
Strike a Balance: Between Metals and Non-Metals, Metalloids as a Source of Anti-Infective Agents


1
Department of Pharmacy, University of Pisa, Via Bonanno Pisano 6, 56126 Pisa, Italy
2
Inter-University Consortium for Research on the Chemistry of Metal Ions in Biological Systems, Via C. Ulpiani 27, 70126 Bari, Italy
*
Authors to whom correspondence should be addressed.
Inorganics 2021, 9(6), 46; https://0-doi-org.brum.beds.ac.uk/10.3390/inorganics9060046
Submission received: 6 May 2021
/
Revised: 24 May 2021
/
Accepted: 25 May 2021
/
Published: 4 June 2021
(This article belongs to the Special Issue Metal-Based Antimicrobials)
Abstract
:Most of the commercially available anti-infective agents are organic molecules. In fact, though, during the pioneering times of modern medicine, at the beginning of the 20th century, several inorganic compounds of transition metals were used for medicinal application, to date, only a small number of inorganic drugs are used in clinical practice. Beyond the transition metals, metalloids—or semimetals—offer a rich chemistry in between that of metallic and non-metallic elements, and accordingly, peculiar features for their exploitation in medicinal chemistry. A few important examples of metalloid-based drugs currently used for the treatment of various diseases do exist. However, the use of this group of elements could be further expanded on the basis of their current applications and the clinical trials they entered. Considering that metalloids offer the opportunity to expand the “chemical-space” for developing novel anti-infective drugs and protocols, in this paper, we briefly recapitulate and discuss the current applications of B-, Si-, As-, Sb- and Te-based anti-infective drugs.
1. Introduction
Metals have been used since ancient times to cure several diseases. With the progress of modern medicine, a number of metal-based agents were then evaluated on scientific basis for applications against a variety of parasites, bacteria and viruses responsible for life-threatening diseases [1,2,3]. Subsequently, the interest in metals in medicine was further fueled by the serendipitous discovery of the anticancer properties of cisplatin. To date, this simple Pt-based molecule—together carboplatin and oxaliplatin—is a cornerstone worldwide for the treatment of malignances [4,5,6,7]. These molecules impact the clinical practice with a role that, at present, is not replaceable by organic compounds. Overall, the success of Pt-based therapeutics spurred a very intense activity of the scientific community aiming to develop novel and ameliorated inorganic chemotherapeutics capable to overcome the existing limitations of established clinical protocols [8,9,10,11]. Even recently, the sudden emergence represented by the SARS-CoV-2 virus, posed the dramatic problem of the rapid development of drugs against this global threat, renewing the interest on approved inorganic therapeutics. Accordingly, Au, Bi, Sb- based complexes were suggested as potentially suitable for the inhibition of viral replication and spreading in the frame of various drug-repurposing programs [12,13,14,15].
These considerations support transition metals as a rich source for novel drugs, indicating the contribution that medicinal inorganic chemistry may offer [16].
Beyond transition metals, the so-called metalloids—even known as semimetals—represent an interesting group of elements endowed with unique features in between those of metals and non-metals. It is beyond the scope of this article to comprehensively describe the chemistry of metalloids, their reactivity profile and the chemical features; nevertheless, it may be useful for the readers to delineate the main properties of this class of elements. When we refer to “metalloids”, we deal with a group of six elements arranged along the diagonal line from boron, also including silicon, germanium, arsenic, antimony and tellurium. It is worthwhile to remember that this categorization is not exclusive or exhaustive and, depending on the authors, other elements might be considered as metalloids (e.g., Po, Ga) [17,18]. These elements share common properties as reported in 1977 by Masterton and Slowinski [17]. These authors highlighted that metalloids typically have first ionization potentials (IP) falling around 200 kcal/mol, accompanied by electronegativity (EN) values of ≈2.0. Additionally, metalloids generally behave as semiconductors with an important application in the field of technology (Table 1).
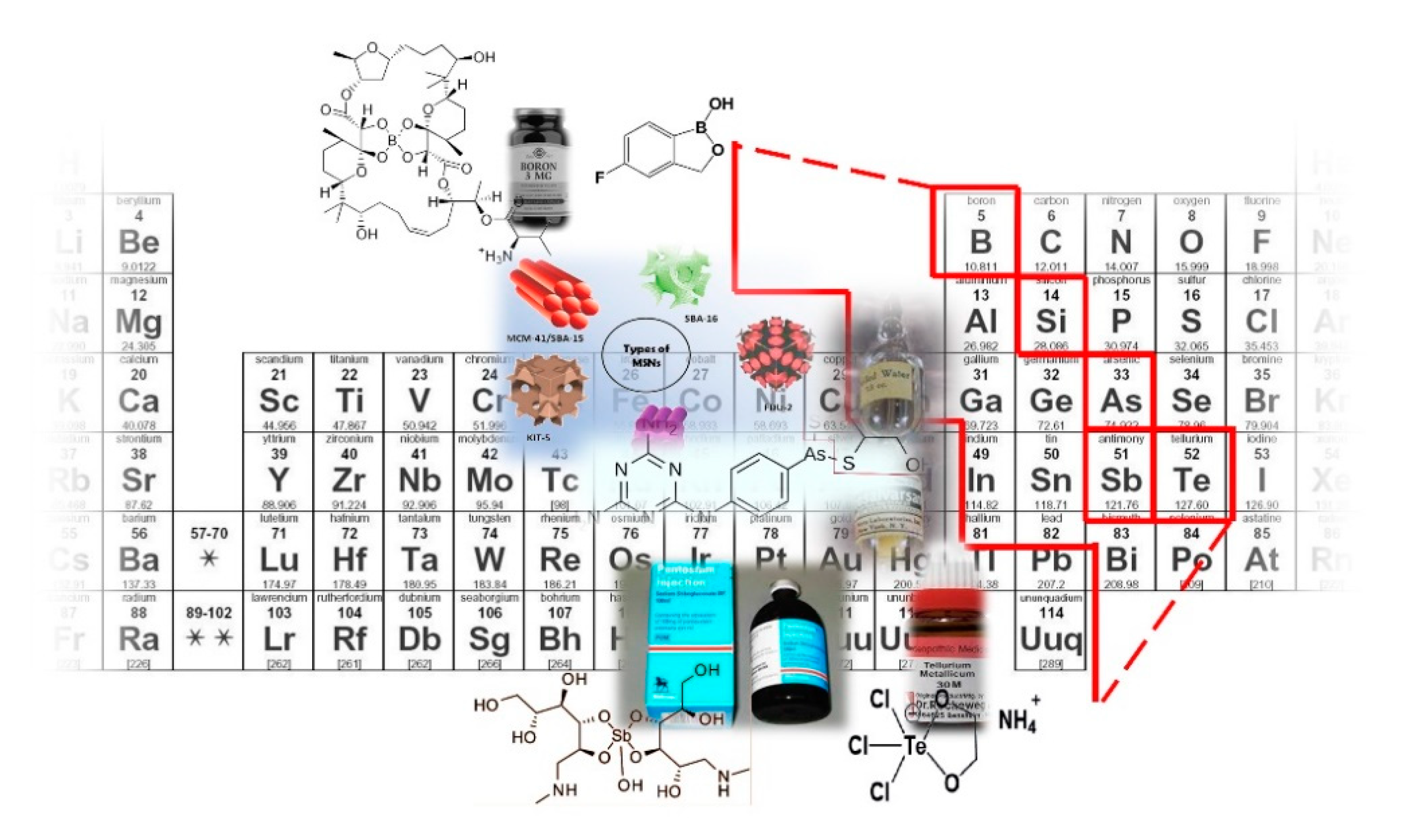
As stated above, while the physicochemical properties of these elements are widely exploited for technology and industrial purposes, less is known on their use in medicine. Metalloids and metalloid-based compounds, owing to their properties, can exert biological activity toward cells and tissues. Hence, even long before the development of the modern inorganic medicinal chemistry, metalloid compounds were used to treat various diseases on empirical basis (Figure 1).
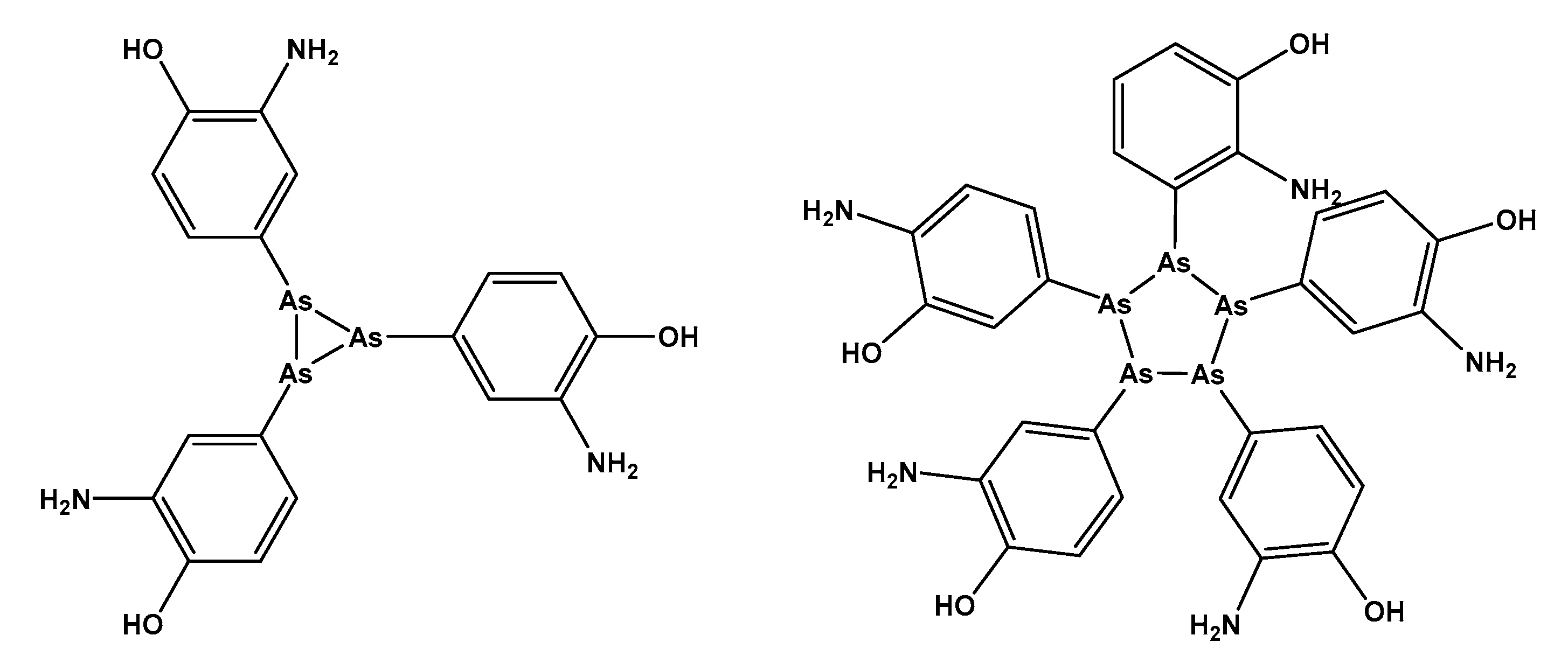
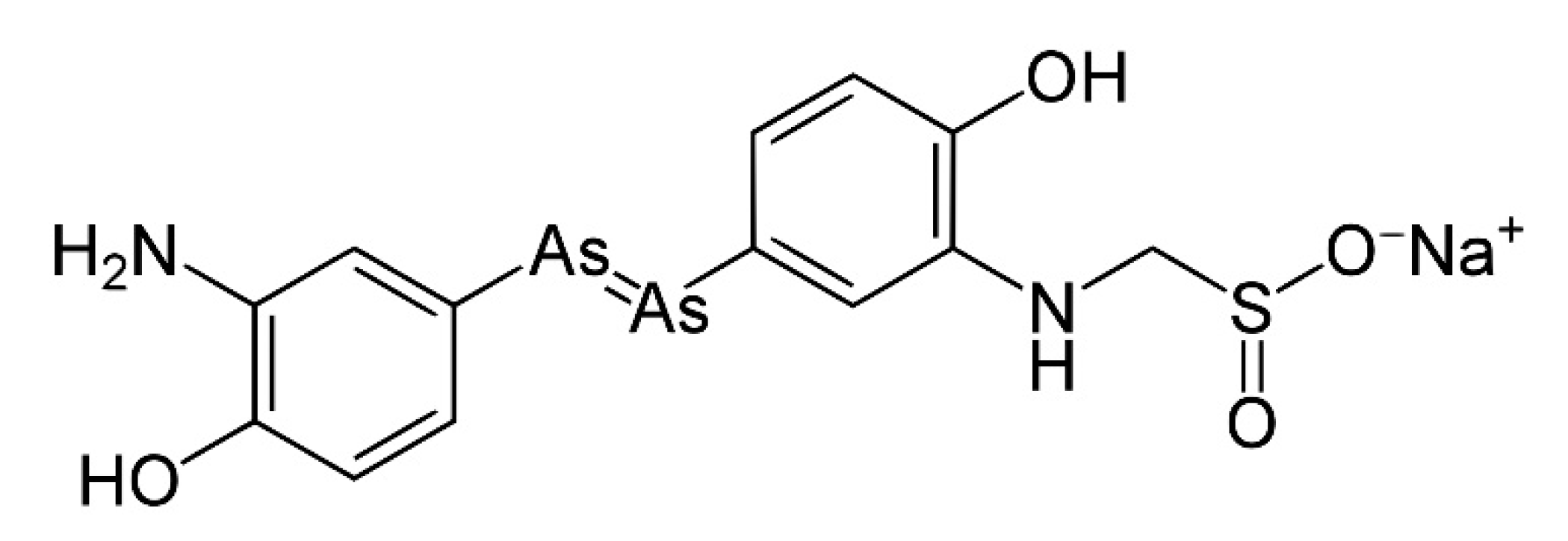
The mixture of 3-amino-4-hydroxyphenyl-AsIII compounds containing acyclic As3 and As5 species (Salvarsan®) (Hoechst AG, Frankfurt, Germany) [19] was introduced by Ehrlich in the early 20th century and marketed as a treatment for syphilis, an event that has marked the beginning of the modern chemotherapy (Figure 2) [8].
According to the above considerations, here we try to summarize some of the indications and the clinical trials that metalloid-containing agents entered for their application in antiparasitic, antibacterial, antifungal, or antiviral therapy. Additionally, we briefly discuss the challenges and the prospects for translating metalloid compounds in further preclinical and clinical development. Specifically, we report on some relevant anti-infective agents containing B, Si, As, Sb and Te. Indeed, using these elements, molecules that were approved, or that entered clinical trials were developed, while -to the best of our knowledge- no Ge-based drugs reached advanced stages of clinical testing neither approval.
2. Boron
The design of pharmacologically-active molecules containing boron is a relatively recent field of research, and accordingly, the use of this element is still largely unexplored. Boron has a very peculiar chemistry. Its position in the periodic table is close to nitrogen and carbon, two elements that form “the chemical backbone of life” [20]. Boron behaves as a strong Lewis acid, is characterized by an empty p-orbital and has an electrophilic character. Owing to the empty p-orbital, it can form coordinate covalent bonds with biological nucleophiles, interacting with enzymes bearing hydroxyl and amine groups, but also with carbohydrates and nucleic acids [21]. Additionally, the boron center, under physiological environment, can switch from sp2 (trigonal planar) to sp3 hybridization corresponding to tetrahedral geometry [22].
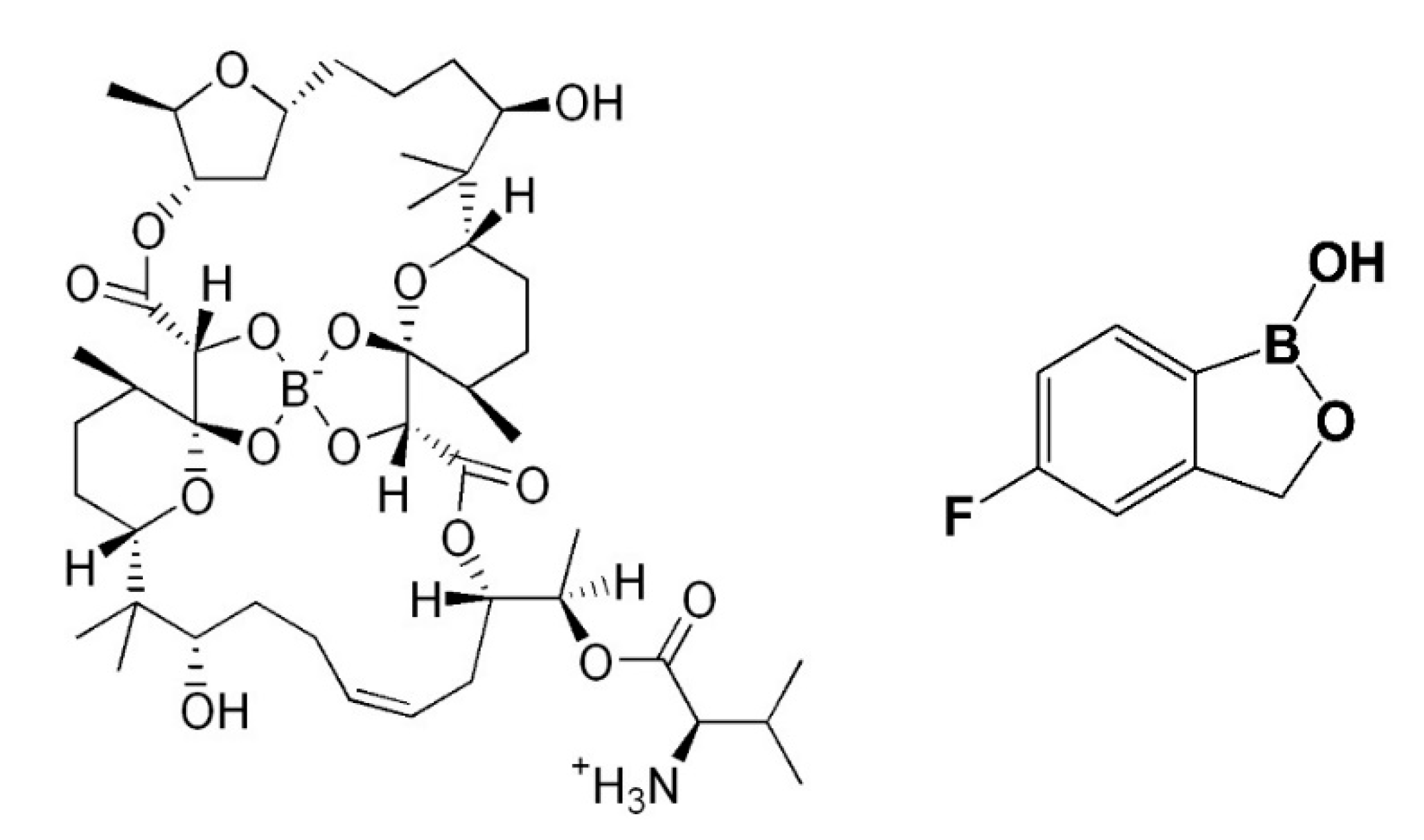
Boromycin, isolated from a fermentation broth of Streptomyces sp. A-3376, was the first natural compound found to contain boron (Figure 3). This polyether-macrolide antibiotic elicits potent activity as anti-human immunodeficiency virus (HIV) with a mechanism likely involving the blocking of the later stage of HIV infection, as well as the replication stages [23]. It was also shown to be active against Gram-positive bacteria, but not against Gram-negative strains. This difference in the activity is likely due to the outer membrane of Gram-negative bacteria capable of blocking the access of the molecule to the cytoplasmic membrane. Recent studies reported boromycin as active against Mycobacterium tuberculosis, the pathogen responsible for the tuberculosis disease. Boromycin is a potent inhibitor of the growth of this bacterium with a MIC50 = 80 nM (MIC—Minimum Inhibitory Concentration). Interestingly, its cytotoxicity and hemolytic activity are very low with a selectivity index of more than 300, indicating a favorable pharmacological profile [24].
Despite boromycin not being currently approved for clinical use, three other boron-based molecules were approved by the Food and Drug Administration (FDA), namely, crisaborole, bortezomib and tavaborole, as treatment for atopic dermatitis, multiple myeloma and onychomycosis, respectively. The latter is a fungal infection of the nails, caused by a number of different types of fungus including dermatophytes of the genus Trichophyton [25]. Tavaborole, sold under the brand Kerydin®, Pfizer, New York, NY, USA, (Figure 3), is the only boron-containing anti-infective agent currently used in clinical practice [21].
Tavaborole, approved by the FDA in 2014, entered several clinical trials aiming to assess the pharmacokinetic safety of the dosages, as well as the efficacy when topically administered against onychomycosis in children, adolescents and adults. Tavaborole has a unique mechanism of action and it is highly specific against pathogenic fungi. It is important to highlight that its antifungal activity strictly depends on the presence of the boron center. Indeed, tavaborole analogs bearing a carbon in place of the boron were synthesized and tested, showing no pharmacological activity [26].
Specifically, tavaborole interferes with protein synthesis in fungal cells by targeting and impairing fungal cytoplasmic leucyl-transfer ribonucleic acid (tRNA) synthetase. This enzyme belongs to the Aminoacyl-tRNA synthetases (AARSs) family, performing a key role in translating the genetic code by catalyzing the attachment of the proper amino acid to its cognate tRNA. Accordingly, they have a crucial role in the protein synthesis [27]. Interestingly, tavaborole has an affinity for fungal leucyl-tRNA synthetase that is >1000-fold higher than for the human leucyl-tRNA synthetase, ensuring safety and tolerability [28]. Some of the clinical trials involving tavaborole are summarized in Table 2 with the main details.
The low molecular weight of the molecule ensures good penetration in the infected nails. The penetration is also improved when administered as 5% solution, despite clinical trials which have comparatively assessed the efficacy for doses ranging from 2.5% up to 7% prepared with a mixture of ethyl acetate and propylene glycol [29].
3. Silicon
Silicon is among the most abundant element in the universe, though it is rarely found in its pure form. It is the element that presents the closest similarities with carbon. Both can form tetravalent compounds. Silicon has a larger covalent radius compared with that of carbon. At variance with carbon, silicon can form five or six coordinated compounds. Even this aspect accounts for a different reactivity from carbon [30,31]. Some of the main differences between carbon and silicon leading to diversity in the pharmacological properties of the silicon-containing analogs are molecular size and shape, electronegativity, and lipophilicity. Indeed, C–C bond is 1.54 Å while the length in C–Si bond is about 1.87 Å. This subtle difference may dramatically affect the interaction with biomolecules—and eventually the pharmacological profile of Si-containing compounds compared with C-containing counterpart. Additionally, Si is more electropositive than carbon, and the hydrogen-bond strength of the silanol is more favorable as a donor than that of the carbinol. Thus, in the drugs containing carbinol acting as hydrogen-bond donor, the replacement of the latter with the silanol moiety represents a suitable strategy to improve the efficacy [32,33]. The higher lipophilicity of Si compared with carbon could result in improved bioavailability and pharmacokinetics of the Si-containing drug analogs [33]. Owing to the aforementioned features, a number of organosilanes entered human clinical trials as anticancer agents and muscle relaxants, as well as drugs for Alzheimer’s disease. However, to the best of our knowledge, despite a number of silicon-based compounds which were synthesized and tested as anti-infective agents, none of them entered clinical trials [34].
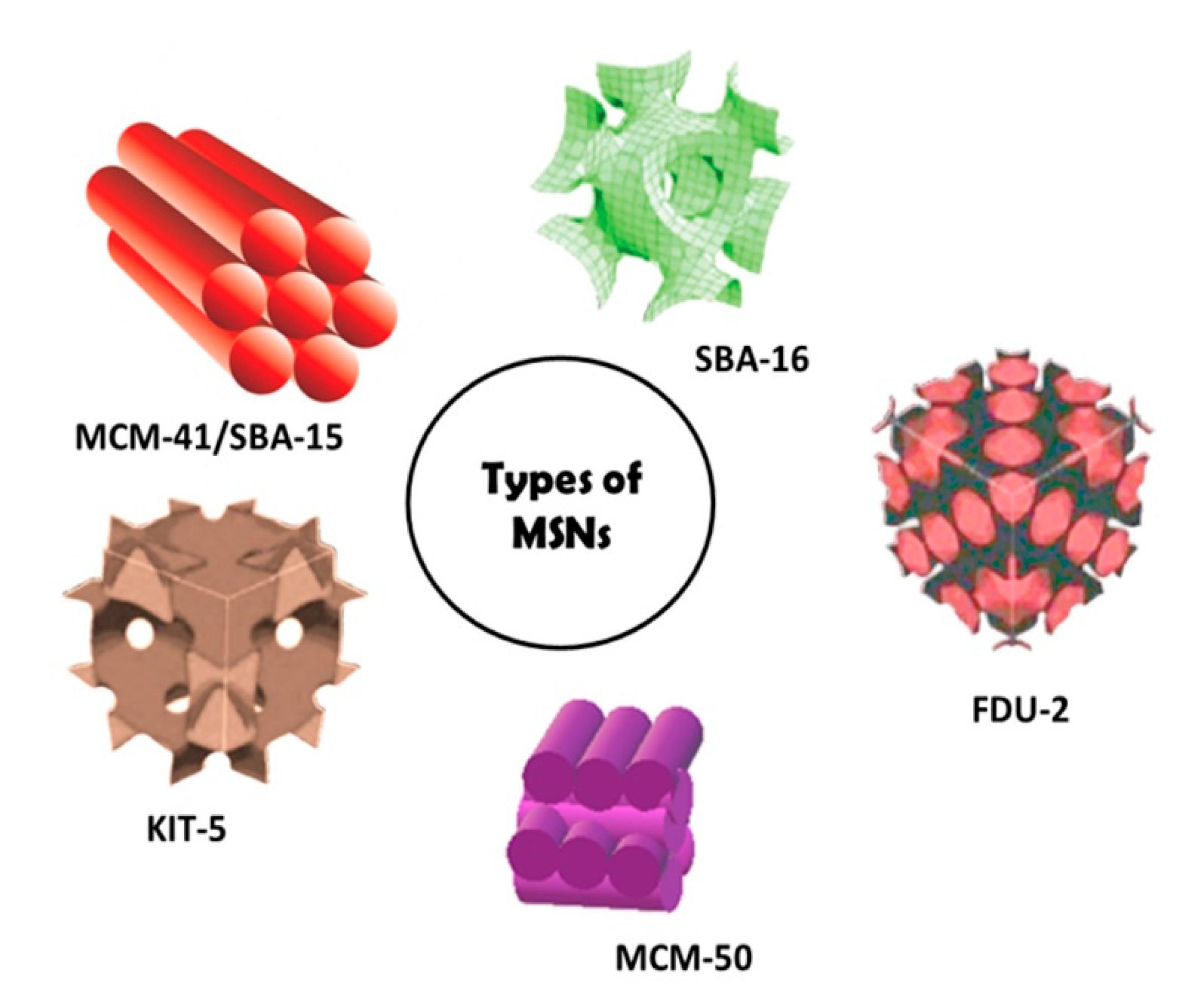
Various Si-containing substances find use in the preparation of medicaments, medical devices, cosmesis and drugs for different indications. Magnesium trisilicate is used as an anti-acid similarly to magnesium aluminum silicate, whereas polydimethylsiloxane (PDMS) is exploited for the production of contact lenses, as an ingredient in preparations for the treatment of irritated eyes and, more in general, in various medical devices [35,36]. To date, one of the most important roles of silicon concerns the synthesis of biocompatible nanoparticles (NPs) as a smart platform for drug delivery (Figure 4). Indeed, the solubility of a drug can be conveniently improved due to the polar surface of the nanostructures. Additionally, the loaded pharmacologically-active agents can be released in a controlled manner [37,38].
Additionally, these NPs can be loaded with anti-infective drugs or can be themselves endowed with antibacterial or antivirus properties [39,40].
Recently, the FDA approved the first hybrid silica nanoparticles for bioimaging, confirming the suitability of these inorganic structures for medicinal purpose [41]. In 2018, Smirnov et al. reported on the antibacterial activity of spherical Si-NPs against Gram-positive and Gram-negative strains (S. aureus and P. aeruginosa respectively) [42]. These NPs were prepared through nanosecond laser ablation techniques, starting from solid silicon. The preparation was carried out in various media including distilled water and isopropyl alcohol. The antibacterial effect was apparently the consequence of the photodynamic activity of the silicon nanoparticles caused by the production of singlet oxygen on their surface [42,43]. Zhou et al. described a high-performance silicon-based antibacterial material wafer made of silver nanoparticle (AgNP)-decorated silicon wafers (AgNP@Si). Compared with free AgNPs, this substrate has shown markedly enhanced antibacterial properties against E. coli that are retained over 30 days. An additional advantage of this material is the rapid and simple preparation relying on the treatment of a wafer of Si in the presence of 5% HF acidic conditions. Next, the wafer is placed in a freshly prepared solution of AgNO3 affording the desired material. Overall, the authors concluded that AgNP@Si coating can act as an “antibacterial surface” to impair the formation of harmful biofilms. In addition, these materials are potentially useful for the development of antibacterial surfaces endowed with high biocompatibility [40].
4. Arsenic
Arsenic is a bright silver-gray element known since very ancient times. Indeed, its name derives from the Greek word ‘‘arsenikon’’ (potent) and several early authors reported on its medicinal properties. In the 5th century A.D., Olympiodorus described the production of arsenic oxide—As2O3. Many alchemists considered arsenic oxide, similarly to sulfur, to be a basic constituent of metals. More recently, the early physician Paracelsus (1493–1541) suggested the use of arsenic for some diseases, and between the middle of the 17th and 18th century, two methods for the preparation of As2O3 were described [44].
Interestingly, among the metalloids, As has a fascinating history. Indeed, on the one hand, its medicinal properties were known since centuries; on the other, it is well known as poison [45,46,47]. Nevertheless, arsenic compounds are currently used in clinical practice for some indications. Particularly important is the case of As2O3, approved by the FDA in 2003 and marketed under the name Trisenox® (Almac Pharma Services Limited, United Kingdom; Almac Pharma Services, Ireland; Teva Pharmaceuticals Europe, The Netherlands). This drug is used to treat acute myeloid leukemia [48].
Organoarsenical compounds also represented a cornerstone in the treatment of bacterial infections. In particular, until the discovery of Salvarsan® and Neosalvarsan® (Hoechst AG, Frankfurt, Germany) by the Nobel Laureate Paul Ehrlich at the beginning of the 1900s, syphilis was a major and often deadly infection (Figure 1 and Figure 5) [45].
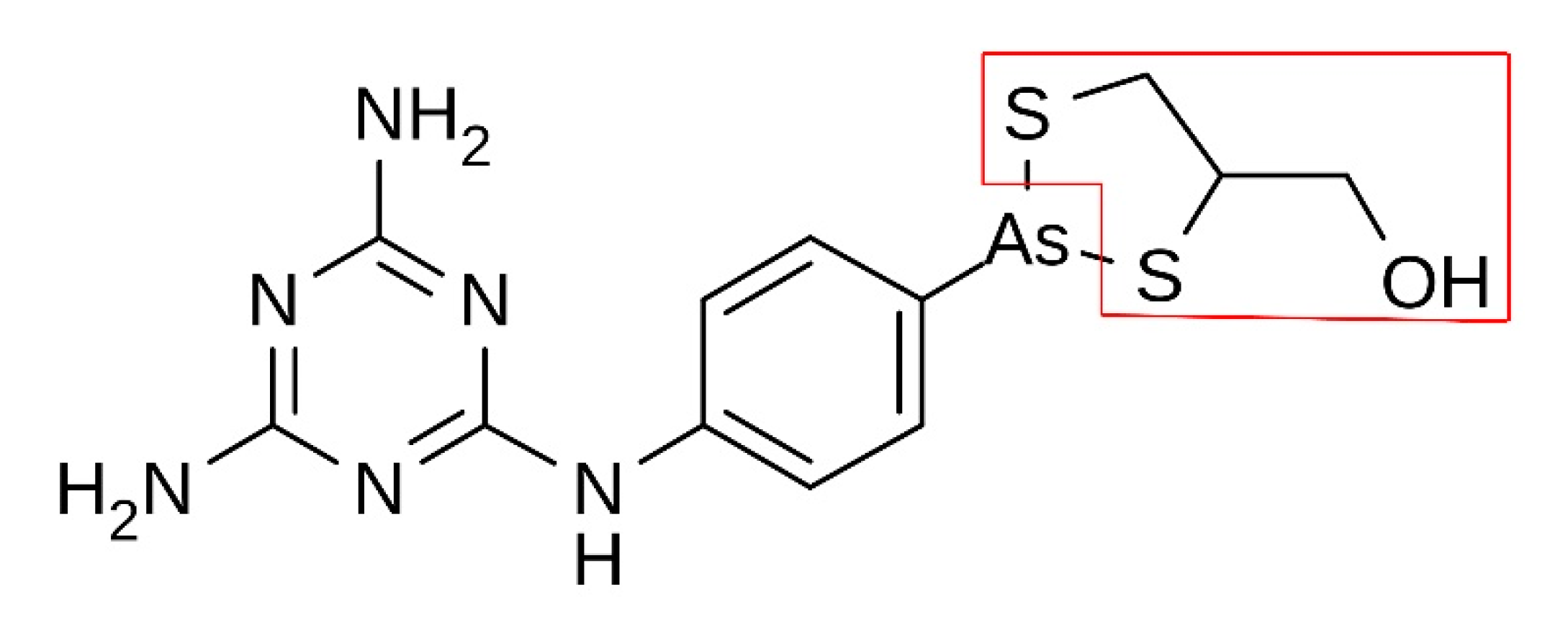
Melarsoprol (Arsobal®, Sanofi, Paris, France) (Figure 6) was introduced in 1949 as the first agent effective in the treatment of Human African trypanosomiasis (HAT, also known as sleeping sickness, transmitted through the bite of infected tsetse flies). This is a neglected tropical disease caused by the protozoan parasites Trypanosoma brucei gambiense (endemic in West and Central Africa) and Trypanosoma brucei rhodesiense (endemic in Eastern and Southern Africa) [49]. African trypanosomiasis caused devastating epidemics in the 20th century, killing millions of people. The disease typically has two stages: a hemolymphatic stage (in which the parasite proliferates in the hemolymphatic system of the host), subsequently, in the meningoencephalitic stage, trypanosomes cross the blood–brain barrier, invading the central nervous system (CNS) and causing neurological disturbances. Among them, sleeping sickness is typical of the second stage [50]. The sleep disorder, from which the name sleeping sickness derives, is not the only consequence of the infection, and several additional problems occur in the advanced stages of the disease including heavy neuropsychiatric symptoms, renal and cardiac failure [50,51].
In the chemical structure of melarsoprol, the As (III) is celated by 2,3-dimercaptopropanol (a compound originally developed as anti-Lewisite molecule, Figure 6) [52].
When administered to patients, melarsoprol is rapidly converted into its pharmacologically-active form, i.e., melarsen oxide, capable of binding serum proteins [53]. The actual mechanism of action of melarsoprol has not been fully understood. However, arsenic is well known to be a promiscuous inhibitor of several different enzymes and biological targets containing thiol groups, and the pharmacological effects of this drug against the pathogen could result from the uptake into the parasite by the trypanosomal P2-purine transporter [54]. Notably, an important enzyme affected by the drug is the trypanothione reductase of the parasite, whose impairment leads to the loss of the redox balance [55]. However, the inhibition of multiple targets and biochemical pathways is likely to determine the pharmacological effects [56,57]. Nevertheless, the use of this important drug is accompanied by heavy—and even fatal—side effects. Owing to its very poor solubility in water media, it is administered intravenously as propylene glycol solution, being this solvent an irritant for tissues. Among various additional side effects including vomiting and peripheral neuropathy, another drawback is reactive encephalopathy, occurring in 5–10% of cases, half of which are characterized by extremely poor prognosis. Importantly, the currently used therapeutic protocols were developed on the basis of trial-and-error approaches. In this view, various pharmacokinetic research suggested that the currently used doses are not optimal and should be improved [52].
Melarsoprol in 2006 entered a clinical trial to assess its efficacy in combinatory therapy: three drug combinations were tested, i.e., melarsoprol 1.8 mg/kg/day, 10 days + nifurtimox 15/20 mg/kg/day, 10 days; melarsoprol 1.8 mg/kg/day, 10 days + eflornithine 400 mg/kg/day, 7 days, and nifurtimox 15/20 mg/kg/day, 10 days + eflornithine 400 mg/kg/day, 7 days, for Late-Stage Gambiense Human African Trypanosomiasis (ClinicalTrials.gov Identifier: NCT00330148). Altogether, despite the importance of melarsoprol-based treatments, there is the urgent need to improve the clinical protocols by means of improved drug combinations capable to overcome the side effects. In this frame, new clinical trials are of outstanding importance. Another As-based drug, namely melarsomine dihydrochloride (marketed as Immiticide® or Merial®, Boehringer Ingelheim Animal Health, Noventana, Italy) is an antiprotozoal trypanocidal agent. Melarsomine is an FDA-approved medicine for the treatment of adult heartworm (Dirofilaria immitis) infection in dogs [58].
Beyond the use in medicinally-active molecules, more recently, As has been used as a prognostic probe to evaluate the course of the COVID-19 disease in a cohort of patients. Indeed, a relationship between the concentration of arsenic in the blood of COVID-19 patients and the severe illness or fatal outcome of the disease was found [59].
5. Antimony
The symbol (Sb) of this metalloid derives from the Latin stibnum which also lends its name to the mineral in which antimony is commonly found, i.e., stibnite (Sb2S3). This mineral was used since very ancient times. Indeed, it was known to the Ancient Egyptians as an eye cosmetic owing to its beautiful black color [60]. Antimony has four allotropes: a stable metallic form and three forms that are metastable (yellow, black and explosive). Nowadays, antimony is used in various applications ranging from the flame-retardant materials, alloys and also as an element for semiconducting materials [61].
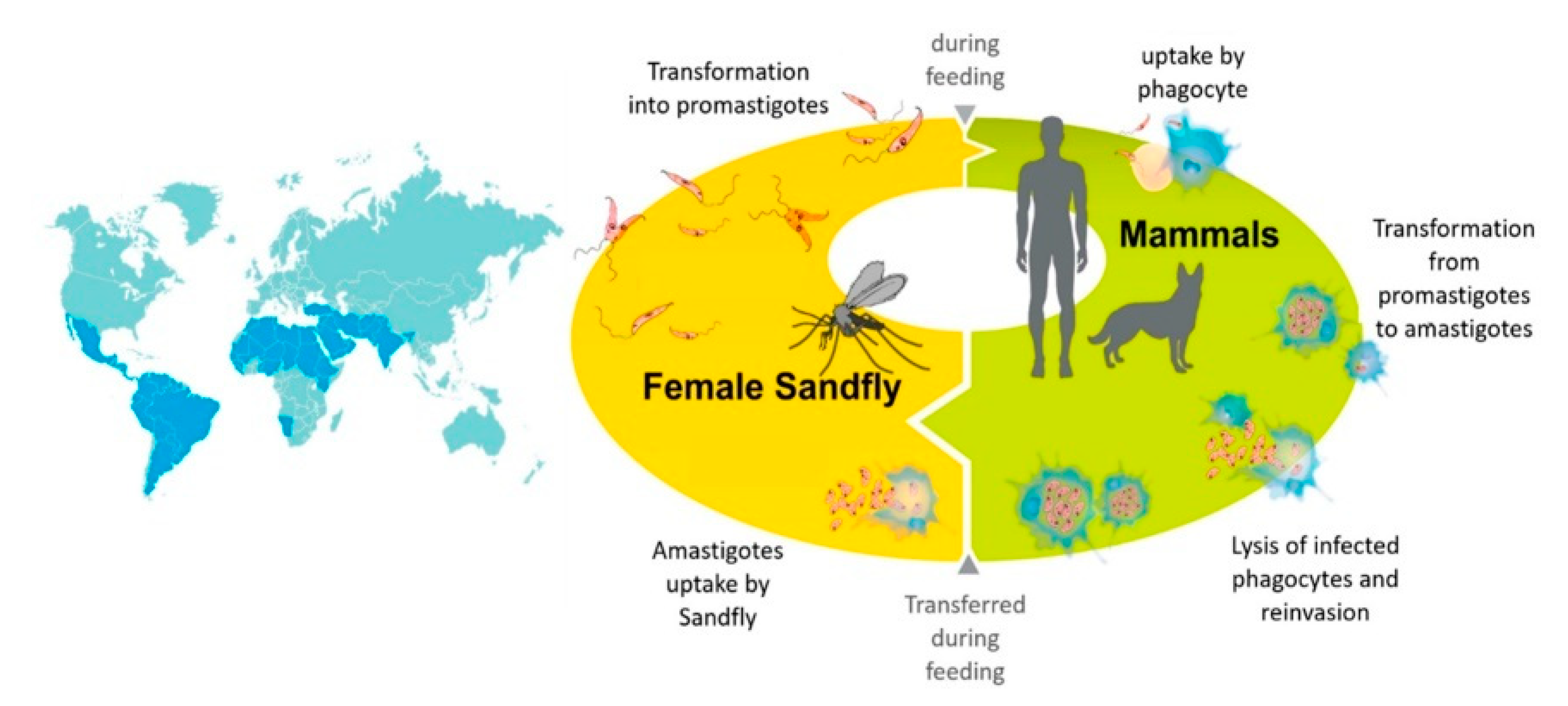
This pnictogen, was used with medicinal purposes for the treatment of parasitic and microbial infections [62]. Indeed, drugs containing Sb were used for the treatment of leishmaniasis since the 1900s, when the role of the Leishmania parasite and the characteristics of the infection process were elucidated (Figure 7) [63]. Distinct species of Leishmania are responsible for different clinical manifestations leading to various degrees of severity, from cutaneous lesions to life-threatening visceral disease [63]. The latter is caused by the pathogen Leishmania donovani or infantum depending on the geographical area. This is the most severe form, being often accompanied with a poor prognosis unless treated. At variance, Post-kala-azar dermal leishmaniasis (PKDL) is a manifestation that may occur after treatment of visceral leishmaniasis. Cutaneous leishmaniasis is usually characterized by an ulcer that typically self-heals in a few months. However, this manifestation may lead to scarring and disfigurement. Based on the infection, one out of ten cases may result in more severe manifestations (known as mucocutaneous leishmaniasis) [63,64,65]. Similarly, antimony-based drugs were extensively used for schistosomiasis, also a neglected acute and chronic parasitic tropical disease [46]. It is caused by the parasitic flatworms of the genus Schistosoma. Both the urinary tract and the intestines are infected by the parasite [66]. People are typically infected during exposure to infested water. Intestinal forms of schistosomiasis are characterized by abdominal pain and diarrhea. The liver and spleen may also be affected, especially in advanced stages of the disease that may also result in an accumulation of fluid in the peritoneal cavity. When urogenital infections occur, they are often accompanied by hematuria (blood in urine), but also kidney damage. Another severe complication is bladder cancer [67].
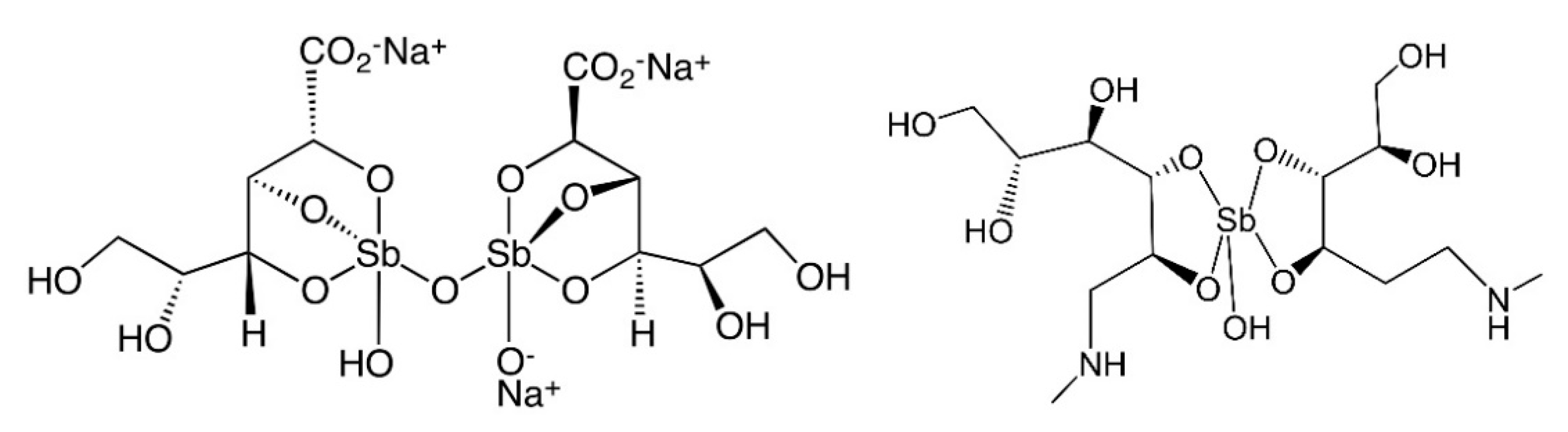
To date, two pentavalent antimonials are used in the clinical practice to treat leishmaniasis. Specifically, sodium stibogluconate (Pentostam®, GlaxoSmithKline, Brentford, UK) and meglumine antimoniate (Glucantim® or Glucantime®, Sanofi, Paris, France) are intravenously administered (Figure 8). Despite these drugs representing an essential arsenal to fight leishmaniasis, major problems are associated with treatments. In particular, resistance phenomena and high toxicity are limiting aspects [69].
The mode of action of these Sb(V) drugs based against leishmaniasis is not fully understood and the redox chemistry of the metalloid center, as well as its ability to bind several biological targets—genomic or non-genomic—are likely involved in the observed pharmacological action [69]. Indeed, it is not clear whether the actual pharmacophore contains Sb(V) or Sb(III). Overall, three main models for the mode of action were proposed that are here summarized [69,70]. In the so called “prodrug model” Sb(V) is a prodrug that undergoes reduction to Sb(III), the latter being a pharmacologically active—but even more toxic—species. Additionally, it is controversial to assess whether the reduction occurs through an enzymatic process. Similarly, it remains unclear the potential role of the parasite in the reduction process [71]. Moreover, the reduction to Sb(V) should involve the action of thiol-bearing compounds both from the host cells (e.g., glutathione) or parasite (trypanothione) [72]. The most likely targets after the reduction process are trypanothione reductase and zinc-finger proteins. Indeed, this kind of mechanism relying on thiol containing aminoacidic residues is typical also for metals with thiophilic character (e.g., Bi, Au) [69]. At variance, the “Intrinsic Antileishmanial Activity Model” indicates the Sb(V) as inherently active. Sodium stibogluconate is capable of type I DNA topoisomerase interaction, leading to the inhibition of unwinding and cleavage processes [69]. Additionally, coordination of Sb(V) to ribonucleosides has been highlighted in physiological-like conditions, supporting this mode of action [73]. In turn, this mode of binding might lead to the pharmacological activity against Leishmania both through the formation of Sb(V)-adenine nucleotide adducts and subsequent inhibition of the Leishmania purine transporters, as well as through the penetration of these complexes inside the parasite. Next, the neutral pH environment allows the adduct itself to impair the purine pathways [74]. Finally, in the “host immune activation model” antimonials are capable of parasite inhibition by activation of the immune system—innate or adaptive—of the infected patient. According to this model, an effective immune response is stimulated allowing to avoid relapse [69].
Sodium stibogluconate and meglumine antimoniate entered several clinical trials for improving the leishmaniasis treatments. Table 3 summarizes some of them.
From Table 3, the results show that the efforts in clinical trials have been directed to overcome the two major problems, i.e., the side effects and the resistance. Indeed, combining different drugs/treatments is a reliable strategy to overcome the resistance of the parasite to antimony-based protocols. Moreover, testing novel dosage might improve the treatment itself, improving the tolerability.
6. Tellurium
Tellurium (from the Latin tellus that means “earth”), is a rare element that belongs to the so called chalcogens and is chemically related to selenium and oxygen. It is a trace element. Interestingly, this “neglected” element has long been considered extremely toxic. A partial reappraisal on its biological role and its toxicity was made after the discovery of the essential role of selenium [75]. Accordingly, the toxicity of Te-based compounds basically depends on the chemical species and on the intake, hence Te is not inherently more cytotoxic than selenium, and its toxicity can be modulated by using specific ligands and controlling the chemical properties and cell internalization [76]. Tellurium can be simply oxidized to the corresponding oxides including TeO32−, TeO42−—tellurite and tellurate—respectively and TeO2. Several Te-based substrates have redox activity with a formal oxidation state of tellurium ranging from −2 to +6 [75].
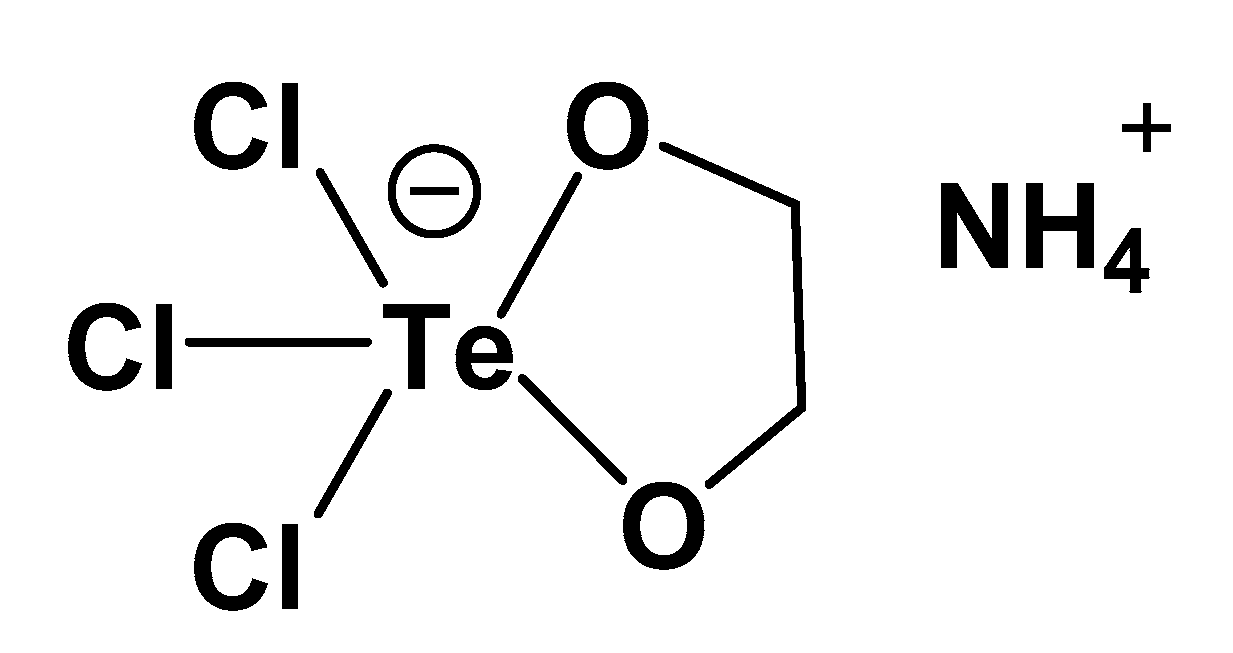
Tellurium finds application in a different field of technology. For instance, it is used as an additive in metallurgical industry, in glass production as well as in ceramic industry. It was also used for the development of diagnostic kits in bacteriological procedures and applications. In fact, some bacteria are able to reduce tellurite solutions to amorphous (black) tellurium [77]. Further technological applications of tellurium concern X-ray detectors, and development of solar panels and semiconductors [78]. Beyond these applications, tellurium compounds were also developed and tested for their medicinal applications. Among various applications, the most important is most probably AS101, namely, ammonium trichloro (dioxyethylene-O,O′) tellurate (Figure 9).
AS101 entered Phase II clinical trials in psoriasis patients, being the first Te-based agent tested for clinical applications. AS101 exerts potent immunomodulator effects and redox-modulating activities. Owing to these features, it was subjected to several studies for the application in autoimmune diseases. AS101 has a potent effect as an immunomodulator potentially suitable for several therapeutic applications [76,79,80]. As an anti-infective agent, AS101 was found effective against various pathogens in both bacterial strains and viruses [81,82,83]. Gram-negative bacteria are a major global problem. Indeed, they are responsible for infection that are often resistant to conventional antibiotics. Pairwise, the discovery rate of novel antibacterial agents has declined steeply [84]. Accordingly, there is the urgent need for novel and effective antibiotics. In this frame, AS101 has been tested against Enterobacter cloacae that represents a dangerous nosocomial pathogen causing infections among hospitalized or debilitated patients [81]. AS101 acts as potent antibiotics against Enterobacter cloacae with MIC and MBC (Minimum Bactericidal Concentration) of 9.4 mg/L. Interestingly, for lower concentration, AS101 possess an antibiofilm activity. Under a mechanistic point of view, by means of liposome swelling assay, Daniel-Hoffmann et al. demonstrated that AS101 penetrates the bacterial cell through a porin, causing damage to Na+ and K+ pumps, and leakage of potassium, phosphorous and sulfur [81].
AS101 is also effective against HIV. Treatment of HIV-1-infected peripheral blood mononuclear cells (PBMC) with AS101 administered at different concentrations have shown a strong inhibition of virus production. Remarkably, the compound determines an enhanced cell proliferation when administered to normal cells at non-cytotoxic concentrations [83]. The anti-HIV-1 effects of AS101 results from the inhibition of the different catalytic functions of viral reverse transcriptase. This effect is accompanied by the substantial absence of drug-related toxicity toward lymphocytes. All these aspects, alongside the immunomodulating activity of AS101, warranted a deeper evaluation, finally leading to clinical trials [83]. Similarly, AS101 entered clinical trials as an agent against HPV (Human Papilloma Virus). It was suggested that AS101 is effective towards HPV by the stimulation of the innate and acquired immune system (Table 4).
Some authors have also demonstrated that simple modification of the AS101 structure led to compounds that are far more active in controlling the replication of human poliovirus through the impairment of the 3C viral cysteine proteinase [82]. This finding opens to further development of the Te-based molecules for medicinal applications, pointing out AS101 as a reliable reference compound.
7. Conclusions
Owing to the increasing mechanistic insights provided by the modern omics techniques, it is possible to gather the most relevant information for the mechanisms of action of inorganic drugs [85]. This family of compounds, despite their limited use in clinical practice, has a huge impact as in the case of imaging techniques for diagnosis or anticancer and anti-infective therapy. In this frame, the clinical use of metalloid-based compounds is even more limited compared with metal-based compounds. However, it should be stressed that the unique chemistry and reactivity, typical of metalloids, can be advantageously exploited for the design of innovative anti-infective drugs. In fact, mechanistic information on the ability of metalloids to bind specific aminoacidic or genomic residues can help the choice of the proper ligands, finely tuning the chemistry, stability, and the activation process of the drug. This approach can significantly expand the “chemical space” leading to innovative and more effective treatments. Additionally, concerning the claims of high toxicity of metalloids, on one hand—as in the case of Tellurium—this aspect has been sometimes exacerbated; on the other, the choice of proper ligands capable of stabilizing the metalloid center could allow to avoid the toxic effects. Finally, as pointed out by the several clinical trials, the already approved metalloid-based molecules are extremely versatile and can be exploited for several and increasing medicinal applications both in diagnosis and therapy, provided that more attention of the research community will be devoted to this family of molecules.
Author Contributions
T.M. and D.L.M. contributed equally to this article. Both authors have read and agreed to the published version of the manuscript.
Funding
This work is supported by the University of Pisa under the “PRA—Progetti di Ricerca di Ateneo” Institutional Research Grants—project number PRA_2020_58 “Agenti innovativi e nanosistemi per target molecolari nell’ambito dell’oncologia di precisione”. The authors also gratefully acknowledge the Beneficentia Stiftung Foundation, Vaduz (BEN2019/48), University of Pisa (Rating Ateneo 2019–2020), for their financial support.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Silvestry-Rodriguez, N.; Sicairos-Ruelas, E.E.; Gerba, C.P.; Bright, K.R. Silver as a Disinfectant. Rev. Environ. Contam. Toxicol. 2007, 191, 23–45. [Google Scholar] [CrossRef]
- Fricker, S.P. Medical Uses of Gold Compounds: Past, Present and Future. Gold Bull. 1996, 29, 53–60. [Google Scholar] [CrossRef] [Green Version]
- Bonaccorso, C.; Marzo, T.; La Mendola, D. Biological Applications of Thiocarbohydrazones and Their Metal Complexes: A Perspective Review. Pharmaceuticals 2020, 13, 4. [Google Scholar] [CrossRef] [Green Version]
- Marzo, T.; La Mendola, D. The Effects on Angiogenesis of Relevant Inorganic Chemotherapeutics. Curr. Top. Med. Chem. 2020, 21, 73–86. [Google Scholar] [CrossRef] [PubMed]
- Johnstone, T.C.; Suntharalingam, K.; Lippard, S.J. The Next Generation of Platinum Drugs: Targeted Part (II) Agents, Nanoparticle Delivery, and Part (IV) Prodrugs. Chem. Rev. 2016, 116, 3436–3486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pillozzi, S.; D’Amico, M.; Bartoli, G.; Gasparoli, L.; Petroni, G.; Crociani, O.; Marzo, T.; Guerriero, A.; Messori, L.; Severi, M.; et al. The Combined Activation of K Ca 3.1 and Inhibition of K V 11.1/Herg1 Currents Contribute to Overcome Cisplatin Resistance in Colorectal Cancer Cells. Br. J. Cancer 2018, 118, 200–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cirri, D.; Pillozzi, S.; Gabbiani, C.; Tricomi, J.; Bartoli, G.; Stefanini, M.; Michelucci, E.; Arcangeli, A.; Messori, L.; Marzo, T. PtI2 (DACH), the Iodido Analogue of Oxaliplatin as a Candidate for Colorectal Cancer Treatment: Chemical and Biological Features. Dalt. Trans. 2017, 46, 3311–3317. [Google Scholar] [CrossRef]
- Anthony, E.J.; Bolitho, E.M.; Bridgewater, H.E.; Carter, O.W.L.; Donnelly, J.M.; Imberti, C.; Lant, E.C.; Lermyte, F.; Needham, R.J.; Palau, M.; et al. Metallodrugs Are Unique: Opportunities and Challenges of Discovery and Development. Chem. Sci. 2020, 11, 12888–12917. [Google Scholar] [CrossRef]
- Van Eldik, R.; Sadler, P. (Eds.) Medicinal Chemistry, 1st ed.; Academic Press: Cambridge, MA, USA, 2020; Volume 75, Available online: www.elsevier.com/books/medicinal-chemistry/van-eldik/978-0-12-819196-5 (accessed on 5 May 2021).
- Barry, N.P.E.; Sadler, P.J. 100 Years of Metal Coordination Chemistry: From Alfred Werner to Anticancer Metallodrugs. Pure Appl. Chem. 2014, 86, 1897–1910. [Google Scholar] [CrossRef] [Green Version]
- Barry, N.P.E.; Sadler, P.J. Exploration of the Medical Periodic Table: Towards New Targets. Chem. Commun. 2013, 49, 5106–5131. [Google Scholar] [CrossRef] [Green Version]
- Cirri, D.; Pratesi, A.; Marzo, T.; Messori, L. Metallo Therapeutics for COVID-19. Exploiting Metal-Based Compounds for the Discovery of New Antiviral Drugs. Expert Opin. Drug. Discov. 2021, 16, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Yuan, S.; Wang, R.; Chan, J.F.W.; Zhang, A.J.; Cheng, T.; Chik, K.K.H.; Ye, Z.W.; Wang, S.; Lee, A.C.Y.; Jin, L.; et al. Metallodrug Ranitidine Bismuth Citrate Suppresses SARS-Cov-2 Replication and Relieves Virus-Associated Pneumonia in Syrian Hamsters. Nat. Microbiol. 2020, 5, 1439–1448. [Google Scholar] [CrossRef] [PubMed]
- Rothan, H.A.; Stone, S.; Natekar, J.; Kumari, P.; Arora, K.; Kumar, M. The FDA-Approved Gold Drug Auranofin Inhibits Novel Coronavirus (SARS-COV-2) Replication and Attenuates Inflammation in Human Cells. Virology 2020, 547, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Marzo, T.; Messori, L. A Role for Metal-Based Drugs in Fighting COVID-19 Infection? The Case of Auranofin. ACS Med. Chem. Lett. 2020, 11, 1067–1068. [Google Scholar] [CrossRef]
- Van Cleave, C.; Crans, D.C. The First-Row Transition Metals in the Periodic Table of Medicine. Inorganics 2019, 7, 111. [Google Scholar] [CrossRef] [Green Version]
- Vernon, R.E. Which Elements Are Metalloids? J. Chem. Educ. 2013, 90, 1703–1707. [Google Scholar] [CrossRef]
- Miller, J.S. Viewpoint: Metalloids—An Electronic Band Structure Perspective. Chem. A. Eur. J. 2019, 25, 11177–11179. [Google Scholar] [CrossRef]
- Lloyd, N.C.; Morgan, H.W.; Nicholson, B.K.; Ronimus, R.S. The Composition of Ehrlich’s Salvarsan: Resolution of a Century-Old Debate. Angew. Chem. Int. Ed. 2005, 44, 941–944. [Google Scholar] [CrossRef] [Green Version]
- Baker, S.J.; Ding, C.Z.; Akama, T.; Zhang, Y.K.; Hernandez, V.; Xia, Y. Therapeutic Potential of Boron-Containing Compounds. Future Med. Chem. 2009, 1, 1275–1288. [Google Scholar] [CrossRef] [Green Version]
- Fernandes, G.F.S.; Denny, W.A.; Dos Santos, J.L. Boron in Drug Design: Recent Advances in the Development of New Therapeutic Agents. Eur. J. Med. Chem. 2019, 179, 791–804. [Google Scholar] [CrossRef]
- Ban, H.S.; Nakamura, H. Boron-Based Drug Design. Chem. Rec. 2015, 15, 616–635. [Google Scholar] [CrossRef] [PubMed]
- Kohno, J.; Kawahata, T.; Otake, T.; Morimoto, M.; Mori, H.; Ueba, N.; Nishio, M.; Kinumaki, A.; Komatsubara, S.; Kawashima, K. Boromycin, an Anti-HIV Antibiotic. Biosci. Biotechnol. Biochem. 1996, 60, 1036–1037. [Google Scholar] [CrossRef] [PubMed]
- Moreira, W.; Aziz, D.B.; Dick, T. Boromycin Kills Mycobacterial Persisters Without Detectable Resistance. Front. Microbiol. 2016, 7, 199. [Google Scholar] [CrossRef] [PubMed]
- Westerberg, D.P.; Voyack, M.J. Onychomycosis: Current Trends in Diagnosis and Treatment. Am. Fam. Physician 2013, 88, 762–770. [Google Scholar]
- Markham, A. Tavaborole: First Global Approval. Drugs 2014, 74, 1555–1558. [Google Scholar] [CrossRef]
- Rock, F.L.; Mao, W.; Yaremchuk, A.; Tukalo, M.; Crépin, T.; Zhou, H.; Zhang, Y.K.; Hernandez, V.; Akama, T.; Baker, S.J.; et al. An Antifungal Agent Inhibits an Aminoacyl-tRNA Synthetase by Trapping tRNA in the Editing Site. Science 2007, 316, 1759–1761. [Google Scholar] [CrossRef] [PubMed]
- Jinna, S.; Finch, J. Spotlight on Tavaborole for the Treatment of Onychomycosis. Drug Des. Devel. Ther. 2015, 9, 6185–6190. [Google Scholar]
- Elewski, B.E.; Aly, R.; Baldwin, S.L.; González Soto, R.F.; Rich, P.; Weisfeld, M.; Wiltz, H.; Zane, L.T.; Pollak, R. Efficacy and Safety of Tavaborole Topical Solution, 5%, a Novel Boron-Based Antifungal Agent, for the Treatment of Toenail Onychomycosis: Results from 2 Randomized Phase-III Studies. J. Am. Acad. Dermatol. 2015, 73, 62–69. [Google Scholar] [CrossRef] [Green Version]
- Junold, K.; Baus, J.A.; Burschka, C.; Vent-Schmidt, T.; Riedel, S.; Tacke, R. Five-Coordinate Silicon(II) Compounds with Si-M Bonds (M = Cr, Mo, W, Fe): Bis[N,N′-Diisopropylbenzamidinato(-)]Silicon(II) as a Ligand in Transition-Metal Complexes. Inorg. Chem. 2013, 52, 11593–11599. [Google Scholar] [CrossRef]
- Petkowski, J.J.; Bains, W.; Seager, S. On the Potential of Silicon as a Building Block for Life. Life 2020, 10, 84. [Google Scholar] [CrossRef]
- Reichstat, M.M.; Mioč, U.B.; Bogunovic, L.J.; Ribnikar, S.V. Theoretical Investigation of Intermolecular Hydrogen-Bonded Complexes in Systems: Substituted Carbinols (Silanols)-Ketones or Ethers. J. Mol. Struct. 1991, 244, 283–290. [Google Scholar] [CrossRef]
- Mills, J.S.; Showell, G.A. Exploitation of Silicon Medicinal Chemistry in Drug Discovery. Expert Opin. Investig. Drugs 2004, 13, 1149–1157. [Google Scholar] [CrossRef]
- Ramesh, R.; Reddy, D.S. Quest for Novel Chemical Entities through Incorporation of Silicon in Drug Scaffolds. J. Med. Chem. 2018, 61, 3779–3798. [Google Scholar] [CrossRef] [PubMed]
- Wolf, M.P.; Salieb-Beugelaar, G.B.; Hunziker, P. PDMS with Designer Functionalities—Properties, Modifications Strategies, and Applications. Prog. Polym. Sci. 2018, 83, 97–134. [Google Scholar] [CrossRef]
- Andersen, F.A. Final Report on the Safety Assessment of Aluminum Silicate, Calcium Silicate, Magnesium Aluminum Silicate, Magnesium Silicate, Magnesium Trisilicate, Sodium Magnesium Silicate, Zirconium Silicate, Attapulgite, Bentonite, Fuller’s Earth, Hectorite, Kaolin, Lithium Magnesium Silicate, Lithium Magnesium Sodium Silicate, Montmorillonite, Pyrophyllite, and Zeolite. Int. J. Toxicol. 2003, 22, 37–102. [Google Scholar] [CrossRef]
- Seljak, K.B.; Kocbek, P.; Gašperlin, M. Mesoporous Silica Nanoparticles as Delivery Carriers: An Overview of Drug Loading Techniques. J. Drug Deliv. Sci. Technol. 2020, 59, 101906. [Google Scholar] [CrossRef]
- Zhou, Y.; Quan, G.; Wu, Q.; Zhang, X.; Niu, B.; Wu, B.; Huang, Y.; Pan, X.; Wu, C. Mesoporous Silica Nanoparticles for Drug and Gene Delivery. Acta Pharm. Sin. B 2018, 8, 165–177. [Google Scholar] [CrossRef] [PubMed]
- O’Farrell, N.; Houlton, A.; Horrocks, B.R. Silicon Nanoparticles: Applications in Cell Biology and Medicine. Int. J. Nanomed. 2006, 1, 451–472. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Jiang, X.; Tang, J.; Su, Y.; Peng, F.; Lu, Y.; Peng, R.; He, Y. A Silicon-Based Antibacterial Material Featuring Robust and High Antibacterial Activity. J. Mater. Chem. B 2014, 2, 691–697. [Google Scholar] [CrossRef]
- Narayan, R.; Nayak, U.Y.; Raichur, A.M.; Garg, S. Mesoporous Silica Nanoparticles: A Comprehensive Review on Synthesis and Recent Advances. Pharmaceutics 2018, 10, 118. [Google Scholar] [CrossRef] [Green Version]
- Smirnov, N.A.; Kudryashov, S.I.; Nastulyavichus, A.A.; Rudenko, A.A.; Saraeva, I.N.; Tolordava, E.R.; Gonchukov, S.A.; Romanova, Y.M.; Ionin, A.A.; Zayarny, D.A. Antibacterial Properties of Silicon Nanoparticles. Laser Phys. Lett. 2018, 15, 105602. [Google Scholar] [CrossRef]
- Fu, P.P.; Xia, Q.; Hwang, H.M.; Ray, P.C.; Yu, H. Mechanisms of Nanotoxicity: Generation of Reactive Oxygen Species. J. Food Drug Anal. 2014, 22, 64–75. [Google Scholar] [CrossRef] [Green Version]
- Grund, S.C.; Hanusch, K.; Wolf, H.U. Arsenic and Arsenic Compounds. IARC Monogr. Eval. Carcinog. Risks Hum. 2011, 100, 41–93. [Google Scholar] [CrossRef]
- Patra, M.; Gasser, G.; Metzler-Nolte, N. Small Organometallic Compounds as Antibacterial Agents. Dalt. Trans. 2012, 41, 6350–6358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sekhon, B.S. Metalloid Compounds as Drugs. Res. Pharm. Sci. 2013, 8, 145–158. [Google Scholar] [PubMed]
- IARC Publications Website. Arsenic, Metals, Fibres, and Dusts. Available online: publications.iarc.fr/Book-And-Report-Series/Iarc-Monographs-On-The-Identification-Of-Carcinogenic-Hazards-To-Humans/Arsenic-Metals-Fibres-And-Dusts-2012 (accessed on 5 May 2021).
- Gurnari, C.; De Bellis, E.; DIvona, M.; Ottone, T.; Lavorgna, S.; Voso, M.T. When Poisons Cure: The Case of Arsenic in Acute Promyelocytic Leukemia. Chemotherapy 2020, 64, 238–247. [Google Scholar] [CrossRef]
- Seixas, J.; Atouguia, J.; Josenando, T.; Vatunga, G.; Bilenge, C.M.M.; Lutumba, P.; Burri, C. Clinical Study on the Melarsoprol-Related Encephalopathic Syndrome: Risk Factors and HLA Association. Trop. Med. Infect. Dis. 2020, 5, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Büscher, P.; Cecchi, G.; Jamonneau, V.; Priotto, G. Human African Trypanosomiasis. Lancet 2017, 390, 2397–2409. [Google Scholar] [CrossRef]
- Blum, J.; Schmid, C.; Burri, C. Clinical Aspects of 2541 Patients with Second Stage Human African Trypanosomiasis. Acta Trop. 2006, 97, 55–64. [Google Scholar] [CrossRef]
- Fairlamb, A.H. Chemotherapy of Human African Trypanosomiasis: Current and Future Prospects. Trends Parasitol. 2003, 19, 488–494. [Google Scholar] [CrossRef] [PubMed]
- Keiser, J.; Ericsson, Ö.; Burri, C. Investigations of the Metabolites of the Trypanocidal Drug Melarsoprol. Clin. Pharmacol. Ther. 2000, 67, 478–488. [Google Scholar] [CrossRef]
- Carter, N.S.; Fairlamb, A.H. Arsenical-Resistant Trypanosomes Lack an Unusual Adenosine Transporter. Nature 1993, 361, 173–176. [Google Scholar] [CrossRef] [PubMed]
- Fairlamb, A.H.; Cerami, A. Metabolism and Functions of Trypanothione in the Kinetoplastida. Annu. Rev. Microbiol. 1992, 46, 695–729. [Google Scholar] [CrossRef]
- Marzo, T.; Ferraro, G.; Merlino, A.; Messori, L. Protein Metalation by Inorganic Anticancer Drugs. In Encyclopedia of Inorganic and Bioinorganic Chemistry; Scott, R.A., Ed.; 2021; pp. 1–17. Available online: https://0-onlinelibrary-wiley-com.brum.beds.ac.uk/doi/abs/10.1002/9781119951438.eibc2747 (accessed on 16 May 2021). [CrossRef]
- Merlino, A.; Marzo, T.; Messori, L. Protein Metalation by Anticancer Metallodrugs: A Joint ESI MS and XRD Investigative Strategy. Chem. A. Eur. J. 2017, 23, 6942–6947. [Google Scholar] [CrossRef] [PubMed]
- Savadelis, M.D.; Day, K.M.; Bradner, J.L.; Wolstenholme, A.J.; Dzimianski, M.T.; Moorhead, A.R. Efficacy and Side Effects of Doxycycline Versus Minocycline in the Three-Dose Melarsomine Canine Adulticidal Heartworm Treatment Protocol. Parasites Vectors 2018, 11, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeng, H.L.; Yang, Q.; Yuan, P.; Wang, X.; Cheng, L. Associations of Essential and Toxic Metals/Metalloids in Whole Blood with Both Disease Severity and Mortality in Patients with COVID-19. FASEB J. 2021, 35, e21392. [Google Scholar] [CrossRef] [PubMed]
- Hansell, C. All Manner of Antimony. Nat. Chem. 2015, 7, 88. [Google Scholar] [CrossRef]
- Voyles, P.M.; Muller, D.A.; Grazul, J.L.; Citrin, P.H.; Gossmann, H.J.L. Atomic-Scale Imaging of Individual Dopant Atoms and Clusters in Highly N-Type Bulk Si. Nature 2002, 416, 826–829. [Google Scholar] [CrossRef]
- Mjos, K.D.; Orvig, C. Metallodrugs in Medicinal Inorganic Chemistry. Chem. Rev. 2014, 114, 4540–4563. [Google Scholar] [CrossRef]
- Burza, S.; Croft, S.L.; Boelaert, M. Leishmaniasis. Lancet 2018, 392, 951–970. [Google Scholar] [CrossRef]
- World Health Organization. Available online: www.euro.who.int/__data/assets/pdf_file/0017/245330/Strategic-framework-for-leishmaniasis-control-in-the-WHO-European-Region-20142020.pdf (accessed on 16 May 2021).
- Ejov, M.; Dagne, D. Strategic Framework for Leishmaniasis Control in the WHO European Region. 2014–2020; World Health Organization, Regional Office for Europe: Copenhagen, Denmark, 2014; ISBN 9789289050166. [Google Scholar]
- McManus, D.P.; Dunne, D.W.; Sacko, M.; Utzinger, J.; Vennervald, B.J.; Zhou, X.N. Schistosomiasis. Nat. Rev. Dis. Prim. 2018, 4, 1–19. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Schistosomiasis. Available online: www.who.int/news-room/fact-sheets/detail/schistosomiasis (accessed on 16 May 2021).
- Jain, S.; Santana, W.; Dolabella, S.S.; Santos, A.L.S.; Souto, E.B.; Severino, P. Are Nanobiosensors an Improved Solution for Diagnosis of Leishmania? Pharmaceutics 2021, 13, 491. [Google Scholar] [CrossRef] [PubMed]
- Frézard, F.; Demicheli, C.; Ribeiro, R.R. Pentavalent Antimonials: New Perspectives for Old Drugs. Molecules 2009, 14, 2317–2336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haldar, A.K.; Sen, P.; Roy, S. Use of Antimony in the Treatment of Leishmaniasis: Current Status and Future Directions. Mol. Biol. Int. 2011, 2011, 1–23. [Google Scholar] [CrossRef] [Green Version]
- Ashutosh; Sundar, S.; Goyal, N. Molecular Mechanisms of Antimony Resistance in Leishmania. J. Med. Microbiol. 2007, 56, 143–153. [Google Scholar] [CrossRef]
- Yan, S.; Li, F.; Ding, K.; Sun, H. Reduction of Pentavalent Antimony by Trypanothione and Formation of a Binary and Ternary Complex of Antimony(III) and Trypanothione. J. Biol. Inorg. Chem. 2003, 8, 689–697. [Google Scholar] [CrossRef]
- Ferreira, C.D.S.; Pimenta, A.M.D.C.; Demicheli, C.; Frézard, F. Characterization of Reactions of Antimoniate and Meglumine Antimoniate with a Guanine Ribonucleoside at Different pH. BioMetals 2006, 19, 573–581. [Google Scholar] [CrossRef] [PubMed]
- Roberts, W.L.; Berman, J.D.; Rainey, P.M. In vitro Antileishmanial Properties of Tri- and Pentavalent Antimonial Preparations. Antimicrob. Agents Chemother. 1995, 39, 1234–1239. [Google Scholar] [CrossRef] [Green Version]
- Cunha, R.L.O.R.; Gouvea, I.E.; Juliano, L. A Glimpse on Biological Activities of Tellurium Compounds. An. Acad. Bras. Cienc. 2009, 81, 393–407. [Google Scholar] [CrossRef] [Green Version]
- Halpert, G.; Sredni, B. The Effect of the Novel Tellurium Compound AS101 on Autoimmune Diseases. Autoimmun. Rev. 2014, 13, 1230–1235. [Google Scholar] [CrossRef]
- Nyska, A.; Waner, T.; Pirak, M.; Albeck, M.; Sredni, B. Toxicity Study in Rats of a Tellurium Based Immunomodulating Drug, AS-101: A Potential Drug for AIDS and Cancer Patients. Arch. Toxicol. 1989, 63, 386–393. [Google Scholar] [CrossRef]
- Zweibel, K. The Impact of Tellurium Supply on Cadmium Telluride Photovoltaics. Science 2010, 328, 699–701. [Google Scholar] [CrossRef] [PubMed]
- Halpert, G.; Halperin Sheinfeld, M.; Monteran, L.; Sharif, K.; Volkov, A.; Nadler, R.; Schlesinger, A.; Barshak, I.; Kalechman, Y.; Blank, M.; et al. The Tellurium-Based Immunomodulator, AS101 Ameliorates Adjuvant-Induced Arthritis in Rats. Clin. Exp. Immunol. 2021, 203, 375–384. [Google Scholar] [CrossRef] [PubMed]
- Hachmo, Y.; Kalechman, Y.; Skornick, I.; Gafter, U.; Caspi, R.R.; Sredni, B. The Small Tellurium Compound AS101 Ameliorates Rat Crescentic Glomerulonephritis: Association with Inhibition of Macrophage Caspase-1 Activity Via Very Late Antigen-4 Inactivation. Front. Immunol. 2017, 8, 240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daniel-Hoffmann, M.; Sredni, B.; Nitzan, Y. Bactericidal Activity of the Organo-Tellurium Compound AS101 against Enterobacter Cloacae. J. Antimicrob. Chemother. 2012, 67, 2165–2172. [Google Scholar] [CrossRef] [PubMed]
- Gouvea, I.E.; Santos, J.A.N.; Burlandy, F.M.; Tersariol, I.L.S.; Da Silva, E.E.; Juliano, M.A.; Juliano, L.; Cunha, R.L.O.R. Poliovirus 3C Proteinase Inhibition by Organotelluranes. Biol. Chem. 2011, 392, 587–591. [Google Scholar] [CrossRef] [PubMed]
- Vonsover, A.; Loya, S.; Sredni, B.; Albeck, M.; Gotlieb-Stematsky, T.; Araf, O.; Hizi, A. Inhibition of the Reverse Transcriptase Activity and Replication of Human Immunodeficiency Virus Type 1 by AS 101 In Vitro. AIDS Res. Hum. Retrovir. 1992, 8, 613–623. [Google Scholar] [CrossRef]
- Di Luca, M.; Marzo, T. Development of Effective Antibacterial Treatment: Lessons from the Past and Novel Approaches. Antibiotics 2021, 10, 230. [Google Scholar] [CrossRef]
- La Mendola, D.; Giacomelli, C.; Rizzarelli, E. Intracellular Bioinorganic Chemistry and Cross Talk Among Different-Omics. Curr. Top. Med. Chem. 2016, 16, 3103–3130. [Google Scholar] [CrossRef]
Figure 1.
The periodic table highlighting the elements considered for the purposes of this article. The group of metalloids with application in the field of anti-infective therapy (B, Si, As, Sb, Te) is indicated by the red line.
Figure 1.
The periodic table highlighting the elements considered for the purposes of this article. The group of metalloids with application in the field of anti-infective therapy (B, Si, As, Sb, Te) is indicated by the red line.

Figure 2.
Chemical structures representing the composition of the mixture known as Salvarsan®.

Figure 3.
Chemical structures of boromycine (left) and tavaborole (right).

Figure 4.
Representation of different types of mesoporous silica nanoparticles (MSNs). IUPAC defines mesoporous materials as characterized by a pore size in the range of 2–50 nm and an ordered arrangement of pores giving an ordered structure to it (Reprinted from ref. [41]. Copyright 2018 by the authors. Licensee MDPI, Basel, Switzerland).
Figure 4.
Representation of different types of mesoporous silica nanoparticles (MSNs). IUPAC defines mesoporous materials as characterized by a pore size in the range of 2–50 nm and an ordered arrangement of pores giving an ordered structure to it (Reprinted from ref. [41]. Copyright 2018 by the authors. Licensee MDPI, Basel, Switzerland).

Figure 5.
Chemical structure of Neosalvarsan®. As in the case of Salvarsan®, this formal structure bearing an arsenic-arsenic double bond is incorrect. Indeed, it is a mixture of differently-sized rings with arsenic-arsenic single bonds.
Figure 5.
Chemical structure of Neosalvarsan®. As in the case of Salvarsan®, this formal structure bearing an arsenic-arsenic double bond is incorrect. Indeed, it is a mixture of differently-sized rings with arsenic-arsenic single bonds.

Figure 6.
Chemical structure of melarsoprol. The red line indicates the dimercaprol ligand.

Figure 7.
Geographical distribution of leishmaniasis in the world (left panel). Life cycle of Leishmania in sandfly and mammalian host (right panel). The two main evolutionary forms during their life cycle: the promastigote (in the invertebrate host) and the amastigote (present in the vertebrate host) are shown. Globally, more than 20 Leishmania species exist, transmitted by over 90 phlebotomine sandfly species (Reprinted from ref. [68]. Copyright 2021 by the authors. Licensee MDPI, Basel, Switzerland).
Figure 7.
Geographical distribution of leishmaniasis in the world (left panel). Life cycle of Leishmania in sandfly and mammalian host (right panel). The two main evolutionary forms during their life cycle: the promastigote (in the invertebrate host) and the amastigote (present in the vertebrate host) are shown. Globally, more than 20 Leishmania species exist, transmitted by over 90 phlebotomine sandfly species (Reprinted from ref. [68]. Copyright 2021 by the authors. Licensee MDPI, Basel, Switzerland).

Figure 8.
Chemical structures of the clinically-used Sb(V) drugs: sodium stibogluconate (left) and meglumine antimoniate (right).
Figure 8.
Chemical structures of the clinically-used Sb(V) drugs: sodium stibogluconate (left) and meglumine antimoniate (right).

Figure 9.
Chemical structures of AS101.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
The six elements commonly recognized as metalloids (Reprinted with permission from ref. [17]. Copyright 2013, American Chemical Society).
Table 1.
The six elements commonly recognized as metalloids (Reprinted with permission from ref. [17]. Copyright 2013, American Chemical Society).
| Element | IP/(kcal/mol) | IP/(kJ/mol) | EN a | EN b |
|---|---|---|---|---|
| β-Boron | 193 | 800 | 2.0 | 2.04 |
| α-Silicon | 189 | 786 | 1.8 | 1.90 |
| α-Germanium | 184 | 762 | 1.8 | 2.01 |
| α-Arsenic | 228 | 944 | 2.0 | 2.18 |
| α-Antimony | 201 | 830 | 1.9 | 2.05 |
| α-Tellurium | 210 | 869 | 2.1 | 2.10 |
| Average | 201 | 832 | 1.9 | 2.05 |
a Original Pauling electronegativity value. b Revised Pauling value.
Table 2.
Clinical trials involving tavaborole as antifungal agent (from https://clinicaltrials.gov/, accessed on 27 April 2021).
Table 2.
Clinical trials involving tavaborole as antifungal agent (from https://clinicaltrials.gov/, accessed on 27 April 2021).
| ClinicalTrials.gov Identifier | Status | Aim | Results |
|---|---|---|---|
| NCT03405818 | C (2018) | S/P | Y |
| NCT01302119 | C (2019) | S/E | Y |
| NCT01270971 | C (2019) | S/E | Y |
| NCT00680160 | C (2019) | A | NA |
| NCT00679601 | C (2018) | A | NA |
| NCT00680134 | C (2018) | S/E | NA |
| NCT01278394 | C (2018) | S/E | Y |
| NCT00679523 | C (2018) | S/E | NA |
| NCT00679965 | C (2018) | D | NA |
| NCT00679770 | C (2018) | D | NA |
C = Completed, the year of the last update is reported in brackets; S = Safety; P = Pharmacokinetic; E = Efficacy; A = Absorption; D = Dosage; Y = Results published; NA= Results not available.
Table 3.
Clinical trials involving sodium meglumine antimoniate and stibogluconate as anti-leishmaniasis agents (from https://clinicaltrials.gov/, accessed on 27 April 2021).
Table 3.
Clinical trials involving sodium meglumine antimoniate and stibogluconate as anti-leishmaniasis agents (from https://clinicaltrials.gov/, accessed on 27 April 2021).
| ClinicalTrials.gov Identifier | Drug(s) | Status | Aim | Results |
|---|---|---|---|---|
| NCT00480883 | Meglumine Antimoniate + Allopurinol | C (2010) | Co | NA |
| NCT01050777 | Nano-liposomal Meglumine Antimoniate | C (2012) | F | NA |
| NCT00317980 | Low-doses Meglumine Antimoniate | C (2009) | D | NA |
| NCT01301937 | Low-doses Meglumine Antimoniate | R | D | NA |
| NCT01301924 | Alternative doses of Meglumine Antimoniate | C (2018) | D | NA |
| NCT01381055 | Meglumine Antimoniate + Pentoxifylline | C (2017) | Co | NA |
| NCT00818818 | Low-doses Meglumine Antimoniate | C (2010) | D | NA |
| NCT00537953 | Meglumine Antimoniate + Miltefosine | U | D/Co | NA |
| NCT00657618 | Sodium Stibogluconate | C (2020) | S | Y |
| NCT02281669 | Sodium Stibogluconate | U | S | NA |
| NCT00508963 | Sodium Stibogluconate | A | E | NA |
| NCT00662012 | Sodium Stibogluconate | C (2021) | E | Y |
| NCT00255567 | Sodium Stibogluconate | C (2016) | E/S | NA |
| NCT01067443 | Sodium Stibogluconate + AmBisome® (Gilead Sciences, Inc., Foster City, CA, USA) | C (2017) | E/S/Co | NA |
| NCT03009422 | Sodium Stibogluconate + Fractional CO2 laser | U | E/Co | NA |
| NCT04699383 | Sodium Stibogluconate + Allopurinol | R | E | NA |
C = Completed, the year of the last update is reported in brackets; R = Recruiting; U= Unknown; A = Available; Co = Novel drug combinations; F = Novel formulations; D = Dosage; E = Efficacy; S = Safety; Y = Results published; NA= Results not available.
Table 4.
Clinical trials involving AS101 as anti-infective agents (from https://clinicaltrials.gov/, accessed on 27 April 2021).
Table 4.
Clinical trials involving AS101 as anti-infective agents (from https://clinicaltrials.gov/, accessed on 27 April 2021).
| ClinicalTrials.gov Identifier | Indication | Status | Aim | Results |
|---|---|---|---|---|
| NCT01555112 | HPV-condyloma acuminata | C (2013) | F/S/E | NA |
| NCT01943630 | External Genital Warts (HPV) | U | S/E | NA |
| NCT00001006 | HIV | C (2012) | E/S | NA |
| NCT00002266 | HIV | C (2005) | D/E | NA |
| NCT00002013 | HIV | C (2005) | Co/S/E/D/P | NA |
| NCT00002033 | HIV | C (2005) | Co/E/S | NA |
C = Completed, the year of the last update is reported in brackets; R = Recruiting; U= Unknown; A = Available; Co = Novel drug combinations; F = Novel formulations; D = Dosage; P = Pharmacokinetic; E = Efficacy; S = Safety; Y = Results published; NA= Results not available.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Marzo, T.; La Mendola, D. Strike a Balance: Between Metals and Non-Metals, Metalloids as a Source of Anti-Infective Agents. Inorganics 2021, 9, 46. https://0-doi-org.brum.beds.ac.uk/10.3390/inorganics9060046
AMA Style
Marzo T, La Mendola D. Strike a Balance: Between Metals and Non-Metals, Metalloids as a Source of Anti-Infective Agents. Inorganics. 2021; 9(6):46. https://0-doi-org.brum.beds.ac.uk/10.3390/inorganics9060046
Chicago/Turabian StyleMarzo, Tiziano, and Diego La Mendola. 2021. "Strike a Balance: Between Metals and Non-Metals, Metalloids as a Source of Anti-Infective Agents" Inorganics 9, no. 6: 46. https://0-doi-org.brum.beds.ac.uk/10.3390/inorganics9060046
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.