A Gluten Free Diet in the Management of Epilepsy in People with Coeliac Disease or Gluten Sensitivity


1
School of Allied Health & Community, University of Worcester, Worcester WR2 6AJ, UK
2
Centre for Medical Education, Medical School, Cardiff University, Cardiff CF14 4YS, UK
*
Author to whom correspondence should be addressed.
Gastrointest. Disord. 2020, 2(3), 281-299; https://doi.org/10.3390/gidisord2030026
Submission received: 2 August 2020
/
Revised: 1 September 2020
/
Accepted: 3 September 2020
/
Published: 8 September 2020
(This article belongs to the Special Issue Coeliac Disease)
Abstract
:The aim of this review was to assess the effects of a gluten free diet (GFD) in the management of epilepsy in people with coeliac disease (CD) or gluten sensitivity (GS). A systematic approach was used to undertake a literature review. Five electronic databases (PubMed; Scopus; Google Scholar; Cochrane Epilepsy Group specialised register; Cochrane Register of Controlled Trails (CENTRAL) via the Cochrane Register of Online Trials) were searched using predetermined relevant search terms. In total, 668 articles were identified. Duplicates were removed and predefined inclusion and exclusion criteria were applied, and a PRISMA flow chart was produced. Data was extracted using Covidence software. Twelve studies on Epilepsy and CD involving a total of 70 participants were selected for analysis; narrative synthesis was used owing to the small sample sizes in the selected studies. None of the 12 studies meeting inclusion criteria investigated gluten sensitivity and epilepsy. All the included studies support a link between epilepsy and CD. GFD was effective in 44 out of 70 participants across the studies in terms of a reduction of seizures, reduction of antiepileptic drugs (AEDs) or normalisation of EEG pattern. A total of 44 participants showed a reduction in seizures (across eight studies) and complete cessation of seizures was reported in 22 participants. In general, the earlier the GFD is implemented after the onset of seizures, the better the likelihood of the GFD being successful in supporting control of seizures. Mechanisms linking gluten with epilepsy are not fully understood; possible hypotheses include gluten mediated toxicity, immune-induced cortical damage and malabsorption. Evidence suggests the effectiveness of a GFD in supporting the management of epilepsy in patients with CD, although the quality of evidence is low. There appears to be a growing number of neurologists who are prepared to advocate the use of a GFD. A multidisciplinary approaches and further research are recommended. It could be argued that when balancing potential treatments such as AEDs or surgery, a GFD has a low likelihood of harm.
1. Introduction
1.1. Epilepsy
Epilepsy is a neurological disorder that affects around 70 million people worldwide [1]. It can have a significant effect on the quality of life of those affected and their families [2]. Seizures are usually sudden, acute and unpredictable. People with epilepsy and their cohabiting relatives report higher levels of anxiety, depression and social anxiety disorders compared with the general population [3]. Epilepsy is not one disorder, but a term used to describe several conditions that share seizures as a common element [4]. There are over 40 different types of seizure [5] and the seizure type and appearance vary depending on which area of the brain is affected. Some people may lose consciousness, collapse and jerk or twitch (tonic-clonic seizure). Other seizures result in a brief loss of consciousness with stiffness, or a complete loss of muscle tone (tonic, atonic, or drop attacks). Absence seizures can cause a person to appear blank and unresponsive for a few seconds. Seizures are classified into two main categories: generalised seizures which affect large areas on both sides of the brain (tonic-clonic, absence or atonic) and focal seizures that affect a specific region of the brain [6].
In some people the cause is known; brain injury accounts for almost 5% of all seizures [7], but they can also be caused by brain tumour, electrolyte imbalance [8], hormone imbalance or genetic factors [4]. However, in 60% of cases the aetiology is unknown [9] and referred to as ‘idiopathic epilepsy’ [4]. Lack of sleep [10], stress and anxiety [11], hyperventilation [12] and high caffeine intake can increase seizure susceptibility (although long term low intake can protect from seizures [13]). Epilepsy is primarily controlled pharmacologically, through prescription AEDs, just over half of those taking medication will become seizure free. A further 20–30% will have a reduction in seizures. However, approximately 20% of people continue to suffer seizures despite taking one or more AEDs and this is termed refractory or intractable epilepsy [6].
1.2. Ketogenic Diet in Management of Epilepsy
The ketogenic diet (KD) might improve outcomes in people with epilepsy [14]. The KD has been used for around 100 years in the treatment of refractory epilepsy [15]. The KD is a high-fat, low carbohydrate, adequate protein diet [16]. Mechanisms by which the KD results in improved seizure control are not fully understood. It is thought that the high-fat, restricted carbohydrate intake, results in the production of ketones due to fat metabolism. The anticonvulsant effect of ketones is thought to be due to an upregulation of gene expression involved in energy metabolism in the brain [17]. In the UK, dietary intervention to support epilepsy management is not considered until AEDs have failed to control seizures. In refractory epilepsy, The National Institute for Health and Care Excellence (NICE) guidelines recommend all children, young people and adults be referred to tertiary services offering non-pharmacological interventions and this should involve a multidisciplinary team and include psychological interventions (relaxation, cognitive behaviour therapy, biofeedback); medical intervention (vagus nerve stimulation) or brain surgery [18]. NICE recommends children and young people (but not adults) whose seizures are not controlled by appropriate AEDs should be referred to a paediatric epilepsy specialist for consideration for the use of the KD [18].
Research into understanding the anti-seizure mechanisms of the KD has led some to postulate that the grain free, and therefore the gluten-free nature of the KD, may be a component in its success.
1.3. Gluten and Coeliac Disease
Gluten is the term used to describe the storage proteins found in wheat, barley and rye [19]. CD is a complex, systemic autoimmune disease triggered by the ingestion of gluten, in genetically susceptible individuals [20]. Worldwide, CD affects approximately 1% of the population [21]. Symptoms associated with CD include diarrhoea, constipation, weight loss and malabsorption [22]. Greater understanding of the pathogenesis of CD in the last few decades has established it can affect any part of the body [23].
CD diagnosis must be confirmed by duodenal biopsy [24]. Carrying HLA-DQ2/HLA-DQ8 genes are a key, but not sufficient, component of genetic susceptibility to developing CD [22]. Treatment is lifelong adherence to a strict GFD and although oats are generally considered safe for most people with CD [25], it appears to cause sensitivity for some people [26] most likely due to contamination with wheat, barley or rye during the production chain [27]. For the majority of individuals with CD after GFD symptoms subside and villi recover [28]. However, despite strict GFD some people with CD experience persistent gastrointestinal (GI) and extraintestinal (EI) symptoms [29].
1.4. Non Coeliac Gluten Sensitivity
Non coeliac gluten sensitivity (NCGS) is a controversial condition [30] and the pathophysiology remains unclear. However, NCGS has been legitimised and three international conferences [31,32] have provided consensus on the definition of NCGS and the criteria for diagnosis [33,34]. NCGS appears more common than CD [34,35] with an estimated prevalence in the general population of 13% [31,36]. Although GI symptoms are similar to CD there is little or no mucosal damage [37] and the serological markers that are effective in diagnosing CD are not detectable in NCGS [37]. As with CD, removing gluten from the diet results in improvement of symptoms and reintroduction leads to relapse [33].
Neurological dysfunction associated with GS was originally thought to be due to malabsorption, but further research has discovered inflammatory cells in histopathological results of individuals with gluten sensitivity and neurological manifestation and the theory of an innate immune mechanism has emerged [31,38]. In contrast, CD involves both innate and adaptive immune responses [21].
1.5. Association between Epilepsy and Coeliac Disease
A meta-analysis on epilepsy and systemic autoimmune disorders suggests that people with epilepsy have a 2.6-fold increased risk for CD [39]. In contrast, a large study of people with CD reported a 1.4-fold increased risk of epilepsy [40,41]. However, this number could be higher given that many people with CD do not have gastrointestinal symptoms [42]. Some studies suggest epilepsy is the most frequent disorder associated with CD [43,44].
Developments in the understanding of the role of gluten and the gut–brain axis [42] has provided a basis for exploring the possibility of supporting epilepsy management through the GFD. GFD has resulted in a reduction in seizures in some cases [45,46], particularly those with temporal lobe epilepsy and hippocampal sclerosis [47]. Other case studies have shown complete remission of intestinal and central nervous system manifestations (including electroencephalogram abnormalities associated with seizures) after a GFD, that reappeared after gluten reintroduction [48]. Hence the aim of this review was to assess the effects of a GFD in the management of epilepsy in people with CD or GS. Strict, lifelong GFD is the cornerstone of treatment for CD.
2. Methods
The research strategy was a stand-alone literature review and a systematic approach was used. A systematic review is widely referred to as the ‘gold standard’ review [49]. Literature review also provides a broad overview on many studies to produce a comprehensive picture of that topic which is not possible in a single study [49] and can also be particularly useful to inform and support policy and practice [50]. An ethical checklist was completed, but as it was a review it did not need full ethical approval.
A search was conducted on the International Prospective Register of Systematic Reviews held by the University of York’s Centre for Reviews and Dissemination: PROSPERO [51]. No existing, current or planned systematic reviews regarding GFD and epilepsy were revealed. An attempt was made to register this review with PROSPERO before the data extraction. Data extraction/analysis in this study was undertaken by a single researcher under supervision, so it did not satisfy the requirements for registering with PROSPERO. This review was however conducted in accordance with the Preferred Reporting Items for Systemic Reviews and Meta-Analyses (PRISMA) [52].
3. Data Collection
Five electronic databases were searched: PubMed, Scopus, Google Scholar, Cochrane Epilepsy Group specialised register and the Cochrane Register of Controlled Trails (CENTRAL) via the Cochrane Register of Online Trials (CRSO). Reference lists from published articles or systematic reviews were hand searched. Covidence software was used for data storage. Boolean operators were used: (Epilepsy/OR Epileptic/OR Epileptiform*/OR Neurological/OR Seizure/OR Seizures/OR Convulsions/OR Absence/OR EEG*) AND (Gluten/OR Gluten-Free/OR Gliadin Antibodies/Gluten-free/OR Transglutaminase/OR TG6*/OR Coeliac/Celiac) NOT Autism. The review was restricted to intervention studies reporting the effects of GFD on epilepsy or the effect of gluten on seizure activity. To ensure transparency and reduce the risk of bias, predefined inclusion (see Table 1) and exclusion criteria were applied.
Exclusion criteria:
- Non-English language papers
- Include participants with other neurological conditions
- Include other known antiepileptic intervention
- Participants with known cause epilepsy
- Non-reporting of compliance to GFD
The following data was collected:
- Participant characteristics: age, sex, number of participants
- Study characteristics: country, study design, controls, outcomes measured
- Seizure type
- Duration of GFD
- Method of measuring adherence to GFD
- Length of follow up
- Outcome results
4. Results
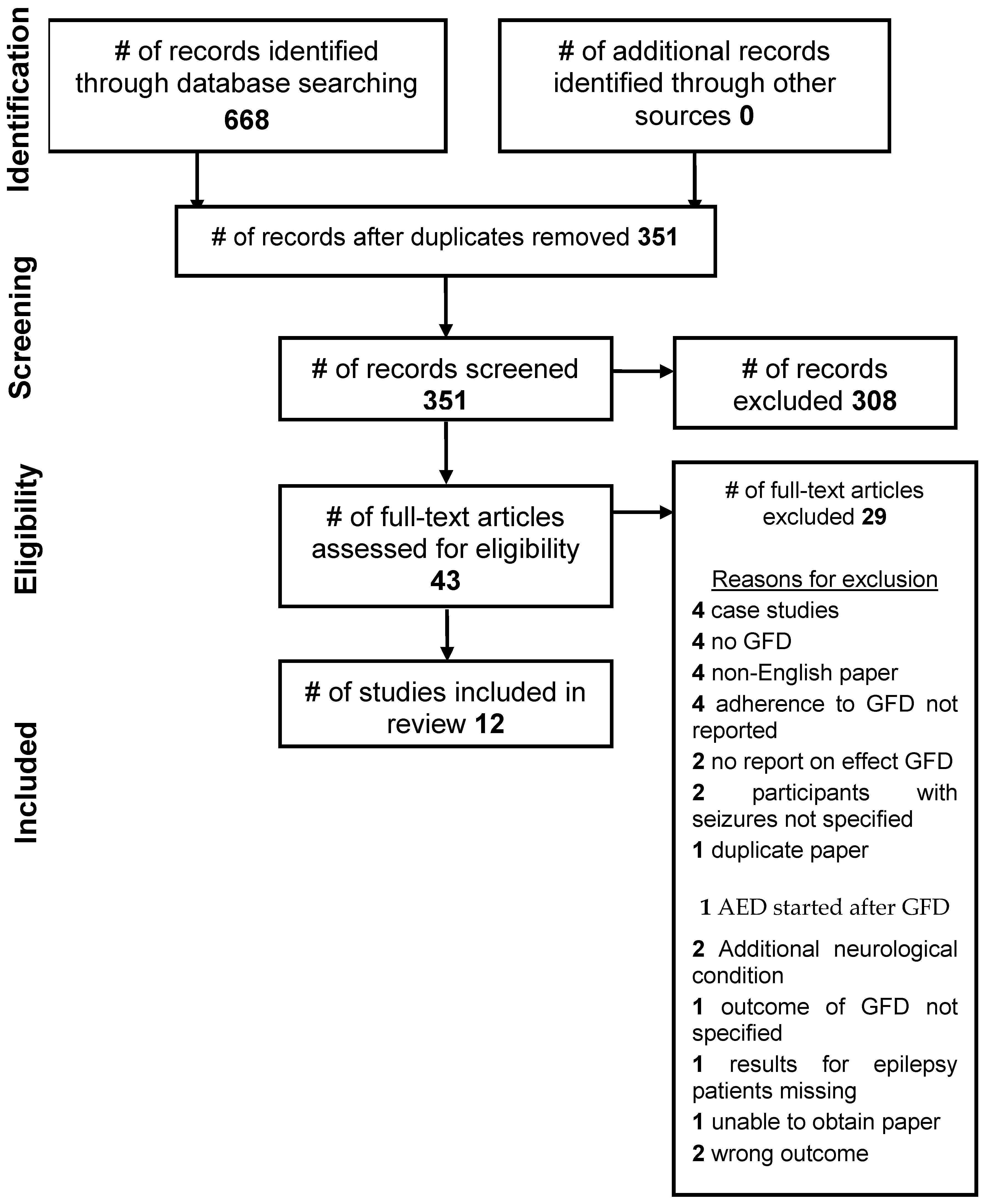
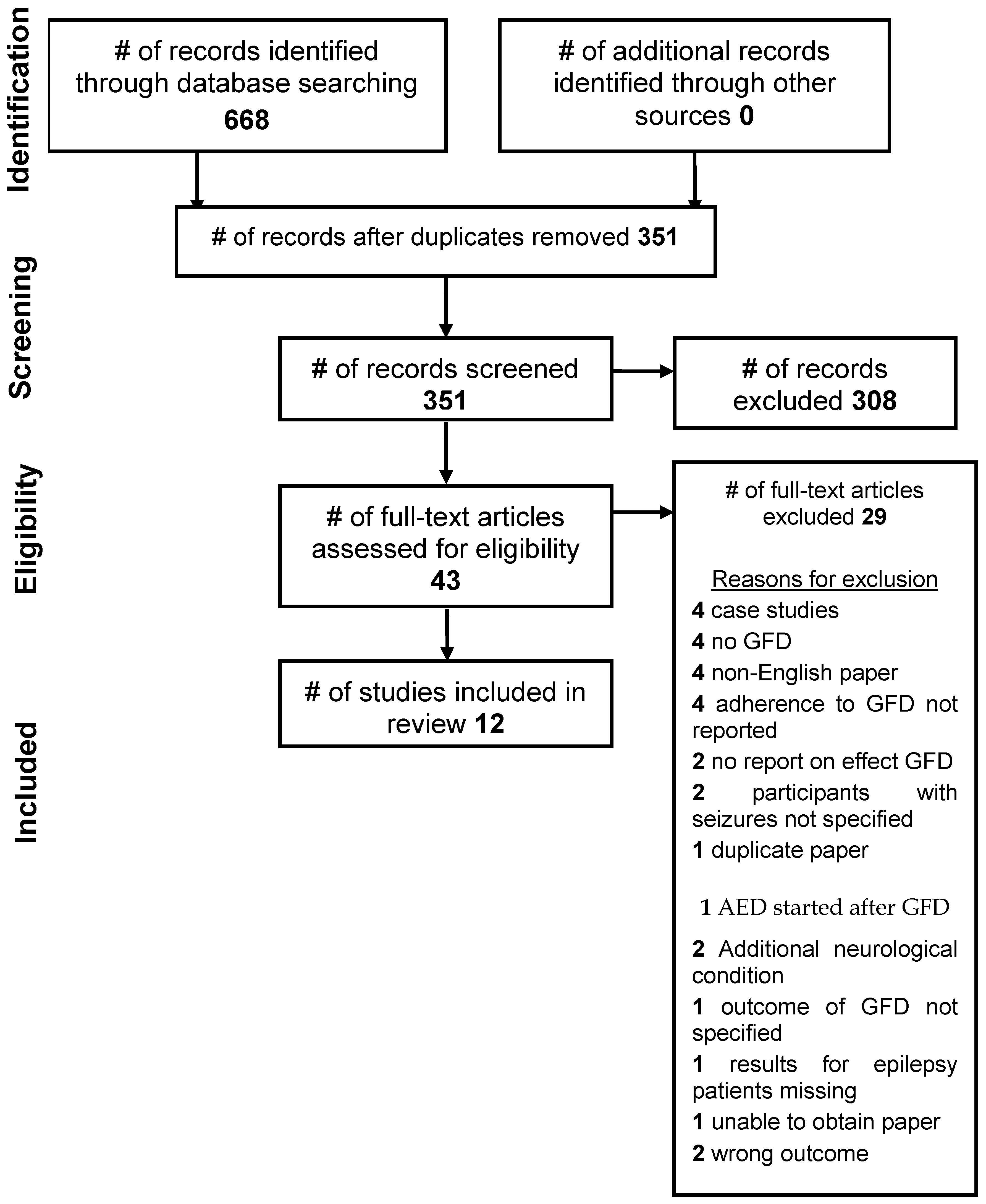
A total of 668 articles were identified (Figure 1) and exported to Covidence. Duplicates were removed; 351 articles remained. Articles were screened (title and abstract), resulting in removal of a further 308. The full-text of 43 articles was read to assess eligibility; inclusion and exclusion criteria were applied. In total, 29 articles were excluded at this stage, with reasons for exclusion detailed in the Supplementary Table S1. A total of 12 articles were reviewed, all investigating CD and epilepsy in which all participants had biopsy proven CD. None of the included studies investigated epilepsy in gluten sensitivity. The selection process was summarised (Figure 1).
Across the 12 studies reviewed, a GFD was effective in 44 out of 70 participants in terms of a reduction of seizures, reduction of AEDs or normalisation of EEG pattern. The earlier the GFD is implemented after the onset, the better the likelihood of the GFD being successful in supporting the control of seizures. Table 2 summarises the results of the included studies. Table 3 details the characteristics of participants in the studies selected for review and also provides further details on serological testing (if it was undertaken). Supplementary Table S2 provides further details of the methodology of the studies included in the review.
The possible mechanisms involved include, reduced inflammation, resulting in improved gut function which facilitates better absorption of AEDs and nutrients, and reduced gluten induced neurotoxicity. Seizures or EEG abnormalities associated with CD include all seizure types. The association between CD and the distinct syndrome ‘CEC’ are well established, but CD can be associated with seizures or EEG abnormalities without calcifications or hippocampal sclerosis. GI symptoms are not always present and often the EI manifestation is the only presenting symptom of CD. There was a low risk of adverse effects of the GFD in these studies.
All the included studies support a link between epilepsy and CD [54,55,56,57,58,59,60,61,62,63,64,65]. Adverse outcomes were reported in two studies although this is not necessarily a result of the GFD [54,56]. Gobbi et al. [54] observed that GFD was more effective in controlling seizures if implemented near the onset of epilepsy, and in childhood.
Gerace et al. [64] using mouse models, demonstrated a correlation between neurotoxicity of proteins associated with gluten: peptide 31–43 and epilepsy. It was shown that the presence of the gliadin peptide 31–43 in the brain, particularly in the hippocampus, where seizures often originate [66], increases the effect of kainate [64]. Kainate suppresses GABA release which is the principal inhibitory neurotransmitter, whilst activating receptors for glutamate; the principal excitatory neurotransmitter in the central nervous system [66]. The researchers hypothesised that transglutaminase activity could mediate the toxic effect of kainate. Hippocampal slices were incubated for 24 h with peptide 31–43 and it was observed that this significantly increased the expression of TG2/TG6 [64]. As a control, the same experiment was performed using maize zein with no effect.
Volta et al. [57] investigated the presence of anti-neuronal antibodies in adult CD patients with EI symptoms (three with epilepsy), after more, or less prompt, start of a GFD. Anti-neuronal antibodies to CNS were detected in 13 (61%) of the patients with EI symptoms, including two out of the three patients with epilepsy [57]. Compared with only one of 20 (5%) of patients without EI manifestations [57]. Furthermore, after GFD, the two out of three patients with epilepsy, who also had CD with GI symptoms, experienced complete cessation of seizures [57]. The third patient with epilepsy, who had CD without GI symptoms, was unaffected by the GFD [57]. The authors report that the anti-neuronal antibodies disappeared in most cases (six out of eight), within a year of starting the GFD [57].
Four studies investigated GFD and EEG patterns [56,61,62,67]. The study by Liccheta et al. [58] recorded EEG pattern before the GFD but unfortunately this was not followed up/reported. Berio et al. [67] documented normalisation in five out of six previously abnormal EEG in patients with good compliance; in contrast with five out of six patients with poor compliance with GFD who showed abnormal EEG pattern. Five of the included studies document AED use [56,58,60,63,65]. However, only two studies documented the effect of GFD on AEDs [63,65].
Arroyo et al. [56] study focused on 24 patients with CEC syndrome, all with calcifications. After GFD, there was no change in calcifications of 10 patients; decreased white-matter density in seven patients, of which three further improved with a marked reduction or disappearance 6–12 months after starting the GFD [56]. Arroyo et al. [56] postulate that the reduction/disappearance of the hypodense areas in the white matter and the stabilising of calcifications, together with improved seizure control relate to improved intestinal absorption. The authors do not clarify whether this relates to improved absorption of nutrients, or AEDs (all patients were on AEDs).
5. Discussion
5.1. Main Findings
All authors discussed the potential theories regarding gluten and epilepsy, but only the study by Gerace et al. [64] sought to explore a possible mechanism underlying the relationship between gluten and epilepsy and gluten related diseases, as the purpose of the study. Although the mechanisms underlying the association between CD and epilepsy are not fully understood, there are three principal hypotheses for potential mechanisms for the association between gluten and epilepsy which were identified by this study. The hypotheses that emerged are:
- Gluten mediated toxicity;
- Gluten involved immune-induced cortical damage; and
- CD related malabsorption of nutrients.
5.2. Gluten Mediated Toxicity
Researchers have proposed the theory that gliadin might have a direct toxic effect on the nervous system and specific brain cells [68]. The only study included in this review that explored gliadin toxicity and seizures, was Gerace et al. [64]. The remaining studies acknowledge toxicity as a potential mechanism linking epilepsy with CD. Gliadin toxicity leading to neuronal damage was suggested [65]. Although kainate is not a cause of seizures in human cases, the use of animal models in this way to replicate epilepsy is generally considered highly valid because they closely reproduce the symptoms and biochemical characteristics of the human disease [69]. Some researchers have theorised that antibodies related to CD may be toxic for neurons and trigger the development of epilepsy [45,70].
The EI manifestations of NCGS affect the nervous system, but also other areas of the body such as the skin and musculoskeletal system [40] and may also include the reproductive system [41]. A number of studies have explored gluten sensitivity with EI manifestations such as tiredness, headache, brain fog [42,43] and neurological and psychiatric disorders such as ataxia [44], anxiety and depression [45,46,47], schizophrenia [48] and epilepsy [49]. For most patients with a neurological manifestation of GS, there are no GI symptoms [50]. Less than 10% of patients with gluten ataxia experience GI symptoms [51]; just over a third will be negative for deaminated-gliadin peptide and tTG2 antibodies [52] but almost three quarters will have circulating antibodies to tissue transglutaminase-6 (TG6) which is primarily associated with the brain [52] and has been associated with CD, epilepsy and cerebral calcifications (CEC) [53].
5.3. Gluten Involved Immune-Mediated Mechanisms
Several studies indicated immune-mediated mechanism linking gluten with epilepsy [56,57,60,61,63,67]. Research by Pratesi et al. [71] showed antibodies of CD patients with EI symptoms significantly reduced after GFD, yet other studies have not confirmed these findings [72,73]. The study by Volta et al. [57] provides support for an autoimmune mechanism linking CD with epilepsy. Autoantibodies TTG, endomysium, and antireticulum have reduced with GFD in patients with epilepsy [74,75,76].
Microbiota and microbiota-derived chemicals, including gut peptides regulate communication between the immune, endocrine, autonomic and enteric nervous systems [77].
Recent evidence from both animal studies and human case studies suggests an imbalance in the microbiome in the gut (known as dysbiosis) may be associated with certain forms of epilepsy [78]. This is an emerging area for research and further work is needed to understand associations; however, it is also recognised that alterations in microbiome may be involved in the immunopathology of CD as there is evidence that gastrointestinal infection and microbiome alterations are associated with the onset or activity of CD [79]. Differences in the composition of the microbiome between patients with CD and patients without it have been reported [80] although no standard CD microbial profile has been identified.
Changes in microbiomes were also seen in a small study of short term GFD [81]. Gut microbe dysregulation could contribute to serotonin dysregulation, as serotonin modulates the cortical excitation/inhibition and imbalance may lead to altered seizure threshold [82]. However, due to the highly individualised pattern of intestinal microbiota, the effect of a GFD on gut microbiota cannot be extrapolated from one population to another [83]. Gut microbiome dysbiosis may be involved in the aetiology of epilepsy [84] due to gut microbiota modulation of proinflammatory T-Cell responses, notably cytokine production, leading to epileptogenesis [85].
Gluten in CD causes an adaptive immune response triggering immune cell activation resulting in an increase in proinflammatory cytokines [86]. Increased gut permeability due to this immune response results in increased neuroinflammation and dysfunction of the blood–brain-barrier leaving the brain vulnerable to gliadin and antigliadin antibodies and antineuronal antibodies [87]. Gliadin has been shown to trigger zonulin which modulates not only intestinal permeability but also blood–brain barrier permeability [88]. Preliminary animal studies have shown antigliadin antibodies cross react with synapsin which it is proposed could alter seizure threshold, providing a potential mechanism for neurological symptoms [89].
Increased levels of cytokines (interleukin 6) in serum or cerebral spinal fluid have been observed in people with epilepsy [90]. Activation of astrocytes and microglial cells has been linked with major proinflammatory pathways in temporal lobe epilepsy [90]. Studies have demonstrated involvement of chemokines and proinflammatory cytokines in the upregulation of genes associated with immune and inflammatory pathways [91]. Although not fully understood, evidence suggests that gliadin triggers upregulation of neuronal response to nerve stimulation in some people. TG6 linked to gluten ataxia [92] and TG6 antibodies have also been associated with CD, epilepsy and cerebral calcifications [93]. High serum anti-tTG antibodies were observed in participants with epilepsy, demonstrating a general stimulation of both innate and adaptive immune response via T cells due to gluten [59,65]. Furthermore, autoimmune disorders are often comorbid with epilepsy [94].
5.4. Malabsorption
Malabsorption caused by CD has been proposed as a potential mechanism contributing to the pathogenesis. Specifically, low levels of folic acid, vitamins B12, D and E have been suggested [95]. Hypocalcaemia has been linked with the development of epilepsy [96]. However, some studies have shown that epilepsy can occur without malabsorption [71,97]. Casciato et al. [60] reported symptoms of vitamin B12 and folate deficiency. Vitamin B12 is important for white matter formation and formation of the myelin sheath. It is hypothesised that if this is compromised it could result in disruption of conductivity of nerves contributing to reduced seizure threshold [55]. Isikay et al. [61] found folic acid levels were lower in a newly diagnosed CD group. The association between low serum and CSF folic acid and CEC was also observed when CD diagnosis is delayed [95]. In a study of 24 patients with CEC, it was suggested that the reduction/disappearance of the hypodense areas in the white matter and the stabilising of calcifications, together with improved seizure control relate to improved intestinal absorption, possibly of folate [56]. Although, as all participants were on AEDs perhaps improved absorption of AEDs might be a factor. Increased serum AEDs were reported by Hernandez et al. [55]. Poor absorption of AEDs has been seen in people with CD [96].
5.5. Timing of Commencement of GFD
5.6. GFD and AEDs
Hernadez et al. [55] found that GFD improved plasma levels of AEDs. Casciato et al. [60] found a rate of 50% positive response to GFD. AED use was documented in five out of the 12 studies included in this review [56,58,60,63,65]. Only two studies investigated the effect of a GFD on AED use, both of the studies reported that after the GFD, AEDs were found to be reduced or discontinued in all of the patients [63,65]. Several case studies have reported GFD resulted in reduction of AEDs [98].
5.7. EEG
Licchetta et al. [58] observed a wide range of EEG variations consistent with the findings of other studies [74,100,101]. Isikay et al. [61] noted a positive correlation between tTG levels and EEG abnormalities in both asleep and awake EEG. This is similar to findings in a study by Emami et al. [92]. Although the overall sample size across the included studies was small, GFD was associated with varying degrees of favourable reduction in abnormalities in all the included studies [56,61,62,65,67] (see Table 2). However, hyperexcitability was observed in one participant despite a GFD [65]. EEG pattern is not disease specific [62]. Abnormalities are indicative of potential epilepsy, and although this can be the case, epilepsy is not the only condition suggested by unusual EEG pattern [102]. For example, endocrine disorders can also show similar EEG irregularities [103,104]. The protocols for EEG recording in the papers included in this review, were not the same, which also limits comparison.
5.8. GFD and Multidisciplinary Team Management
A GFD may result in nutritional deficiencies if poorly implemented and there is evidence that it can be associated with high sugar and low fibre intake if poorly planned [105]. Studies highlight nutrient imbalances when following GFD, particularly in adolescents. GFD can lead to high consumption of lipids and protein and low carbohydrate intake [105], low intake of calcium, fibre and particularly in adolescent girls, low intake of iron [106]. GFD is indicated as a risk factor for metabolic syndrome [107]. It should be noted that no information was provided on the nutritional status of participants in the studies included in this review. Therefore, further studies or research in this area could potentially be improved by consideration of nutritional status. Nutrition professionals are also a useful resource providing information, education, and support for those following a GFD. There is concern regarding self-administration of nutritional supplements and drug interactions for people with epilepsy [108], hence multidisciplinary team working is recommended, and interactions need to be checked. It should be noted sodium starch glycolate can contain gluten and can be used as an excipient in AEDs. GFD has a high rate of non-adherence [109]. Studies have shown that when whole families are following the GFD, transgressions are more likely than when only one member of the family is following the GFD [109]. Non-adherence is also higher among teenagers [109].
5.9. Limitations
Overall there is a paucity of data in this area and none of the studies in this review are randomised controlled trials, the included studies are predominantly single centre studies and they treat epilepsy as a single disorder, whereas it is highly heterogeneous. They are also limited by small numbers of participants which limits generalisability [110]. Furthermore, the participants were preselected, having either epilepsy and CD or CD with differing methods used for CD diagnosis with seizures and all but three were without a control population creating further limitations for comparability and generalisability [110]. Additionally, whilst imaging would not be used as a diagnostic test for epilepsy, it may be used to rule out tumours or calcification, imaging was not used in many of the studies. The studies are from five different countries but most (n = 7) from Italy, which also limits generalisability. Moreover, no standardised GFD protocol exists. Three studies described the method of adherence to GFD [58,60,63]. There were differences in length of GFD in each study and methods of measuring adherence. Compliance with GFD is challenging because gluten is present in many food products [111]. Additionally, for people with CD it is generally accepted that GFD must be permanent [112]. Although, some studies have shown that some people with CD can experience symptom resolution despite transgressions from GFD [111]. Strict adherence to the GFD is critical to assessing whether the intervention might work but, studies show that non-compliance is high [112]. All the included studies in this review implied adherence to GFD but there was a lack of information as to how adherence was assessed. Only two of the studies explicitly stated serological or histological testing to assess compliance with GFD [60,63].
Placebo and nocebo effects of interventions are widely reported in health research [63]. No reference was made to this in the studies included in this review, and therefore it is a factor that affects the reliability. Adherence to existing AED regime was not reported and is therefore a confounding variable and no information about other medications that the participants may be taking. Overall, there is a paucity of research in this field and none of the studies in this review are randomised controlled trials. Consequently, the risk of bias is high and affects the overall quality of evidence available for review.
6. Conclusions
Mechanisms linking gluten with epilepsy are not fully understood but possible hypotheses include gluten mediated toxicity, gluten involved immune-induced cortical damage and CD related malabsorption of dietary nutrients or AEDs. Evidence suggests the effectiveness of a GFD in supporting management of epilepsy when co-morbid with CD, although due to inherent low quality and limitations in methodology, a cautious approach is necessary. There appears to be a growing number of neurologists who are prepared to advocate the use of a GFD; hence multidisciplinary approaches to care are recommended. It could be argued that when balancing potential treatments for epilepsy such as AEDs or surgery with associated side-effects, a well-planned GFD has a low likelihood of harm. Papers about GS and epilepsy were not identified for inclusion in this review and therefore findings do not cover the area of GS and epilepsy. Although there is evidence that GS can at times be exclusively a neurological disease and it is established that patients can show neurological symptoms without gut involvement, this review did not identify studies regarding GS and seizures. Hence, further controlled studies are needed on both GS and epilepsy and CD and epilepsy with tighter protocols concerning education about a GFD before intervention and monitoring compliance with GFD. It is also recommended that research is undertaken to explore the association between GS and antigliadin antibodies and that there is further investigation of the relationship between tTG levels and epilepsy.
Supplementary Materials
The following are available online at https://0-www-mdpi-com.brum.beds.ac.uk/2624-5647/2/3/26/s1, Table S1: List of excluded studies with reasons for exclusion. Table S2: Characteristics of selected studies for review.
Author Contributions
Z.G., conceptualization, data curation, formal analysis, investigation, methodology, project administration, resources, software, validation, visualisation, writing original draft, writing review and editing; J.B., conceptualization, methodology, project administration, supervision, validation, visualisation, writing original draft, writing review and editing. All authors have read and agreed to the published version of the manuscript.
Funding
This project was completed without any external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Singh, A.; Trevick, S. The Epidemiology of Global Epilepsy. Neurol. Clin. 2016, 34, 837–847. [Google Scholar] [CrossRef]
- Jones, C.; Reilly, C. Parental anxiety in childhood epilepsy: A systematic review. Epilepsia 2016, 57, 529–537. [Google Scholar] [CrossRef]
- Altintas, E.; Yerdelen, D.; Taskintuna, N. Social anxiety level in adult patients with epilepsy and their first-degree cohabiting relatives. J. Neuropsychiatry Clin. Neurosci. 2015, 27, 339–344. [Google Scholar] [CrossRef]
- What Is Epilepsy? Available online: http://www.epilepsysociety.org.uk (accessed on 18 March 2019).
- Berg, A.; Berkovic, S.; Brodie, M.; Buchhalter, J.; Cross, J.; Van Emde Boas, W.; Engel, J.; French, J.; Glauser, T.; Mathern, G.; et al. Revised terminology and concepts for organization of seizures and epilepsies: Report of the ILAE Commission on Classification and Terminology, 2005–2009. Epilepsia 2010, 51, 676–685. [Google Scholar] [CrossRef]
- What Is Epilepsy? Epilepsy Research UK: London, UK, 2018.
- Diaz-Arrastia, R.; Agostini, M.A.; Madden, C.J.; Van Ness, P.C. Posttraumatic epilepsy: The endophenotypes of a human model of epileptogenesis. Epilepsia 2009, 50, 14–20. [Google Scholar] [CrossRef]
- Castilla-Guerra, L.; del Carmen Fernandez-Moreno, M.; Lopez-Chozas, M.; Fernandez-Bolanos, R. Electrolytes disturbances and seizures. Epilepsia 2006, 47, 1990–1998. [Google Scholar] [CrossRef]
- Fiest, K.; Sauro, K.; Wiebe, S.; Patten, S.; Kwon, C.; Dykeman, J.; Pringsheim, T.; Lorenzetti, D.; Jette, N. Prevalence and incidence of epilepsy: A systematic review and meta-analysis of international studies. Neurology 2017, 88, 296–303. [Google Scholar] [CrossRef]
- Ferlisi, M.; Shorvon, S. Seizure precipitants (triggering factors) in patients with epilepsy. Epilepsy Behav. 2014, 33, 101–105. [Google Scholar] [CrossRef]
- McKee, H.; Privitera, M.D. Stress as a seizure precipitant: Identification, associated factors and treatment options. Seizure 2017, 44, 21–26. [Google Scholar] [CrossRef]
- Chater, S.; Simpson, K. Effect of passive hyperventilation on seizure duration in patients undergoing ECT. Br. J. Anaesth. 1988, 60, 70–73. [Google Scholar] [CrossRef]
- van Koert, R.R.; Bauer, P.R.; Schuitema, I.; Sander, J.W.; Visser, G.H. Caffeine and seizures: Asystematic review and quantitative analysis. Epilepsy Behav. 2018, 80, 37–47. [Google Scholar] [CrossRef]
- Martin, K.; Jackson, C.F.; Levy, R.G.; Cooper, P.N. Ketogenic diet and other dietary treaments for epilepsy. Cochrane Database Syst. Rev. 2016, 2, CD001903. [Google Scholar]
- Neal, E.; Chaffe, H.; Schwartz, R.; Lawson, M.; Edwards, N.; Fitzsimmons, G.; Whitney, A.; Cross, J. The ketogenic diet for the treatment of childhood epilepsy: A randomised controlled trial. Lancet Neurol. 2008, 7, 500–506. [Google Scholar] [CrossRef]
- Zhang, Y.; Xu, J.; Zhang, K.; Yang, W.; Li, B. The anticonvulsant effects of ketogenic diet on epileptic seizures and potential mechanisms. Curr. Neuropharmacol. 2018, 16, 66–70. [Google Scholar] [CrossRef]
- Bough, K.; Wetherington, J.; Hassel, B.; Pare, J.; Gawryluk, J.; Greene, J.; Shaw, R.; Smith, Y.; Geiger, J.; Dingledine, R. Mitochondrial Biogenesis in the Anticonvulsant Mechanism of the Ketogenic Diet. Ann. Neurol. 2006, 60, 223–235. [Google Scholar] [CrossRef]
- Epilepsies: Diagnosis and Management. Clinical Guideline [CG137]: NICE; NICE National Institute for Health and Care Excellence: London, UK, 2012.
- Biesiekierski, J.R. What is gluten? J. Gastroenterol. Hepatol. 2017, 32, 78–81. [Google Scholar] [CrossRef] [Green Version]
- Husby, S.; Koletzko, S.; Korponay-Szabo, I.; Mearin, M.; Phillips, A.; Shamir, R. European Society for Pediatric Gastroenterology, Hepatology, and Nutrition guidelines for the diagnoss of coeliac disease. J. Pediatric Gastroenterol. Nutr. 2012, 54, 136–160. [Google Scholar] [CrossRef]
- Catassi, C.; Gatti, S.; Fasano, A. The new epidemiology of celiac disease. J. Pediatric Gastroenterol. Nutr. 2014, 59, 7–9. [Google Scholar] [CrossRef] [Green Version]
- Sollid, L.M. Coeliac disease: Dissecting a complex inflammatory disorder. Nat. Rev. 2002, 2, 647–655. [Google Scholar] [CrossRef]
- Fasano, A.; Catassi, C. Clinical Practice. Celiac disease. N. Engl. J. Med. 2012, 367, 2419–2426. [Google Scholar] [CrossRef]
- Ludvigsson, J.F.; Leffler, D.A.; Bai, J.C.; Biai, F.; Fasano, A.; Green, P.; Hadjivassilliou, M.; Kaukinen, K.; Kelly, C.; Leonard, J.N.; et al. The Oslo definitions for coeliac disease and related terms. Gut 2013, 62, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Garsed, K.; Scott, B.B. Can oats be taken in a gluten-free diet? A systematic review. Scand. J. Gastroenterol. 2007, 42, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Silano, M.; Dessi, M.; De Vincenzi, M.; Cornell, H. In vitro tests indicate that certain varieties of oats may be harmful to patients with coeliac disease. J. Gastroenterol. Hepatol. 2007, 22, 528–531. [Google Scholar] [CrossRef]
- Rostami, K.; Bold, J.; Parr, A.; Johnson, M. Gluten-free diet indications, safety, quality, labels and challenges. Nutrients 2017, 9, 846. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Sabatino, A.; Corazza, G.R. Clinical Practice. Celiac disease. Lancet 2009, 373, 1480–1493. [Google Scholar] [CrossRef]
- Abdulkarim, A.S.; Burgart, L.J.; See, J.; Murray, J.A. Eitiology of nonresponsive celiac disease: Results of a systematic approach. Am. J. Gastroenterol. 2002, 97, 2016–2021. [Google Scholar] [CrossRef] [PubMed]
- Spence, D. Bad medicine: Food intolerance. Br. Med. J. 2013, 346. [Google Scholar] [CrossRef] [PubMed]
- Catassi, C.; Bai, J.; Bonaz, B.; Bouma, G.; Calabro, A.; Carroccio, A.; Castillejo, G.; Ciacci, C.; Cristofori, F.; Dolinsek, J.; et al. Non-celiac gluten sensitivity: The new frontier of gluten related disorders. Nutrients 2013, 5, 3839–3853. [Google Scholar] [CrossRef]
- Biesiekierski, J.R.; Iven, J. Non-coeliac gluten sensitivity: Piecing the puzzle together. United Eur. Gastroenterol. J. 2015, 3, 160–165. [Google Scholar] [CrossRef] [Green Version]
- Sapone, A.; Bai, J.C.; Dolinsek, J.; Green, P.H.; Hadjivassiliou, M.; Kaukinen, K.; Rostami, K.; Sanders, D.S.; Schumann, M.; Ullrich, R.; et al. Spectrum of gluten-related disorders: Consensus on new nomeclature and classification. BMC Med. 2012, 10, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Catassi, C.; Elli, L.; Bonaz, B.; Bouma, G.; Carroccio, A.; Cellier, C.; Cristofori, F.; de Magistris, L.; Dolinsek, J.; Dieterich, W.; et al. Diagnosis of non-celiac gluten sensitivity (NCGS): The Salerno experts’ criteria. Nutrients 2015, 7, 4966–4977. [Google Scholar] [CrossRef] [PubMed]
- Volta, U.; Bardella, M.T.; Calabro, A.; Troncone, R.; Corazza, G.R. Study group for non-coeliac gluten sensitivity. BMC Med. 2014, 12. [Google Scholar] [CrossRef]
- Molina-Infante, J.; Santolaria, S.; Sanders, D.S.; Fernandez-Banares, F. Systematic review: Noncoeliac gluten sensitivity. Aliment. Pharmacol. Ther. 2015, 41, 807–820. [Google Scholar] [CrossRef]
- Tonutti, E.; Bizzaro, N. Diagnosis and classification of celiac disease and gluten sensitivity. Autoimmun. Rev. 2014, 13, 472–476. [Google Scholar] [CrossRef]
- Sapone, A.; Lammers, K.M.; Mazzarella, G.; Mikhailenko, I.; Carten, M.; Casolaro, V.; Fasano, A. Differential mucosal IL-17 expression in two gliadin-induced disorders: Guten sensitivity and the autoimmune enteropathy celiac disease. Int. Arch. Allergy Immunol. 2010, 152, 75–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, Z.; Si, Q.; Xiaoyi, Z. Association between epilepsy and systemic autoimmune diseases: A meta-analysis. Seizure 2016, 41, 160–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ludvigsson, J.F.; Zingone, F.; Tomson, T.; Ekbom, A.; Ciacci, C. Increased risk of epilepsy in biopsy-verified celiac disease: A population-based cohort study. Neurology 2012, 78, 1401–1407. [Google Scholar] [CrossRef]
- Rana, A.; Musto, A. The role of inflammation in the development of epilepsy. J. Neuroinflamm. 2018, 15, 144. [Google Scholar] [CrossRef]
- Hadjivassiliou, M.; Sanders, D.; Grunewald, R.; Woodroofe, N.; Boscolo, S.; Aeschlimann, D. Gluten sensitivity: From gut to brain. Lancet Neurol. 2010, 9, 318–330. [Google Scholar] [CrossRef]
- Fois, A.; Vascotto, M.; Di Bartolo, R.M.; Di Marco, V. Celiac disease and epilepsy in pediatric patients. Childs Nerv. Syst. 1994, 10, 450–454. [Google Scholar] [CrossRef]
- Zelnik, N.; Pacht, A.; Obeid, R.; Lerner, A. Range of neurologic disorders in patients with celiac disease. Pediatrics 2004, 113, 1672–1676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canales, P.; Mery, V.P.; Larrondo, F.J.; Bravo, F.L.; Godoy, J. Epilepsy and celiac disease: Favourable outcome with a gluten-free diet in a patient refractory to antiepileptic drugs. Neurologist 2006, 12, 318–321. [Google Scholar] [CrossRef] [PubMed]
- Hadjivassiliou, M.; Dasappaiah, G.; Grunewald, R.; Aeschlimann, D.; Sarrigiannis, P.; Hoggard, N.; Aeschlimann, P.; Mooney, P.; DAvid, S. Neurological dysfunction in coeliac disease and non-coeliac gluten sensitivity. Am. J. Gastroenterol. 2016, 9, 561–567. [Google Scholar] [CrossRef] [Green Version]
- Peltola, M.; Kaukinen, K.; Dastidar, P.; Haimila, K.; Partanen, J.; Haapala, A.; Maki, M.; Keranen, T.; Peltola, J. Hippocampal sclerosis in refractory temporal lobe epilepsy is associated with gluten sensitivity. J. Neurol. Neurosurg. Psychiatry 2009, 80, 626–630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pratesi, R.; Modelli, I.C.; Martins, R.C.; Almeida, P.L.; Gandolfi, L. Celiac disease and epilepsy:favourable outcome in a child with difficult to control seizures. Acta Neurol. Scand. 2003, 108, 290–293. [Google Scholar] [CrossRef] [PubMed]
- Gough, D.; Oliver, S.; Thomas, J. Introducing Systematic Reviews. In An Introduction to Systematic Reviews; Gough, D., Oliver, S., Thomas, J., Eds.; Sage Publications Ltd.: London, UK, 2017; pp. 1–17. [Google Scholar]
- Petticrew, M.; Roberts, H. Systematic Reviews in the Social Sciences: A Practical Guide; Blackwell: Oxford, UK, 2006. [Google Scholar]
- Boland, A.; Cherry, G.; Dickson, R. Doing a Systematic Review; Sage: London, UK, 2017. [Google Scholar]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ionnidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analysis of studies that evaluate health care interventions: Explanation and elaboration. Ann. Int. Med. 2009, 151, 65–94. [Google Scholar] [CrossRef] [Green Version]
- Critical Appraisal Skills Programme (CASP). 2017. Available online: https://casp-uk.net/casp-tools-checklists/ (accessed on 24 November 2018).
- Gobbi, G.; Bouquet, F.; Greco, L.; Lambertini, A.; Tassinari, C.; Ventura, A.; Zaniboni, M. Coeliac disease, epilepsy, and calcifications. The Italian Working Group on Coeliac Disease and Epilepsy. Lancet 1992, 340, 439–443. [Google Scholar]
- Hernadez, M.A.; Colina, G.; Ortigosa, L. Epilepsy, cerebral calcifications and clinical or subclinical coeliac disease. Course and follow up with gluten-free diet. Seizure 1998, 7, 49–54. [Google Scholar] [CrossRef] [Green Version]
- Arroyo, H.A.; De Rosa, S.; Ruggieri, V.; de Davila, M.T.G.; Fejerman, N. Epilepsy, occipital calcifications, and oligosymptomatic celiac disease in childhood. J. Child Neurol. 2002, 17, 800–806. [Google Scholar] [CrossRef]
- Volta, U.; De Giorgio, R.; Petrolini, N.; Stanghellini, V.; Barbara, G.; Granito, F.; De Ponti, F. Clinical findings and anti-neuronal antibodies in coeliac disease with neurological disorders. Scand. J. Gastroenterol. 2002, 37, 1276–1281. [Google Scholar] [CrossRef]
- Licchetta, L.; Bisulli, F.; Di Vito, L.; La Morgia, C.; Naldi, I.; Volta, U.; Tinuper, P. Epilepsy in coeliac disease: Not just a matter of calcifications. Neurol. Sci. 2011, 32, 1069–1074. [Google Scholar] [CrossRef] [PubMed]
- Berio, A.; Mangiate, G.; Mariottini, G.L.; Piazzi, A. Gluten sensitivity and neurological manifestations. J. Biol. Res. 2015, 88, 170–172. [Google Scholar] [CrossRef]
- Casciato, S.; Morano, A.; Albini, M.; Fanella, M.; Lapenta, L.; Fattouch, J.; Carni, M.; Colonnese, C.; Manfredi, M.; Giallonardo, A.T.; et al. Crytogenic focal epilepsy and "hidden" celiac disease in adulthood: A causal or accidental link? Int. J. Neurosci. 2015, 125, 913–917. [Google Scholar] [CrossRef] [PubMed]
- Isikay, S.; Kocamaz, H.; Sezer, S.; Ozkars, M.; Isikay, N.; Filik, B.; San, M.; Kanmaz, A. The frequency of epileptiform discharges in celiac disease. Pediatric Neurol. 2015, 53, 78–82. [Google Scholar] [CrossRef] [PubMed]
- Parisi, P.; Pietropaoli, N.; Ferreti, A.; Nenna, R.; Mastrogiorgio, G.; Del Pozzo, M.; Principessa, L.; Bonamico, M.; Villa, M.P. Role of gluten-free diet on neurological-EEG findings and sleep disordered breathing in children with celiac disease. Seizure 2015, 25, 181–183. [Google Scholar] [CrossRef] [Green Version]
- Bashiri, H.; Afshari, D.; Babaei, N.; Ghadami, M. Celiac disease and epilepsy: The effect of gluten-free diet on seizure control. Adv. Clin. Exp. Med. 2016, 25, 751–754. [Google Scholar] [CrossRef] [Green Version]
- Gerace, E.; Resta, F.; Landucci, E.; Renzi, D.; Masi, A.; Pellegrini-Giampietro, D.E.; Calabro, A.; Mannaioni, G. The gliadin peptide 31-43 exacerbateskainate neurotoxicity in epilepsy models. Sci. Rep. 2017, 7, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Sel, C.G.; Aksoy, E.; Aksoy, A.; Yuksel, D.; Ozbay, F. Neurological manifestations of atypical celiac disease in childhood. Acta Neurol. Belg. 2017, 117, 719–727. [Google Scholar] [CrossRef]
- Falcon-Moya, R.; Sihra, T.S.; Rodriguez-Moreno, A. Kainate receptors: Role in epilepsy. Front. Mol. Neurosci. 2018, 11. [Google Scholar] [CrossRef]
- Berio, A.; Badolati, G.; Mangiante, G.; Calcagno, E.; Piazzi, A. Anti-tissue transglutaminase antibodies and EEG pattern in celiac patients on prolonged gluten-free diet. J. Biol. Res. 2013, 86. [Google Scholar] [CrossRef] [Green Version]
- Giovanni, C.; Sanchez, M.; Straface, E.; Scazzocchio, B.; Silano, M.; De Vincenzi, M. Induction of apoptosis in caco-2 cells by wheat gliadin peptides. Toxicology 2000, 145, 63–71. [Google Scholar] [CrossRef]
- Kandratavicius, L.; Balista, P.A.; Lopes-Aguiar, C.; Ruggiero, R.N.; Umeoka, E.H.; Garcia-Cairasco, N.; Bueno-Junior, L.S.; Leite, J.P. Animal models of epilepsy: Use and limitations. Neuropsychiatr. Dis. Treat. 2014, 10, 1693–1705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pennisi, M.; Bramanti, A.; Cantone, M.; Pennisi, G.; Bella, R.; Lanza, G. Neurophysiology of the "celiac brain": Disentangling gut-brain connections. Front. Neurosci. 2017, 11, 498. [Google Scholar] [CrossRef] [PubMed]
- Pratesi, R.; Gandolfi, L.; Friedman, H.; Farage, L.; De Castro, C.A.M.; Catassi, C. Serum IgA antibodies from patients with coeliac disease strongly react with human brain blood-vessel structures. Scand. J. Gastroenterol. 1998, 33, 817–822. [Google Scholar] [PubMed]
- Pellecchia, M.T.; Scala, R.; Filla, A.; De Michele, G.; Ciacci, C.; Barone, P. Idiopathic cerebellar ataxia associated with celiac disease: Lack of distinctive neurological features. J. Neurol. Neurosurg. Psychiatry 1999, 66, 32–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salur, L.; Uibo, O.; Talvik, I.; Justus, I.; Metskula, K.; Talvik, T.; Uibo, R. The high frequency of coeliac disease among children with neurological disorders. Eur. J. Neurol. 2002, 7, 707–711. [Google Scholar] [CrossRef] [PubMed]
- Labate, A.; Gambardella, A.; Messina, D.; Tammaro, S.; Le Piane, E.; Pirritano, D.; Cosco, C.; Doldo, P.; Mazzei, R.; Oliveri, R.L.; et al. Silent celiac disease in patients with childhood localization-related epilepsies. Epilepsia 2001, 42, 1153–1155. [Google Scholar] [CrossRef] [Green Version]
- Mavroudi, A.; Karatza, E.; Papastravou, T.; Panteliadis, C.; Spiroglou, K. Successful treatment of epilepsy and celiac disease with a gluten-free diet. Pediatric Neurol. 2005, 33, 292–295. [Google Scholar] [CrossRef]
- Emami, M.H.; Taheri, H.; Kohestani, S.; Chitsaz, A.; Etemadifar, M. How frequent is celiac disease among epileptic patients? J. Gastroenterol. Liver Dis. 2008, 17, 379–382. [Google Scholar]
- Geuking, M.B.; Koller, Y.; Rupp, S.; McCoy, K.D. The interplay between the gut microbiota and the immune system. Gut Microbes 2014, 5, 411–418. [Google Scholar] [CrossRef]
- Dahlin, M.; Prast-Neilsen, S. The gut and epilepsy. EBioMedicine 2019, 44, 741–746. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verdu, E.; Galipeau, H.; Jabri, B. Novel players in coeliac disease pathogenesis: Role of the gut microbiota. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Valitutti, F.; Cucchiara, S.; Fasano, A. Celiac disease and the microbiome. Nutrients 2019, 11, 2403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonder, M.J.; Tigchelaar, E.F.; Cai, X.; Trynka, G.; Cenit, M.C.; Hrdlickova, B.; Zhong, H.; Vatanen, T.; Gevers, D.; Wijmenga, C.; et al. The influence of a short-term gluten-free diet on the gut microbiome. Genome Med. 2016, 8, 45. [Google Scholar] [CrossRef]
- Epps, S.A.; Weinshenker, D. Rhythm and blues: Animal models of epilepsy and depression comorbidity. Biochem. Pharmacol. 2013, 85, 135–146. [Google Scholar] [CrossRef] [Green Version]
- Garcia-Mazcorro, J.F.; Noratto, G.; Remes-Troche, J.M. The effect of gluten-free diet on health and the gut microbiota cannot be extrapolated from one population to others. Nutrients 2018, 10, 1421. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.; Zhang, Y.; Yang, H.; Rao, Y.; Miao, J.; Lu, X. Intestinal Microbiota as an Alternative Therapeutic Target for Epilepsy. Can. J. Infect. Dis. Med Microbiol. 2016, 2016, 9032809. [Google Scholar] [CrossRef] [Green Version]
- Ye, F.; Chen, G.; Bao, Y.; Hua, Z.; Wang, D.; Bao, Y. Effect of topiramate on interleukin 6 expression in the hippocampus of amygdala-kindled epileptic rats. Exp. Ther. Med. 2014, 7, 223–227. [Google Scholar] [CrossRef]
- Cani, P.D.; Everard, A.; Duparc, T. Gut microbiota, enteroendocrine functions and metabolism. Curr. Opin. Pharmacol. 2013, 13, 935–940. [Google Scholar] [CrossRef]
- Pruimbom, L.; de Punder, K. The opioid effects of gluten exorphins: Asymptomatic celiac disease. J. Health Popul. Nutr. 2015, 33, 1–31. [Google Scholar] [CrossRef] [Green Version]
- Fasano, A. Zonulin and its regulation of intestinal barrier function: The biological door to inflammation, autoimmunity and cancer. Physiol. Rev. 2011, 91, 151–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alaedini, A.; Okamoto, H.; Briani, C.; Wollenberg, K.; Shill, H.A.; Bushara, K.O.; Sander, H.W.; Green, P.H.R.; Hallett, M.; Latov, N. Immune cross-reactivity in celiac disease: Anti-gliadin antiboides bind to neuronal synapsin I. J. Immunol. 2007, 178, 6590–6595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aronica, E.; Crino, P.B. Inflammation in epilepsy: Clinical observations. Epilepsia 2011, 52, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Aronica, E.; Gorter, J.A. Gene expression profile in temporal lobe epilepsy. Neuroscientist 2007, 13, 100–108. [Google Scholar] [CrossRef]
- Aziz, I.; Hadjivassiliou, M. Coeliac disease: Noncoeliac gluten sensitivity—Food for thought. Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 398–399. [Google Scholar] [CrossRef]
- Johnson, A.M.; Dale, R.C.; Wienholt, L.; Hadjivassiliou, M.; Aeschlimann, D.; Lawson, J.A. Coeliac disease, epilepsy, and cerebral calcifications: Association with TG6 autoantibodies. Dev. Med. Child Neurol. 2012, 55, 90–93. [Google Scholar] [CrossRef]
- Amanat, M.; Thijs, R.D.; Salehi, M.; Sander, J.W. Seizures as a clinical manifestation in somatic autoimmune disorders. Seizure 2018, 12. [Google Scholar] [CrossRef] [Green Version]
- Lea, M.E.; Harbord, M.; Sage, M.R. Bilateral occipital calcification associated with celiac disease, folate deficiency, and epilepsy. Am. J. Neuroradiol. 1995, 16, 1498–1500. [Google Scholar]
- Maniar, V.; Yadav, S.; Gokhale, Y. Intractable seizures and metabolic bone disease secondary to celiac disease. J. Assoc. Physicians India 2010, 58, 512–515. [Google Scholar]
- Hadjivassiliou, M.; Gibson, A.; Davies-Jones, G.A.B.; Lobo, A.; Stephenson, T.J.; Millford-Ward, A. Does cryptic gluten sensitivity play a part in neurological illness? Lancet 1996, 347, 369–371. [Google Scholar] [CrossRef]
- Molteni, N.; Bardella, M.T.; Baldassarri, A.R.; Bianchi, P.A. Celiac disease associated with epilepsy and intracranial calcifications: Report of two patients. Am. J. Gastroenterol. 1988, 83, 992–994. [Google Scholar] [PubMed]
- Sansotta, N.; Amirikian, K.; Guandalini, S.; Jericho, H. Celiac disease symptom resolution: Effectiveness of the gluten-free diet. J. Pediatric Gastroenterol. Nutr. 2018, 66, 48–52. [Google Scholar] [CrossRef] [PubMed]
- Pratesi, R.; Gandolfi, L.; Martins, R.C.; Tauil, P.; Nobrega, Y.N.; Teixeira, W.A. Is the prevalence of celiac disease increased among epiletic patients? Arq. Neuro-Psiquiatr. 2003, 61, 330–334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lionetti, E.; Francavilla, R.; Pavone, P.; Pavone, L.; Francavilla, T.; Pulvirenti, A. The neurology of coeliac disease in childhood: What is the evidence? A systematic review and meta-analysis. Dev. Med. Child Neurol. 2010, 52, 700–707. [Google Scholar] [CrossRef]
- Benbadis, S.R.; Tatum, W.O. Overinterpretation of EEGs and misdiagnosis of epilepsy. J. Clin. Neurophysiol. 2003, 20, 42–44. [Google Scholar] [CrossRef]
- Smith, S.J.M. EEG in neurological conditions other than epilepsy: When does it help, what does it add? J. Neurol. Neurosurg. Psychiatry 2005, 76, 8–12. [Google Scholar] [CrossRef] [Green Version]
- Vincent, A.; Crino, P.B. Systemic and neurologic autoimmune disorders assoicated with seizures or epilepsy. Epilepsia 2011, 52, 12–17. [Google Scholar] [CrossRef]
- Vici, G.; Belli, L.; Biondi, M.; Polzonetti, V. Gluten free diet and nutrient deficiencies: A review. Clin. Nutr. 2016, 35, 1236–1241. [Google Scholar] [CrossRef]
- Mariani, P.; Viti, M.G.; Montuori, M.; La Vecchia, A.; Cipolletta, E.; Calvani, L.; Bonamico, M. The gluten-free diet: A nutritional risk factor for adolescents with celiac disease? J. Pediatr. Gastroenterol. Nutr. 1998, 27, 519–523. [Google Scholar] [CrossRef]
- Tortora, R.; Capone, P.; De Stefano, G. Metabolic syndrome in patients with coeliac disease on a gluten-free diet. Aliment. Pharmacol. Ther. 2015, 41, 352–359. [Google Scholar] [CrossRef] [Green Version]
- Patsalos, P.N.; Froscher, W.; Pisani, F.; van Rijn, C.M. The importance of drug interations in epilepsy therapy. Epilepsia 2002, 43, 365–385. [Google Scholar] [CrossRef] [PubMed]
- Xhakollari, V.; Canavari, M.; Osman, M. Factors affecting consumers’ adherence to gluten-free diet, a systematic review. Trends Food Sci. Technol. 2019, 85, 23–33. [Google Scholar] [CrossRef]
- Greenhalgh, T. How to Read a Paper. The Basics of Evidence-Based Medicine, 5th ed.; John Wiley and Sons: Chichester, UK, 2014. [Google Scholar]
- Balakireva, A.V.; Zamyatin, J.A. Properties of gluten intolerance: Gluten structure, evolution and detoxification properties. Nutrients 2016, 8, 644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Itzlinger, A.; Branchi, F.; Schumann, M. Gluten-free diet in celiac disease—Forever and for all? Nutrients 2018, 10, 1796. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Prisma flow diagram.

{kind=link}
Table 1.
Inclusion criteria.
| Location | Worldwide |
| Language | English |
| Population | No age restriction, people with a diagnosis of idiopathic epilepsy (irrespective of seizure type); people with seizure disorders and CD with seizure-related neurological abnormalities Animal studies/models investigating gluten and seizure/epileptiform activity EEG |
| Intervention | Gluten-free diet |
| Comparisons | No intervention |
| Setting | No restriction |
| Outcomes | Any of the following: Reduction in seizures Reduction in medication Reduction in EEG abnormalities Adverse reactions Cognitive or behavioural outcomes Quality of life outcomes |
| Study design |
|
Table 2.
Study results summary.
| Study | Number of Participants on GFD | Method of Measuring Adherence to Gluten-Free Diet | Outcome Seizure Reduction | Outcome AED Reduction | EEG before GFD | EEG after GFD | Adverse Outcome |
|---|---|---|---|---|---|---|---|
| Arroyo 2002 | 24 | Patients described as compliant with diet in group 3 and implied for other patients Authors comment on patients who had not strictly followed the diet which indicates adherence was monitored | 11 patients (45.8%) on AED became seizure free before GFD Nine patients (37.5%) who were on AED became seizure free after introduction of GFD | Not documented | 15/32 normal | 20/32 normal | Four patients on an AED had uncontrolled seizures Three developed epileptic encephalopathy despite GFD |
| Bashiri 2016 | 7 | Intestinal biopsy repeated 3 months after starting GFD | Six patients became seizure free One patient seizures controlled | AEDs discontinued in 6 patients AED reduced by half in 1 patient | n/a | n/a | None reported |
| Berio 2013 | 12 | Groups differentiated good/poor compliance | n/a | n/a | Not measured | 5/6 normal with good compliance to GFD 5/6 abnormal with poor compliance | None reported |
| Casciato 2015 | 10 | Serological and histological testing | Two patients non-compliant GFDOne patient lost at follow-up Of the remaining seven patients: Three patients became seizure free Three reduction in number of seizures One no change | Not reported | 10 abnormal | Not measured | None reported |
| Gobbi 1992 | 29 20 followed up | Adherence assumed. Authors state patients were ‘prescribed’ a GFD | Four patients’ seizures decreased by more than 50% Six patients seizure free; Nine patients no change | Not reported | Four normal 25 abnormal | Not measured | One patient increased seizures >50% |
| Hernandez 1998 | 4 | Monitored and reported Poor compliance noted | Patient 1: seizure frequency decreased by 30% Patient 2: seizure free Patient 3: seizure frequency decreased by 10% Patient 4: seizure frequency decreased by 50% | Not reported | Four abnormal | Not measured | None reported |
| Isikay 2015 | 132 patients 99 controls | Notes ‘effective GFD’ for formerly diagnosed CD patients and ‘ineffective GFD’ for newly diagnosed CD patients | n/a | n/a | Four new patients abnormal 9.3% Two former patients abnormal 1.5% One control case abnormal 1% | All normal, including case control which spontaneously normalised | None reported |
| Liccheta 2011 | 8 | Control visit interviews in the last 12 months to assess compliance | Five patients no clinical benefit One patient reduced seizure frequency One patient seizure free. One not F/U | Not reported | Eight abnormal | Not reported | None reported |
| Parisi 2014 | 19 | Complete adherence confirmed by parents | n/a | n/a | Nine abnormal | One abnormal One unknown (parents refused follow-up EEG) Seven normal (77.7%) | None reported |
| Sel 2017 | 5 | Adherence implied. Reported non-compliance in 1 patient | Three patients stopped AEDs One due to stop AEDs | Three patients stopped AEDs One due to stop AEDs | Four abnormal One normal | None reported | |
| Volta 2002 | 3 | Monitored, recorded and reported in paper | Two patients improved, one patient not | n/a | n/a | n/a | None reported |
Table 3.
Characteristics of participants in studies selected for review.
| Study | Mean Age (Years) | Sex f/m | Mean Age at Seizure Onset (Years) | Seizure Type | Seizure Frequency | EEG | AEDs | Gastrointestinal Symptoms | Coeliac Disease |
|---|---|---|---|---|---|---|---|---|---|
| Arroyo 2002 | 11 | 22/10 | 6.13 | 31 partial One generalised tonic-clonic | Most patients: monthly or less Three patients daily | 19 normal 13 abnormal | Yes, all | Absent or rare at time of CD diagnosis but chronic diarrhoea in all cases, appearing at mean age 2.8 years, preceding seizure onset | Yes Biopsy proven |
| Bashiri 2016 | 30.2 | 3/4 | 16.2 | 46% generalised tonic-clonic 38% complex partial | Three patients weekly Four patients monthly | Not measured | Yes, all | No | Yes IgA serum antibodiesBiopsy proven |
| Berio 2013 | 10–44 | Not reported | No seizures | n/a | n/a | Five normal Six abnormal One not measured | n/a | Not reported | Yes anti-tTG serum antibodies and/or biopsy proven |
| Casciato 2015 | 31.5 | 9/1 | 21.4 | Six generalised tonic-clonic Four partial | Two patients daily Three patients weekly Five patients monthly | 10 abnormal | Yes, all | Yes, three | Yes IgA/IgG-Ttg, IgA/IgG-DGP and IgA EMA serum antibodies Biopsy proven |
| Gerace 2017 | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a | n/a |
| Gobbi 1992 | 16.4 | 28/15 | 4.5 | Five generalised tonic-clonic 24 partial | Eight patients >1/day Seven patients >1/week Five patients >1/month | Four normal 25 abnormal | Not reported | Yes, 26 No, three | Yes Biopsy proven |
| Hernandez 1998 | 18 | 1/3 | 7 | Three partial One generalised tonic-clonic | Two patients > 1/day One patient > 1/week One patient = 1/week | Four abnormal | Not reported | Yes, two No, two | Yes Biopsy proven |
| Isikay 2015 | 10.6 | 76/56 | n/a | n/a | n/a | Four new patients abnormal 9.3% Two former patients abnormal 1.5% One control case abnormal 1% | n/a | Yes, 121 No, 11 | Yes Biopsy proven |
| Liccheta 2011 | 25.7 | 7/1 | 12.85 | Eight partial | 2 >daily 3 daily 2 weekly 1 yearly | Eight abnormal | Yes, all | No | Yes Biopsy proven |
| Parisi 2014 | 9.82 | 16/3 | No seizures | n/a | n/a | Nine abnormal After 6 months GFD EEG abnormalities in one patient and one patient unknown as parents refused follow-up EEG | n/a | Not reported | Yes Biopsy proven |
| Sel 2017 | 6.4 | 0/4 | 4.5 | Two generalised tonic-clonic Two partial One no seizures (EEG abnormalities only) | Not documented | All normalised | Four out of five | No | Yes Biopsy proven Anti-tTG serum antibodies |
| Volta 2002 | 32 | 3/0 | 23 | One complex partial temporal lobe One simple partial One generalised absence | Not documented | Not measured | Not documented | Yes, one No, two | Yes Biopsy proven IgaAGA, IgAEMA, IgA h-tTGA serum antibodies |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Gilbey, Z.; Bold, J. A Gluten Free Diet in the Management of Epilepsy in People with Coeliac Disease or Gluten Sensitivity. Gastrointest. Disord. 2020, 2, 281-299. https://0-doi-org.brum.beds.ac.uk/10.3390/gidisord2030026
AMA Style
Gilbey Z, Bold J. A Gluten Free Diet in the Management of Epilepsy in People with Coeliac Disease or Gluten Sensitivity. Gastrointestinal Disorders. 2020; 2(3):281-299. https://0-doi-org.brum.beds.ac.uk/10.3390/gidisord2030026
Chicago/Turabian StyleGilbey, Zoë, and Justine Bold. 2020. "A Gluten Free Diet in the Management of Epilepsy in People with Coeliac Disease or Gluten Sensitivity" Gastrointestinal Disorders 2, no. 3: 281-299. https://0-doi-org.brum.beds.ac.uk/10.3390/gidisord2030026