
Pilot Study to Reduce Added Salt on a University Canteen through the Use of an Innovative Dosage Equipment

 , , ,
, , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.1.1. Step 1—Baseline Assessment
2.1.2. Step 2—Intervention
2.2. Salt Content of Meals
2.2.1. Sodium Analysis
2.2.2. Added Salt Levels
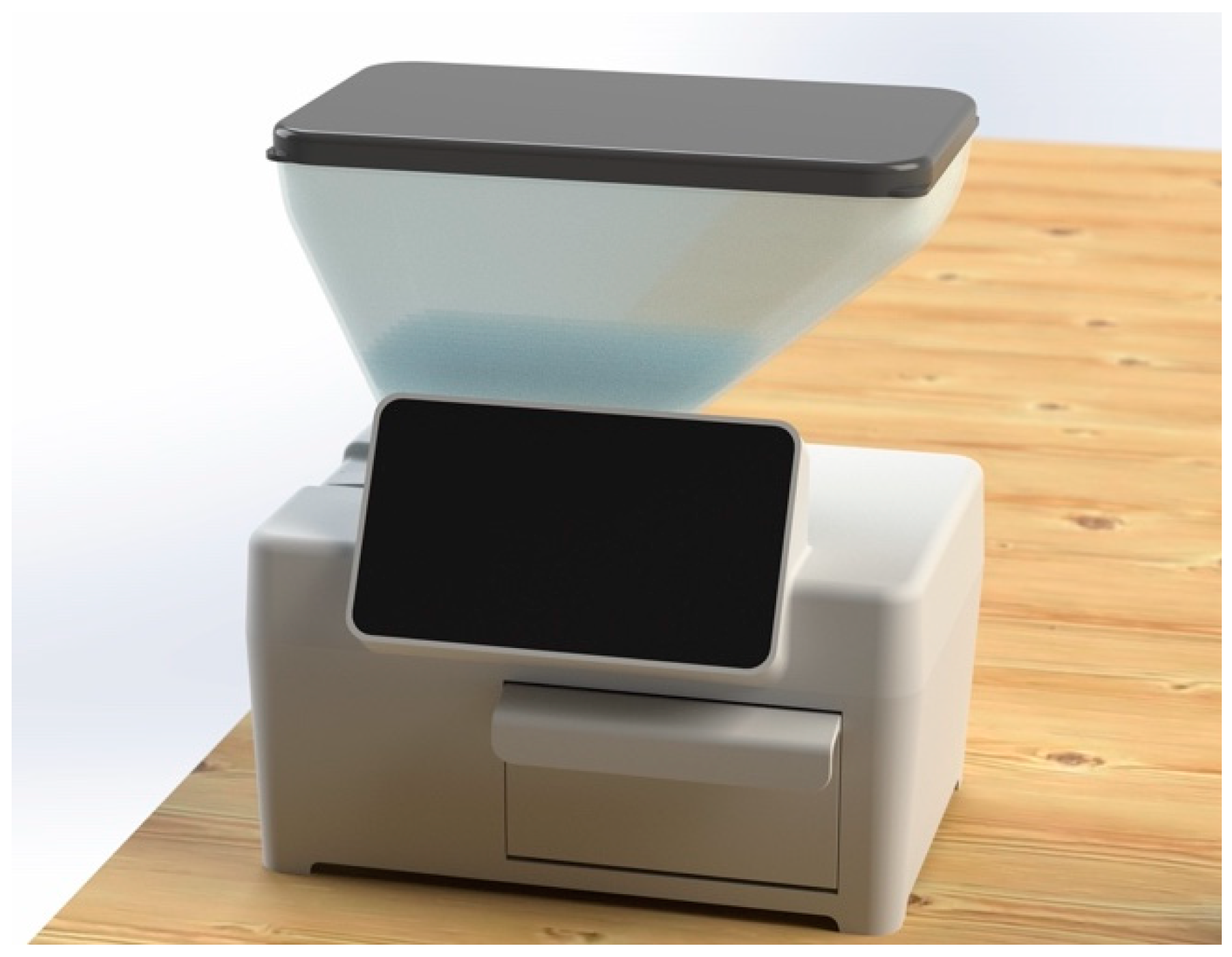
2.3. Equipment to Dosage Cooking Salt: SC-C
2.4. Satisfaction
2.4.1. Consumers Satisfaction Questionnaires
2.4.2. Consumers Food Waste
2.4.3. Food Handlers Satisfaction Questionnaires
2.5. Data Analysis
2.6. Ethics Committee
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Mean ± SD | Baseline Week 1–3 (n = 5) | Week 7–8 (n = 3) | Week 9–10 (n = 3) | Week 11 (n = 3) | ||
|---|---|---|---|---|---|---|
| Control Canteen | Soup | g/100 g | 0.4 ± 0.1 | 0.4 ± 0.1 | 0.5 ± 0.0 | 0.7 ± 0.2 |
| g/portion | 1.1 ± 0.4 | 1.1 ± 0.3 | 1.4 ± 0.2 | 2.4 ± 0.5 | ||
| Vegetarian | g/100 g | 0.8 ± 0.2 | 0.4 ± 0.2 | 0.7 ± 0.2 | 0.8 ± 0.2 | |
| g/portion | 2.5 ± 0.7 | 1.6 ± 0.9 | 3.1 ± 0.7 | 3.6 ± 0.7 | ||
| Meat | g/100 g | 0.8 ± 0.3 | 0.6 ± 0.2 | 0.9 ± 0.4 | 0.9 ± 0.1 | |
| g/portion | 2.7 ± 1.0 | 2.6 ± 1.2 | 3.4 ± 1.2 | 3.5 ± 1.0 | ||
| Fish | g/100 g | 0.5 ± 0.3 | 0.6 ± 0.3 | 0.5 ± 0.2 | 0.9 ± 0.3 | |
| g/portion | 1.5 ± 0.8 | 2.1 ± 1.2 | 1.9 ± 0.6 | 3.4 ± 1.1 | ||
| Intervention Canteen | Soup | g/100 g | 0.8 ± 0.2 | 0.5 ± 0.1 | 0.5 ± 0.2 | 0.5 ± 0.1 |
| g/portion | 2.5 ± 0.7 | 1.3 ± 0.4 | 1.4 ± 0.6 | 1.3 ± 0.3 | ||
| Vegetarian | g/100 g | 0.7 ± 0.3 | 0.6 ± 0.1 | 0.7 ± 0.2 | 0.8 ± 0.3 | |
| g/portion | 2.9 ± 1.4 | 2.4 ± 0.3 | 3.1 ± 1.1 | 3.2 ± 0.8 | ||
| Meat | g/100 g | 1.1 ± 0.7 | 0.8 ± 0.3 | 0.8 ± 0.1 | 0.7 ± 0.2 | |
| g/portion | 4.3 ± 2.4 | 3.3 ± 1.6 | 2.3 ± 0.6 | 2.8 ± 1.1 | ||
| Fish | g/100 g | 0.9 ± 0.4 | 1.0 ± 0.6 | 0.8 ± 0.1 | 0.6 ± 0.1 | |
| g/portion | 3.6 ± 2.1 | 3.3 ± 1.7 | 2.7 ± 0.8 | 1.6 ± 0.5 |
References
- Bibbins-Domingo, K.; Chertow, G.M.; Coxson, P.G.; Moran, A.; Lightwood, J.M.; Pletcher, M.J.; Goldman, L. Projected effect of dietary salt reductions on future cardiovascular disease. N. Engl. J. Med. 2010, 362, 590–599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cappuccio, F.P. Cardiovascular and other effects of salt consumption. Kidney Int. Suppl. 2013, 3, 312–315. [Google Scholar] [CrossRef] [Green Version]
- Ezzati, M.; Lopez, A.D.; Rodgers, A.; Vander Hoorn, S.; Murray, C.J.; Group, C.R.A.C. Selected major risk factors and global and regional burden of disease. Lancet 2002, 360, 1347–1360. [Google Scholar] [CrossRef]
- Graudal, N.A.; Hubeck-Graudal, T.; Jurgens, G. Effects of low sodium diet versus high sodium diet on blood pressure, renin, aldosterone, catecholamines, cholesterol, and triglyceride. Cochrane Database Syst. Rev. 2020, 12, CD004022. [Google Scholar]
- He, F.J.; MacGregor, G.A. Importance of salt in determining blood pressure in children: Meta-analysis of controlled trials. Hypertension 2006, 48, 861–869. [Google Scholar] [CrossRef]
- He, F.J.; MacGregor, G.A. A comprehensive review on salt and health and current experience of worldwide salt reduction programmes. J. Hum. Hypertens. 2009, 23, 363–384. [Google Scholar] [CrossRef]
- WHO. Guideline: Sodium Intake for Adults and Children; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- Afshin, A.; Sur, P.J.; Fay, K.A.; Cornaby, L.; Ferrara, G.; Salama, J.S.; Mullany, E.C.; Abate, K.H.; Abbafati, C.; Abebe, Z. Health effects of dietary risks in 195 countries, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef] [Green Version]
- Timmis, A.; Townsend, N.; Gale, C.; Grobbee, R.; Maniadakis, N.; Flather, M.; Wilkins, E.; Wright, L.; Vos, R.; Bax, J. European Society of Cardiology: Cardiovascular disease statistics 2017. Eur. Heart J. 2018, 39, 508–579. [Google Scholar] [CrossRef] [Green Version]
- Leal, J.; Luengo-Fernández, R.; Gray, A.; Petersen, S.; Rayner, M. Economic burden of cardiovascular diseases in the enlarged European Union. Eur. Heart J. 2006, 27, 1610–1619. [Google Scholar] [CrossRef] [Green Version]
- Gregório, M.J.; Sousa, S.d.; Ferreira, B.; Figueira, I.; Taipa, M.; Bica, M.; Amaral, T.; Graça, P. Relatório do Programa Nacional para a Promoção da Alimentação Saudável 2020. Direção-Geral Da Saúde 2020. Available online: https://alimentacaosaudavel.dgs.pt/activeapp2020/wp-content/uploads/2020/11/Relato%CC%81rio-PNPAS-2020.pdf (accessed on 20 October 2021).
- Collins, M.; Mason, H.; O’Flaherty, M.; Guzman-Castillo, M.; Critchley, J.; Capewell, S. An economic evaluation of salt reduction policies to reduce coronary heart disease in England: A policy modeling study. Value Health 2014, 17, 517–524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Webb, M.; Fahimi, S.; Singh, G.M.; Khatibzadeh, S.; Micha, R.; Powles, J.; Mozaffarian, D. Cost effectiveness of a government supported policy strategy to decrease sodium intake: Global analysis across 183 nations. BMJ 2017, 356, i6699. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Reducing Salt Intake in Populations: Report of a WHO Forum and Technical Meeting; World Health Organization: Paris, France, 2007. [Google Scholar]
- Asaria, P.; Chisholm, D.; Mathers, C.; Ezzati, M.; Beaglehole, R. Chronic disease prevention: Health effects and financial costs of strategies to reduce salt intake and control tobacco use. Lancet 2007, 370, 2044–2053. [Google Scholar] [CrossRef]
- Beaglehole, R.; Bonita, R.; Horton, R.; Adams, C.; Alleyne, G.; Asaria, P.; Baugh, V.; Bekedam, H.; Billo, N.; Casswell, S. Priority actions for the non-communicable disease crisis. Lancet 2011, 377, 1438–1447. [Google Scholar] [CrossRef]
- Selmer, R.M.; Kristiansen, I.S.; Haglerød, A.; Graff-Iversen, S.; Larsen, H.K.; Meyer, H.E.; Bønaa, K.H.; Thelle, D.S. Cost and health consequences of reducing the population intake of salt. J. Epidemiol. Community Health 2000, 54, 697–702. [Google Scholar] [CrossRef] [Green Version]
- Graça, P. Relatório Estratégia Para a Redução Do Consumo de Sal na Alimentação em Portugal; Direção-Geral da Saúde: Lisboa, Portugal, 2013. [Google Scholar]
- WHO. Global Action Plan for the Prevention and Control of Noncommunicable Diseases 2013–2020; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Brown, I.J.; Tzoulaki, I.; Candeias, V.; Elliott, P. Salt intakes around the world: Implications for public health. Int. J. Epidemiol. 2009, 38, 791–813. [Google Scholar] [CrossRef] [Green Version]
- Gonçalves, C.; Abreu, S.; Padrão, P.; Pinho, O.; Graça, P.; Breda, J.; Santos, R.; Moreira, P. Sodium and potassium urinary excretion and dietary intake: A cross-sectional analysis in adolescents. Food Nutr. Res. 2016, 60, 29442. [Google Scholar] [CrossRef] [Green Version]
- Sanchez-Castillo, C.; Warrender, S.; Whitehead, T.; James, W. An assessment of the sources of dietary salt in a British population. Clin. Sci. 1987, 72, 95–102. [Google Scholar] [CrossRef] [Green Version]
- Mattes, R.D.; Donnelly, D. Relative contributions of dietary sodium sources. J. Am. Coll. Nutr. 1991, 10, 383–393. [Google Scholar] [CrossRef]
- Goncalves, C.; Silva, G.; Pinho, O.; Camelo, S.; Amaro, L.; Teixeira, V.; Padrao, P.; Moreira, P. Sodium content in vegetable soups prepared outside the home: Identifying the problem. In Proceedings of the International Symposium on Occupational Safety and Hygiene, Guimarães, Portugal, 9–10 February 2012; pp. 278–281. [Google Scholar]
- Gonçalves, C.; Pinho, O.; Padrão, P.; Santos, C.; Abreu, S.; Moreira, P. Knowledge and practices related to added salt in meals by food handlers. Nutricias 2014, 21, 20–24. [Google Scholar]
- Beauchamp, G.K.; Cowart, B.J. Preference for high salt concentrations among children. Dev. Psychol. 1990, 26, 539. [Google Scholar] [CrossRef]
- Beauchamp, G.K.; Engelman, K. High salt intake. Sensory and behavioral factors. Hypertension 1991, 17, I176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Birch, L.L.; Fisher, J.O. Development of eating behaviors among children and adolescents. Pediatrics 1998, 101, 539–549. [Google Scholar] [CrossRef] [PubMed]
- Leshem, M. Biobehavior of the human love of salt. Neurosci. Biobehav. Rev. 2009, 33, 1–17. [Google Scholar] [CrossRef]
- Sullivan, S.A.; Birch, L.L. Pass the sugar, pass the salt: Experience dictates preference. Dev. Psychol. 1990, 26, 546. [Google Scholar] [CrossRef]
- Bertino, M.; Beauchamp, G.K.; Engelman, K. Long-term reduction in dietary sodium alters the taste of salt. Am. J. Clin. Nutr. 1982, 36, 1134–1144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blais, C.A.; Pangborn, R.M.; Borhani, N.O.; Ferrell, M.F.; Prineas, R.J.; Laing, B. Effect of dietary sodium restriction on taste responses to sodium chloride: A longitudinal study. Am. J. Clin. Nutr. 1986, 44, 232–243. [Google Scholar] [CrossRef]
- Kim, G.; Lee, H. Frequent consumption of certain fast foods may be associated with an enhanced preference for salt taste. J. Hum. Nutr. Diet. 2009, 22, 475–480. [Google Scholar] [CrossRef] [PubMed]
- Lucas, L.; Riddell, L.; Liem, G.; Whitelock, S.; Keast, R. The influence of sodium on liking and consumption of salty food. J. Food Sci. 2011, 76, S72–S76. [Google Scholar] [CrossRef]
- Dorresteijn, J.A.; van der Graaf, Y.; Zheng, K.; Spiering, W.; Visseren, F.L. The daily 10 kcal expenditure deficit: A before-and-after study on low-cost interventions in the work environment. BMJ Open 2013, 3, e002125. [Google Scholar] [CrossRef] [Green Version]
- Reynoso-Marreros, I.A.; Piñarreta-Cornejo, P.K.; Mayta-Tristán, P.; Bernabé-Ortiz, A. Effect of a salt-reduction strategy on blood pressure and acceptability among customers of a food concessionaire in Lima, Peru. Nutr. Diet. 2019, 76, 250–256. [Google Scholar] [CrossRef]
- Mozaffarian, D.; Afshin, A.; Benowitz, N.L.; Bittner, V.; Daniels, S.R.; Franch, H.A.; Jacobs, D.R., Jr.; Kraus, W.E.; Kris-Etherton, P.M.; Krummel, D.A. Population approaches to improve diet, physical activity, and smoking habits: A scientific statement from the American Heart Association. Circulation 2012, 126, 1514–1563. [Google Scholar] [CrossRef]
- Mota, I.; Padrão, P.; Silva-Santos, T.; Pinho, O.; Gonçalves, C. Intervenções para a redução do sal em cantinas. Ata Port. Nutr. 2021, 25, 70–75. [Google Scholar]
- Ferreira, I.M.; Lima, J.L.; Rangel, A.O. Flow injection sequential determination of chloride by potentiometry and sodium by flame emission spectrometry in instant soups. Anal. Sci. 1994, 10, 801–805. [Google Scholar] [CrossRef] [Green Version]
- INSA. Tabela da Composição dos Alimentos-PortFIR. Available online: http://portfir.insa.pt/recipe/compose (accessed on 2 September 2021).
- Oliveira, D.; Liz Martins, M.; Fonseca, L.; Rocha, A. Food waste index as an indicator of menu adequacy and acceptability in a Portuguese mental health hospital. Acta Port. Nutr. 2020, 20, 14–18. [Google Scholar]
- Jacko, C.C.; Dellava, J.; Ensle, K.; Hoffman, D.J. Use of the plate-waste method to measure food intake in children. J. Ext. 2007, 45. [Google Scholar]
- Liem, D.G.; Miremadi, F.; Keast, R.S. Reducing sodium in foods: The effect on flavor. Nutrients 2011, 3, 694–711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boon, C.S.; Taylor, C.L.; Henney, J.E. Strategies to Reduce Sodium Intake in the United States; The National Academies Press: Washington, DC, USA, 2010. [Google Scholar]
- Rivera, M.; Shani, A. Attitudes and orientation toward vegetarian food in the restaurant industry: An operator’s perspective. Int. J. Contemp. Hosp. Manag. 2013, 25, 1049–1065. [Google Scholar] [CrossRef] [Green Version]
- Šmugović, S.; Kalenjuk-Pivarski, B.; Grubor, B.; Knežević, N. Vegetarian Diet: Perceptions and Attitudes of Hospitality Management. Zb. Rad. Departmana Za Geogr. Turiz. Hotel. 2021, 70–77. Available online: https://scindeks-clanci.ceon.rs/data/pdf/1452-0133/2021/1452-01332150070Q.pdf (accessed on 21 October 2021). [CrossRef]
- Gonçalves, C.; Monteiro, S.; Padrão, P.; Rocha, A.; Abreu, S.; Pinho, O.; Moreira, P. Salt reduction in vegetable soup does not affect saltiness intensity and liking in the elderly and children. Food Nutr. Res. 2014, 58, 24825. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malherbe, M.; Walsh, C.M.; van der Merwe, C.A. Consumer acceptability and salt perception of food with a reduced sodium content. J. Consum. Sci. 2003, 31. [Google Scholar] [CrossRef]
- De Moura, P.N.; Honaiser, A.; Bolognini, M.C.M. Avaliação do índice de Resto-ingesta e sobras em Unidade de Alimentação e Nutrição (UAN) do Colégio Agrícola de Guarapuava/PR. Salus 2009, 3, 71–77. [Google Scholar]
- Nonino-Borges, C.B.; Rabito, E.I.; Silva, K.D.; Ferraz, C.A.; Chiarello, P.G.; Santos, J.S.D.; Marchini, J.S. Desperdício de alimentos intra-hospitalar. Rev. Nutr. 2006, 19, 349–356. [Google Scholar] [CrossRef] [Green Version]
- Aires, C.; Saraiva, C.; Fontes, M.C.; Moreira, D.; Moura-Alves, M.; Gonçalves, C. Food Waste and Qualitative Evaluation of Menus in Public University Canteens—Challenges and Opportunities. Foods 2021, 10, 2325. [Google Scholar] [CrossRef] [PubMed]
- Tapsell, L.C.; Hemphill, I.; Cobiac, L.; Patch, C.S.; Sullivan, D.R.; Fenech, M.; Roodenrys, S.; Keogh, J.B.; Clifton, P.M.; Williams, P.G.; et al. Health benefits of herbs and spices: The past, the present, the future. Med. J. Aust. 2006, 185, S1–S24. [Google Scholar] [CrossRef] [Green Version]
- Barbosa, M.I.; Fernandes, A.; Gonçalves, C.; Pena, M.J.; Padrão, P.; Pinho, O.; Moreira, P. Sodium and potassium content of meals served in university canteens. Port. J. Public Health 2017, 35, 172–178. [Google Scholar] [CrossRef]
- Martins, B.M. Quantificação de Sódio e Potássio em Sopas de Ementas Escolares do 1°, 2° e 3° Ciclos; Universidade do Porto: Porto, Portugal, 2012. [Google Scholar]
- Mattes, R.D. The taste for salt in humans. Am. J. Clin. Nutr. 1997, 65, 692S–697S. [Google Scholar] [CrossRef] [Green Version]
- Wanjek, C. Food at Work: Workplace Solutions for Malnutrition, Obesity and Chronic Diseases; International Labour Organization: Geneva, Switzerland, 2005. [Google Scholar]
- Geaney, F.; Harrington, J.; Fitzgerald, A.P.; Perry, I.J. The impact of a workplace catering initiative on dietary intakes of salt and other nutrients: A pilot study. Public Health Nutr. 2011, 14, 1345–1349. [Google Scholar] [CrossRef] [Green Version]



| Baseline Week 1–3 | Week 7–8 | Week 9–10 | Week 11 | Δ% Baseline vs. Week 11 | p-Value | |||
|---|---|---|---|---|---|---|---|---|
| Control Canteen | ||||||||
| Samples (n) | 5 | 3 | 3 | 3 | ||||
| Added Salt Mean ± SD | Soup | g/100 g | 0.4 ± 0.1 | 0.4 ± 0.1 | 0.4 ± 0.0 | 0.7 ± 0.2 | 66.8 | 0.050 a |
| g/portion | 1.0 ± 0.4 | 1.0 ± 0.3 | 1.3 ± 0.2 | 2.3 ± 0.4 | 135.0 | 0.025 a | ||
| Vegetarian | g/100 g | 0.7 ± 0.2 | 0.3 ± 0.2 | 0.7 ± 0.2 | 0.7 ± 0.2 | −9.9 | 0.633 b | |
| g/portion | 2.4 ± 0.7 | 1.5 ± 0.9 | 3.0 ± 0.7 | 3.1 ± 1.0 | 32.0 | 0.683 b | ||
| Meat | g/100 g | 0.7 ± 0.2 | 0.5 ± 0.2 | 0.8 ± 0.4 | 0.6 ± 0.2 | −1.9 | 1.000 a | |
| g/portion | 2.3 ± 0.8 | 2.1 ± 1.0 | 3.0 ± 1.1 | 2.6 ± 1.3 | 12.7 | 0.880 a | ||
| Fish | g/100 g | 0.5 ± 0.3 | 0.5 ± 0.3 | 0.4 ± 0.2 | 0.7 ± 0.4 | 59.4 | 0.315 b | |
| g/portion | 1.3 ± 0.7 | 1.8 ± 1.1 | 1.7 ± 0.6 | 2.9 ± 1.7 | 117.9 | 0.297 a | ||
| Food waste Mean ± SD | Consumers (n) | 71 | 84 | 66 | 28 | |||
| Soup | % | 7.3 ± 5.0 | 5.8 ± 8.2 | 11.7 ± 1.1 | 8.1 | 30.2 * | 0.585 *,a | |
| Main dish | 7.5 ± 5.9 | 10.5 ± 2.5 | 12.0 ± 1.1 | 12.5 | 69.1 * | 0.245 *,a | ||
| Total | 7.5 ± 4.5 | 8.6 ± 4.8 | 11.9 ± 0.1 | 10.5 | 49.0 * | 0.245 *,a | ||
| Consumers satisfaction (score 1–5) Mean ± SD | Global | |||||||
| answers (n) | 36 | 32 | 40 | 7 | −1.0 | 0.892 b | ||
| evaluation | 4.5 ± 0.8 | 4.1 ± 0.8 | 4.2 ± 0.9 | 4.4 ± 0.5 | ||||
| Soup—global | ||||||||
| answers (n) | 31 | 30 | 39 | 7 | −6.6 | 0.452 b | ||
| evaluation | 4.1 ± 0.8 | 3.9 ± 0.9 | 3.7 ± 1.2 | 3.9 ± 1.1 | ||||
| Soup—flavor | ||||||||
| answers (n) | 31 | 28 | 37 | 7 | −13.6 | 0.148 b | ||
| evaluation | 4.1 ± 0.9 | 3.8 ± 1.1 | 3.6 ± 1.3 | 3.6 ± 1.0 | ||||
| Soup—salt | ||||||||
| answers (n) | 31 | 28 | 37 | 7 | −7.5 | 0.394 b | ||
| evaluation | 4.3 ± 0.9 | 3.6 ± 1.2 | 3.9 ± 1.3 | 4.0 ± 0.8 | ||||
| Main dish—global | ||||||||
| answers (n) | 31 | 31 | 38 | 7 | −9.8 | 0.271 b | ||
| evaluation | 4.3 ± 0.9 | 3.7 ± 1.0 | 4.0 ± 0.8 | 3.9 ± 1.1 | ||||
| Main dish—flavor | ||||||||
| answers (n) | 31 | 29 | 36 | 7 | −10.4 | 0.230 b | ||
| evaluation | 4.3 ± 0.9 | 3.7 ± 1.1 | 4.0 ± 0.8 | 3.9 ± 0.9 | ||||
| Main dish—salt | ||||||||
| answers (n) | 31 | 29 | 36 | 7 | −13.0 | 0.336 b | ||
| evaluation | 4.5 ± 0.8 | 3.6 ± 1.1 | 4.0 ± 1.0 | 3.9 ± 1.5 | ||||
| Intervention Canteen | ||||||||
| Samples (n) | 5 | 3 | 3 | 3 | ||||
| Added Salt Mean ± SD | Soup | g/100 g | 0.7 ± 0.2 | 0.5 ± 0.1 | 0.5 ± 0.2 | 0.5 ± 0.1 | −34.3 | 0.131 a |
| g/portion | 2.4 ± 0.7 | 1.2 ± 0.4 | 1.3 ± 0.6 | 1.2 ± 0.3 | −48.6 | 0.053 a | ||
| Vegetarian | g/100 g | 0.7 ± 0.3 | 0.6 ± 0.1 | 0.7 ± 0.2 | 0.7 ± 0.2 | 6.1 | 0.855 b | |
| g/portion | 2.8 ± 1.4 | 2.3 ± 0.4 | 3.0 ± 1.0 | 2.9 ± 0.6 | 1.2 | 0.906 b | ||
| Meat | g/100 g | 1.0 ± 0.7 | 0.7 ± 0.2 | 0.7 ± 0.2 | 0.5 ± 0.2 | −48.0 | 0.230 a | |
| g/portion | 3.8 ± 2.4 | 2.8 ± 1.2 | 2.0 ± 0.5 | 1.8 ± 0.4 | −51.8 | 0.230 a | ||
| Fish | g/100 g | 0.8 ± 0.4 | 0.9 ± 0.5 | 0.8 ± 0.1 | 0.5 ± 0.3 | −41.1 | 0.284 b | |
| g/portion | 3.4 ± 2.2 | 3.0 ± 1.6 | 2.5 ± 0.8 | 1.3 ± 0.8 | −60.9 | 0.297 a | ||
| Food waste Mean ± SD | Consumers (n) | 36 | 438 | 312 | 123 | |||
| Soup | % | 1.4 ± 2.5 | 3.9 ± 2.2 | 0.4 ± 0.4 | 3.9 | 167.6 * | 0.252 *,a | |
| Main dish | 3.0 ± 2.1 | 2.1 ± 0.2 | 1.8 ± 1.7 | 3.9 | 17.5 * | 0.699 *,a | ||
| Total | 2.2 ± 1.8 | 2.8 ± 0.8 | 2.7 ± 0.9 | 3.9 | 62.4 * | 0.699 *,a | ||
| Consumers satisfaction (score 1–5) Mean ± SD | Global | |||||||
| answers (n) | 28 | 96 | 141 | 46 | 2.9 | 0.607 b | ||
| evaluation | 4.0 ± 0.9 | 3.7 ± 0.9 | 3.8 ± 0.9 | 4.2 ± 1.0 | ||||
| Soup—global | ||||||||
| answers (n) | 28 | 94 | 132 | 44 | 3.0 | 0.660 b | ||
| evaluation | 3.9 ± 1.1 | 3.2 ± 1.1 | 3.4 ± 1.1 | 4.0 ± 1.1 | ||||
| Soup—flavor | ||||||||
| answers (n) | 27 | 88 | 123 | 44 | 6.8 | 0.354 b | ||
| evaluation | 3.7 ± 1.2 | 3.0 ± 1.0 | 3.4 ± 1.0 | 4.0 ± 1.0 | ||||
| Soup—salt | ||||||||
| answers (n) | 27 | 88 | 124 | 44 | 12.2 | 0.098 b | ||
| evaluation | 3.6 ± 1.1 | 3.0 ± 1.3 | 3.5 ± 1.1 | 4.1 ± 1.1 | ||||
| Main dish—global | ||||||||
| answers (n) | 27 | 95 | 140 | 46 | −3.3 | 0.611 b | ||
| evaluation | 3.8 ± 0.9 | 3.3 ± 0.9 | 3.5 ± 1.0 | 3.7 ± 1.1 | ||||
| Main dish—flavor | ||||||||
| answers (n) | 26 | 90 | 136 | 45 | 15.7 | 0.044 b | ||
| evaluation | 3.4 ± 1.2 | 3.3 ± 1.0 | 3.5 ± 1.1 | 4.0 ± 1.0 | ||||
| Main dish—salt | ||||||||
| answers (n) | 26 | 90 | 136 | 45 | 7.4 | 0.299 b | ||
| evaluation | 3.6 ± 1.1 | 3.4 ± 1.0 | 3.6 ± 1.1 | 3.9 ± 1.0 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Faria, A.P.; Padrão, P.; Pinho, O.; Silva-Santos, T.; Oliveira, L.; Esteves, S.; Pereira, J.P.; Graça, P.; Moreira, P.; Gonçalves, C. Pilot Study to Reduce Added Salt on a University Canteen through the Use of an Innovative Dosage Equipment. Foods 2022, 11, 149. https://0-doi-org.brum.beds.ac.uk/10.3390/foods11020149
Faria AP, Padrão P, Pinho O, Silva-Santos T, Oliveira L, Esteves S, Pereira JP, Graça P, Moreira P, Gonçalves C. Pilot Study to Reduce Added Salt on a University Canteen through the Use of an Innovative Dosage Equipment. Foods. 2022; 11(2):149. https://0-doi-org.brum.beds.ac.uk/10.3390/foods11020149
Chicago/Turabian StyleFaria, Ana Patrícia, Patrícia Padrão, Olívia Pinho, Tânia Silva-Santos, Luís Oliveira, Sílvia Esteves, João Paulo Pereira, Pedro Graça, Pedro Moreira, and Carla Gonçalves. 2022. "Pilot Study to Reduce Added Salt on a University Canteen through the Use of an Innovative Dosage Equipment" Foods 11, no. 2: 149. https://0-doi-org.brum.beds.ac.uk/10.3390/foods11020149