Comparative Evaluation of Digitization of Diagnostic Dental Cast (Plaster) Models Using Different Scanning Technologies

 , , , and
, , , and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Experimental Models
2.2. Scanning Devices and Strategies
2.3. Image Registration and Accuracy Analysis
2.4. Statistical Analysis
3. Results
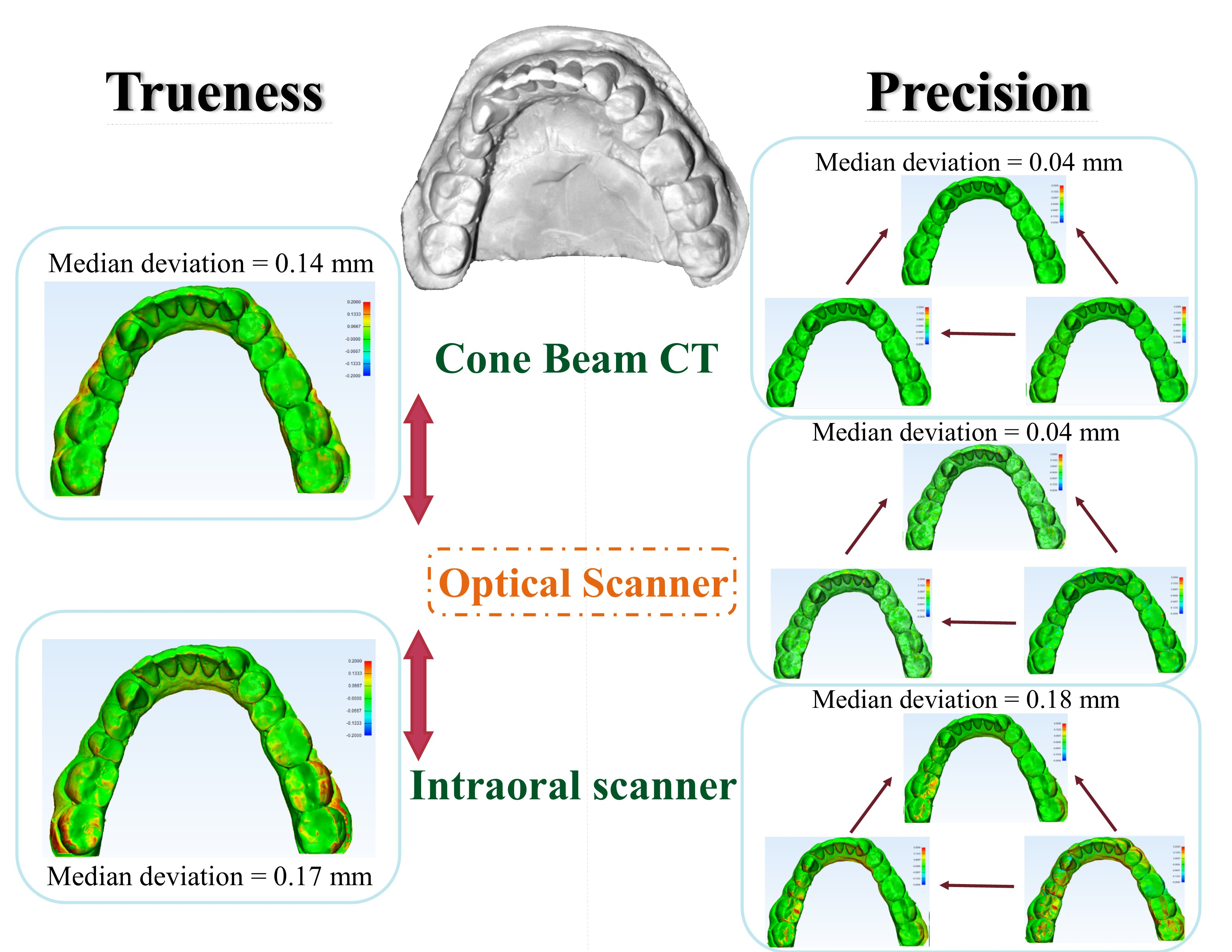
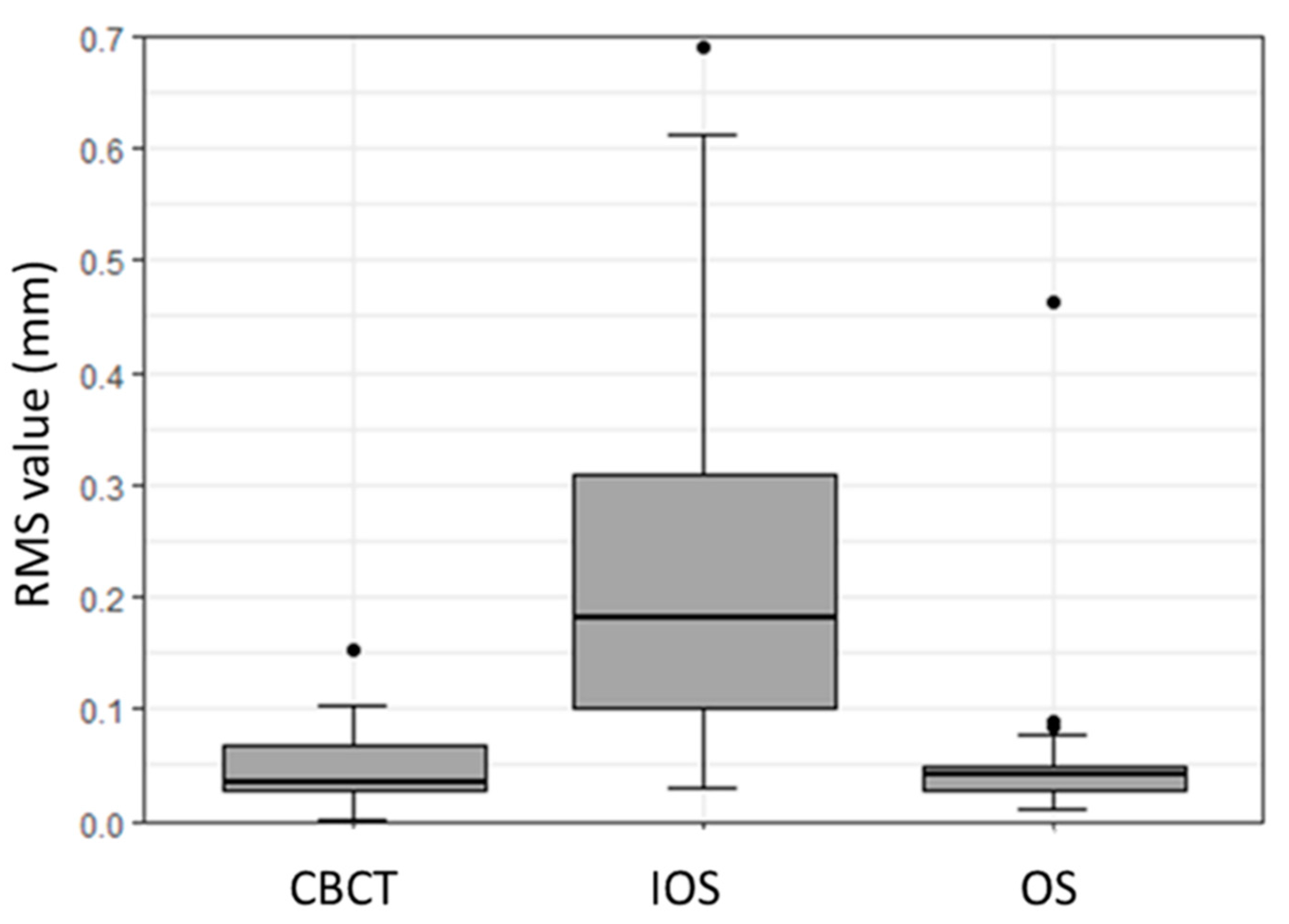
3.1. Precision Assessment
3.2. Trueness Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| ANOVA | Analysis of variance |
| CAD/CAM | Computer-aided design/computer-aided manufacturing |
| CBCT | Cone-beam computed tomography |
| DDT | Digital dental technology |
| IOS | Intraoral scanner |
| OS | Optical scanner |
| STL | Standard tessellation language |
| RMS | Root mean square |
| 3D | Three-dimensional |
References
- Shah, N.; Bansal, N.; Logani, A. Recent advances in imaging technologies in dentistry. World J. Radiol. 2014, 6, 794–807. [Google Scholar] [CrossRef] [PubMed]
- Joda, T.; Bragger, U. Digital vs. conventional implant prosthetic workflows: A cost/time analysis. Clin. Oral Implants Res. 2015, 26, 1430–1435. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Gallucci, G.O. Digital vs. conventional implant impressions: Efficiency outcomes. Clin. Oral Implants Res. 2013, 24, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Christensen, G.J. Will digital impressions eliminate the current problems with conventional impressions? J. Am. Dent. Assoc. 2008, 139, 761–763. [Google Scholar] [CrossRef]
- Fleming, P.S.; Marinho, V.; Johal, A. Orthodontic measurements on digital study models compared with plaster models: A systematic review. Orthod. Craniofac. Res. 2011, 14, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Marcel, T.J. Three-dimensional on-screen virtual models. Am. J. Orthod. Dentofacial. Orthop. 2001, 119, 666–668. [Google Scholar] [CrossRef]
- Peluso, M.J.; Josell, S.D.; Levine, S.W.; Lorei, B.J. Digital models: An introduction. Semin. Orthod. 2004, 10, 26–38. [Google Scholar] [CrossRef]
- Rekow, E.D. Dental CAD/CAM systems: A 20-year success story. J. Am. Dent. Assoc. 2006, 137, 5S–6S. [Google Scholar] [CrossRef] [Green Version]
- Beuer, F.; Schweiger, J.; Edelhoff, D. Digital dentistry: An overview of recent developments for CAD/CAM generated restorations. Br. Dent. J. 2008, 204, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Vlaar, S.T.; Zel, J.M. Accuracy of dental digitizers. Int. Dent. J. 2006, 56, 301–309. [Google Scholar] [CrossRef]
- Patzelt, S.B.; Emmanouilidi, A.; Stampf, S.; Strub, J.R.; Att, W. Accuracy of full-arch scans using intraoral scanners. Clin. Oral Investig. 2014, 18, 1687–1694. [Google Scholar] [CrossRef]
- Wiranto, M.G.; Engelbrecht, W.P.; Tutein, H.E.; Meer, W.J.; Ren, Y. Validity, reliability, and reproducibility of linear measurements on digital models obtained from intraoral and cone-beam computed tomography scans of alginate impressions. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 140–147. [Google Scholar] [CrossRef] [PubMed]
- Logozzo, S.; Zanetti, E.M.; Franceschini, G.; Kilpela, A.; Makynen, A. Recent advances in dental optics—Part I: 3D intraoral scanners for restorative dentistry. Opt. Lasers Eng. 2014, 54, 203–221. [Google Scholar] [CrossRef]
- International Organization for Standardization. Accuracy (Trueness and Precision) of Measurement Methods and Results—Part 1; General Principles and Definitions; International Organization for Standardization: Geneva, Switzerland, 1994. [Google Scholar]
- Flugge, T.V.; Schlager, S.; Nelson, K.; Nahles, S.; Metzger, M.C. Precision of intraoral digital dental impressions with iTero and extraoral digitization with the iTero and a model scanner. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 471–478. [Google Scholar] [CrossRef]
- Baumgaertel, S.; Palomo, M.; Palomo, L.; Hans, M.G. Reliability and accuracy of cone-beam computed tomography dental measurements. Am. J. Orthod. Dentofac. Orthop. 2009, 136, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Mangano, F.G.; Veronesi, G.; Hauschild, U.; Mijiritsky, E.; Mangano, C. Trueness and Precision of Four Intraoral Scanners in Oral Implantology: A Comparative In Vitro Study. PLoS ONE 2016, 11, e0163107. [Google Scholar] [CrossRef]
- Schnutenhaus, S.; Edelmann, C.; Rudolph, H.; Dreyhaupt, J.; Luthardt, R.G. 3D accuracy of implant positions in template-guided implant placement as a function of the remaining teeth and the surgical procedure: A retrospective study. Clin. Oral Investig. 2018, 22, 2363–2372. [Google Scholar] [CrossRef]
- Lemos, L.S.; Rebello, M.C.; Vogel, C.J.; Barbosa, M.C. Reliability of measurements made on scanned cast models using the 3 Shape R 700 scanner. Dentomaxillofac. Radiol. 2015, 44, 20140337. [Google Scholar] [CrossRef] [Green Version]
- Mandelli, F.; Gherlone, E.; Gastaldi, G.; Ferrari, M. Evaluation of the accuracy of extraoral laboratory scanners with a single-tooth abutment model: A 3D analysis. J. Prosthodont. Res. 2017, 61, 363–370. [Google Scholar] [CrossRef]
- Nowak, R.; Wesemann, C.; Robben, J.; Muallah, J.; Bumann, A. An In-Vitro study comparing the accuracy of full-arch casts digitized with desktop scanners. Quintessence Int. 2017, 48, 667–676. [Google Scholar] [CrossRef]
- De-Luca-Canto, G.; Pacheco-Pareira, C.; Lagravere, M.O.; Flores-Mir, C.; Major, P.W. Intra-arch dimensional measurement validity of laser-scanned digital dental models compared with the original plaster models: A systematic review. Orthod. Craniofac. Res. 2015, 18, 65–76. [Google Scholar] [CrossRef]
- Oh, K.C.; Lee, B.; Park, Y.B.; Moon, H.S. Accuracy of three digitization methods for the dental arch with various tooth preparation designs: An In Vitro study. J. Prosthodont. 2019, 28, 195–201. [Google Scholar] [CrossRef]
- Imburgia, M.; Logozzo, S.; Hauschild, U.; Veronesi, G.; Mangano, C.; Mangano, F.G. Accuracy of four intraoral scanners in oral implantology: A comparative In Vitro study. BMC Oral Health 2017, 17, 92. [Google Scholar] [CrossRef] [PubMed]
- Kim, R.J.; Park, J.M.; Shim, J.S. Accuracy of 9 intraoral scanners for complete-arch image acquisition: A qualitative and quantitative evaluation. J. Prosthet. Dent. 2018, 120, 895–903. [Google Scholar] [CrossRef] [PubMed]
- Becker, K.; Schmucker, U.; Schwarz, F.; Drescher, D. Accuracy and eligibility of CBCT to digitize dental plaster casts. Clin. Oral Investig. 2018, 22, 1817–1823. [Google Scholar] [CrossRef] [PubMed]
- Park, J.Y.; Kim, D.; Han, S.S.; Yu, H.S. Three-dimensional comparison of 2 digital models obtained from cone-beam computed tomographic scans of polyvinyl siloxane impressions and plaster models. Imaging Sci. Dent. 2019, 49, 257–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bilmenoglu, C.; Cilingir, A.; Geckili, O.; Bilhan, H.; Bilgin, T. In Vitro comparison of trueness of 10 intraoral scanners for implant-supported complete-arch fixed dental prostheses. J. Prosthet. Dent. 2020, S0022-3913(19)30754-1. [Google Scholar] [CrossRef]
- Anh, J.W.; Park, J.M.; Chun, Y.S.; Kim, M.; Kim, M. A comparison of the precision of three-dimensional images acquired by 2 digital intraoral scanners: Effects of tooth irregularity and scanning direction. Korean J. Orthod. 2016, 46, 3–12. [Google Scholar] [CrossRef] [Green Version]
- Maeng, J.; Lim, Y.G.; Kim, B.; Kim, M.J.; Kwon, H.B. A New Approach to Accuracy Evaluation of Single-Tooth Abutment Using Two-Dimensional Analysis in Two Intraoral Scanners. Int. J. Environ. Res. Public Health 2019, 16, 1021. [Google Scholar] [CrossRef] [Green Version]
- Abduo, J.E.M. Accuracy of Intraoral Scanners: A Systematic Review of Influencing Factors. Eur. J. Prosthodont. Restor. Dent. 2018, 26, 101–121. [Google Scholar] [CrossRef]
- Revilla-León, J.P.; Sadeghpour, M.; Piedra-Cascón, W.; Zandinejad, A.; Özcan, M.; Krishnamurthy, V.R. Intraoral digital scans-Part 1: Influence of ambient scanning light conditions on the accuracy (trueness and precision) of different intraoral scanners. J. Prosthet. Dent. 2019, S0022-3913(18)30992-2. [Google Scholar] [CrossRef]
- Michelinakis, G.; Apostolakis, D.; Tsagarakis, A.; Kourakis, G.; Pavlakis, E. A comparison of accuracy of 3 intraoral scanners: A single-blinded In Vitro study. J. Prosthet. Dent. 2019. [Google Scholar] [CrossRef]
- Zhang, F.; Suh, K.J.; Lee, K.M. Validity of Intraoral Scans Compared with Plaster Models: An In-Vivo Comparison of Dental Measurements and 3D Surface Analysis. PLoS ONE 2016, 11, e0157713. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, S.; Shinya, A.; Kuroda, S.; Gomi, H. The accuracy of the CAD system using intraoral and extraoral scanners for designing of fixed dental prostheses. Dent. Mater. J. 2017, 36, 402–407. [Google Scholar] [CrossRef] [Green Version]
- Favero, R.; Volpato, A.; Francesco, M.D.; Fiore, A.D.; Guazzo, R.; Favero, L. Accuracy of 3D digital modeling of dental arches. Dental Press J. Orthod. 2019, 24, 38e1–38e7. [Google Scholar] [CrossRef] [Green Version]
- Alikhasi, M.; Siadat, H.; Nasirpour, A.; Hasanzade, M. Three-Dimensional Accuracy of Digital Impression versus Conventional Method: Effect of Implant Angulation and Connection Type. Int. J. Dent. 2018. [Google Scholar] [CrossRef] [PubMed]
- Sim, J.Y.; Jang, Y.; Kim, W.C.; Kim, H.Y.; Lee, D.H.; Kim, J.H. Comparing the accuracy (trueness and precision) of models of fixed dental prostheses fabricated by digital and conventional workflows. J. Prosthodont. Res. 2019, 63, 25–30. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Kennedy Classification | ||
|---|---|---|
| Group | Maxillary Model | Mandibular Model |
| Case 1 | Not applicable | Class III |
| Case 2 | Class III | Not applicable |
| Case 3 | Not applicable | Not applicable |
| Case 4 | Not applicable | Class III |
| Case 5 | Class III | Not applicable |
| Scanner | Mean (SD) | Median (Q1 to Q3) | Range |
|---|---|---|---|
| OS | 0.06 (0.08) | 0.04 (0.03 to 0.05) | 0.01 to 0.46 |
| IOS | 0.23 (0.18) | 0.18 (0.1 to 0.31) | 0.03 to 0.69 |
| CBCT | 0.05 (0.03) | 0.04 (0.03 to 0.07) | 0.002 to 0.15 |
| CBCT (max.) | CBCT (mand.) | OS (max.) | OS (mand.) | IOS (max.) | |
|---|---|---|---|---|---|
| CBCT (mand.) | 0.03 | ||||
| OS (max.) | 0.378 | 0.376 | |||
| OS (mand.) | 0.411 | 0.376 | 0.862 | ||
| IOS (max.) | <0.01 * | <0.01 * | <0.01 * | <0.01 * | |
| IOS (mand.) | <0.01 * | <0.01 * | <0.01 * | <0.01 * | 0.376 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Emara, A.; Sharma, N.; Halbeisen, F.S.; Msallem, B.; Thieringer, F.M. Comparative Evaluation of Digitization of Diagnostic Dental Cast (Plaster) Models Using Different Scanning Technologies. Dent. J. 2020, 8, 79. https://0-doi-org.brum.beds.ac.uk/10.3390/dj8030079
Emara A, Sharma N, Halbeisen FS, Msallem B, Thieringer FM. Comparative Evaluation of Digitization of Diagnostic Dental Cast (Plaster) Models Using Different Scanning Technologies. Dentistry Journal. 2020; 8(3):79. https://0-doi-org.brum.beds.ac.uk/10.3390/dj8030079
Chicago/Turabian StyleEmara, Aalaa, Neha Sharma, Florian S. Halbeisen, Bilal Msallem, and Florian M. Thieringer. 2020. "Comparative Evaluation of Digitization of Diagnostic Dental Cast (Plaster) Models Using Different Scanning Technologies" Dentistry Journal 8, no. 3: 79. https://0-doi-org.brum.beds.ac.uk/10.3390/dj8030079