Auricular Acupuncture for Preoperative Anxiety—Protocol of Systematic Review and Meta-Analysis of Randomized Controlled Trials

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria for Including Studies in the Review
2.1.1. Types of Studies
2.1.2. Types of Participants
2.1.3. Types of Interventions/Comparators
2.1.4. Types of Outcome Measures
2.1.5. Safety of Intervention
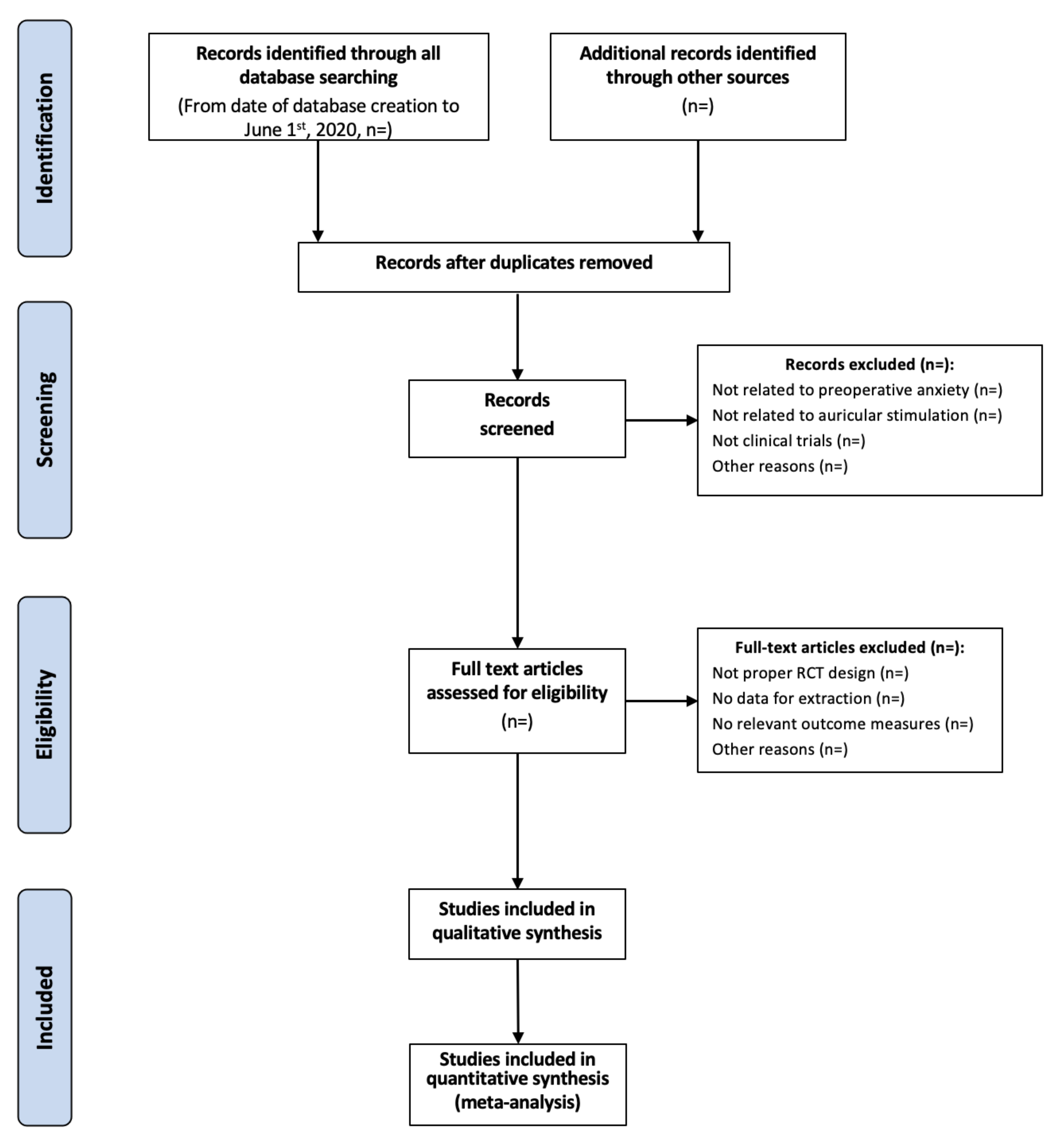
2.2. Search Methods for Identification of Studies
2.3. Data Extraction and Management
2.3.1. Study Identification
2.3.2. Data Extraction
2.3.3. Assessment of Risk of Bias in Included Studies
2.3.4. Measures of Treatment Effects
2.3.5. Dealing with Missing Data
2.3.6. Assessment of Heterogeneity
2.3.7. Assessment of Reporting Biases
2.4. Data Synthesis
2.4.1. Subgroup Analysis and Investigation of Heterogeneity
2.4.2. Sensitivity Analysis
2.4.3. Quality of Outcome Evidence
3. Discussion
Investigation Status
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Walker, E.M.K.; Bell, M.; Cook, T.M.; Grocott, M.P.W.; Moonesinghe, S.R. Patient reported outcome of adult perioperative anaesthesia in the United Kingdom: A crosssectional observational study. Br. J. Anaesth. 2016, 117, 758–766. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Breemhaar, B.; van den Borne, H.W.; Mullen, P.D. Inadequacies of surgical patient education. Patient Educ. Couns. 1996, 28, 31–36. [Google Scholar] [CrossRef]
- Eberhart, L.; Aust, H.; Schuster, M.; Sturm, T.; Gehling, M.; Euteneuer, F.; Rüsch, D. Preoperative anxiety in adults—A cross-sectional study on specific fears and risk factors. BMC Psychiatry 2020, 20, 140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maranets, I.; Kain, Z.N. Preoperative anxiety and intraoperative anesthetic requirements. Anesth. Analg. 1999, 89, 1346–1351. [Google Scholar]
- Kain, Z.N.; Sevarino, F.; Alexander, G.M.; Pincus, S.; Mayes, L.C. Preoperative anxiety and postoperative pain in women undergoing hysterectomy. A repeated-measures design. J. Psychosom. Res. 2000, 49, 417–422. [Google Scholar] [CrossRef]
- Scott, A. Managing anxiety in ICU patients: The role of preoperative information provision. Nurs. Crit. Care 2004, 9, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Theunissen, M.; Peters, M.L.; Bruce, J.; Gramke, H.F.; Marcus, M.A. Preoperative anxiety and catastrophizing: A systematic review and meta-analysis of the association with chronic postsurgical pain. Clin. J. Pain 2012, 28, 819–841. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.; Altun, D.; Oguz, B.H.; Ilhan, M.; Demircan, F.; Koltka, K. The effect of preoperative anxiety on postoperative analgesia and anesthesia recovery in patients undergoing laparascopic cholecystectomy. J. Anesth. 2014, 28, 222–227. [Google Scholar] [CrossRef]
- Maurice-Szamburski, A.; Auquier, P.; Viarre-Oreal, V.; Cuvillon, P.; Carles, M.; Ripart, J.; Honore, S.; Triglia, T.; Loundou, A.; Leone, M.; et al. Effect of sedative premedication on patient experience after general anesthesia: A randomized clinical trial. JAMA 2015, 313, 916–925. [Google Scholar] [CrossRef] [Green Version]
- Powell, R.; Scott, N.W.; Manyande, A.; Bruce, J.; Vögele, C.; Byrne-Davis, L.M.; Unsworth, M.; Osmer, C.; Johnston, M. Psychological preparation and postoperative outcomes for adults undergoing surgery under general anaesthesia. Cochrane Database Syst. Rev. 2016, 5, CD008646. [Google Scholar] [CrossRef]
- Kim, J.; Chiesa, N.; Raazi, M.; Wright, K.D. A systematic review of technology-based preoperative preparation interventions for child and parent anxiety. Can. J. Anaesth. 2019, 66, 966–986. [Google Scholar] [CrossRef]
- Pilkington, K.; Kirkwood, G.; Rampes, H.; Cummings, M.; Richardson, J. Acupuncture for anxiety and anxiety disorders—A systematic literature review. Acupunct. Med. 2007, 25, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.M.; Maranets, I.; Weinberg, M.E.; Caldwell-Andrews, A.A.; Kain, Z.N. Parental auricular acupuncture as an adjunct for parental presence during induction of anesthesia. Anesthesiology 2004, 100, 1399–1404. [Google Scholar] [CrossRef] [PubMed]
- Michalek-Sauberer, A.; Gusenleitner, E.; Gleiss, A.; Tepper, G.; Deusch, E. Auricular acupuncture effectively reduces state anxiety before dental treatment—A randomised controlled trial. Clin. Oral Investig. 2012, 16, 1517–1522. [Google Scholar] [CrossRef] [PubMed]
- Luo, L.; Dai, Q.; Mo, Y.; Yan, Y.; Qian, M.; Zhuang, X.; Huang, L.; Wang, J. The effect of auricular acupressure on preoperative anxiety in patients undergoing gynecological surgery. Int. J. Clin. Exp. Med. 2016, 9, 4065–4070. [Google Scholar]
- Lewis, G.B.H.; Litt, M. An alternative approach to premedication: Comparing diazepam with auriculotherapy and a relaxation method. Am. J. Acupunct. 1987, 15, 205–211. [Google Scholar]
- Karst, M.; Winterhalter, M.; Münte, S.; Francki, B.; Hondronikos, A.; Eckardt, A.; Hoy, L.; Buhck, H.; Bernateck, M.; Fink, M. Auricular acupuncture for dental anxiety: A randomized controlled trial. Anesth. Analg. 2007, 104, 295–300. [Google Scholar] [CrossRef]
- Peuker, E.T.; Filler, T.J. The nerve supply of the human auricle. Clin. Anat. 2002, 15, 35–37. [Google Scholar] [CrossRef]
- Frangos, E.; Ellrich, J.; Komisaruk, B.R. Non-invasive Access to the Vagus Nerve Central Projections via Electrical Stimulation of the External Ear: fMRI Evidence in Humans. Brain Stimul. 2015, 8, 624–636. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Barrett, D.W.; He, Y.; Gonzalez-Lima, F. Anxiolytic-like behavioural effects of head electroacupuncture in rats susceptible to stress. Acupunct. Med. 2016, 34, 235–240. [Google Scholar] [CrossRef]
- Qu, F.; Zhang, D.; Chen, L.T.; Wang, F.F.; Pan, J.X.; Zhu, Y.M.; Ma, C.M.; Huang, Y.T.; Ye, X.Q.; Sun, S.J.; et al. Auricular acupressure reduces anxiety levels and improves outcomes of in vitro fertilization: A prospective, randomized and controlled study. Sci. Rep. 2014, 4, 5028. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walker, K.J.; Smith, A.F. Premedication for anxiety in adult day surgery. Cochrane Database Syst. Rev. 2009, 4, CD002192. [Google Scholar] [CrossRef] [PubMed]
- Zemła, A.J.; Nowicka-Sauer, K.; Jarmoszewicz, K.; Wera, K.; Batkiewicz, S.; Pietrzykowska, M. Measures of preoperative anxiety. Anaesthesiol. Intensive Ther. 2019, 51, 64–69. [Google Scholar] [CrossRef]
- Wilson, C.J.; Mitchelson, A.J.; Tzeng, T.H.; El-Othmani, M.M.; Saleh, J.; Vasdev, S.; LaMontagne, H.J.; Saleh, K.J. Caring for the surgically anxious patient: A review of the interventions and a guide to optimizing surgical outcomes. Am. J. Surg. 2016, 212, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Usichenko, T.; Hacker, H.; Lotze, M. Transcutaneous auricular vagal nerve stimulation (taVNS) might be a mechanism behind the analgesic effects of auricular acupuncture. Brain Stimul. 2017, 10, 1042–1044. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.S.; Jun, H.; Chae, Y.; Park, H.J.; Kim, B.H.; Chang, I.M.; Kang, S.K.; Lee, H.J. The practice of Korean medicine: An overview of clinical trials in acupuncture. Evid. Based Complement Alternat. Med. 2005, 2, 325–352. [Google Scholar] [CrossRef] [Green Version]
- Carreno, F.R.; Frazer, A. The Allure of Transcutaneous Vagus Nerve Stimulation as a Novel Therapeutic Modality. Biol. Psychiatry 2016, 79, 260–261. [Google Scholar] [CrossRef]


{kind=link}
| N | Search Item [Title/Abstract] |
|---|---|
| 1 | Randomized controlled trial |
| 2 | Controlled clinical trial |
| 3 | Randomized |
| 4 | Randomly |
| 5 | Trial |
| 6 | OR #1-6 |
| 7 | Anxiety |
| 8 | Fear |
| 9 | Preoperative |
| 11 | Surgical |
| 12 | Intervention |
| 14 | Anesthesia |
| 15 | OR #7-14 |
| 16 | Auricular acupuncture |
| 17 | Auricular |
| 18 | Ear |
| 19 | Acupressure |
| 20 | Electro-acupuncture |
| 21 | OR #16-20 |
| N | Categories | Items Extracted |
|---|---|---|
| 1 | General information | Author, year of publication, title, journal (title, volume, pages), country, language of publication |
| 2 | Research method | Random allocation, allocation concealment, blinding, baseline level |
| 3 | Participants | Total sample size, number in experimental group, number in control group, gender, age, ethnicity, type of surgery, setting |
| 4 | Intervention | Type of intervention (auricular acupuncture, auricular acupressure, auricular electro-acupuncture, etc.), selection of auricular sites/auricular acupuncture points, selected for stimulation, type of device/needles, used for auricular stimulation, length of auricular stimulation, type of control condition |
| 5 | Outcome parameter | Levels of preoperative anxiety (taken using questionnaires and psychophysical scales), physiological parameters (heart rate, blood pressure, respiratory rate, sweating reaction, etc.), preoperative requirement of anxiolytic medication, intraoperative requirement of anaesthetic and analgesic medication, the intensity of postoperative pain, postoperative requirement of analgesic medication, patient satisfaction with the treatment of preoperative anxiety, safety and side effects of intervention and type of control condition |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dietzel, J.; Cummings, M.; Hua, K.; Hahnenkamp, K.; Brinkhaus, B.; Usichenko, T.I. Auricular Acupuncture for Preoperative Anxiety—Protocol of Systematic Review and Meta-Analysis of Randomized Controlled Trials. Medicines 2020, 7, 73. https://0-doi-org.brum.beds.ac.uk/10.3390/medicines7120073
Dietzel J, Cummings M, Hua K, Hahnenkamp K, Brinkhaus B, Usichenko TI. Auricular Acupuncture for Preoperative Anxiety—Protocol of Systematic Review and Meta-Analysis of Randomized Controlled Trials. Medicines. 2020; 7(12):73. https://0-doi-org.brum.beds.ac.uk/10.3390/medicines7120073
Chicago/Turabian StyleDietzel, Joanna, Mike Cummings, Kevin Hua, Klaus Hahnenkamp, Benno Brinkhaus, and Taras I. Usichenko. 2020. "Auricular Acupuncture for Preoperative Anxiety—Protocol of Systematic Review and Meta-Analysis of Randomized Controlled Trials" Medicines 7, no. 12: 73. https://0-doi-org.brum.beds.ac.uk/10.3390/medicines7120073