many efforts have been focuses on the application of synthetic materials. In seven patients with myelomeningocele needing cystoplasty, synthetic and composite synthetic natural bladder-shaped scaffolds were seeded with bladder cells obtained via biopsy, in order to augment the native bladder. After 46 months from implantation, the bladders were functioning normally [28].
An in vivo bladder augmentation was performed using in vitro PGA scaffolds seeded with fibroblasts in rat model. Seeded scaffolds resulted in complete epithelialization while in unseeded one no epithelialization was found in the central region [54].
PLLA scaffolds seeded with bone marrow mesenchymal stem cells (MSCs) have been used for patients needing cystoplasty. The scaffolds provided a 3D structure to maximize the cell-matrix penetration, maintain myogenic differentiation of growth factor-induced bone marrow MSCs and promote tissue remodeling with revascularization in vivo [55].
Recently, an antimicrobial polymethyl siloxane-modified polyurethanes (TPU/PDMS) has been designed and assessed for its potential application as urologic implant. The successful integration of varying contents of PDMS within the molten polyurethane matrix has been reported. The antimicrobial composition has been demonstrated to support the growth of the mitochondrially viable and interconnected murine fibroblasts over 7 days in culture [56].
4. Seeded and Unseeded Scaffolds: The Choice of Cells Type
Autologous cell cultures and scaffolds for three-dimensional cell growth are essential for successful urinary tract replacement and reconstruction. For this application, two tissue engineering strategies have been investigated: biomatrices that have been seeded by the surrounding healthy tissue after implantation (this approach highly depends on regenerative activity of surrounding tissue), and various types of scaffolds already seeded for example with epithelial and mesenchymal cell in vitro and then transplanted.
In both cases, scaffold has a fundamental role and must be well chosen with the appropriate features considering the specific application in which it is needed to be applied.
First of all, in both unseeded and seeded scaffold, an important role is given by porosity and pore size distribution that determine the interaction of the biomaterials and cells. Pore size has been shown to be one of the most important factors which controls the rate of invasion as well as the type of invading cells. Based on the structure and cell growth, scaffolds have been classified by Brehmer et al. in carrier-, fleece- and sponge-type. The first group, whose microstructure is made by fiber meshes with very small pore sizes (<15 µm) or foils with no pores, has no or small pore size with few or no ingrowth of cells. The third one has pores (>15 µm) which can be invaded by cells. The second group supports cell growth inside scaffold, but the epithelial coverage is poor. In fact, cell growth inside and the covering of the scaffold by a multi-layered epithelium is dependent on scaffold and pore size. It has been shown that, in case of pore size < 38 µm, the formation of multi-layered epithelial lining on the surface was possible. No epithelium was present on top of fleece-type scaffolds with huge (200 µm) pores, but good epithelium covering sponge-type scaffolds (26 µm) was observed [57]. Another important factor is represented by the interconnecting pores from which complete migration of cells through the scaffold and cell nutrition inside the scaffold depend. Beyond the pore size inside the scaffolds, the surface is important as well. In fact, even if a scaffold is porous but the surface is smooth, cells cannot invade into the porosity segments inside. For these reasons, epithelial differentiation on the surface and cellular ingrowth into the scaffolds have been found to be possible only in scaffolds with a certain pore size and the ingrowth will be one of the most important factors for epithelium survival and regrowth when exposed to urine flow and mechanical strain in vivo [57].
In case of bladder substitution, scaffolds consisting in fibrillary collagen type I and porous basement membrane such as BAM [13,14,58] and small intestinal submucosa (SIS) [11,12,13,14] have been employed. The porosity of these scaffolds can be increased adding an oxidation treatment with peracetic acid enhancing decellularization process. The increasing porosity is demonstrated to be a critical requirement for successful formation of urethral tubular structure, contributing to high cell proliferation rate and cell-matrix infiltration, leading to better in vivo tissue regeneration [15]. On the other hand, in order to produce porous urinary bladder scaffolds with different degrees of porosity and with a wide range of pore morphologies, natural polymer scaffolds can be produced by many different methods, such as: solvent casting, phase separation, gas-foaming techniques, electrospinning, freeze extraction, lyophilization and 3D printing. However, it is important to take in consideration that a too porous structural configuration can lead to urine permeation into the scaffold causing abnormal bladder regeneration [59,60].
Another important issue is represented by the chance of seeding different cell types to enhance tissue regeneration and reduce the inflammatory response after implantation. Bioengineered scaffolds can be implanted unseeded, pre-seeded with cultured cells or seeded with minced tissue. After implantation, the scaffolds need to integrate with surrounding host tissue and mimic its histology, biomechanics and physiological features.
In tissue engineered bladder case, the appropriate formation of a smooth muscle layer and urothelium, including innervation and vascularization, can be considered a prerequisite to reach the required biomechanical and functional properties [8].
Unseeded scaffolds may have a substantial limitation in terms of regeneration depending on the presence and proximity of native cells of surrounding tissues, since cells can migrate in limited distances. In case native cells are unable to reach the defect, scar formation occurs preventing fibrin deposition, re-epithelialization and remodeling of tissue. In case of urethral replacements, it has been demonstrated that normal tissue formation using acellular grafts was possible only weather the maximum defect distance was 0.5 cm [39].
Currently, the perfect cell line has not been identified for cell seeding in urology context. The ideal one should be easily obtained from ethical acceptable sources, have the potential to be maintained in culture indefinitely, be inducible to form the functional cell types and should proliferate efficiently in culture conditions without invoking immunological response. A tissue engineered urinary conduit should resemble to native urothelial tissue, consisting of urothelial cells (UCs) and smooth muscle cells (SMCs) which respectively provide an impermeable barrier to urine and provide structure and contractility for urine transport. However, the choice of cell type to seed can vary from a fully differentiated one, capable of target cell differentiation, to an undifferentiated that can supply a suitable environment for target cell ingrowth, but also a combination of both can be appropriate. Moreover, autologous cells should be the best candidates in order to avoid immune response, with the disadvantages of issues associated with cell harvest and significant concerns in the setting of malignancy, especially in case of using differentiated UCs. Furthermore, especially in the case of bladder cancer which requires cystectomy, a relevant issue is the proliferative cell capacity leading to poor outcomes [9].
Several autologous cell types have been harvested from patients, cultured and expanded in vitro and seeded into various scaffold types in urological context. Each cell type used, showed advantages and disadvantages that must be taken in consideration when the best candidate has to be chosen. Among differentiated cell types, urothelial cells can be easily obtained from biopsies or washes of autologous healthy bladder or urine and present low immunogenicity, but the basic limitation is the impossibility to use in malignant applications. Whereas UCs form an impermeable barrier of urothelial tissue, smooth muscle cells (SMCs) provide support and allow contractility. Like UCs, SMCs can be harvested form urothelial tissue of patient, which however has malignancy concerns. This type of cells can be also obtained from a variety of tissues, including adipose, peripheral blood, cord blood and bone marrow. Epithelial progenitor cells can be obtained from oral mucosa and foreskin and, like UCs, present low immunogenicity, but the harvesting is dependent on retrieval site availability.
On the other hand, stem cells are interesting alternative candidates that are subject of intense investigation because of their regenerative ability and their ability to produce specialized tissue from an undifferentiated state. Stem cells are obtained from embryonic (embryonic stem cells—ESCs) tissue or non-embryonic (adult stem cells or somatic stem cells—SSCs) tissue. Recently, induced pluripotent stem cells (iPSCs) have become another source of stem cells. ESCs can give rise to any fully differentiated SSCs because of their ability to proliferate in an undifferentiated, but pluripotent state (self-renewal) and the ability to differentiate into many different cell types. However, they present ethical concerns and can be associated to malignancies in vivo. SSCs are undifferentiated cells that are easily obtained from several sources like bone marrow, adipose tissue, hair follicles, amniotic fluid, endometrium and even urine, but they do not have ethical or malignancy issues. Bone marrow stem cells have low immunogenicity, are rich in several growth factors and present the possibility to differentiate into various cells types, including urothelium and SMCs, but the main limitation is given by the very invasive surgical procedure to harvest them from the patient beyond limited self-renewal and low urothelial and endothelial differentiation. Urine-derived stem cells are: easily retrievable, potentially high replicative and can differentiate into several cells types, including urothelium and SMCs. Adipose-derived stem cells are easily retrievable too and can successful differentiate in urothelium.
Finally, iPSCs are fully differentiated adult cells genetically manipulated to behave like ESCs, overcoming ethical issues and becoming a reliable source of autologous tissue in urinary applications, avoiding the potential for immune rejection. iPSCs possess self-renewal and pluripotency properties like ESCs, but malignant potential is a real possibility since they are genetically modified with a consequent possibility to introduce unwanted oncogenes [9,10,49].
5. Mechanical Stimulation of Scaffold Using a Bioreactor
Tissue engineering has a high potential for regenerative medicine that combines the patient’s cells with an in vitro cultivated and functionalized biomaterial before replacing damaged organs. In fact, a seeding prior to implantation could prevent a shrinkage and stenosis formation in case of tissue engineered urinary conduits.
The most appropriate cells for epithelium regeneration are UCs in case of benign diseases, while in case of urinary cancer alternative cell source is needed. For muscle layer reconstruction, the best candidate seems to be bone-marrow MSCs and adipose-derived stem cells. Despite their invasive cell collection method, they seems the best choice for their good proliferation capacity, easy isolation method and enhanced neovascularization [7].
However, one of the major limits of the bioengineered tissues consists in the unsatisfactory blood supply and oxygen diffusion inside the tissue. While angiogenesis can take several days to provide a sufficient blood supply, the available oxygen will be depleted in few hours. A possible solution could be to induce angiogenesis by engineering a scaffold that slowly release growth factors, but vessels formation could be too slow and insufficient to maintain constructs over the long term [10]. In fact, it is fundamental reproducing the correct macroscopic and molecular architecture of scaffold, cell and microvascular tissue for the functioning of the bioengineered tissue. However, even if in some cases cells can be seeded on the construct, the appropriate tissue architecture can be not achieved resulting in the failure of the scaffold.
Bioreactors could be a potential solution in order to provide the appropriate physiological forces such as compression, sheer stresses and pulsatile flow during production of the tissue in vitro. In fact, the exposure of the scaffold to these stresses can improve the mechanical properties of the bioengineered tissues [10].
In this phase, on the basis of biological and technological requirements, bioreactors properly adapted to the specific application are important tools to allow the incubation and functionalization under standardized conditions. Regarding the setup, the proper bioreactor system should be adjustable to the specific scaffold geometries and should allow visual inspection from outside. The geometry should be as small as possible and a particular attention has to be paid for material choice that must be biocompatible, sterilizable/autoclavable, durable and dimensionally stable at the same time [61].
A bioreactor system for urological applications has been developed for seamless and tubular scaffold materials with different lengths and diameters. The cylindrical bioreactor was developed for seeding and co-culturing two different cell types inside and outside the tubular scaffold. The several advantages that this bioreactor demonstrated included the possible application to different scaffold geometries and the use of designed lids for the medium reservoir that allowed regular sampling and application of substances under sterile conditions. In case of urinary conduits, smooth muscle cells should be applied onto the outer surface of the tubular constructs, whereas urothelial cells have to be applied along the luminal side [61].
Especially in case of urinary bladder, whose function is to store and evacuate urine, keeping in the meanwhile the proper chemical gradients between urine and blood, mechanical properties could be achieved by using a bioreactor. The two factors that allow bladder functions are the cellular compartment (urothelium in the lumen of the bladder which serves as an effective blood-urine barrier and SMCs within the bladder wall which maintain low pressure during filling and contract during bladder emptying) and extracellular compartment which is composed by collagen, proteoglycans and glycosaminoglycans, which function as a reservoir for growth factors that strongly influence cell growth, differentiation, development and metabolic responses [62]. Probably, different results achieved in vivo can be cause by the necessity to use a more controlled tissue building process, for example preconditioning the bladder tissue in vitro by applying mechanical stimuli. To improve tissue engineered bladder, it is necessary reconstitute in vitro cellular and acellular components of normal urinary bladder and mechanical features such as compliance and impermeable epithelial surface. For these reasons, the ideal bioreactor should include the ability to regulate mechanical and nutrient environments in order to promote cell proliferation, differentiation and favorable matrix deposition [63].
Bioreactors are normally designed to control environmental factors such as pH, temperature and oxygen concentration, but also they can produce a variety of forces, including compression, shear stress and continuous or pulsatile flow of culture media, in order to improve tissue and organ regeneration [62,63,64,65].
Studies exploring the impact of force generation on urinary bladder are performed using custom-made devices that can present several limitations. These devices provide isolated mechanical stimulus such as strain or hydrostatic pressure in a non-physiological manner, since normal urinary bladder stretches upon filling with very little pressure generation, while do not exist instruments that deform cell culture substratum in a multiaxial direction with or without pressure. Even if simultaneous hydrostatic pressure and strain are applied, the pressure and strain are settled in a non-physiological range. Furthermore, it is necessary to chance media manually, increasing the risk of contamination.
A new type of urinary bladder bioreactor system using hydrostatic pressures have been designed to study urinary bladder tissue engineering, providing a suitable 3D matrix for in vitro cell attachment using biodegradable natural scaffold, seeded with porcine bladder SMCs or UCs. Authors concluded that the use of bladder bioreactor can accelerate tissue organization and maturation in vivo, shortening the time required to achieved a fully functional organ [62].
In another study, hydrostatic pressure (10 cm H2O) and stretch forces were exerted on human bladder smooth muscle cells seeded on aligned nanofibrous PCL/PLLA scaffolds resulted in functional improvement of the engineered tissue. Authors demonstrated the positive effect of mechanical forces since the proper hydrostatic pressure in combination with appropriate surface stimulation on cells causes a tissue-specific phenotype that needs to be considered in bladder tissue engineering [66].
In case of tissue engineered bladder, since the native organ is continuously filled and emptied, resulting in continuous loading of the tissue, a better outcome may be achieved by mimicking these dynamic conditions. Tiemessen et al. evaluated strips of lyophilized porous natural type I collagen scaffolds clamped in a Bose Electroforce Bio-Dynamic bioreactor that were mechanically stimulated using cyclical uniaxial strain, mimicking the filling and emptying of the bladder. The strips were initially seeded statically with SMC or UC and then dynamically in the bioreactor, while control scaffolds were cultured under static conditions. The results demonstrated that conditioning of collagen-based scaffolds by mechanical stimulation leads to more SMC, probably bypassing difficulties related to poor SMC in-growth and muscle development in tissue engineered bladders [67].
Recently, with the aim to restore the neuronal network propagating signals which regulate urine storage and voiding of tissue engineered urinary bladder, it has been developed a conductive bio-composite combining graphene and amniotic membrane. Amniotic membrane has been used for its unique properties supporting regeneration of smooth muscle layer, while graphene has been chosen to create the interface between cells and external stimuli replacing neuronal network. The constructs have been seeded with porcine UCs and SMCs derived from porcine detrusor. It has been demonstrated that the presence of graphene layer significantly increased electrical conductivity of the bio-composite and the contractile response indicated the effective SMCs stimulation [68].
6. Conclusions
In case of tissue engineered urinary substitutes, the main objective consists in the obtaining of a fully impermeable scaffold. The scaffold has to maintain his patency in case of urinary conduits for diversions, and also has to recreate bladder’s mechanical properties such as compliance and elasticity in order to act as a urine reservoir in case of urinary bladder.
Further efforts have to be done in order to find the best material which has to be enough impermeable to prevent urine leakage, while allowing adequate cells migration, adhesion, proliferation and differentiation.
Nearby the choice of scaffold material, relevant is the issue about cells which could be grown. It is possible that for shorter defects (0.5 cm), pre-seeding is not necessary, but for longer ones it could be necessary due to the limited capacity of cells to migrate through the host tissue [39]. Cell type is another important matter: UCs have reported positive results in case of urethral and bladder reconstruction, but they are not applicable in case of malignancy, which is the most recurring clinical issue. Moreover, muscle layer is relevant for mechanical behavior of the construct, but the using of SMCs presents the same malignancy issue of UCs. For these reasons, stem cells are good candidates for pre-seeding of urinary tissue engineered scaffolds. In particular, MSCs could be the best one as they can be harvested from various tissue types such as bone marrow and adipose tissue. Further examinations have to be performed to demonstrate the superiority of one of this type of cells.
Moreover, an eventual involvement of a bioreactor could be useful, especially in case of urinary bladder engineering to recreate physiological environment, enhancing the scaffold repopulation in vitro and then tissue regeneration in vivo. Additional experiments still need to be performed.
The ideal tissue engineered urinary scaffold and possible cell types to pre-seed have still to be found, even if some of them demonstrated promising results.
Author Contributions
Conceptualization: all authors, literature search and data collection: M.C., manuscript writing: M.C., A.M., writing—review and editing: all authors, supervision: F.D.M. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by LifeLab Program of the Consorzio per la Ricerca Sanitaria (CORIS) of the Veneto Region, Italy (DGR1017, 17 July 2018).
Acknowledgments
The authors would like to thank the Consorzio per la Ricerca Sanitaria (CORIS) of the Veneto Region for financial and administrative support.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Serrano-Aroca, Á.; Vera-Donoso, C.D.; Moreno-Manzano, V. Bioengineering approaches for bladder regeneration. Int. J. Mol. Sci. 2018, 19, 1796. [Google Scholar] [CrossRef] [Green Version]
- Witjes, J.A.; Lebret, T.; Compérat, E.M.; Cowan, N.C.; De Santis, M.; Bruins, H.M.; Hernández, V.; Espinos, E.L.; Dunn, J.; Rouanne, M.; et al. Updated 2016 EAU guidelines on muscle-invasive and metastatic bladder cancer. Eur. Urol. 2016, 71, 462–475. [Google Scholar] [CrossRef]
- Bazargani, S.T.; Djaladat, H.; Ahmadi, H.; Miranda, G.; Cai, J.; Schuckman, A.K.; Daneshmand, S. Gastrointestinal complications following radical cystectomy using enhanced recovery protocol. Eur. Urol. Focus 2017, 4, 889–894. [Google Scholar] [CrossRef] [PubMed]
- Yuh, B.E.; Nazmy, M.; Ruel, N.H.; Jankowski, J.T.; Menchaca, A.R.; Torrey, R.R.; Linehan, J.A.; Lau, C.S.; Chan, K.G.; Wilson, T.G. Standardized analysis of frequency and severity of complications after robot-assisted radical cystectomy. Eur. Urol. 2012, 62, 806–813. [Google Scholar] [CrossRef] [PubMed]
- Sloff, M.; De Vries, R.; Geutjes, P.; IntHout, J.; Ritskes-Hoitinga, M.; Oosterwijk, E.; Feitz, W. Tissue engineering in animal models for urinary diversion: A systematic review. PLoS ONE 2014, 9, e98734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kloskowski, T.; Jundzill, A.; Kowalczyk, T.; Nowacki, M.; Bodnar, M.; Marszałek, A.; Pokrywczynska, M.; Frontczak-Baniewicz, M.; Kowalewski, T.; Chłosta, P.; et al. Ureter regeneration—The proper scaffold has to be defined. PLoS ONE 2014, 9, e106023. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kloskowski, T.; Kowalczyk, T.; Nowacki, M.; Drewa, T. Tissue engineering and ureter regeneration: Is it possible? Int. J. Artif. Organs 2013, 36, 392–405. [Google Scholar] [CrossRef] [PubMed]
- Ajalloueian, F.; Lemon, G.; Hilborn, J.; Chronakis, I.S.; Fossum, M. Bladder biomechanics and the use of scaffolds for regenerative medicine in the urinary bladder. Nat. Rev. Urol. 2018, 15, 155–174. [Google Scholar] [CrossRef]
- Johnson, S.C.; Smith, Z.L.; Sack, B.S.; Steinberg, G.D. Tissue engineering and conduit substitution. Urol. Clin. N. Am. 2018, 45, 133–141. [Google Scholar] [CrossRef] [PubMed]
- Murphy, S.V.; Atala, A. Organ engineering—Combining stem cells, biomaterials, and bioreactors to produce bioengineered organs for transplantation. BioEssays 2012, 35, 163–172. [Google Scholar] [CrossRef]
- Drewa, T. The artificial conduit for urinary diversion in rats: A preliminary study. Transplant. Proc. 2007, 39, 1647–1651. [Google Scholar] [CrossRef] [PubMed]
- Kropp, B.P.; Rippy, M.K.; Badylak, S.; Adams, M.C.; Keating, M.A.; Rink, R.C.; Thor, K.B. Regenerative urinary bladder augmentation using small intestinal submucosa: Urodynamic and histopathologic assessment in long-term canine bladder augmentations. J. Urol. 1996, 155, 2098–2104. [Google Scholar] [CrossRef]
- Wu, S.; Liu, Y.; Bharadwaj, S.; Atala, A.; Zhang, Y. Human urine-derived stem cells seeded in a modified 3D porous small intestinal submucosa scaffold for urethral tissue engineering. Biomaterials 2011, 32, 1317–1326. [Google Scholar] [CrossRef]
- Campodonico, F.; Benelli, R.; Michelazzi, A.; Ognio, E.; Toncini, C.; Maffezzini, M. Bladder cell culture on small intestinal submucosa as bioscaffold: Experimental study on engineered urothelial grafts. Eur. Urol. 2004, 46, 531–537. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Bharadwaj, S.; Lee, S.J.; Atala, A.; Zhang, Y. Optimization of a natural collagen scaffold to aid cell–matrix penetration for urologic tissue engineering. Biomaterials 2009, 30, 3865–3873. [Google Scholar] [CrossRef] [PubMed]
- Liao, W.-B.; Song, C.; Li, Y.-W.; Yang, S.-X.; Meng, L.-C.; Li, X.-H. Tissue-engineered conduit using bladder acellular matrix and bladder epithelial cells for urinary diversion in rabbits. Chin. Med. J. 2013, 126, 335–339. [Google Scholar] [PubMed]
- Micol, L.; da Silva, L.F.A.; Geutjes, P.J.; Oosterwijk, E.; Hubbell, J.; Feitz, W.F.; Frey, P. In-vivo performance of high-density collagen gel tubes for urethral regeneration in a rabbit model. Biomaterials 2012, 33, 7447–7455. [Google Scholar] [CrossRef]
- Sayeg, K.; Freitas-Filho, L.G.; Waitzberg, A.F.L.; Arias, V.E.A.; Laks, M.; Egydio, F.M.; Oliveira, A.S. Integration of collagen matrices into the urethra when implanted as onlay graft. Int. Braz. Urol. 2013, 39, 414–423. [Google Scholar] [CrossRef] [Green Version]
- Pinnagoda, K.; Larsson, H.M.; Vythilingam, G.; Vardar, E.; Engelhardt, E.-M.; Thambidorai, R.C.; Hubbell, J.A.; Frey, P. Engineered acellular collagen scaffold for endogenous cell guidance, a novel approach in urethral regeneration. Acta Biomater. 2016, 43, 208–217. [Google Scholar] [CrossRef]
- Aufderklamm, S.; Vaegler, M.; Kelp, A.; Maurer, S.; Gustafsson, L.; Mundhenk, J.; Daum, L.; Stenzl, A.; Sievert, K.-D.; Amend, B.; et al. Collagen cell carriers seeded with human urothelial cells for urethral reconstructive surgery: First results in a xenograft minipig model. World J. Urol. 2016, 35, 1125–1132. [Google Scholar] [CrossRef] [PubMed]
- Xie, M.; Song, L.; Wang, J.; Fan, S.; Zhang, Y.; Xu, Y. Evaluation of stretched electrospun silk fibroin matrices seeded with urothelial cells for urethra reconstruction. J. Surg. Res. 2013, 184, 774–781. [Google Scholar] [CrossRef] [PubMed]
- Algarrahi, K.; Franck, D.; Ghezzi, C.; Cristofaro, V.; Yang, X.; Sullivan, M.P.; Chung, Y.G.; Affas, S.; Jennings, R.; Kaplan, D.L.; et al. Acellular bi-layer silk fibroin scaffolds support functional tissue regeneration in a rat model of onlay esophagoplasty. Biomaterials 2015, 53, 149–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, B.; Zhang, Y.; Zhou, L.; Sun, Z.; Zheng, J.; Chen, Y.; Dai, Y. Development of a porcine bladder acellular matrix with well-preserved extracellular bioactive factors for tissue engineering. Tissue Eng. Part C Methods 2010, 16, 1201–1211. [Google Scholar] [CrossRef]
- Oberpenning, F.; Meng, J.; Yoo, J.J.; Atala, A. De novo reconstitution of a functional mammalian urinary bladder by tissue engineering. Nat. Biotechnol. 1999, 17, 149–155. [Google Scholar] [CrossRef]
- Lai, J.-Y.; Yoon, C.Y.; Yoo, J.J.; Wulf, T.; Atala, A. Phenotypic and functional characterization of in vivo tissue engineered smooth muscle from normal and pathological bladders. J. Urol. 2002, 168, 1853–1858. [Google Scholar] [CrossRef]
- Nakanishi, Y.; Chen, G.; Komuro, H.; Ushida, T.; Kaneko, S.; Tateishi, T.; Kaneko, M. Tissue-engineered urinary bladder wall sing PLGA mesh-collagen hybrid scaffolds: A omparison study of collagen sponge and gel as a caffold. J. Pediatr. Surg. 2003, 38, 1781–1784. [Google Scholar] [CrossRef]
- Atala, A.; Freeman, M.R.; Vacanti, J.P.; Shepard, J.; Retik, A.B. Implantation in vivo and retrieval of artificial structures consisting of rabbit and human urothelium and human bladder muscle. J. Urol. 1993, 150, 608–612. [Google Scholar] [CrossRef]
- Atala, A.; Bauer, S.B.; Soker, S.; Yoo, J.J.; Retik, A.B. Tissue-engineered autologous bladders for patients needing cystoplasty. Lancet 2006, 367, 1241–1246. [Google Scholar] [CrossRef]
- Crapo, P.M.; Gilbert, T.; Badylak, S.F. An overview of tissue and whole organ decellularization processes. Biomaterials 2011, 32, 3233–3243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, M.H.; Chen, J.; Kirilak, Y.; Willers, C.; Xu, J.; Wood, D. Porcine small intestine submucosa (SIS) is not an acellular collagenous matrix and contains porcine DNA: Possible implications in human implantation. J. Biomed. Mater. Res. Part B Appl. Biomater. 2005, 73, 61–67. [Google Scholar] [CrossRef]
- Gilbert, T.; Freund, J.M.; Badylak, S.F. Quantification of DNA in biologic scaffold materials. J. Surg. Res. 2009, 152, 135–139. [Google Scholar] [CrossRef] [Green Version]
- Badylak, S.F.; Gilbert, T. Immune response to biologic scaffold materials. Semin. Immunol. 2008, 20, 109–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Record, R.D.; Hillegonds, D.; Simmons, C.; Tullius, R.; Rickey, F.; Elmore, D.; Badylak, S. In vivo degradation of 14C-labeled small intestinal submucosa (SIS) when used for urinary bladder repair. Biomaterials 2001, 22, 2653–2659. [Google Scholar] [CrossRef]
- Liao, W.; Yang, S.; Song, C.; Li, Y.; Meng, L.; Li, X.; Xiong, Y. Tissue-engineered tubular graft for urinary diversion after radical cystectomy in rabbits. J. Surg. Res. 2013, 182, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Adamowicz, J.; Kloskowski, T.; Stopel, M.; Gniadek, M.; Rasmus, M.; Balcerczyk, D.; Buhl, M.; Gagat, M.; Antosik, P.; Grzanka, D.; et al. The development of marine biomaterial derived from decellularized squid mantle for potential application as tissue engineered urinary conduit. Mater. Sci. Eng. C 2020, 119, 111579. [Google Scholar] [CrossRef]
- Bhargava, S.; Chapple, C.; Bullock, A.; Layton, C.; MacNeil, S. Tissue-engineered buccal mucosa for substitution urethroplasty. BJU Int. 2004, 93, 807–811. [Google Scholar] [CrossRef]
- Fu, Q.; Deng, C.-L.; Liu, W.; Cao, Y.-L. Urethral replacement using epidermal cell-seeded tubular acellular bladder collagen matrix. BJU Int. 2007, 99, 1162–1165. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Xu, Y.-M.; Song, L.-J.; Fu, Q.; Cui, L.; Yin, S. Urethral Reconstruction Using Oral Keratinocyte Seeded Bladder Acellular Matrix Grafts. J. Urol. 2008, 180, 1538–1542. [Google Scholar] [CrossRef]
- Dorin, R.P.; Pohl, H.; De Filippo, R.E.; Yoo, J.J.; Atala, A. Tubularized urethral replacement with unseeded matrices: What is the maximum distance for normal tissue regeneration? World J. Urol. 2008, 26, 323–326. [Google Scholar] [CrossRef]
- Feng, C.; Xu, Y.-M.; Fu, Q.; Zhu, W.-D.; Cui, L. Reconstruction of three-dimensional neourethra using lingual keratinocytes and corporal smooth muscle cells seeded acellular corporal spongiosum. Tissue Eng. Part A 2011, 17, 3011–3019. [Google Scholar] [CrossRef]
- Li, H.; Xu, Y.; Xie, H.; Li, C.; Song, L.; Feng, C.; Zhang, Q.; Xie, M.; Wang, Y.; Lv, X. Epithelial-differentiated adipose-derived stem cells seeded bladder acellular matrix grafts for urethral reconstruction: An animal model. Tissue Eng. Part A 2014, 20, 774–784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moon, S.J.; Kim, D.H.; Jo, J.K.; Chung, J.H.; Lee, J.Y.; Park, S.Y.; Kim, Y.T.; Park, H.K.; Choi, H.Y.; Moon, H.S. Bladder reconstruction using bovine pericardium in a case of enterovesical fistula. Korean J. Urol. 2011, 52, 150–153. [Google Scholar] [CrossRef] [Green Version]
- Davis, N.F.; Callanan, A.; McGuire, B.B.; Flood, H.D.; McGloughlin, T. Evaluation of viability and proliferative activity of human urothelial cells cultured onto xenogenic tissue-engineered extracellular matrices. Urology 2011, 77, 1007.e1–1007.e7. [Google Scholar] [CrossRef] [PubMed]
- Caione, P.; Boldrini, R.; Salerno, A.; Nappo, S.G. Bladder augmentation using acellular collagen biomatrix: A pilot experience in exstrophic patients. Pediatr. Surg. Int. 2012, 28, 421–428. [Google Scholar] [CrossRef] [PubMed]
- Geutjes, P.; Roelofs, L.; Hoogenkamp, H.; Walraven, M.; Kortmann, B.; De Gier, R.; Farag, F.; Tiemessen, D.; Sloff, M.; Oosterwijk, E.; et al. Tissue engineered tubular construct for urinary diversion in a preclinical porcine model. J. Urol. 2012, 188, 653–660. [Google Scholar] [CrossRef] [PubMed]
- Sloff, M.; Simaioforidis, V.; Tiemessen, D.M.; Janke, H.P.; Kortmann, B.B.; Roelofs, L.A.; Geutjes, P.J.; Oosterwijk, E.; Feitz, W.F. Tubular constructs as artificial urinary conduits. J. Urol. 2016, 196, 1279–1286. [Google Scholar] [CrossRef] [PubMed]
- De Filippo, R.; Yoo, J.J.; Atala, A. Urethral replacement using cell seeded tubularized collagen matrices. J. Urol. 2002, 168, 1783–1789. [Google Scholar] [CrossRef]
- Jia, W.; Tang, H.; Wu, J.; Hou, X.; Chen, B.; Chen, W.; Zhao, Y.; Shi, C.; Zhou, F.; Yu, W.; et al. Urethral tissue regeneration using collagen scaffold modified with collagen binding VEGF in a beagle model. Biomaterials 2015, 69, 45–55. [Google Scholar] [CrossRef] [PubMed]
- Pederzoli, F.; Joice, G.; Salonia, A.; Bivalacqua, T.J.; Sopko, N.A. Regenerative and engineered options for urethroplasty. Nat. Rev. Urol. 2019, 16, 453–464. [Google Scholar] [CrossRef]
- Basu, J.; Jayo, M.J.; Ilagan, R.M.; Guthrie, K.I.; Sangha, N.; Genheimer, C.W.; Quinlan, S.F.; Payne, R.; Knight, T.; Rivera, E.; et al. Regeneration of Native-Like Neo-Urinary Tissue from Nonbladder Cell Sources. Tissue Eng. Part A 2012, 18, 1025–1034. [Google Scholar] [CrossRef]
- Raya-Rivera, A.; Esquiliano, D.R.; Yoo, J.J.; Lopez-Bayghen, E.; Soker, S.; Atala, A. Tissue-engineered autologous urethras for patients who need reconstruction: An observational study. Lancet 2011, 377, 1175–1182. [Google Scholar] [CrossRef] [Green Version]
- Zhang, K.; Guo, X.; Zhao, W.; Niu, G.; Mo, X.; Fu, Q. Application of Wnt pathway inhibitor delivering scaffold for inhibiting fibrosis in urethra strictures: In vitro and in vivo study. Int. J. Mol. Sci. 2015, 16, 27659–27676. [Google Scholar] [CrossRef] [Green Version]
- Zhang, K.; Fu, Q.; Yoo, J.; Chen, X.; Chandra, P.; Mo, X.; Song, L.; Atala, A.; Zhao, W. 3D bioprinting of urethra with PCL/PLCL blend and dual autologous cells in fibrin hydrogel: An in vitro evaluation of biomimetic mechanical property and cell growth environment. Acta Biomater. 2017, 50, 154–164. [Google Scholar] [CrossRef]
- Drewa, T.; Sir, J.; Czajkowski, R.; Wozniak, A. Scaffold seeded with cells is essential in urothelium regeneration and tissue remodeling in vivo after bladder augmentation using in vitro engineered graft. Transplant. Proc. 2006, 38, 133–135. [Google Scholar] [CrossRef]
- Tian, H.; Bharadwaj, S.; Liu, Y.; Ma, P.X.; Atala, A.; Zhang, Y. Differentiation of human bone marrow mesenchymal stem cells into bladder cells: Potential for urological tissue engineering. Tissue Eng. Part A 2010, 16, 1769–1779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, S.; Mandhani, A.; Bose, S.; Basu, B. Dynamically crosslinked polydimethylsiloxane-based polyurethanes with contact-killing antimicrobial properties as implantable alloplasts for urological reconstruction. Acta Biomater. 2021, 129, 122–137. [Google Scholar] [CrossRef]
- Brehmer, B.; Rohrmann, D.; Becker, C.; Rau, G.; Jakse, G. Different types of scaffolds for reconstruction of the urinary tract by tissue engineering. Urol. Int. 2007, 78, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Sutherland, R.S.; Baskin, L.S.; Hayward, S.W.; Cunha, G.R. Regeneration of bladder urothelium, smooth muscle, blood vessels and nerves into an acellular tissue matrix. J. Urol. 1996, 156, 571–577. [Google Scholar] [CrossRef]
- Farhat, W.; Chen, J.; Erdeljan, P.; Shemtov, O.; Courtman, D.; Khoury, A.; Yeger, H. Porosity of porcine bladder acellular matrix: Impact of ACM thickness. J. Biomed. Mater. Res. 2003, 67, 970–974. [Google Scholar] [CrossRef] [PubMed]
- Cartwright, L.M.; Shou, Z.; Yeger, H.; Farhat, W.A. Porcine bladder acellular matrix porosity: Impact of hyaluronic acid and lyophilization. J. Biomed. Mater. Res. Part A 2006, 77, 180–184. [Google Scholar] [CrossRef]
- Seifarth, V.; Gossmann, M.; Janke, H.P.; Grosse, J.O.; Becker, C.; Heschel, I.; Artmann, G.M.; Artmann, A.T. Development of a bioreactor to culture tissue engineered ureters based on the application of tubular OPTIMAIX 3D scaffolds. Urol. Int. 2015, 95, 106–113. [Google Scholar] [CrossRef]
- Farhat, W.A.; Yeger, H. Does mechanical stimulation have any role in urinary bladder tissue engineering? World J. Urol. 2008, 26, 301–305. [Google Scholar] [CrossRef]
- Wallis, M.C.; Yeger, H.; Cartwright, L.; Shou, Z.; Radisic, M.; Haig, J.; Suoub, M.; Antoon, R.; Farhat, W.A. Feasibility study of a novel urinary bladder bioreactor. Tissue Eng. Part A 2008, 14, 339–348. [Google Scholar] [CrossRef] [PubMed]
- Hubschmid, U.; Leong-Morgenthaler, P.-M.; Basset-Dardare, A.; Ruault, S.; Frey, P. In vitro growth of human urinary tract smooth muscle cells on laminin and collagen type i-coated membranes under static and dynamic conditions. Tissue Eng. 2005, 11, 161–171. [Google Scholar] [CrossRef] [PubMed]
- Shaikh, F.M.; O’Brien, T.P.; Callanan, A.; Kavanagh, E.G.; Burke, P.E.; Grace, P.A.; McGloughlin, T.M. New pulsatile hydrostatic pressure bioreactor for vascular tissue-engineered constructs. Artif. Organs 2010, 34, 153–158. [Google Scholar] [CrossRef] [PubMed]
- Ahvaz, H.H.; Soleimani, M.; Mobasheri, H.; Bakhshandeh, B.; Shakhssalim, N.; Soudi, S.; Hafizi, M.; Vasei, M.; Dodel, M. Effective combination of hydrostatic pressure and aligned nanofibrous scaffolds on human bladder smooth muscle cells: Implication for bladder tissue engineering. J. Mater. Sci. Mater. Med. 2012, 23, 2281–2290. [Google Scholar] [CrossRef] [PubMed]
- Tiemessen, D.; De Jonge, P.; Daamen, W.F.; Feitz, W.; Geutjes, P.; Oosterwijk, E. The effect of a cyclic uniaxial strain on urinary bladder cells. World J. Urol. 2017, 35, 1531–1539. [Google Scholar] [CrossRef] [Green Version]
- Adamowicz, J.; Pasternak, I.; Kloskowski, T.; Gniadek, M.; Van Breda, S.V.; Buhl, M.; Balcerczyk, D.; Gagat, M.; Grzanka, D.; Strupinski, W.; et al. Development of a conductive biocomposite combining graphene and amniotic membrane for replacement of the neuronal network of tissue-engineered urinary bladder. Sci. Rep. 2020, 10, 5824. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Urinary diversions. 1 (left) uretero-ileo-cutaneostomy (ileal conduit). 2 (center) ileal neobladder (VIP). 3 (right) robotic neobladder (VesPa).
Figure 1.
Urinary diversions. 1 (left) uretero-ileo-cutaneostomy (ileal conduit). 2 (center) ileal neobladder (VIP). 3 (right) robotic neobladder (VesPa).

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Casarin, M.; Morlacco, A.; Dal Moro, F. Bladder Substitution: The Role of Tissue Engineering and Biomaterials. Processes 2021, 9, 1643. https://0-doi-org.brum.beds.ac.uk/10.3390/pr9091643
AMA Style
Casarin M, Morlacco A, Dal Moro F. Bladder Substitution: The Role of Tissue Engineering and Biomaterials. Processes. 2021; 9(9):1643. https://0-doi-org.brum.beds.ac.uk/10.3390/pr9091643
Chicago/Turabian StyleCasarin, Martina, Alessandro Morlacco, and Fabrizio Dal Moro. 2021. "Bladder Substitution: The Role of Tissue Engineering and Biomaterials" Processes 9, no. 9: 1643. https://0-doi-org.brum.beds.ac.uk/10.3390/pr9091643
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.