Salvage of Dental Implant Located in Mandibular Odontogenic Cyst. A Conservative Surgical Treatment Proposal

 ,
,  ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
- Odontogenic cysts of inflammatory origin (radicular cyst, inflammatory collateral cysts).
- Odontogenic and non-odontogenic developmental cysts (dentigerous cyst, odontogenic keratocyst, lateral periodontal cyst and botryoid odontogenic cyst, gingival cysts, glandular odontogenic cyst, calcifying odontogenic cyst, orthokeratinized odontogenic cyst, nasopalatine duct cyst) [3].
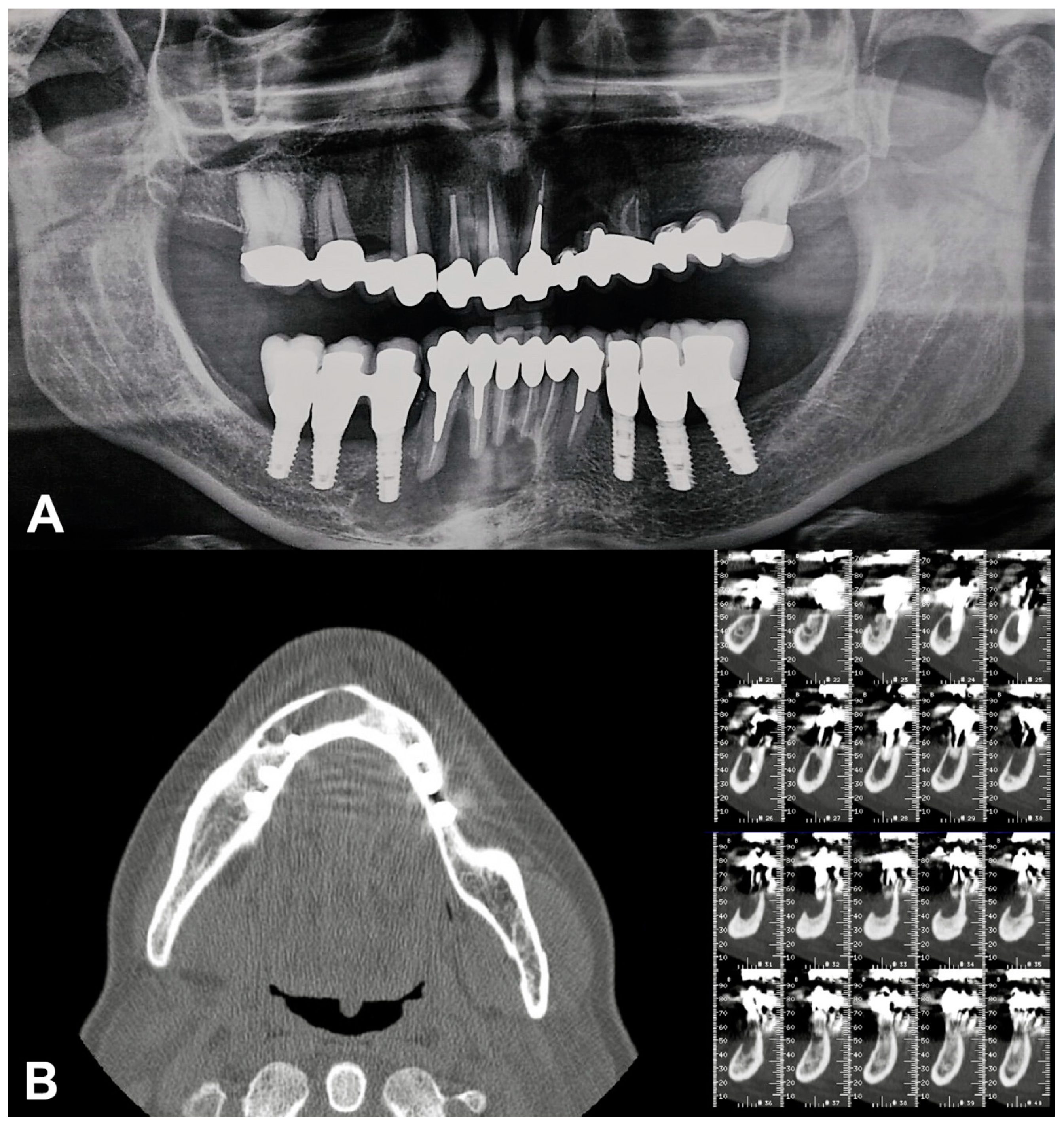
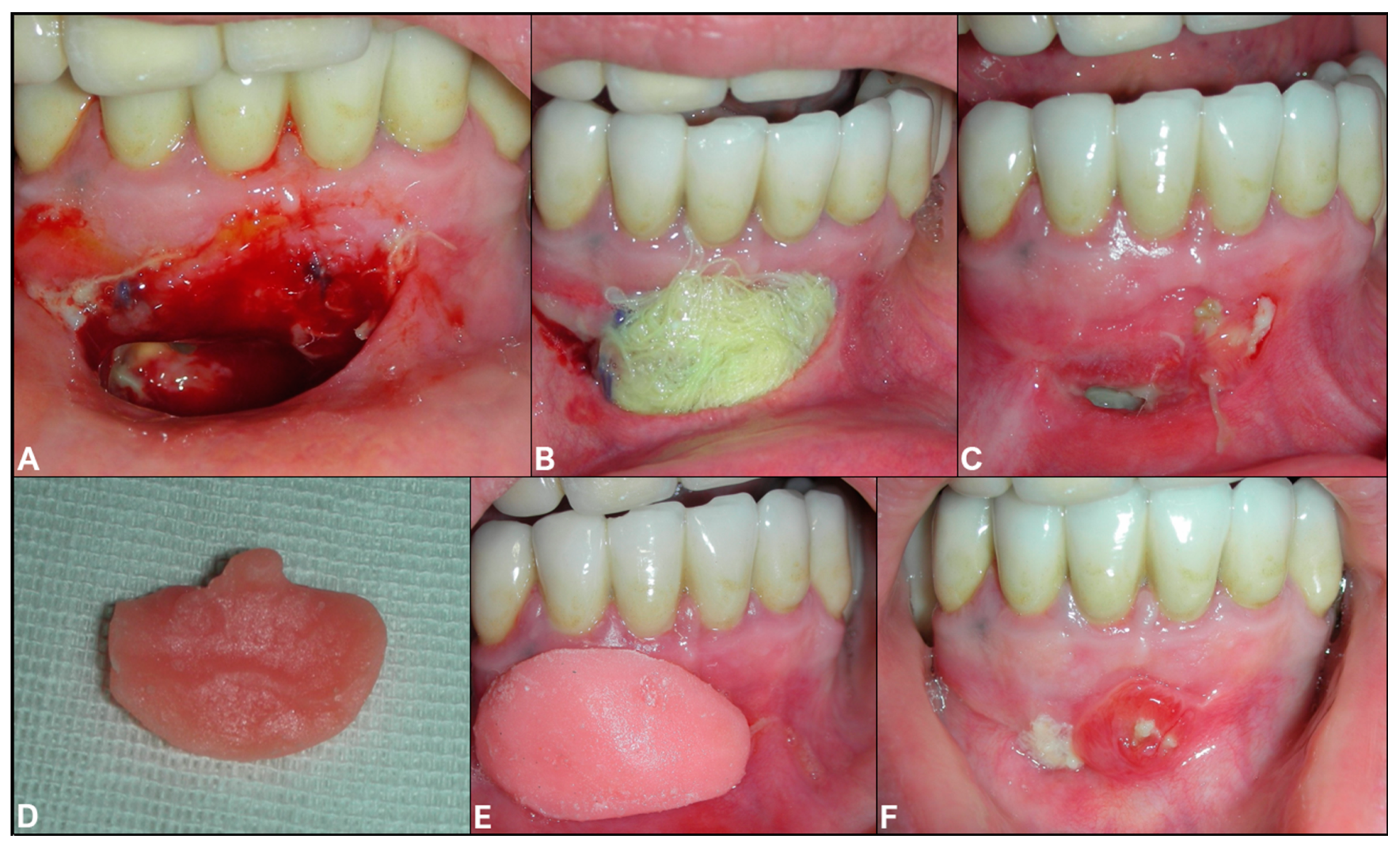
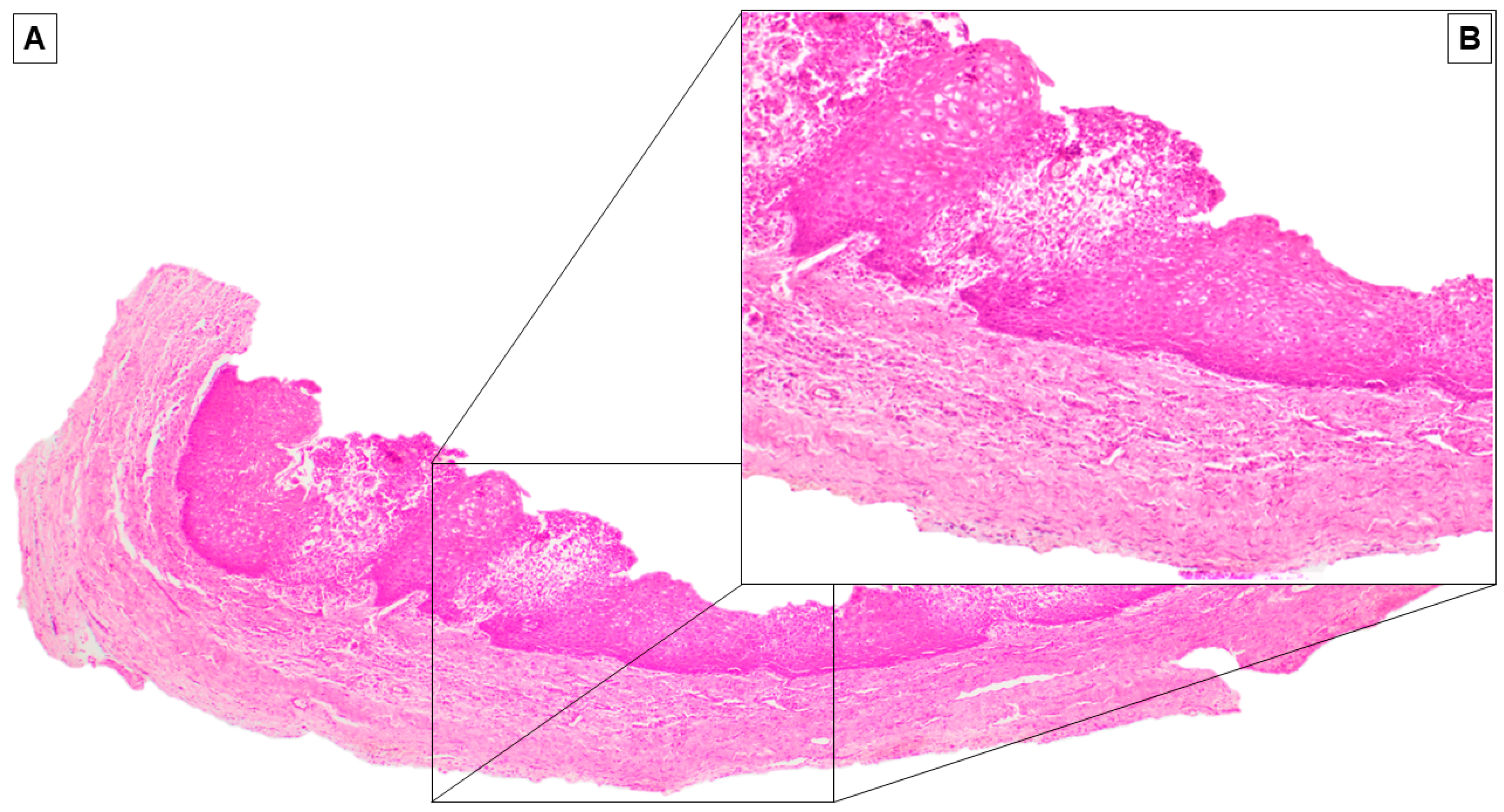
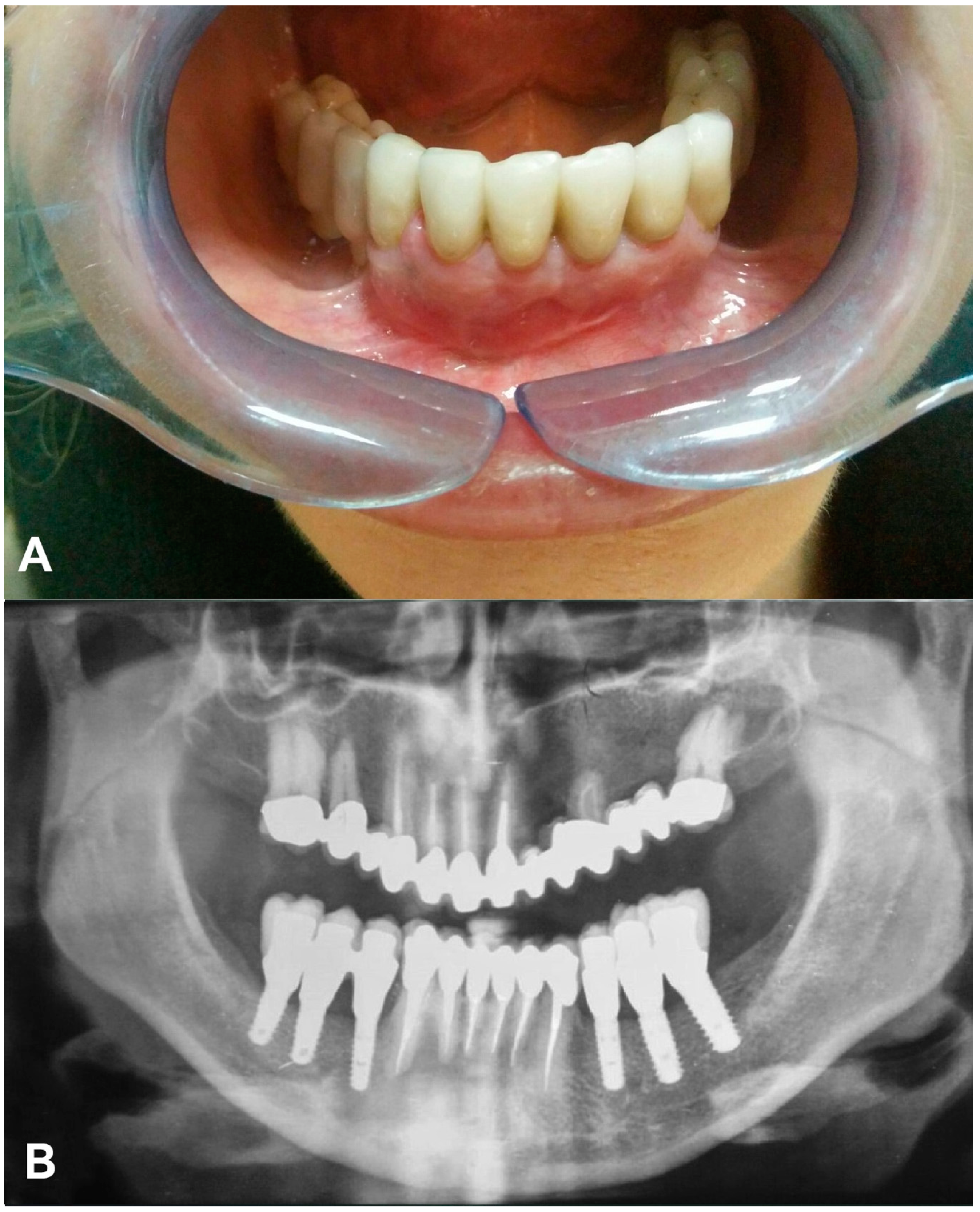
2. Case Report
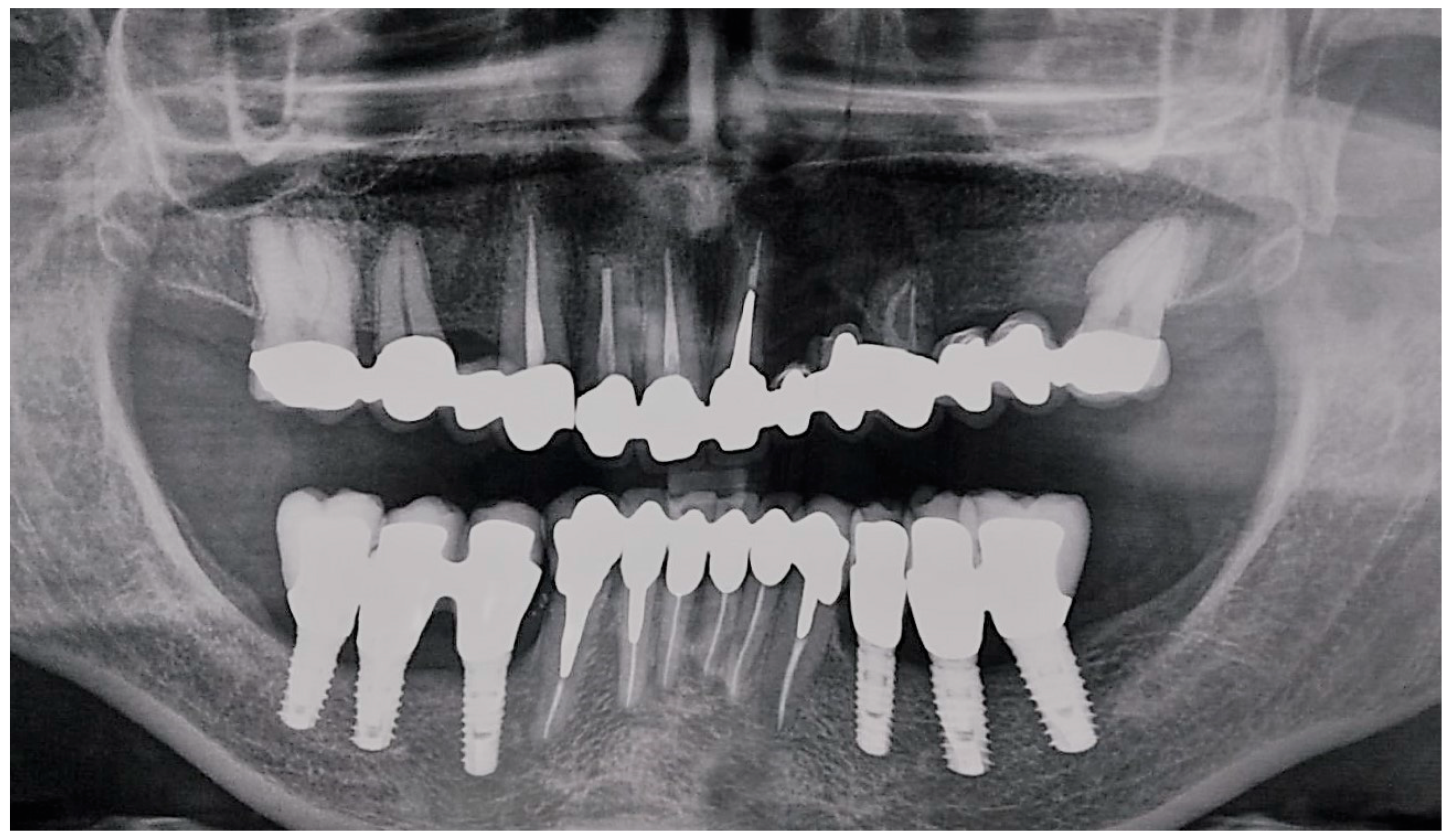
- Implant-supported prostheses from 3.4 to 3.6 and from 4.4 to 4.6.
- Prosthetic rehabilitation on dental support from 3.3 to 4.3. Metallic endocanalar posts in 3.3, 4.2, and 4.3.
- Endodontic treatment on 3.1, 3.2, 3.3, 4.1, 4.2, and 4.3.
3. Discussion
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Johnson, N.; Gannon, O.; Savage, N.W.; Batstone, M.D. Frequency of odontogenic cysts and tumors: A systematic review. J. Investig. Clin. Dent. 2013, 5, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Jansson, L.; Ehnevid, H.; Lindskog, S.; Blomlöf, L. Development of periapical lesions. Swed. Dent. J. 1993, 17, 85–93. [Google Scholar] [PubMed]
- Wright, J.M.; Vered, M. Update from the 4th Edition of the World Health Organization Classification of Head and Neck Tumours: Odontogenic and Maxillofacial Bone Tumors. Head Neck Pathol. 2017, 11, 68–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manor, E.; Kachko, L.; Puterman, M.B.; Szabo, G.; Bodner, L. Cystic Lesions of the Jaws—A Clinicopathological Study of 322 Cases and Review of the Literature. Int. J. Med. Sci. 2011, 9, 20–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giudice, R.L.; Puleio, F.; Rizzo, D.; Alibrandi, A.; Giudice, G.L.; Centofanti, A.; Fiorillo, L.; Di Mauro, D.; Nicita, F. Comparative Investigation of Cutting Devices on Bone Blocks: An SEM Morphological Analysis. Appl. Sci. 2019, 9, 351. [Google Scholar] [CrossRef] [Green Version]
- Castro-Núñez, J.; Information, P.E.K.F.C. Decompression of Odontogenic Cystic Lesions: Past, Present, and Future. J. Oral Maxillofac. Surg. 2016, 74, 104.e1–104.e9. [Google Scholar] [CrossRef] [PubMed]
- Piattelli, A.; Scarano, A.; Piattelli, M.; Podda, G. Implant periapical lesions: Clinical, histologic, and histochemical aspects. A case report. Int. J. Periodontics Restor. Dent. 1998, 18, 181–187. [Google Scholar]
- Oh, T.-J.; Yoon, J.; Wang, H.-L. Management of the Implant Periapical Lesion: A Case Report. Implant Dent. 2003, 12, 41–46. [Google Scholar] [CrossRef]
- Blaya-Tárraga, J.-A.; Cervera-Ballester, J.; Peñarrocha-Oltra, D.; Peñarrocha-Diago, M. Periapical implant lesion: A systematic review. Medicina Oral Patología Oral Y Cirugia Bucal 2017, 22, e737–e749. [Google Scholar] [CrossRef]
- Casado, P.; Donner, M.; Pascarelli, B.; Derocy, C.; Duarte, M.E.L.; Barboza, E.P. Immediate Dental Implant Failure Associated With Nasopalatine Duct Cyst. Implant Dent. 2008, 17, 169–175. [Google Scholar] [CrossRef] [Green Version]
- Karamanis, S.; Kitharas, T.; Tsoukalas, D.; Parissis, N. Implant Placement After Marsupialization of a Dentigerous Cyst. J. Oral Implant. 2006, 32, 313–316. [Google Scholar] [CrossRef] [PubMed]
- Aboulhosn, M.; Noujeim, Z.; Nader, N.; Berbéri, A. Decompression and Enucleation of a Mandibular Radicular Cyst, Followed by Bone Regeneration and Implant-Supported Dental Restoration. Case Rep. Dent. 2019, 2019, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aoki, N.; Ise, K.; Inoue, A.; Kosugi, Y.; Koyama, C.; Iida, M.; Baba, J.; Iwai, T.; Mitsudo, K. Multidisciplinary approach for treatment of a dentigerous cyst – marsupialization, orthodontic treatment, and implant placement: A case report. J. Med. Case Rep. 2018, 12, 305. [Google Scholar] [CrossRef] [PubMed]
- Al-Shamiri, H.M.; Elfaki, S.; Al-Maweri, S.; Alaizari, N.A.; Tarakji, B. Development of Nasopalatine Duct Cyst in Relation to Dental Implant Placement. N. Am. J. Med. Sci. 2016, 8, 13–16. [Google Scholar] [CrossRef] [Green Version]
- Narad, C.; Lingraj, J.; Aulakh, K.K.; Handa, K.; Kotrashetti, S.; Pinto, P. Assessment of primary stability of the implant placed in prepared infected extraction sockets. J. Oral Biol. Craniofacial Res. 2016, 8, 154–157. [Google Scholar] [CrossRef]
- Jofré, J.; Valenzuela, D.; Quintana, P.; Asenjo-Lobos, C. Protocol for Immediate Implant Replacement of Infected Teeth. Implant Dent. 2012, 21, 287–294. [Google Scholar] [CrossRef] [Green Version]
- Crespi, R.; Capparè, P.; Giudice, G.L.; Gastaldi, G.; Gherlone, E. Immediate Implant Placement in Sockets with Asymptomatic Apical Periodontitis. Clin. Implant Dent. Relat. Res. 2016, 19, 20–27. [Google Scholar] [CrossRef]
- Crespi, R.; Capparè, P.; Crespi, G.; Giudice, G.L.; Gastaldi, G.; Gherlone, E. Dental Implants Placed in Periodontally Infected Sites in Humans. Clin. Implant Dent. Relat. Res. 2016, 19, 131–139. [Google Scholar] [CrossRef] [Green Version]
- Solderer, A.; Al-Jazrawi, A.; Sahrmann, P.; Jung, R.E.; Attin, T.; Schmidlin, P. Removal of failed dental implants revisited: Questions and answers. Clin. Exp. Dent. Res. 2019, 5, 712–724. [Google Scholar] [CrossRef] [Green Version]
- Park, W.-B.; Kim, Y.-J.; Han, J.-Y.; Kang, P. Successful Management of Dental Implants in Postoperative Maxillary Cyst: A Case Report With a 13-Year Follow-Up. J. Oral Implant. 2020, 46, 133–138. [Google Scholar] [CrossRef]
- Jimbo, R.; Takahashi, T.; Takeshita, K.; Funaki, K. Nasopalatine duct cyst developed in association with dental implant treatment: A case report and histopathological observation. J. Oral Maxillofac. Pathol. 2013, 17, 319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sukegawa, S.; Kanno, T.; Kawai, H.; Takebe, Y.; Shibata, A.; Takahashi, Y.; Nagatsuka, H.; Furuki, Y. Nasopalatine duct cyst associated with dental implant treatment: A case report. Oral Maxillofac. Surg. Cases 2015, 1, 38–41. [Google Scholar] [CrossRef] [Green Version]
- Contar, C.M.M.; Thomé, C.A.; Pompermayer, A.; Sarot, J.R.; Vinagre, R.O.; Machado, M.A.N. Marsupialization of Dentigerous Cyst: Report of a Case. J. Maxillofac. Oral Surg. 2011, 14, 4–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, X.; Zhao, Y.-F.; Man, Q.-W.; Li, R.-F.; Liu, B.; Zhao, Y.-F. The effects of marsupialization on bone regeneration adjacent to keratocystic odontogenic tumors, and the mechanisms involved. J. Oral Sci. 2017, 59, 475–481. [Google Scholar] [CrossRef] [Green Version]
- Sennerby, L.; Meredith, N. Implant stability measurements using resonance frequency analysis: Biological and biomechanical aspects and clinical implications. Periodontology 2008, 47, 51–66. [Google Scholar] [CrossRef]
- Andreotti, A.M.; Goiato, M.C.; Nobrega, A.S.; Da Silva, E.V.F.; Filho, H.G.; Pellizzer, E.P.; Dos Santos, D.M. Relationship Between Implant Stability Measurements Obtained by Two Different Devices: A Systematic Review. J. Periodontol. 2017, 88, 281–288. [Google Scholar] [CrossRef]
- Lee, S.-T.; Kim, S.-G.; Moon, S.Y.; Oh, J.; You, J.-S.; Kim, J.-S. The effect of decompression as treatment of the cysts in the jaws: Retrospective analysis. J. Korean Assoc. Oral Maxillofac. Surg. 2017, 43, 83–87. [Google Scholar] [CrossRef] [Green Version]
- Moturi, K.; Puvvada, D.; Kotha, P.R. A Novel, Minimally Invasive Technique in the Management of a Large Cyst Involving the Maxilla in a Child: A Case Report. Cureus 2018, 10. [Google Scholar] [CrossRef] [Green Version]
- Castro-Núñez, J. An Innovative Decompression Device to Treat Odontogenic Cysts. J. Craniofacial Surg. 2016, 27, 1. [Google Scholar] [CrossRef]
- Lee, F. Ameloblastoma of the maxilla with probable origin in a residual cyst. Oral Surg. Oral Med. Oral Pathol. 1970, 29, 799–805. [Google Scholar] [CrossRef]
- Van Der Wal, K.G.; De Visscher, J.G.; Eggink, H.F. Squamous cell carcinoma arising in a residual cyst. A case report. Int. J. Oral Maxillofac. Surg. 1993, 22, 350–352. [Google Scholar] [CrossRef]
- Ghandour, L.; Bahmad, H.F.; Bou-Assi, S. Conservative Treatment of Dentigerous Cyst by Marsupialization in a Young Female Patient: A Case Report and Review of the Literature. Case Rep. Dent. 2018, 2018, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valderrama, P.; Thomas, G.W., Jr. Detoxification of Implant Surfaces Affected by Peri-Implant Disease: An Overview of Surgical Methods. Int. J. Dent. 2013, 2013, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Zabtotsky, M.H.; Diedrich, D.L.; Meffert, R.M. Detoxification of endotoxin-contaminated titanium and hydroxyapatite-coated surfaces utilizing various chemotherapeutic and mechanical modalities. Implant Dent. 1992, 1, 154–158. [Google Scholar] [CrossRef]
- An, Y.-Z.; Lee, J.-H.; Heo, Y.-K.; Lee, J.-S.; Jung, U.-W.; Choi, S.-H. Surgical Treatment of Severe Peri-Implantitis Using a Round Titanium Brush for Implant Surface Decontamination: A Case Report with Clinical Reentry. J. Oral Implant. 2017, 43, 218–225. [Google Scholar] [CrossRef] [PubMed]





© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Troiano, A.; Lo Giudice, G.; De Luca, R.; Lo Giudice, F.; D’Amato, S.; Tartaro, G.; Colella, G. Salvage of Dental Implant Located in Mandibular Odontogenic Cyst. A Conservative Surgical Treatment Proposal. Dent. J. 2020, 8, 49. https://0-doi-org.brum.beds.ac.uk/10.3390/dj8020049
Troiano A, Lo Giudice G, De Luca R, Lo Giudice F, D’Amato S, Tartaro G, Colella G. Salvage of Dental Implant Located in Mandibular Odontogenic Cyst. A Conservative Surgical Treatment Proposal. Dentistry Journal. 2020; 8(2):49. https://0-doi-org.brum.beds.ac.uk/10.3390/dj8020049
Chicago/Turabian StyleTroiano, Antonio, Giorgio Lo Giudice, Roberto De Luca, Fabrizio Lo Giudice, Salvatore D’Amato, Gianpaolo Tartaro, and Giuseppe Colella. 2020. "Salvage of Dental Implant Located in Mandibular Odontogenic Cyst. A Conservative Surgical Treatment Proposal" Dentistry Journal 8, no. 2: 49. https://0-doi-org.brum.beds.ac.uk/10.3390/dj8020049