Effective Lenvatinib Treatment Complicated with Secondary Tracheocutaneous Fistula in Patients with Advanced Anaplastic Thyroid Carcinoma


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Presentation
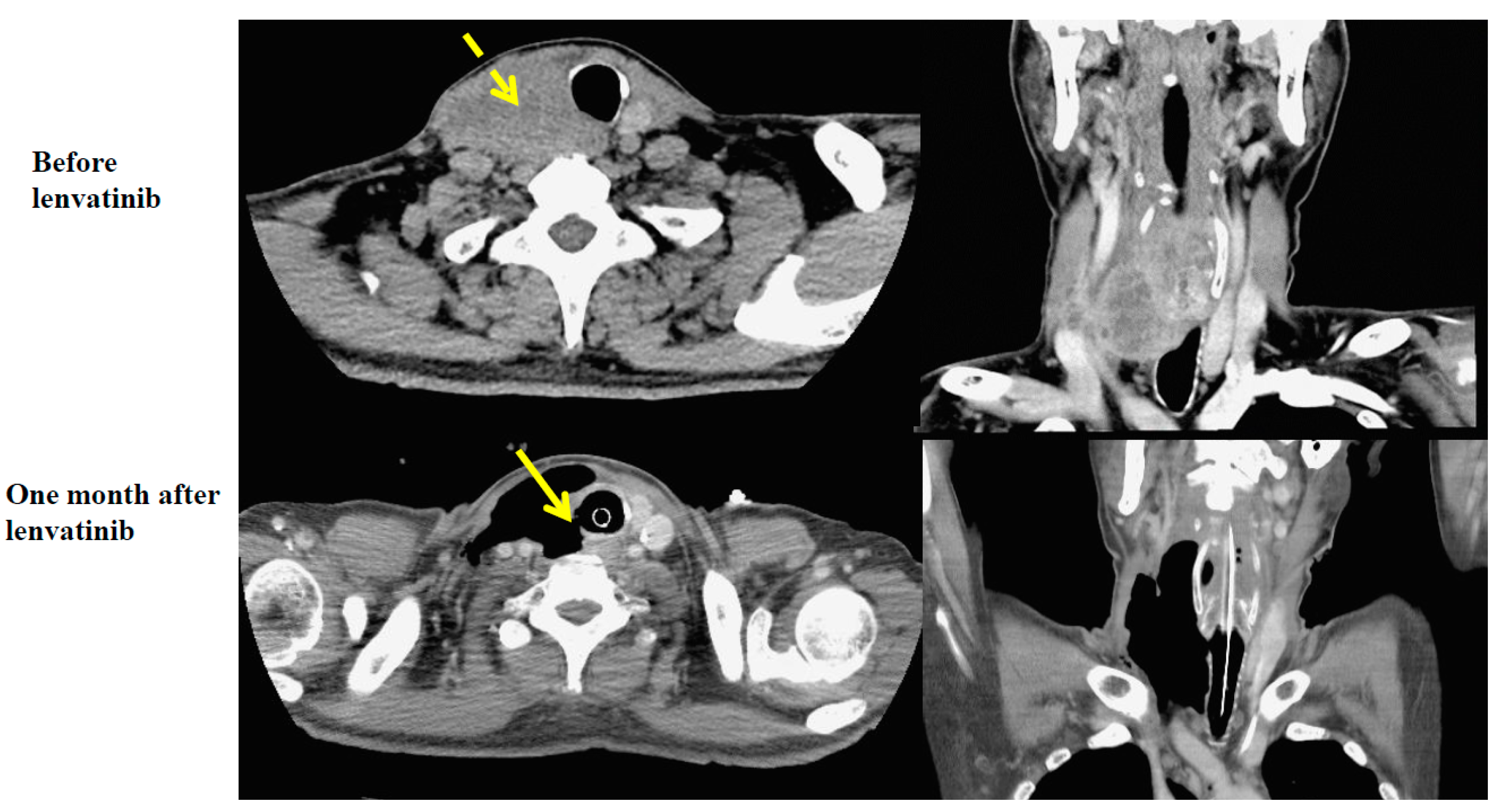
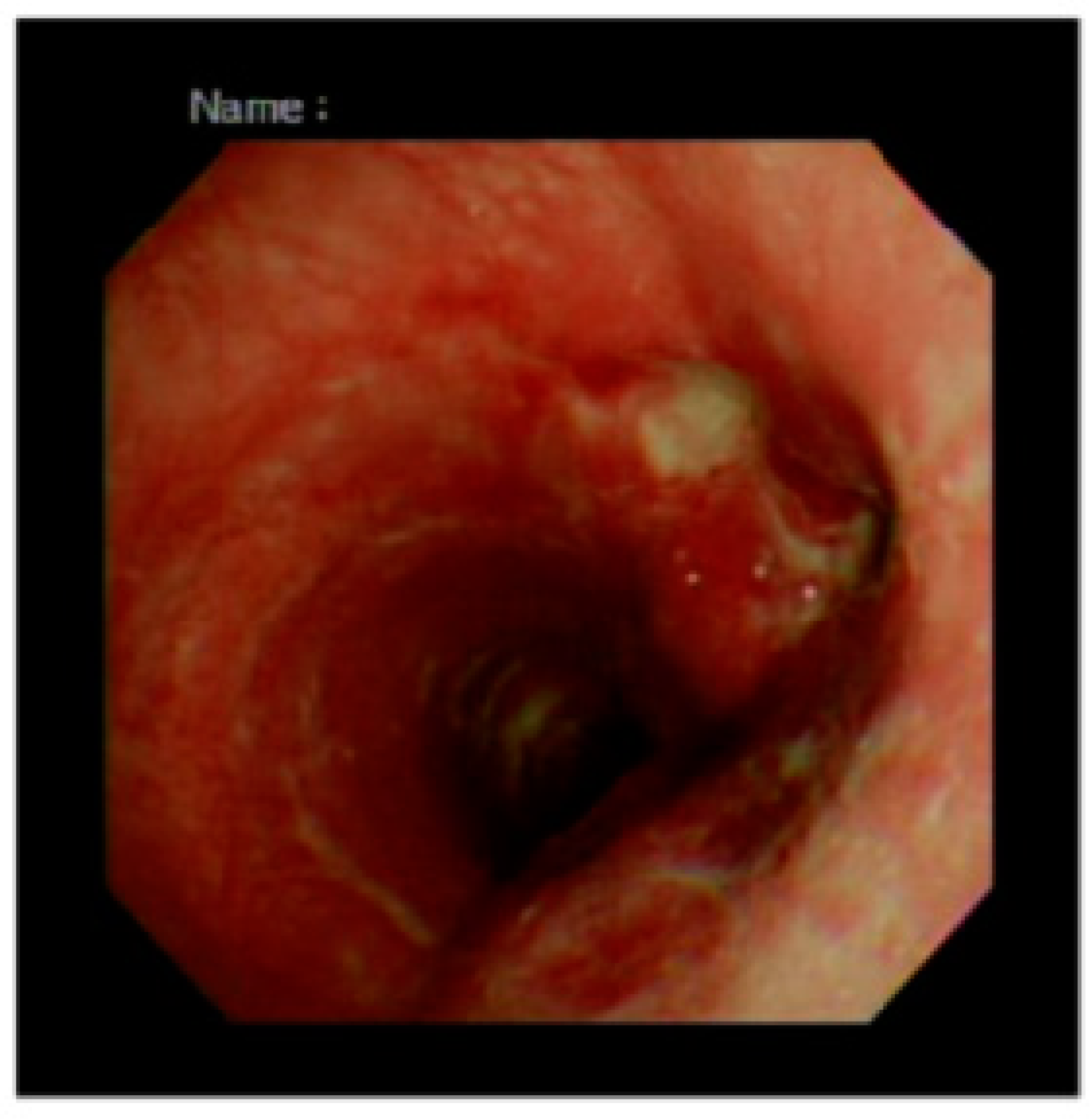
2.1. Case 1
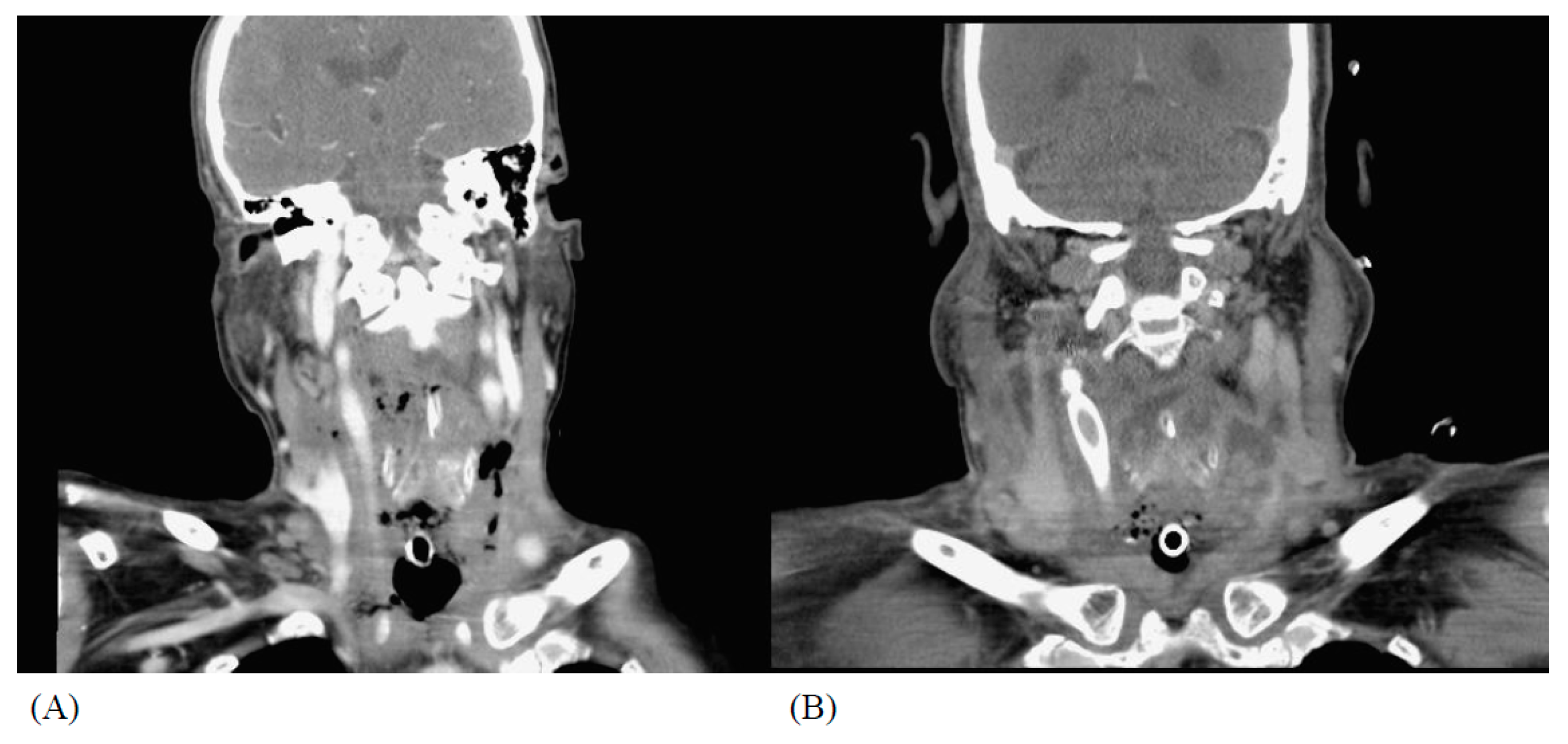
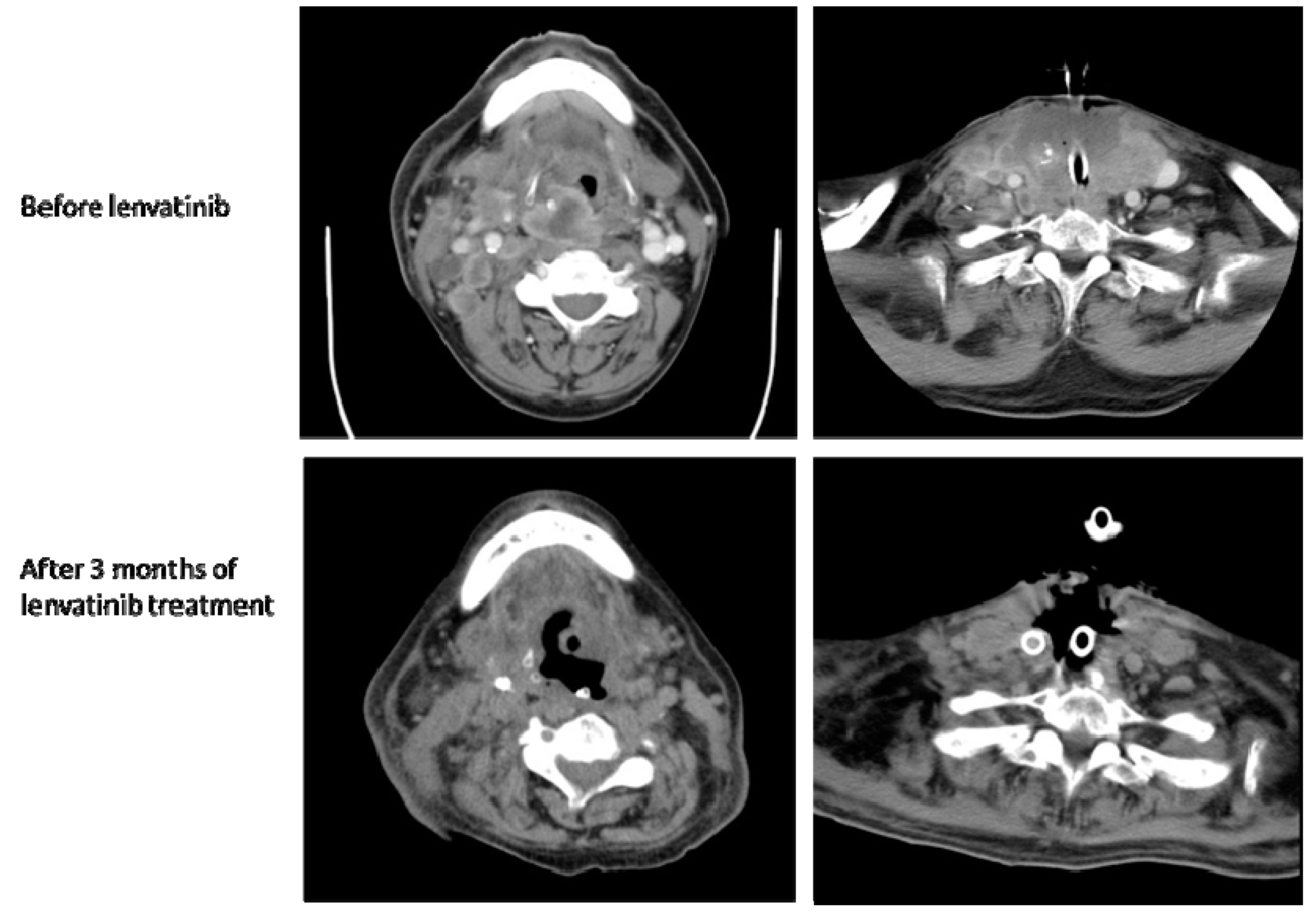
2.2. Case 2
3. Discussion
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Saini, S.; Tulla, K.; Maker, A.V.; Burman, K.D.; Prabhakar, B.S. Therapeutic advances in anaplastic thyroid cancer: A current perspective. Mol. Cancer 2018, 17, 154. [Google Scholar] [CrossRef]
- Sugitani, I.; Miyauchi, A.; Sugino, K.; Okamoto, T.; Yoshida, A.; Suzuki, S. Prognostic factors and treatment outcomes for anaplastic thyroid carcinoma: ATC Research Consortium of Japan cohort study of 677 patients. World J. Surg. 2012, 36, 1247–1254. [Google Scholar] [CrossRef]
- Keutgen, X.M.; Sadowski, S.M.; Kebebew, E. Management of anaplastic thyroid cancer. Gland Surg. 2015, 4, 44–51. [Google Scholar]
- Glaser, S.M.; Mandish, S.F.; Gill, B.S.; Balasubramani, G.K.; Clump, D.A.; Beriwal, S. Anaplastic thyroid cancer: Prognostic factors, patterns of care, and overall survival. Head Neck 2016, 38, E2083–E2090. [Google Scholar] [CrossRef]
- Iwasaki, H.; Yamazaki, H.; Takasaki, H.; Suganuma, N.; Nakayama, H.; Toda, S.; Masudo, K. Lenvatinib as a novel treatment for anaplastic thyroid cancer: A retrospective study. Oncol. Lett. 2018, 16, 7271–7277. [Google Scholar] [CrossRef] [Green Version]
- Tahara, M.; Kiyota, N.; Yamazaki, T.; Chayahara, N.; Nakano, K.; Inagaki, L.; Toda, K.; Enokida, T.; Minami, H.; Imamura, Y.; et al. Lenvatinib for Anaplastic Thyroid Cancer. Front Oncol. 2017, 7, 25. [Google Scholar] [CrossRef]
- Schlumberger, M.; Tahara, M.; Wirth, L.J.; Robinson, B.; Brose, M.S.; Elisei, R.; Habra, M.A.; Newbold, K.; Shah, M.H.; Hoff, A.O.; et al. Lenvatinib versus placebo in radioiodine-refractory thyroid cancer. N. Engl. J. Med. 2015, 372, 621–630. [Google Scholar] [CrossRef]
- Okamoto, K.; Ikemori-Kawada, M.; Jestel, A.; von König, K.; Funahashi, Y.; Matsushima, T.; Tsuruoka, A.; Inoue, A.; Matsui, J. Distinct binding mode of multikinase inhibitor lenvatinib revealed by biochemical characterization. ACS Med. Chem. Lett. 2015, 6, 89–94. [Google Scholar] [CrossRef]
- Shah, D.R.; Dholakia, S.; Shah, R.R. Effect of tyrosine kinase inhibitors on wound healing and tissue repair: Implications for surgery in cancer patients. Drug Saf. 2014, 37, 135–149. [Google Scholar] [CrossRef]





© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, W.-C.; Lai, J.-I.; Chen, J.-Y.; Liu, C.-Y. Effective Lenvatinib Treatment Complicated with Secondary Tracheocutaneous Fistula in Patients with Advanced Anaplastic Thyroid Carcinoma. Reports 2019, 2, 22. https://0-doi-org.brum.beds.ac.uk/10.3390/reports2030022
Wu W-C, Lai J-I, Chen J-Y, Liu C-Y. Effective Lenvatinib Treatment Complicated with Secondary Tracheocutaneous Fistula in Patients with Advanced Anaplastic Thyroid Carcinoma. Reports. 2019; 2(3):22. https://0-doi-org.brum.beds.ac.uk/10.3390/reports2030022
Chicago/Turabian StyleWu, Wen-Chi, Jiun-I Lai, Jui-Yu Chen, and Chun-Yu Liu. 2019. "Effective Lenvatinib Treatment Complicated with Secondary Tracheocutaneous Fistula in Patients with Advanced Anaplastic Thyroid Carcinoma" Reports 2, no. 3: 22. https://0-doi-org.brum.beds.ac.uk/10.3390/reports2030022