
Rapidly Growing Aneurysm with Ulcer-like Projection Complicated with Bacteroides ovatus Bacteremia



1
Department of Critical Care and Emergency Medicine, Shimane Prefectural Central Hospital, Izumo 693-0068, Shimane, Japan
2
Community Care, Unnan City Hospital, Unnan 699-1221, Shimane, Japan
3
Department of Community Medicine Management, Faculty of Medicine, Shimane University, Izumo 693-8501, Shimane, Japan
*
Author to whom correspondence should be addressed.
Reports 2021, 4(3), 28; https://0-doi-org.brum.beds.ac.uk/10.3390/reports4030028
Submission received: 28 July 2021
/
Revised: 16 August 2021
/
Accepted: 31 August 2021
/
Published: 3 September 2021
(This article belongs to the Special Issue Case Reports in Oncology)
{kind=link}
{kind=link}
Abstract
:The incidence of anaerobic bacteremia has been increasing over the past several decades. Further, antibiotic resistance in Bacteroides is a pertinent issue. A 76-year-old man was brought to our hospital with complaints of fever, chills, and abdominal pain. Empiric antibiotics induced minimal relief. The blood culture was positive for multi-drug resistant Bacteroides ovatus. Our patient developed a periaortic abscess in the abdominal aorta and a thoracic aortic aneurysm with ulcer-like projection (ULP), which rapidly increased in size. He was transferred to the tertiary medical institution for surgical drainage. This case suggests that bacteremia can exacerbate aneurysms with ulcerative lesions. Anaerobic bacteremia is a possible differential diagnosis when periaortic abscess formation is present. Early surgical consultation and appropriate antibiotic selection are crucial in anaerobic bacteremia treatment.
1. Introduction
The incidence of anaerobic bacteremia has been increasing over the past several decades [1]. The anaerobes can cause various infections in humans, such as pneumonia, intraabdominal infections, and deep soft tissue infections. As the infection becomes severe or the host immune system is deterred, the anaerobes can invade into the blood stream, causing blood stream infection as a form of bacteremia [1]. The anaerobic bacteremia can cause further complications, such as intraluminal infection of vessels and abscess formation [2]. Infected aortic aneurysm is a rare fulminant infectious disease, of which the most common pathogens are Staphylococcus aureus and Salmonella species [2]. The risk factors for infected aneurysms include IV drug use [3], diabetes mellitus, chronic steroid use, chemotherapy, use of immunosuppressant drugs, chronic kidney disease, malnutrition, rheumatoid arthritis, and lymphoma [4,5]. Chlamydia pneumoniae and Brucella species have previously been reported as less common causative pathogens in infected aneurysms [6,7]. Anaerobes are rare causative pathogens of this disease [2]. Bacteroides ovatus, one of the related strains of the Bacteroides genus, which constitutes 30% of the total colonic bacteria, is known as an anaerobic microbe that causes abscess formation in most anatomical sites [8]. In this case, we experienced the deterioration of aortic aneurysm caused by multi-drug resistant Bacteroides ovatus blood stream infections accompanying periaortic abscess formation. The purpose of this case report was to show the importance of considering antibiotic resistance in Bacteroides and predicting the exacerbation of existing diseases such as aortic aneurysm.
2. Case Presentation
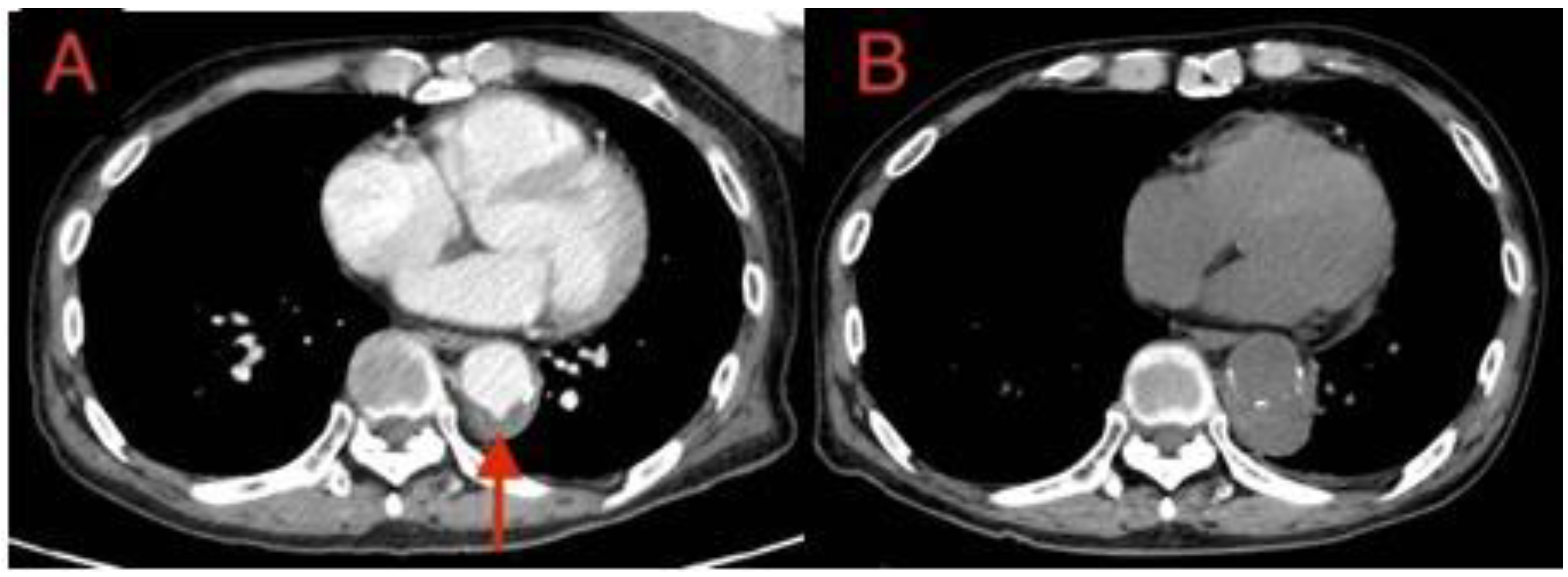
A 76-year-old man was brought to our hospital with complaints of fever, chills, and abdominal pain. He underwent chemotherapy for diffuse large B-cell lymphoma (DLBCL) 2 years before the presentation and failed to be followed up since then. His medical records for DLBCL treatment were not accessible as he was treated at another hospital. Chest CT with contrast on admission day showed an ulcer-like projection (ULP) in a thoracic aortic aneurysm (TAA) (37 mm) (Figure 1A).
In addition, abdominal CT showed a periaortic abscess around the bifurcation of the common iliac arteries (Figure 2).
He was diagnosed with a periaortic abscess in the abdominal aorta. Intravenous vancomycin + ceftriaxone helped him attain minimal relief of abdominal pain and fever. A day after the admission, we consulted the cardiovascular surgeon for the possibility of surgical intervention in this patient. Surgical intervention was not warranted at this stage, and antibiotic treatment was continued.
On day 3, the blood culture turned positive for Gram-negative rods (GNRs). Considering the possibility of failure to cover the extended-spectrum beta-lactamase-producing species, we changed the antibiotic to carbapenem. On day 6, the blood culture was positive for Bacteroides ovatus, which was multidrug-resistant (including carbapenem) and yet showed susceptibility to cefmetazole. Subsequently, the antibiotic treatment was changed to cefmetazole. Fever and abdominal pain persisted despite the appropriate administration of antibiotics for 6 days. A follow-up CT showed rapid eccentric enlargement of the TAA (52 mm) with perivascular fluid collection, strongly suggesting an exacerbating thoracic aortic aneurysm (Figure 1B). This imaging result prompted emergent consultation with the cardiovascular surgeon. The patient was transferred to a tertiary hospital for emergency aneurysm excision and surgical drainage of the abscess. However, he did not consent to the surgical treatment. Therefore, the antibiotic treatment was continued for a longer period. He was discharged from the tertiary hospital for rehabilitation after approximately 2 months of antibiotic treatment. However, his general condition did not improve to allow him to perform activities of daily living. Eventually, the patient succumbed to his condition due to malnutrition and disuse syndrome.
3. Discussion
Our patient developed a periaortic abscess in the abdominal aorta and a TAA, which rapidly increased in size. Despite the less typical clinical presentation, the patient’s TAA had become exacerbated due to bacterial infection. Therefore, it was rational to diagnose this patient with infected aneurysm. ULP as a CT finding may be associated with hematoma within the media and may progress to perforation or aortic dissection [9,10,11]. Our observations from this case suggest that early surgical intervention may be necessary in a patient having a pre-existing aneurysm with ULP complicated with a severe infection such as bacteremia. In the presented case, ULP was found in a CT scan before the deterioration of the aneurysm. Through this case and discussion, we have showed the importance of considering antibiotic resistance in Bacteroides and predicting the exacerbation of existing diseases such as aortic aneurysm.
The patient had an unfavorable outcome, which can be attributed mainly to his refusal of surgery. Although surgical intervention is almost always required in the treatment of infected aneurysms, the urgency of surgical intervention can be determined by estimating the risk of aneurysm rupture, and also considering the patient’s general condition [4]. The principles of surgical treatment for infected aneurysms include obtaining a tissue sample, performing wide debridement of the infected arterial wall, ensuring copious irrigation of the surgical field, and reconstructing the artery [12]. In addition to traditional surgical intervention, endovascular stent graft placement has been recently introduced as another option in the treatment of infected aneurysms. In a recent literature review of endovascular stent graft treatment, the 30-day survival rate was 89.6% and 2-year survival was 82.2% [13]. Although placing a stent in an infected environment is associated with a risk of persistent infection, endovascular aortic stent grafting is a possible alternative method for treating infected aneurysms [4].
In the present case, it is unknown why this patient refused surgery, or how much information had been provided to him, since informed consent was obtained at another hospital. It may have been due to his poor understanding of the disease itself, or perhaps because he had no family or close relatives to discuss his decision. Serban et al. have argued that the process of obtaining informed consent should include the sharing of sufficient information regarding the specific and general risks associated with the procedure, and a discussion of possible therapeutic alternatives [14]. If the process of obtaining informed consent is performed with care, it will likely lead to better treatment compliance in the postoperative period, as well as increased trust and patient satisfaction [14]. The present case illustrates the importance of obtaining informed consent for procedures with great care, especially in elderly patients who are likely to have difficulties understanding their health conditions.
Anaerobes are rare causative pathogens of infected aneurysms [2]. To the best of our knowledge, this is the first case report of an infected aneurysm caused by Bacteroides ovatus, one of the related strains of the Bacteroides genus, which constitutes 30% of the total colonic bacteria, and is known to cause abscess formation in most anatomical sites [8]. We could not determine the route of entry of the pathogen into the bloodstream or the mechanism of formation of a periaortic abscess and the subsequent infected aneurysm. The condition could be explained by the possibility of pre-existing lower gastrointestinal lesions, such as colon cancer, which were undetectable on CT.
The incidence of anaerobic bacteremia has been increasing since 1993 [1]. Further, antibiotic resistance in Bacteroides is a pertinent issue [15]. To improve the outcome of patients with anaerobic bacteremia, the selection of an appropriate antibiotic treatment at an early stage is crucial. Our report suggests that periaortic abscess formation is a sign of anaerobic bacteremia.
4. Conclusions
Bacteremia can exacerbate pre-existing aneurysms with ulcerative lesions. Anaerobic bacteremia is a possible differential diagnosis in cases of periaortic abscess formation.
Author Contributions
Conceptualization: M.K. and R.O.; methodology: M.K. and R.O.; validation: M.K., R.O. and J.S.; formal analysis: M.K. and R.O.; investigation: M.K. and R.O.; resources: M.K. and R.O.; data curation: M.K., R.O. and J.S.; writing—original draft preparation: M.K. and R.O.; writing—review and editing: M.K., R.O., J.S. and C.S.; visualization: M.K.; supervision: R.O. and C.S.; project administration: R.O. and C.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The ethical review and approval were waived for this study, due to the description of a single clinical case.
Informed Consent Statement
Written informed consent has been obtained from the patient to publish this paper.
Data Availability Statement
The data used in this case report is available upon reasonable request from the corresponding author.
Acknowledgments
We would like to thank the patient for agreeing to have this case report published.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Lassmann, B.; Gustafson, D.R.; Wood, C.M.; Rosenblatt, J.E. Reemergence of Anaerobic Bacteremia. Clin. Infect. Dis. 2007, 44, 895–900. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.-L.; Liu, K.-H.; Yang, Y.-J.; Kan, C.-D. Bacteroides fragilis aortic arch pseudoaneurysm: Case report with review. J. Cardiothorac. Surg. 2008, 3, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raman, S.P.; Fishman, E.K. Mycotic aneurysms: A critical diagnosis in the emergency setting. Emerg. Radiol. 2014, 21, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.-W. Infected Aneurysm: Current Management. Ann. Vasc. Dis. 2010, 3, 7–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steverlynck, L.; Van De Walle, S. Mycotic thoracic aortic aneurysm: Review of the diagnostic and therapeutic options. Acta Clin. Belg. 2013, 68, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Loehe, F.; Bittmann, I.; Weilbach, C.; Lauterjung, L.; Schildberg, F.-W.; Heiss, M.M. Chlamydia pneumoniae in Atherosclerotic Lesions of Patients Undergoing Vascular Surgery. Ann. Vasc. Surg. 2002, 16, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Kakkos, S.K.; Papadoulas, S.; Lampropoulos, G.; Marangos, M.; Kalogeropoulou, C.; A Tsolakis, I. Aorto-iliac aneurysm infected by Brucella: Distinctive presentation patterns of a rare entity. Vascular 2013, 21, 307–315. [Google Scholar] [CrossRef] [PubMed]
- Garrett, W.S.; Onderdonk, A.B. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases, 8th ed.; Bennett, J.E., Dolin, R., Blaser, M.J., Eds.; W.B. Saunders: Philadelphia, PA, USA, 2015; Volume 2, pp. 2773–2780. ISBN 9781455748013. [Google Scholar]
- Stanson, A.W.; Kazmier, F.J.; Hollier, L.H.; Edwards, W.D.; Pairolero, P.C.; Sheedy, P.F.; Joyce, J.W.; Johnson, M.C. Penetrating atherosclerotic ulcers of the thoracic aorta: Natural history and clinicopathologic correlations. Ann. Vasc. Surg. 1986, 1, 15–23. [Google Scholar] [CrossRef]
- Tsai, T.T.; Nienaber, C.A.; Eagle, K.A. Acute Aortic Syndromes. Circulation 2005, 112, 3802–3813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ganaha, F.; Miller, D.C.; Sugimoto, K.; Do, Y.S.; Minamiguchi, H.; Saito, H.; Mitchell, R.S.; Dake, M.D. Prognosis of Aortic Intramural Hematoma With and Without Penetrating Atherosclerotic Ulcer. Circulation 2002, 106, 342–348. [Google Scholar] [CrossRef] [PubMed]
- Leon, L.R.; Ihnat, D.M.; Mills, J.L. Native Arterial Infections. In Comprehensive Vascular and Endovascular Surgery; Elsevier BV: Amsterdam, The Netherlands, 2009; pp. 714–726. [Google Scholar] [CrossRef]
- Kan, C.-D.; Lee, H.-L.; Yang, Y.-J. Outcome after endovascular stent graft treatment for mycotic aortic aneurysm: A systematic review. J. Vasc. Surg. 2007, 46, 906–912. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serban, D.; Spataru, R.; Vancea, G.; Balasescu, S.; Socea, B.; Tudor, C.; Dascalu, A. Informed consent in all surgical specialties: From legal obligation to patient satisfaction. Romanian J. Leg. Med. 2020, 28, 317–321. [Google Scholar] [CrossRef]
- Hecht, D.W. Prevalence of Antibiotic Resistance in Anaerobic Bacteria: Worrisome Developments. Clin. Infect. Dis. 2004, 39, 92–97. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
(A) Thoracic aortic aneurysm (TAA) with “ulcer-like projection” (red arrow). (B) Rapid eccentric enlargement of TAA (52 mm) with perivascular fluid collection.
Figure 1.
(A) Thoracic aortic aneurysm (TAA) with “ulcer-like projection” (red arrow). (B) Rapid eccentric enlargement of TAA (52 mm) with perivascular fluid collection.

Figure 2.
Periaortic abscess around the bifurcation of the common iliac arteries.

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Kusunoki, M.; Ohta, R.; Sawa, J.; Sano, C. Rapidly Growing Aneurysm with Ulcer-like Projection Complicated with Bacteroides ovatus Bacteremia. Reports 2021, 4, 28. https://0-doi-org.brum.beds.ac.uk/10.3390/reports4030028
AMA Style
Kusunoki M, Ohta R, Sawa J, Sano C. Rapidly Growing Aneurysm with Ulcer-like Projection Complicated with Bacteroides ovatus Bacteremia. Reports. 2021; 4(3):28. https://0-doi-org.brum.beds.ac.uk/10.3390/reports4030028
Chicago/Turabian StyleKusunoki, Masayoshi, Ryuichi Ohta, Jumpei Sawa, and Chiaki Sano. 2021. "Rapidly Growing Aneurysm with Ulcer-like Projection Complicated with Bacteroides ovatus Bacteremia" Reports 4, no. 3: 28. https://0-doi-org.brum.beds.ac.uk/10.3390/reports4030028