Impact of Different Types of Physical Activity in Green Urban Space on Adult Health and Behaviors: A Systematic Review

 ,
,  , , ,
, , ,  ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Method
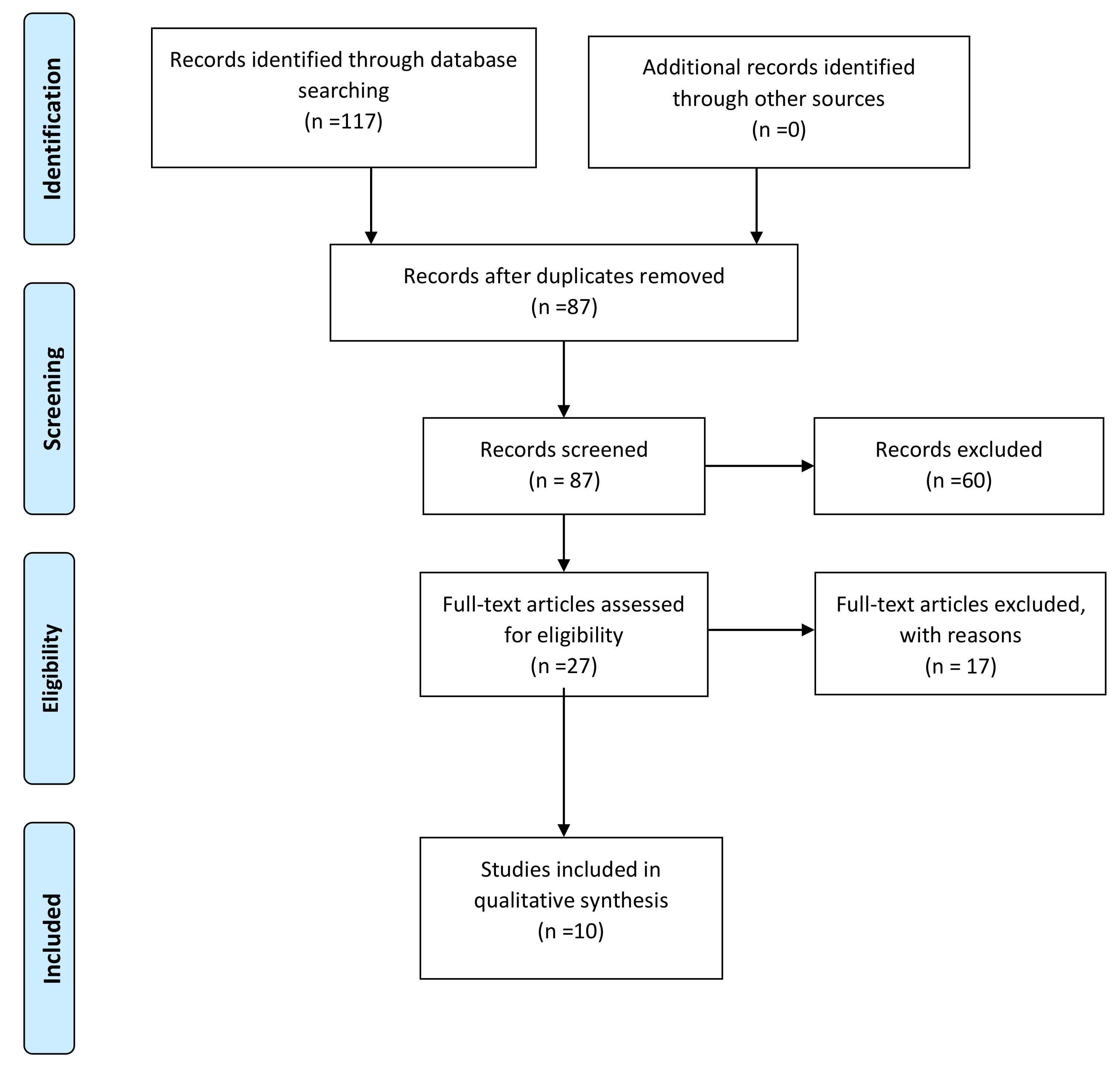
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Article Information
2.4. Effect Size and Treatment Effect
3. Results
3.1. Participant Characteristics
3.2. Impact of Outdoor Fitness on Participants’ Health
3.3. Impact of Green Spaces on Physical Activity Behaviors
3.4. Summary Statistics
4. Discussion
4.1. Limitations
4.2. Future Implication
5. Conclusions
6. Future Research Directions
Author Contributions
Funding
Conflicts of Interest
References
- Martine, G.; Marshall, A. State of World Population 2007: Unleashing the Potential of Urban Growth; UNFPA: New York, NY, USA, 2007. [Google Scholar]
- Dadvand, P.; Bartoll, X.; Basagana, X.; Dalmau-Bueno, A.; Martinez, D.; Ambros, A.; Cirach, M.; Triguero-Mas, M.; Gascon, M.; Borrell, C.; et al. Green spaces and general health: Roles of mental health status, social support, and physical activity. Environ. Int. 2016, 91, 161–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fong, K.C.; Hart, J.E.; James, P. A review of epidemiologic studies on greenness and health: Updated literature through. Curr. Environ. Health Rep. 2018, 5, 77–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nieuwenhuijsen, M.J.; Khreis, H.; Triguero-Mas, M.; Gascon, M.; Dadvand, P. Fifty shades of green: Pathway to health urban living. Epidemiology 2018, 28, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Shanahan, D.F.; Fuller, R.A.; Bush, R.; Lin, B.B.; Gaston, K.J. The health benefits of urban nature: How much do we need? BioScience 2015, 65, 476e485. [Google Scholar] [CrossRef] [Green Version]
- Wolf, K.L.; Robbins, A.S. Metro nature, environmental health, and economic value. Environ. Health Perspect. 2015, 123, 3990–3998. [Google Scholar] [CrossRef] [Green Version]
- Gong, Y.; Palmer, S.; Gallacher, J.; Marsden, T.; Fone, D. A systematic review of the relationship between objective measurements of the urban environment and psychological distress. Environ. Int. 2016, 96, 48–57. [Google Scholar] [CrossRef] [Green Version]
- Selander, J.; Nilsson, M.E.; Bluhm, G.; Rosssenlund, M.; Lindqvist, M.; Nise, G. Long term exposure to road traffic noise and myocardial infarction. Epidemiology 2009, 20, 272–279. [Google Scholar] [CrossRef]
- Basagaña, X.; Sartini, C.; Barrera-Gómez, J.; Dadvand, P.; Cunillera, J.; Ostro, B.; Sunyer, J.; Medina-Ramon, M. Heat waves and cause-specific mortality at all ages. Epidemiology 2011, 22, 765–772. [Google Scholar] [CrossRef]
- Hoek, G.; Krishnan, R.M.; Beelen, R.; Peters, A.; Ostro, B.; Brunekreef, B. Longtermair pollution exposure and cardio-respiratorymortality: A review. Environ. Health 2013, 12, 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gidlof-Gunnarsson, A.; Ohrstrom, E. Noise and well-being in urban residential environments: The potential role of perceived availability to nearby green areas. Landsc. Urban. Plan. 2007, 83, 115–126. [Google Scholar] [CrossRef]
- Uejio, C.K.; Wilhelmi, O.V.; Golden, J.S.; Mills, D.M.; Gulino, S.P.; Samenow, J.P. Intraurban societal vulnerability to extreme heat: The role of heat exposure and the built environment, socioeconomics, and neighborhood stability. Health Place 2011, 17, 498–507. [Google Scholar] [CrossRef] [PubMed]
- Dadvand, P.; de Nazelle, A.; Triguero-Mas, M.; Schembari, A.; Cirach, M.; Amoly, E.; Figueras, F.; Basagana, X.; Ostro, B.; Nieuwenhuijsen, M. Surrounding greenness and exposure to air pollution during pregnancy: An analysis of personal monitoring data. Environ. Health Perspect. 2012, 120, 1286–1290. [Google Scholar] [CrossRef]
- Dadvand, P.; Rivas, I.; Basagana, X.; Alvarez-Pedrerol, M.; Su, J.; De Castro Pascual, M.; Amato, F.; Jerret, M.; Querol, X.; Sunyer, J.; et al. The association between greenness and traffic-related air pollution at schools. Sci. Total Environ. 2015, 523, 59–63. [Google Scholar] [CrossRef]
- Rook, G.A. Regulation of the immune system by biodiversity from the natural environment: An ecosystem service essential to health. Proc. Natl. Acad. Sci. USA 2013, 110, 18360–18368. [Google Scholar] [CrossRef] [Green Version]
- Dzhambov, A.M.; Dimitrova, D.D. Urban green spaces’ effectiveness as a psychological buffer for the negative health impact of noise pollution: A systematic review. Noise Health 2014, 16, 157–165. [Google Scholar] [CrossRef] [PubMed]
- Shanahan, D.F.; Lin, B.B.; Bush, R.; Gaston, K.J.; Dean, J.H.; Barber, E.; Fuller, R.A. Toward improved public health outcomes from urban nature. Toward improved public health outcomes from urban nature. Am. J. Public Health 2015, 105, 470–477. [Google Scholar] [CrossRef] [PubMed]
- Bowler, D.E.; Buyung-Ali, L.M.; Knight, T.M.; Pullin, A.S. A systematic review of evidence for the added benefits to health of exposure to natural environments. BMC Public Health 2010, 10, 456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lachowycz, K.; Jones, A.P. Towards a better understanding of the relationship between greenspace and health: Development of a theoretical framework. Landsc. Urban Plan. 2013, 118, 62–69. [Google Scholar] [CrossRef]
- Hong, A.; Sallis, J.F.; King, A.C.; Conway, T.L.; Saelens, B.; Cain, K.L.; Fox, E.H.; Frank, L.D. Linking green space to neighborhood social capital in older adults: The role of perceived safety. Soc. Sci. Med. 2018, 207, 38–45. [Google Scholar] [CrossRef]
- Hallal, P.C.; Andersen, L.B.; Bull, F.C.; Guthold, R.; Haskell, W.; Ekelund, U. Global physical activity levels: Surveillance progress, pitfalls, and prospects. Lancet 2012, 380, 247–257. [Google Scholar] [CrossRef]
- Warburton, D.E.; Bredin, S.S. Health benefits of physical activity: A systematic review of current systematic reviews. Curr. Opin. Cardiol. 2017, 32, 541–556. [Google Scholar] [CrossRef]
- Löllgen, H.; Böckenhoff, A.; Knapp, G. Physical activity and all-cause mortality: An updated meta-analysis with different intensity categories. Int. J. Sports Med. 2009, 30, 213–224. [Google Scholar] [CrossRef]
- World Health Organization. Global Health Risks-Mortality and Burden of Disease Attributable to Selected Major Risks; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Annerstedt, M.; Ostergren, P.-O.; Björk, J.; Grahn, P.; Skärbäck, E.; Währborg, P. Green qualities in the neighbourhood and mental health—Results from a longitudinal cohort study in southern Sweden. BMC Public Health 2012, 12, 337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Department of Health and Social Care. Be Active Be Healthy; Department of Health and Social Care: London, UK, 2009.
- Gascon, M.; Triguero-Mas, M.; Martinez, D.; Dadvand, P.; Rojas-Rueda, D.; Plasencia, A.; Nieuwenhuijsen, M.J. Residential green spaces and mortality: A systematic review. Environ. Int. 2016, 86, 60–67. [Google Scholar] [CrossRef] [Green Version]
- Pretty, J.; Griffin, M.; Sellens, M.; Pretty, C. Green Exercise: Complementary Roles of Nature, Exercise and Diet in Physical and Emotional Wellbeing and Implications for Public Health Policy; University of Essex: Colchester, UK, 2003. [Google Scholar]
- Hartig, T.; Mang, M.; Evans, G.W. Restorative effects of natural environment experience. Environ. Behav. 1991, 23, 3–26. [Google Scholar] [CrossRef]
- Tester, J.; Baker, R. Making the playfields even: Evaluating the impact of an environmental intervention on park use and physical activity. Prev. Med. 2009, 48, 316–320. [Google Scholar] [CrossRef]
- Kaczynski, A.T.; Henderson, K.A. Parks and recreation settings and active living: A review of association with physical activity function and intensity. J. Phys. Act. Health 2008, 5, 619. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F.; Floyd, M.F.; Rodriguez, D.A.; Saelens, B.F. Role of built environments in physical activity, obesity and cardiovascular disease. Circulation 2012, 125, 729–737. [Google Scholar] [CrossRef] [PubMed]
- Kelly, B.; Fry, J. Camden Outdoor Gyms Evaluation: Phase 1; NHS Camden: London, UK, 2011. Available online: http://www.camdendata.info/ (accessed on 1 October 2020).
- Berke, E.M.; Koepsell, T.D.; Moudon, A.V.; Hoskins, R.E.; Larson, E.B. Association of the built environment with physical activity and obesity in older persons. Am. J. Public Health 2007, 97, 486–492. [Google Scholar] [CrossRef]
- Atkinson, J.L.; Sallis, J.F.; Saelens, B.E.; Cain, K.L.; Black, J.B. The association of neighborhood design and recreational environments with physical activity. Am. J. Health Promot. 2005, 19, 304–309. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, G.; Michael, Y.L. Concepts guiding the study of the impact of the built environment on physical activity for older adults: A review of the literature. Am. J. Health Promot. 2004, 18, 435–443. [Google Scholar] [CrossRef]
- Brownson, R.C.; Hoehner, C.M.; Day, K.; Forsyth, A.; Sallis, J.F. Measuring the built environment for physical activity: State of the science. Am. J. Prev. Med. 2009, 36 (Suppl. 1), S99–S123. [Google Scholar] [CrossRef] [Green Version]
- Li, F.Z.; Harmer, P.A.; Cardinal, B.J.; Bosworth, M.; Acock, A.; Johnson-Shelton, D.; Moore, J.M. Built environment, adiposity, and physical activity in adults aged 50±75. Am. J. Prev. Med. 2008, 35, 38–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Powell, K.E. Land use, the built environment, and physical activity: A public health mixture; a public health solution. Am. J. Prev. Med. 2005, 28 (Suppl. 2), 216–217. [Google Scholar] [CrossRef]
- Sallis, J.F. Measuring physical activity environments: A brief history. Am. J. Prev. Med. 2009, 36 (Suppl. 1), S86–S92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carlin, A.; Perchoux, C.; Puggina, A.; Aleksovska, K.; Buck, C.; Burns, C. A life course examination of the physical environmental determinants of physical activity behaviour: A “Determinants of Diet and Physical Activity” (DEDIPAC) umbrella systematic literature review. PLoS ONE 2017, 12, e0182083. [Google Scholar] [CrossRef]
- Brug, J.; van der Ploeg, H.P.; Loyen, A.; Ahrens, W.; Allais, O.; Andersen, L.F. Determinants of diet and physical activity (DEDIPAC): A summary of findings. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 150. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.; Li, F.; Li, J.; Zhang, Y. The relationship between urban parks, residents’ physical activity, an mental health benefits: A case study from Beijing, China. J. Environ. Manag. 2017, 190, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Miller, S.A. Four Elements of the Clinical Question: PICO Worksheet and Search Strategy. 2001. Available online: https://libguides.uthscsa.edu/ld.php?content_id=30804351.pdf (accessed on 1 November 2020).
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: New York, NY, USA, 1988. [Google Scholar]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. Introduction to Meta-Analysis; John Wiley & Sons, Ltd.: Edison, NJ, USA, 2009. [Google Scholar]
- Johnson, U.; Ivarsson, A.; Parker, J.; Andersen, M.J.; Svetoft, M. Connection in the fresh air: A study on the benefits of partecipation in an eletronic tracking outdoor gym exercise program. Monten. J. Sci. Med. 2019, 1, 61–67. [Google Scholar] [CrossRef]
- Astell-Burt, T.; Feng, X.; Kolt, G.S. Green space is associated with walking and moderate-to-vigorous physical activity (MVPA) in middle-to-older aged adults: Finding from 203 883 Australians in the 45 and up study. Br. J. Sports Med. 2014, 48, 404–406. [Google Scholar] [CrossRef] [PubMed]
- Cranney, L.; Phongsavan, P.; Kariuki, M.; Stride, V.; Scott, A.; Hua, M.; Bauman, A. Impact of an outdoor gym on park users’ physical activity: A natural experiment. Health Place 2016, 37, 26–34. [Google Scholar] [CrossRef]
- Schoffman, D.E.; Kaczynski, A.T.; Forthofer, M.; Wilcox, S.; Hutto, B.; Child, S.T.; Hughey, S.M. Longitudinal associations with changes in outdoor recreation area use for physical activity during a community-based intervention. Prev. Med. 2015, 78, 29–32. [Google Scholar] [CrossRef]
- Veitch, J.; Ball, K.; Crawford, D.; Abbott, G.R.; Salmon, J. Park Improvement and Park Actviity, a natural Experimetn. Am. J. Prev. Med. 2012, 42, 616–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marselle, M.R.; Irvine, K.N.; Lorenzo-Arribas, A.; Warber, S.L. Moving beyond Green: Exploring the relationship of environment type and indicators of perceived environmental quality on emotional well-being following group walks. Int. J. Environ. Res. Public Health 2015, 12, 106–130. [Google Scholar] [CrossRef]
- Apaychev, O.; Zakharina, I.; Hrybovska, I.; Pityn, M.; Hrybovskyy, R. Fitness correction of men using an “outdoor activity”. JPES 2018, 18, 2382–2388. [Google Scholar]
- Wu, L.; Wang, K.; Liao, P.; Kao, Y.; Huang, Y. Effects of an 8-week outdoor brisk walking program on fatigue in Hi-tech industry employees. Workplace Health Saf. 2015, 63, 436–445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, D.; Hoon, D.H.; Hong, S.; Jo, S.; Won, Y.; Jeon, J.Y. Six weeks of combined aerobic and resistance exercise using outdoor exercise machines improves fitness, insulin resistance and chemerin in the Korean elderly: A pilot randomized trial. Arch. Gerontol. Geriatr. 2018, 75, 59–64. [Google Scholar] [CrossRef]
- Cohen, D.A.; Williamson, S.; Golinelli, D.; McKenzie, T.L. Impact and Cost-Effectiveness of Family Fitness Zones: A Natural Experiment in Urban Public Parks. Health Place 2012, 18, 39–45. [Google Scholar] [CrossRef] [Green Version]
- Aparicio, E.H.; Rodríguez, E.F.; Marbán, R.M.; Minguet, J.L.C. Analysis of the public geriatric parks for elderly people in Málaga (Spain). Retos Nuevas tendencias en Educación Física. Deporte y Recreación 2010, 17, 99–102. [Google Scholar]
- American Geriatrics Society; British Geriatrics Society; American Academy of Orthopaedic Surgeons Panel on Falls Prevention. Guideline for the prevention of falls in older persons. J. Am. Geriatr. Soc. 2001, 49, 664–672. [Google Scholar] [CrossRef]
- Robertson, M.C.; Campbell, A.J.; Gardner, M.M.; Devlin, N. Preventing injuries in older people by preventing falls: A meta-analysis of individual-level data. J. Am. Geriatr. Soc. 2002, 50, 905–911. [Google Scholar] [CrossRef]
- Pratt, M.; Macera, C.A.; Wang, G. Higher direct medical costs associated with physical inactivity. Phys. Sportsmed. 2000, 28, 63–70. [Google Scholar] [CrossRef]
- Bettencourt, L.; Neves, R. Seniors’ playground and physical activity: Perceptions and practices. J. Aging Phys. Act. 2012, 20, S276. [Google Scholar]
- Cohen, A. Playgrounds for Seniors in Europe, Asia and North America 2010. Available online: http://www.athleticbusiness.com/articles/article.aspx?articleid=3609&zoneid=10 (accessed on 1 October 2020).
- Scott, A.; Stride, V.; Neville, L.; Hua, M. Design and promotion of an outdoor gym for older adults: A collaborative project. Health Promot. J. Aust. 2014, 25, 212–214. [Google Scholar] [CrossRef] [Green Version]
- Fujita, K.; Fujiwara, Y.; Cahves, P.; Motohashi, Y.; Shinkai, S. Frequency of going outdoors as a good predictor for incidents disability of physical function as well as disability recovery in community-dwelling older adults in rural Japan. J. Epidemiol. 2006, 16, 261–270. [Google Scholar] [CrossRef] [Green Version]
- DiPietro, L.; Al-Ansari, S.S.; Biddle, S.J.; Borodulin, K.; Bull, F.C.; Buman, M.P.; Willumsen, J.F. Advancing the global physical activity agenda: Recommendations for future research by the 2020 WHO physical activity and sedentary behavior guidelines development group. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 1–11. [Google Scholar] [CrossRef]
- Lee, I.; Buchner, D.M. The importance of walking to public health. Med. Sci. Sports Exerc. 2008, 40, S512–S518. [Google Scholar] [CrossRef]
- Lee, I.M.; Rexrode, K.M.; Cook, N.R.; Manson, J.E.; Buring, J.E. Physical activity and coronary heart disease in women: Is ‘‘no pain, no gain’’ passe? JAMA 2001, 285, 1447–1454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simpson, M.E.; Serdula, M.; Galuska, D.A.; Gillespie, C.; Donehoo, R.; Macera, C.; Mack, K. Walking trends among US adults: The Behavioral Risk Factor Surveillance System, 1987–2000. Am. J. Prev. Med. 2003, 25, 95–100. [Google Scholar] [CrossRef]
- Furber, S.; Pomroy, H.; Grego, S.; Tavener-Smith, K. People’s experiences of using outdoor gym equipment in parks. Health Promot. J. Aust. 2014, 25, 211. [Google Scholar] [CrossRef] [Green Version]
- Greyling, G.A. The Usage of Outdoor Gyms in South Africa. MBA Thesis, Nelson Mandela Metropolitan University, Port Elisabeth, South Africa, 2016. [Google Scholar]
- The Trust for Public Land. Fitness Zone Program: From Miami to Los Angeles, There Are 68 Fitness Zone Areas Already in Use Ðand More on the Way 2015. Available online: http://www.tpl.org/our-work/parks-people/fitness-zone-area (accessed on 1 December 2020).
- Chow, H.-W. Need Assessment and Health Evaluation of Seniors Use of Local Parks; National Science Council: Taipei, Taiwan, 2012.
- Mora, R. Moving bodies: Open gyms and physical activity in Santiago. J. Urban Des. 2012, 17, 485–497. [Google Scholar] [CrossRef]
- Aparicio, E.H. Study biosaludables circuits for seniors in Spain: A study of geriatric parks for erderly people in Spain. Int. J. Med. Sci. Phys. Act. Sport 2009, 9, 25–38. [Google Scholar]
- Chow, H. Outdoor fitness equipment in parks: A qualitative study from older adults’ perception. BMC Public Health 2013, 13, 1216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Government of Western Australia. Public Parkland Planning and Design Guide WA; Department of Sport and Recreation: Perth, Australia, 2014.
- Chow, H.; Ho, C. Does the use of outdoor fitness equipment by older adults qualify as moderate to vigorous physical activity? PLoS ONE 2018, 13, e0196507. [Google Scholar] [CrossRef] [Green Version]
- Chow, H.; Wu, D. Outdoor fitness equipment usage behaviors in natural settings. Int. J. Environ. Res. Public Health 2019, 16, 391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xie, J. An analysis of the injury accidents of fitness route in non-central city, Sichuan Province. Sports Cult Guide 2012, 10, 82–84. [Google Scholar]
- Yan, J. Common problems analysis of outdoor fitness equipment. Technol. Wind 2016, 19, 104. [Google Scholar]
- Copeland, J.L.; Currie, C.; Walker, A.; Mason, E.; Willoughby, T.N.; Amson, A. Fitness equipment in public parks: Frequency of use and community perception in a small urban center. J. Phys. Act. Health 2017, 17, 485–497. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Population | Healthy adults (18 ≤ age ≤ 80) | People < 18 or >80 |
| Unhealthy people | ||
| Intervention | PA in green urban spaces and gym equipment installation | PE indoors or in different natural environments such as beaches or blue areas |
| Comparator | Control group (if presented); baseline observation; park with no gym equipment | Participants receiving different protocol from PA |
| Outcome | Impact of PE in green urban spaces and/or PA and health indicators and behavior characteristics of park users | No information about PA |
| Study design | Observational or experimental with original primary data | Study protocols or other papers without original data |
| English language | Not in English language | |
| Timing | No time restrictions until 10 June 2020 | After 10 June 2020 |
| Study | Country | Participants | Age (yrs.) | Gender |
|---|---|---|---|---|
| Veitch et al. (2012) | Australia | 1309 | ≥18 | M and F |
| Cohen et al. (2012) | USA | 2636 | 40 ± 12.5 * | F = 61%; M = 39% |
| Wu et al. (2015) | Taiwan | 86 | 31.28 ± 4.93 * | F = 50%; M = 50% |
| Johnson et al. (2019) | Sweden | 6 | 41.2 ± 6.5 * | F = 33%; M = 67% |
| Apaychev et al. (2018) | Ukraine | 60 | 40–50 | M |
| Schoffman et al. (2015) | USA | 295 | 49.4 ± 13.3 * | F = 86%; M = 14% |
| Marselle et al. (2015) | UK | 127 | 55–74 | F = 55.5%; M = 44.5% |
| Astell-Burt et al. (2013) | Australia | 203883 | 61.5 * | F = 53.2%; M = 46.8% |
| Cranney et al. (2015) | Australia | 796 | ≥18 | F = 47.6%; M = 52.4% |
| Kim et al. (2018) | Korea | 35 | 73.2 ± 4.95 | F = 91.5%; M = 8.5% |
| Study | Design | EG | CG | Other Group | Treatment | Duration | Cohen’s d | Hedge’s g | p-Value | Measurements | Analysis |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Wu et al. (2015) | RCT | 41 | 45 | no | Walking program | 8 weeks | 1.325 | 1.313 | 0.0005 | Overall fatigue | Stand. Mean diff. |
| Schoffman et al. (2015) | CT | Cross-sectional | Walking program | 6 months | 1.036 | 1.02 | 0.007 | %Weekly MVPA | Correlation coefficient | ||
| 194 | no | 6.08 | 5.99 | >0.001 | Self-efficacy | ||||||
| Marselle et al. (2015) | CT | Pre | Post | Walking program | 13 weeks | 2 | 1.99 | >0.001 | Walk happiness | Correlation coefficient | |
| 127 | 127 | no | |||||||||
| Apaychev et al. (2018) | CT | EC | CG | Outdoor activity | 6 months | 4.02 | 3.03 | >0.001 | Motor activity | Stand. Mean diff. | |
| 20 | 20 | no | |||||||||
| Johnson et al. (2019) | CT | Pre | Post | Outdoor activity | 10 weeks | 1.08 | 0.99 | 0.004 | Number of steps | Stand. Mean diff. | |
| 6 | 6 | no | 0.83 | 0.76 | 0.02 | Cardiovascular fitness | |||||
| Kim et al. (2018) | RCT | EG1 | CG | EG2 | Outdoor activity | 6 weeks | 0.4 | 0.385 | 0.017 | Number of push-ups | Stand. Mean diff. |
| 12 | 10 | 13 | 0.41 | 0.395 | 0.0003 | 6-min walk | |||||
| Study | Design | Participants | Exercise Type | Duration | Cohen’s d | Hedge’s g | p-Value | Outcome | Measurements | Analysis |
|---|---|---|---|---|---|---|---|---|---|---|
| Astell-Burt et al. (2013) | OBS | 203883 | Walking and MVPA | not specified | 1.98 | 1.98 | >0.001 | Impact of distance on park usage | Walking near green space | Odds ratio difference |
| 1.97 | 1.97 | >0.001 | MVPA near green space | |||||||
| Cranney et al. (2015) | OBS | 358 | Outdoor gym | 12 months | 2.63 | 2.63 | >0.03 | Impact of gym installation on park usage | MVPA frequency pre–post | Proportion difference |
| Cohen et al. (2012) | OBS | 958 | Outdoor gym | 16 months | 0.61 | 0.61 | >0.0001 | Exercise in gym park vs. no gym park | Exercise frequency | Proportion difference |
| Veitch et al. (2012) | OBS | 609 | Outdoor gym | 12 months | <7 | <7 | >0.0001 | Impact of gym installation on park usage | Usage frequency pre–post | Proportion difference |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grigoletto, A.; Mauro, M.; Maietta Latessa, P.; Iannuzzi, V.; Gori, D.; Campa, F.; Greco, G.; Toselli, S. Impact of Different Types of Physical Activity in Green Urban Space on Adult Health and Behaviors: A Systematic Review. Eur. J. Investig. Health Psychol. Educ. 2021, 11, 263-275. https://0-doi-org.brum.beds.ac.uk/10.3390/ejihpe11010020
Grigoletto A, Mauro M, Maietta Latessa P, Iannuzzi V, Gori D, Campa F, Greco G, Toselli S. Impact of Different Types of Physical Activity in Green Urban Space on Adult Health and Behaviors: A Systematic Review. European Journal of Investigation in Health, Psychology and Education. 2021; 11(1):263-275. https://0-doi-org.brum.beds.ac.uk/10.3390/ejihpe11010020
Chicago/Turabian StyleGrigoletto, Alessia, Mario Mauro, Pasqualino Maietta Latessa, Vincenzo Iannuzzi, Davide Gori, Francesco Campa, Gianpiero Greco, and Stefania Toselli. 2021. "Impact of Different Types of Physical Activity in Green Urban Space on Adult Health and Behaviors: A Systematic Review" European Journal of Investigation in Health, Psychology and Education 11, no. 1: 263-275. https://0-doi-org.brum.beds.ac.uk/10.3390/ejihpe11010020