
Accuracy of Guided Surgery and Real-Time Navigation in Temporomandibular Joint Replacement Surgery

 , , and
, , and {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Virtual Surgical Planning (VSP)
2.2. Drilling Procedure
2.3. Data Evaluation
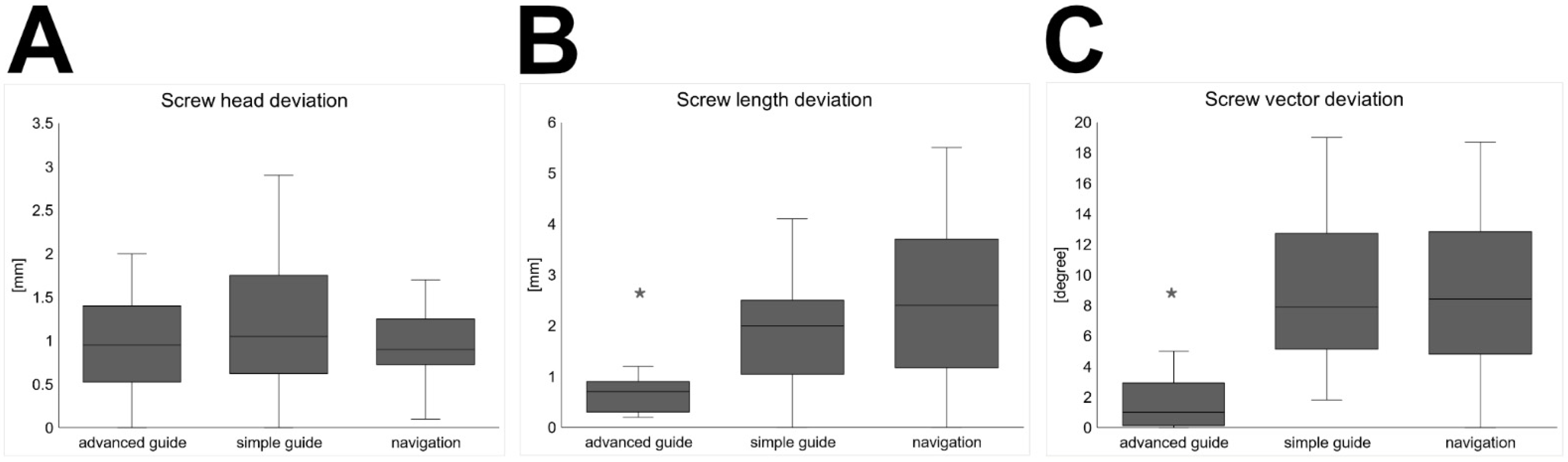
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Guarda-Nardini, L.; Manfredini, D.; Ferronato, G. Temporomandibular joint total replacement prosthesis: Current knowledge and considerations for the future. Int. J. Oral Maxillofac. Surg. 2008, 37, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Aagaard, E.; Thygesen, T. A prospective, single-centre study on patient outcomes following temporomandibular joint replacement using a custom-made Biomet TMJ prosthesis. Int. J. Oral Maxillofac. Surg. 2014, 43, 1229–1235. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.E.; Robinson, M. A new surgical procedure in bilateral reconstruction of condyles, utilizing iliac bone grafts and creation of new joints by means of non-electrolytic metal. A preliminary report. Plast. Reconstr. Surg. 1952, 9, 393–409. [Google Scholar] [CrossRef] [PubMed]
- Ware, W.H.; Taylor, R.C. Cartilaginous growth centers transplanted to replace mandibular condyles in monkeys. J. Oral Surg. 1966, 24, 33–43. [Google Scholar] [CrossRef] [PubMed]
- Matukas, V.J.; Szymela, V.F.; Schmidt, J.F. Surgical treatment of bony ankylosis in a child using a composite cartilage-bone iliac crest graft. J. Oral Surg. 1980, 38, 903–905. [Google Scholar] [PubMed]
- Wolford, L.M.; Cottrell, D.A.; Henry, C. Sternoclavicular grafts for temporomandibular joint reconstruction. J. Oral Maxillofac. Surg. 1994, 52, 119–128. [Google Scholar] [CrossRef]
- Mercuri, L.G. Total joint reconstruction—Autologous or alloplastic. Oral Maxillofac. Surg. Clin. N. Am. 2006, 18, 399–410. [Google Scholar] [CrossRef]
- Henry, C.H.; Wolford, L.M. Treatment outcomes for temporomandibular joint reconstruction after Proplast-Teflon implant failure. J. Oral Maxillofac. Surg. 1993, 51, 352–358. [Google Scholar] [CrossRef]
- Lindqvist, C.; Söderholm, A.L.; Hallikainen, D.; Sjövall, L. Erosion and heterotopic bone formation after alloplastic temporomandibular joint reconstruction. J. Oral Maxillofac. Surg. 1992, 50, 942–949. [Google Scholar] [CrossRef]
- Westermark, A.; Koppel, D.; Leiggener, C. Condylar replacement alone is not sufficient for prosthetic reconstruction of the temporomandibular joint. Int. J. Oral Maxillofac. Surg. 2006, 35, 488–492. [Google Scholar] [CrossRef]
- Elledge, R.; Mercuri, L.G.; Speculand, B. Extended total temporomandibular joint replacements: A classification system. Br. J. Oral Maxillofac. Surg. 2018, 56, 578–581. [Google Scholar] [CrossRef]
- Sidebottom, A.J.; Gruber, E. One-year prospective outcome analysis and complications following total replacement of the temporomandibular joint with the TMJ Concepts system. Br. J. Oral Maxillofac. Surg. 2013, 51, 620–624. [Google Scholar] [CrossRef]
- Neuhaus, M.T.; Zeller, A.N.; Jehn, P.; Lethaus, B.; Gellrich, N.C.; Zimmerer, R.M. Intraoperative real-time navigation and intraoperative three-dimensional imaging for patient-specific total temporomandibular joint replacement. Int. J. Oral Maxillofac. Surg. 2021. [Google Scholar] [CrossRef]
- Verstreken, K.; Van Cleynenbreugel, J.; Marchal, G.; Van Steenberghe, D.; Suetens, P. Computer-assisted planning of oral implant surgery: An approach using virtual reality. Stud. Health Technol. Inform. 1996, 29, 423–434. [Google Scholar] [CrossRef]
- Jacobs, R.; Adriansens, A.; Verstreken, K.; Suetens, P.; Van Steenberghe, D. Predictability of a three-dimensional planning system for oral implant surgery. Dentomaxillofac. Radiol. 1999, 28, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Flügge, T.V.; Nelson, K.; Schmelzeisen, R.; Metzger, M.C. Three-dimensional plotting and printing of an implant drilling guide: Simplifying guided implant surgery. J. Oral Maxillofac. Surg. 2013, 71, 1340–1346. [Google Scholar] [CrossRef]
- Schmelzeisen, R.; Gellrich, N.C.; Schramm, A.; Schn, R.; Otten, J.E. Navigation-guided resection of temporomandibular joint ankylosis promotes safety in skull base surgery. J. Oral Maxillofac. Surg. 2002, 60, 1275–1283. [Google Scholar] [CrossRef] [PubMed]
- Schramm, A.; Gellrich, N.C.; Schmelzeisen, R. Navigational Surgery of the Facial Skeleton; Springer: Berlin/Heidelberg, Germany, 2007; pp. 1–170. [Google Scholar] [CrossRef]
- Heiland, M.; Habermann, C.R.; Schmelzle, R. Indications and limitations of intraoperative navigation in maxillofacial surgery. J. Oral Maxillofac. Surg. 2004, 62, 1059–1063. [Google Scholar] [CrossRef] [PubMed]
- Boccalatte, L.A.; Nassif, M.G.; Figari, M.; Gómez, N.L.; Argibay, M.C.; Mancino, A.V.; Ritacco, L.E. Computer-assisted surgery for replacement of the temporomandibular joint with customized prostheses: Can we validate the results? Oral Maxillofac. Surg. 2020, 24, 317–325. [Google Scholar] [CrossRef]
- Ackland, D.C.; Robinson, D.; Redhead, M.; Lee, P.V.S.; Moskaljuk, A.; Dimitroulis, G. A personalized 3D-printed prosthetic joint replacement for the human temporomandibular joint: From implant design to implantation. J. Mech. Behav. Biomed. Mater. 2017, 69, 404–411. [Google Scholar] [CrossRef] [PubMed]
- Movahed, R.; Teschke, M.; Wolford, L.M. Protocol for concomitant temporomandibular joint custom-fitted total joint reconstruction and orthognathic surgery utilizing computer-assisted surgical simulation. J. Oral Maxillofac. Surg. 2013, 71, 2123–2129. [Google Scholar] [CrossRef] [PubMed]
- Movahed, R.; Wolford, L.M. Protocol for concomitant temporomandibular joint custom-fitted total joint reconstruction and orthognathic surgery using computer-assisted surgical simulation. Oral Maxillofac. Surg. Clin. N. Am. 2015, 27, 37–45. [Google Scholar] [CrossRef] [PubMed]
- Wolford, L.M. Computer-assisted surgical simulation for concomitant temporomandibular joint custom-fitted total joint reconstruction and orthognathic surgery. Atlas Oral Maxillofac. Surg. Clin. N. Am. 2016, 24, 55–66. [Google Scholar] [CrossRef]
- Wilde, F.; Hanken, H.; Probst, F.; Schramm, A.; Heiland, M.; Cornelius, C.-P. Multicenter study on the use of patient-specific CAD/CAM reconstruction plates for mandibular reconstruction. Int. J. CARS 2015, 10, 2035–2051. [Google Scholar] [CrossRef] [PubMed]
- Gomez, N.L.; Boccalatte, L.A.; Ruiz, Á.L.; Nassif, M.G.; Figari, M.F.; Ritacco, L. Total temporomandibular joint replacement and simultaneous orthognathic surgery using computer-assisted surgery. J. Maxillofac. Oral Surg. 2020, 20, 394–403. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Neuhaus, M.-T.; Zeller, A.-N.; Bartella, A.K.; Sander, A.K.; Lethaus, B.; Zimmerer, R.M. Accuracy of Guided Surgery and Real-Time Navigation in Temporomandibular Joint Replacement Surgery. Dent. J. 2021, 9, 87. https://0-doi-org.brum.beds.ac.uk/10.3390/dj9080087
Neuhaus M-T, Zeller A-N, Bartella AK, Sander AK, Lethaus B, Zimmerer RM. Accuracy of Guided Surgery and Real-Time Navigation in Temporomandibular Joint Replacement Surgery. Dentistry Journal. 2021; 9(8):87. https://0-doi-org.brum.beds.ac.uk/10.3390/dj9080087
Chicago/Turabian StyleNeuhaus, Michael-Tobias, Alexander-Nicolai Zeller, Alexander K. Bartella, Anna K. Sander, Bernd Lethaus, and Rüdiger M. Zimmerer. 2021. "Accuracy of Guided Surgery and Real-Time Navigation in Temporomandibular Joint Replacement Surgery" Dentistry Journal 9, no. 8: 87. https://0-doi-org.brum.beds.ac.uk/10.3390/dj9080087