A New Technique for Direct Fabrication of Fiber-Reinforced Composite Bridge: A Long-Term Clinical Observation †

 ,
,
Abstract
:1. Introduction
2. Material and Methods
- Maintenance of good oral hygiene;
- No parafunctional habits;
- The absence of large restorations or caries lesions on the abutment teeth;
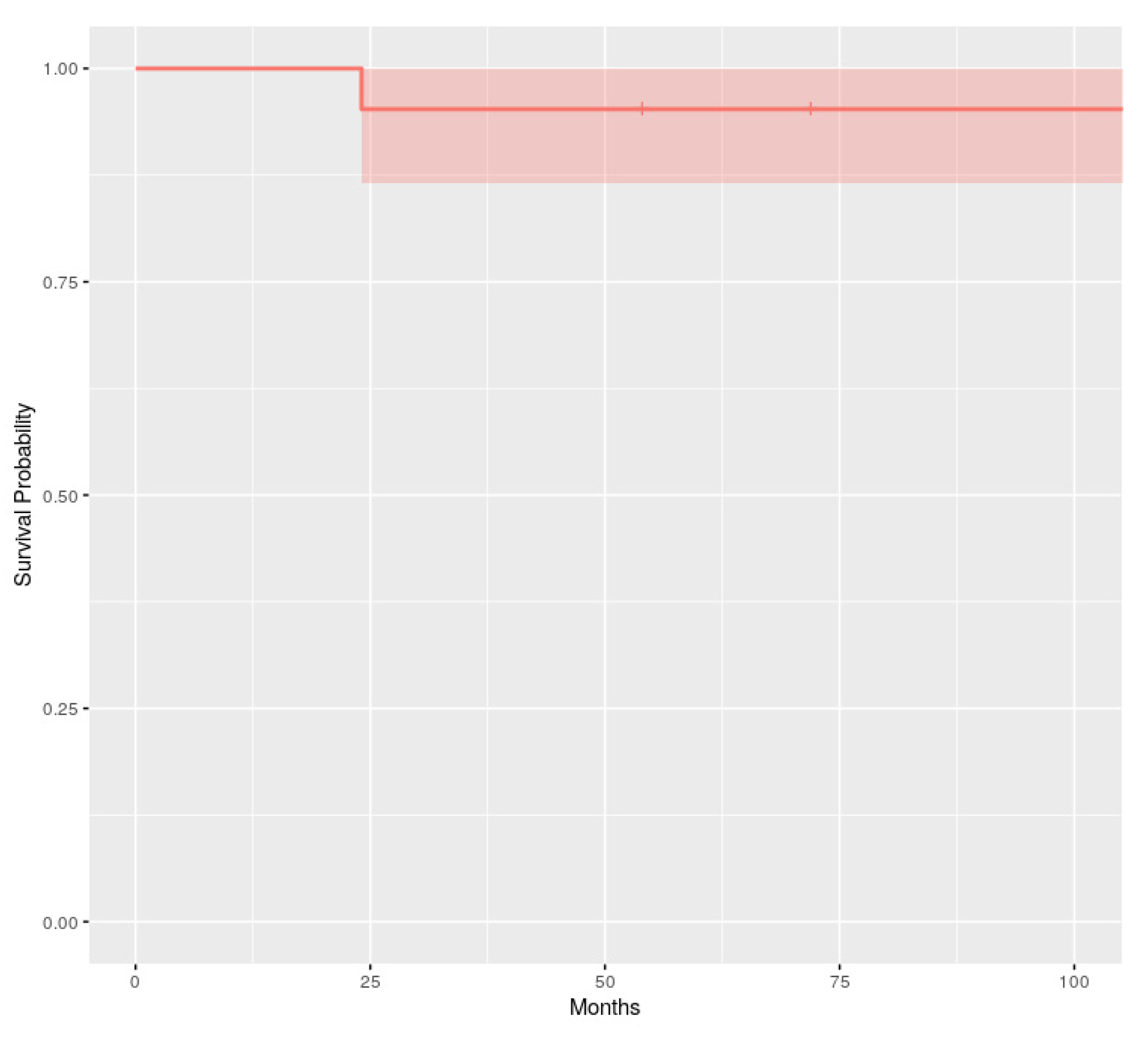
3. Results
4. Discussion
- The periodontal inflammation aspect on the pontic area: the framework design releases the embrasures allowing adequate interproximal brushing, avoiding periodontal disease and interproximal caries.
- Long term survival: this proposed protocol which uses inlay retainers and a core with two “T” shaped pins reinforces and stabilizes the FRCB, allowing greater survival over time.
Author Contributions
Funding
Conflicts of Interest
References
- Ahmed, K.E.; Li, K.Y.; Murray, C.A. Longevity of fiber-reinforced composite fixed partial dentures (FRC FPD)-Systematic review. J. Dent. 2017, 61, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Izgi, A.D.; Eskimez, S.; Kale, E.; Değer, Y. Directly fabricated inlay-retained glass- and polyethylene fiber-reinforced composite fixed dental prostheses in posterior single missing teeth: A short-term clinical observation. J. Adhes. Dent. 2011, 13, 383–391. [Google Scholar]
- Iglesia-Puig, M.A.; Arellano-Cabornero, A. Inlay fixed partial denture as a conservative approach for restoring posterior missing teeth: A clinical report. J. Prosthet. Dent. 2003, 89, 443–445. [Google Scholar] [CrossRef]
- Wolff, D.; Schach, C.; Kraus, T.; Ding, P.; Pritsch, M. Fiber-reinforced composite fixed dental prostheses: A retrospective clinical examination. J. Adhes. Dent. 2011, 13, 187–194. [Google Scholar] [PubMed]
- Ayna, E.; Celenk, S. Polyethylene fiber-reinforced composite inlay fixed partial dentures: Two-year preliminary results. J. Adhes. Dent. 2005, 7, 337–342. [Google Scholar] [PubMed]
- Frese, C.; Schiller, P.; Staehle, H.J.; Wolff, D. Fiber-reinforced composite fixed dental prostheses in the anterior area: A 4.5-year follow-up. J. Prosthet. Dent. 2014, 112, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Song, M.J.; Shin, S.J.; Lee, Y.; Park, J.W. Esthetic rehabilitation of single anterior edentulous space using fiber-reinforced composite. Restor. Dent. Endod. 2014, 39, 220–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Isola, G.; Matarese, G.; Ramaglia, L.; Pedullà, E.; Rapisarda, E.; Iorio-Siciliano, V. Association between periodontitis and glycosylated haemoglobin before diabetes onset: A cross-sectional study. Clin. Oral Investig. 2019, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Isola, G.; Alibrandi, A.; Rapisarda, E.; Matarese, G.; Williams, R.C.; Leonardi, R. Association of vitamin D in patients with periodontitis: A cross-sectional study. J. Periodontal Res. 2020. [Google Scholar] [CrossRef] [PubMed]
- Perea-Lowery, L.; Vallittu, P.K. Framework design and pontics of fiber-reinforced composite fixed dental prostheses—An overview. J. Prosthodont. Res. 2018, 62, 281–286. [Google Scholar] [CrossRef]
- Song, H.Y.; Yi, Y.J.; Cho, L.R.; Park, D.Y. Effects of two preparation designs and pontic distance on bending and fracture strength of fiber-reinforced composite inlay fixed partial dentures. J. Prosthet. Dent. 2003, 90, 347–353. [Google Scholar] [CrossRef]
- Goguta, L.M.; Candea, A.; Lungeanu, D.; Frandes, M.; Jivanescu, A. Direct Fiber-Reinforced Interim Fixed Partial Dentures: Six-Year Survival Study. J. Prosthodont. Off. J. Am. Coll. Prosthodont. 2019, 28, 604–608. [Google Scholar] [CrossRef] [PubMed]
- Strassler, H.E.; Tomona, N.; Spitznagel, J.K. Stabilizing periodontally compromised teeth with fiber-reinforced composite resin. Dent. Today 2003, 22, 102–109. [Google Scholar] [PubMed]
- Meiers, J.C.; Freilich, M.A. Use of a prefabricated fiber-reinforced composite resin framework to provide a provisional fixed partial denture over an integrating implant: A clinical report. J. Prosthet. Dent. 2006, 95, 14–18. [Google Scholar] [CrossRef] [PubMed]
- Singh, K.; Gupta, N.; Unnikrishnan, N.; Kapoor, V.; Arora, D.; Khinnavar, P.K. A Conservative Treatment Approach to Replacing a Missing Anterior Tooth. Case Rep. Dent. 2014, 14, 10–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benito, P.P.; Trushkowsky, R.D.; Magid, K.S.; David, S.B. Fiber-reinforced framework in conjunction with porcelain veneers for the esthetic replacement of a congenitally missing maxillary lateral incisor: A case study. Oper. Dent. 2012, 37, 576–583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bagis, B.; Satiroglu, I.; Korkmaz, F.M.; Ates, S.M. Rehabilitation of an extracted anterior tooth space using fiber-reinforced composite and the natural tooth. Dent. Traumatol. Off. Publ. Int. Assoc. Dent. Traumatol. 2010, 26, 191–194. [Google Scholar] [CrossRef]
- Newbrun, E. Indices to measure gingival bleeding. J. Periodontol. 1996, 67, 555–561. [Google Scholar] [CrossRef]
- Fischman, S.L. Current status of indices of plaque. J. Clin. Periodontol. 1986, 13, 371–374. [Google Scholar] [CrossRef]
- Magne, P. A new approach to the learning of dental morphology, function, and esthetics: The “2D-3D-4D” concept. Int. J. Esthet. Dent. 2015, 10, 32–47. [Google Scholar]
- Gupta, A.; Yelluri, R.K.; Munshi, A.K. Fiber-reinforced Composite Resin Bridge: A Treatment Option in Children. Int. J. Clin. Pediatr. Dent. 2015, 8, 62–65. [Google Scholar] [CrossRef] [PubMed]
- Chafaie, A.; Dahan, S.; Le Gall, M. Fiber-reinforced composite anterior bridge in pediatric traumatology: Clinical considerations. Int. Orthod. 2013, 11, 445–456. [Google Scholar] [CrossRef] [PubMed]
- Pankratz, V.; Zimmer, S.; Marković, L. Anterior fiber-reinforced ribbon composite resin bridge—A case report. Clin. Case Rep. 2018, 6, 1941–1946. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tacir, I.H. Comparison of Load-Bearing Capacities of 3-Unit Fiber-Reinforced Composite Adhesive Bridges with Different Framework Designs. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2018, 24, 4440–4448. [Google Scholar] [CrossRef] [PubMed]
- Ozcan, M.; Breuklander, M.H.; Vallittu, P.K. The effect of box preparation on the strength of glass fiber-reinforced composite inlay-retained fixed partial dentures. J. Prosthet. Dent. 2005, 93, 337–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spinas, E.; Aresu, M.; Canargiu, F. Prosthetic rehabilitation interventions in adolescents with fixed bridges: A 5-year observational study. Eur. J. Paediatr. Dent. 2013, 14, 59–62. [Google Scholar] [PubMed]
- Cenci, M.S.; da Rosa Rodolpho, P.A.; Pereira-Cenci, T.; Del Bel Cury, A.A.; Demarco, F.F. Fixed partial dentures in an up to 8-year follow-up. J. Appl. Oral Sci. Rev. FOB 2010, 18, 364–371. [Google Scholar] [CrossRef] [Green Version]
- Kurthukoti, A.J.; Paul, J.; Gandhi, K.; Rao, D.B. Fracture resistance of endodontically treated permanent anterior teeth restored with three different esthetic post systems: An in vitro study. J. Indian Soc. Pedod. Prev. Dent. 2015, 33, 296–301. [Google Scholar] [CrossRef]
- Stiesch-Scholz, M.; Schulz, K.; Borchers, L. In vitro fracture resistance of four-unit fiber-reinforced composite fixed partial dentures. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2006, 22, 374–381. [Google Scholar] [CrossRef]
- Saritha, M.K.; Paul, U.; Keswani, K.; Jhamb, A.; Mhatre, S.H.; Sahoo, P.K. Comparative Evaluation of Fracture Resistance of Different Post Systems. J. Int. Soc. Prev. Commun. Dent. 2017, 7, 356–359. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n = 21 | Age (Years) | Gender (Male/Female) | Location of Prosthesis (Abutment Teeth n1–n2) | Type of Framework | |
|---|---|---|---|---|---|
| 1 | 83 | M | Maxillary left | (3–5) | Glass fiber |
| 2 | 36 | M | Maxillary right | (3–5) | Glass fiber |
| 3 | 57 | M | Maxillary left | (4–6) | Glass fiber |
| 4 | 35 | M | Maxillary right | (1–3) | Glass fiber |
| 5 | 77 | M | Mandibular left | (4–6) | Glass fiber |
| 6 | 50 | M | Maxillary left | (3–5) | Glass fiber |
| 7 | 67 | F | Mandibular right | (1–3) | Glass fiber |
| 8 | 67 | F | Maxillary right | (3–5) | Glass fiber |
| 9 | 45 | M | Mandibular left | (5–7) | Glass fiber |
| 10 | 25 | F | Maxillary right | (4–6) | Glass fiber |
| 11 | 36 | M | Mandibular right | (5–7) | Glass fiber |
| 12 | 62 | M | Mandibular right | (1–2) | Glass fiber |
| 13 | 88 | M | Maxillary right | (3–5) | Glass fiber |
| 14 | 64 | M | Maxillary right | (1–3) | Glass fiber |
| 15 | 35 | F | Maxillary right | (4–6) | Glass fiber |
| 16 | 53 | M | Maxillary right | (1–3) | Glass fiber |
| 17 | 85 | M | Maxillary right | (2–4) | Glass fiber |
| 18 | 87 | F | Maxillary left | (3–5) | Glass fiber |
| 19 | 38 | F | Maxillary right | (3–5) | Glass fiber |
| 20 | 65 | M | Maxillary right | (1–3) | Glass fiber |
| 21 | 81 | F | Maxillary right | (3–5) | Glass fiber |
| n = 21 | Partial or Total Debonding of Prosthesis | Fracture Area of Prosthesis (Months) | Survival Time (Months) | ||
|---|---|---|---|---|---|
| Mesial Abutment | Pontic | Distal Abutment | |||
| 1 | - | - | - | 84 M | 108 M |
| 2 | - | - | - | - | 108 M |
| 3 | - | - | - | - | 108 M |
| 4 | - | - | - | - | 108 M |
| 5 | - | - | - | - | 108 M |
| 6 | - | - | - | - | 108 M |
| 7 | - | - | - | - | 108 M |
| 8 | - | - | - | 60 M | 108 M |
| 9 | - | - | - | 72 M | 108 M |
| 10 | - | - | - | - | 108 M |
| 11 | - | - | - | - | 108 M |
| 12 | - | - | - | - | 108 M |
| 13 | - | - | - | - | 72 M (EXITUS) |
| 14 | - | - | - | - | 108 M |
| 15 | - | - | - | - | 108 M |
| 16 | Total debonding | - | - | - | 24 M |
| 17 | - | - | - | - | 108 M |
| 18 | - | - | - | - | 54 M (EXITUS) |
| 19 | - | - | - | - | 108 M |
| 20 | - | - | - | - | 108 M |
| 21 | - | - | - | - | 108 M |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Escobedo Martínez, M.F.; Rodríguez López, S.; Valdés Fontela, J.; Olay García, S.; Mauvezín Quevedo, M. A New Technique for Direct Fabrication of Fiber-Reinforced Composite Bridge: A Long-Term Clinical Observation. Dent. J. 2020, 8, 48. https://0-doi-org.brum.beds.ac.uk/10.3390/dj8020048
Escobedo Martínez MF, Rodríguez López S, Valdés Fontela J, Olay García S, Mauvezín Quevedo M. A New Technique for Direct Fabrication of Fiber-Reinforced Composite Bridge: A Long-Term Clinical Observation. Dentistry Journal. 2020; 8(2):48. https://0-doi-org.brum.beds.ac.uk/10.3390/dj8020048
Chicago/Turabian StyleEscobedo Martínez, Matías Ferrán, Samuel Rodríguez López, Jairo Valdés Fontela, Sonsoles Olay García, and Mario Mauvezín Quevedo. 2020. "A New Technique for Direct Fabrication of Fiber-Reinforced Composite Bridge: A Long-Term Clinical Observation" Dentistry Journal 8, no. 2: 48. https://0-doi-org.brum.beds.ac.uk/10.3390/dj8020048