
Development of a Three-Dimensional (3D) Printed Biodegradable Cage to Convert Morselized Corticocancellous Bone Chips into a Structured Cortical Bone Graft

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
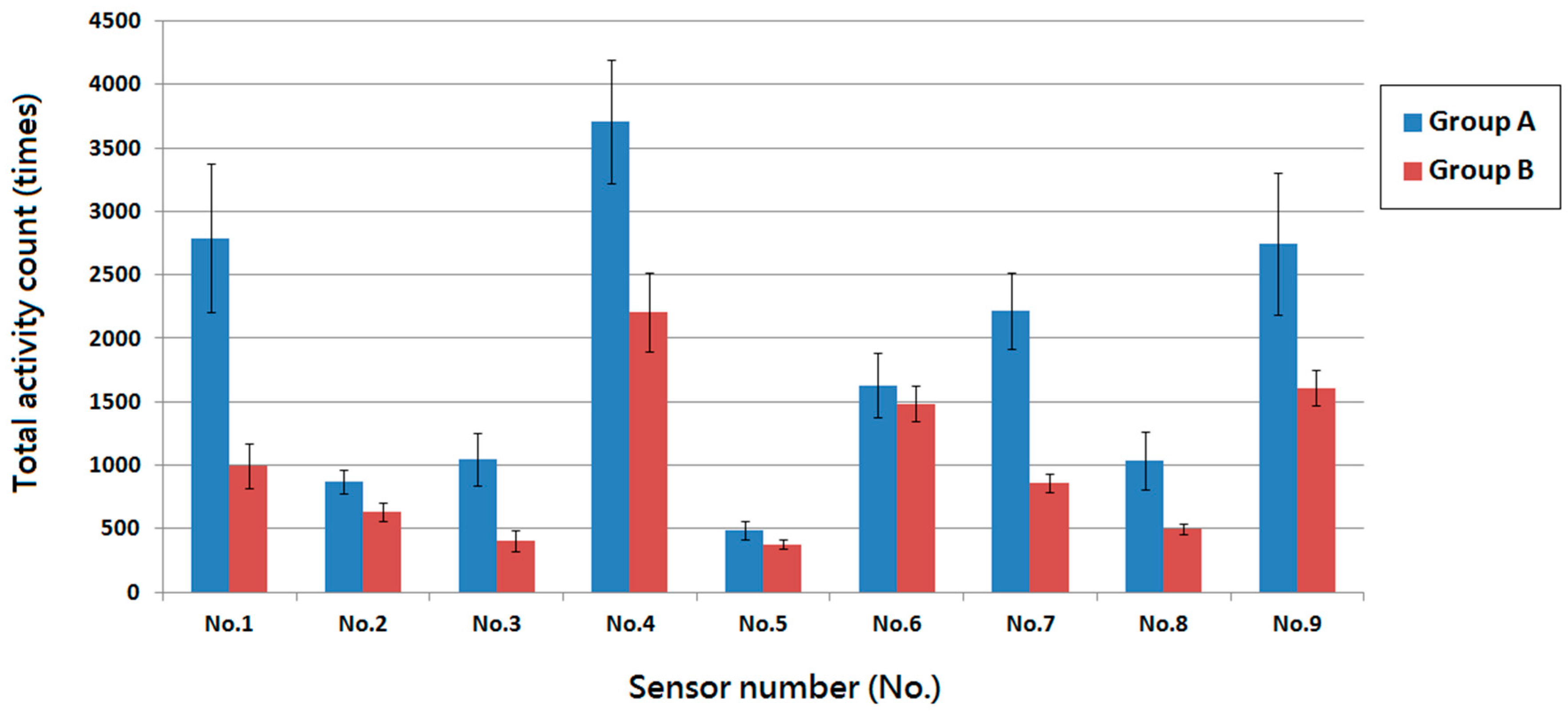
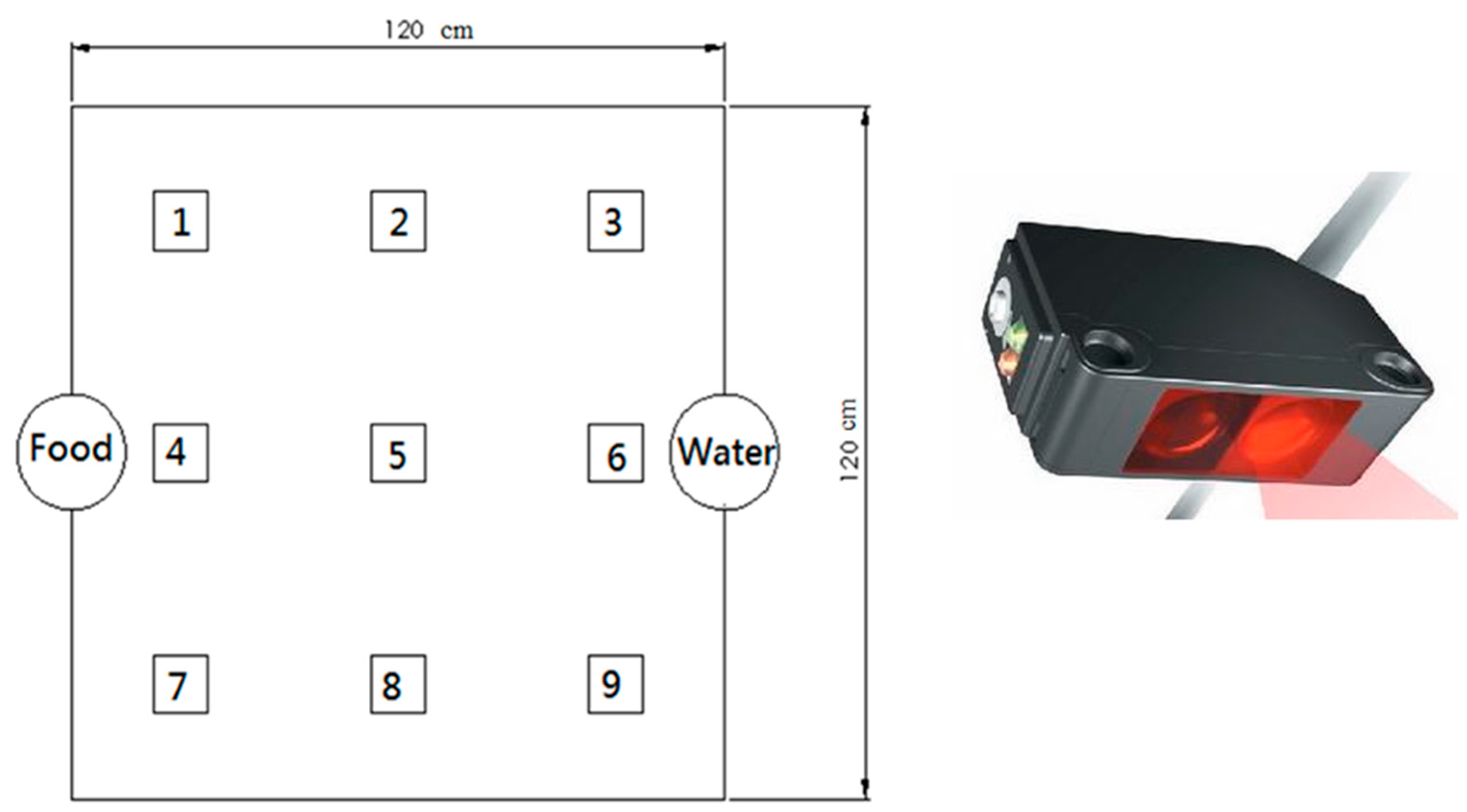
2.1. Animal Activity
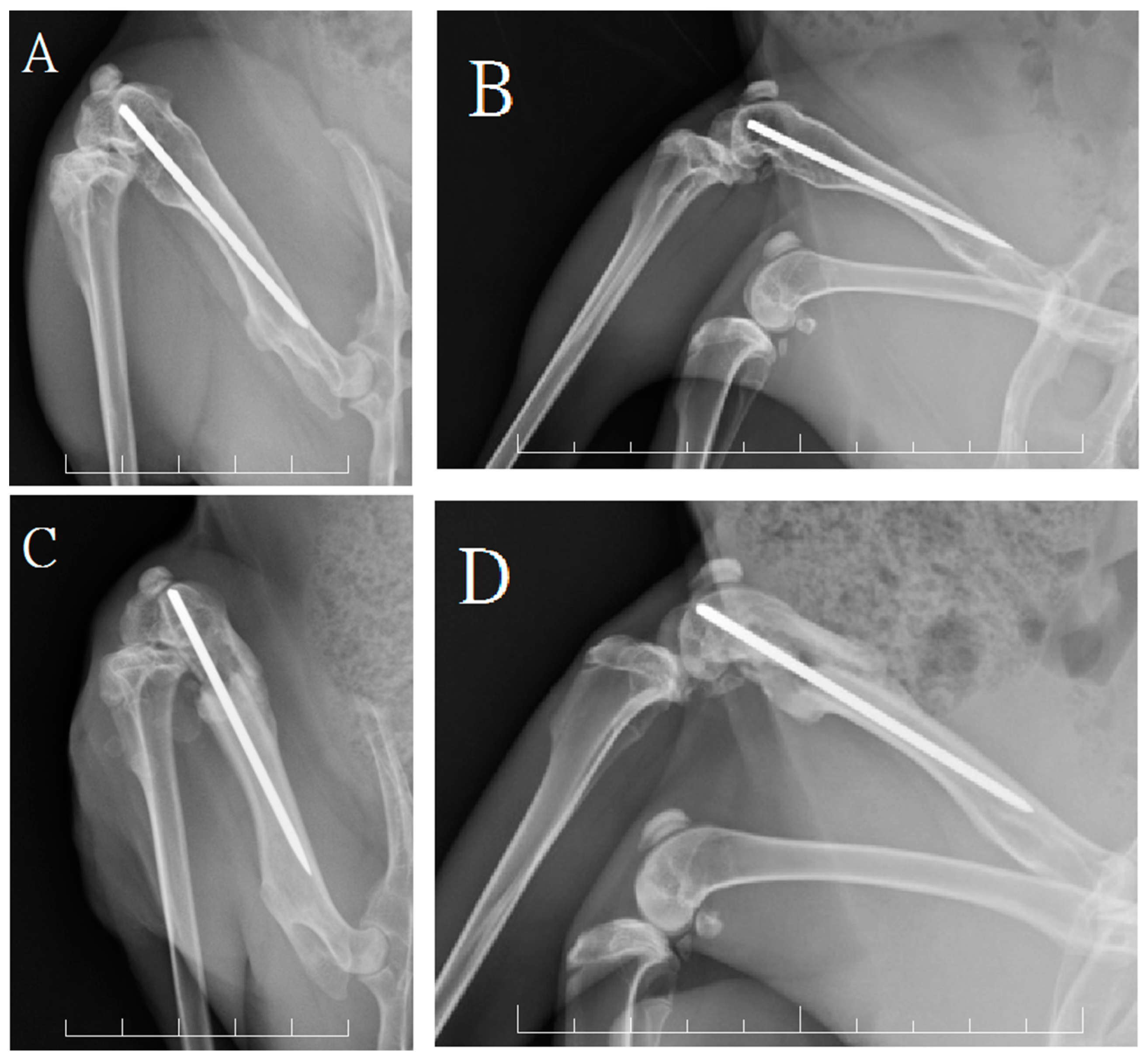
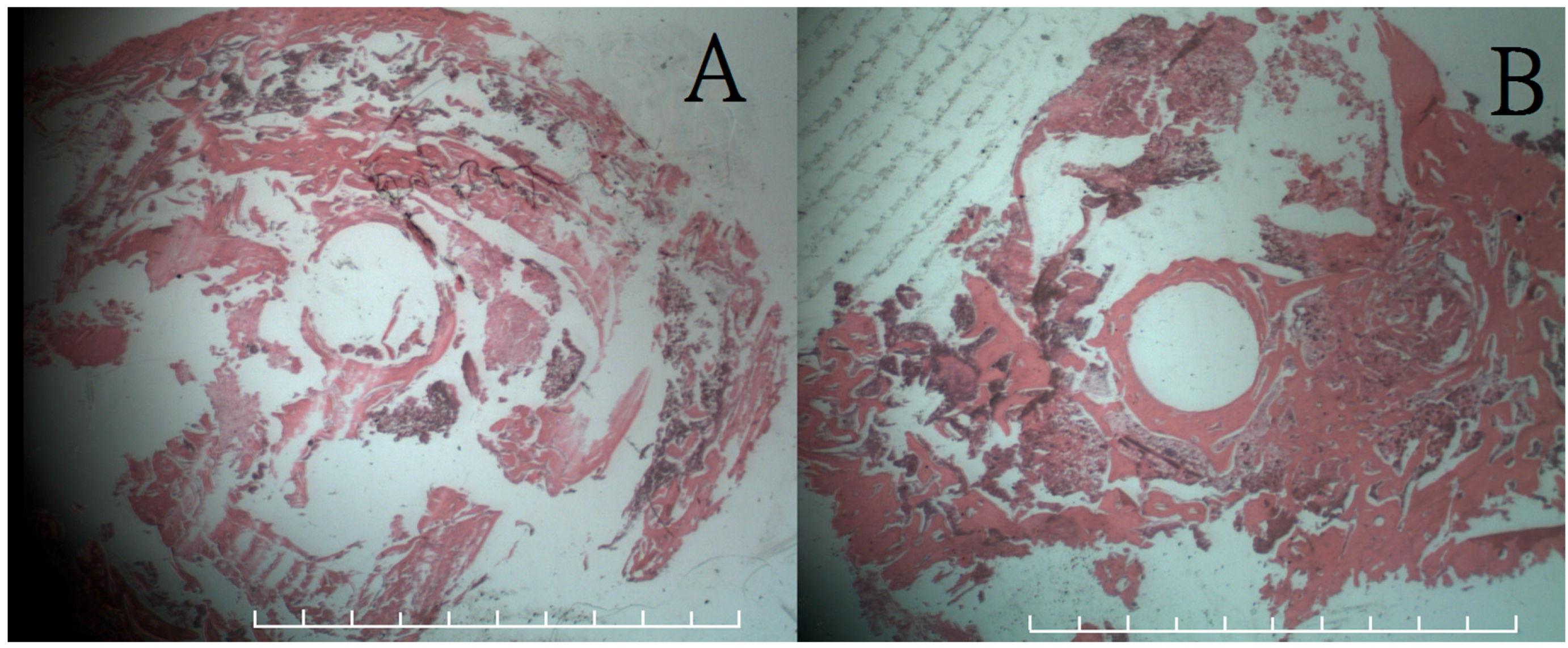
2.2. Radiographic and Histological Examination of Bone Healing
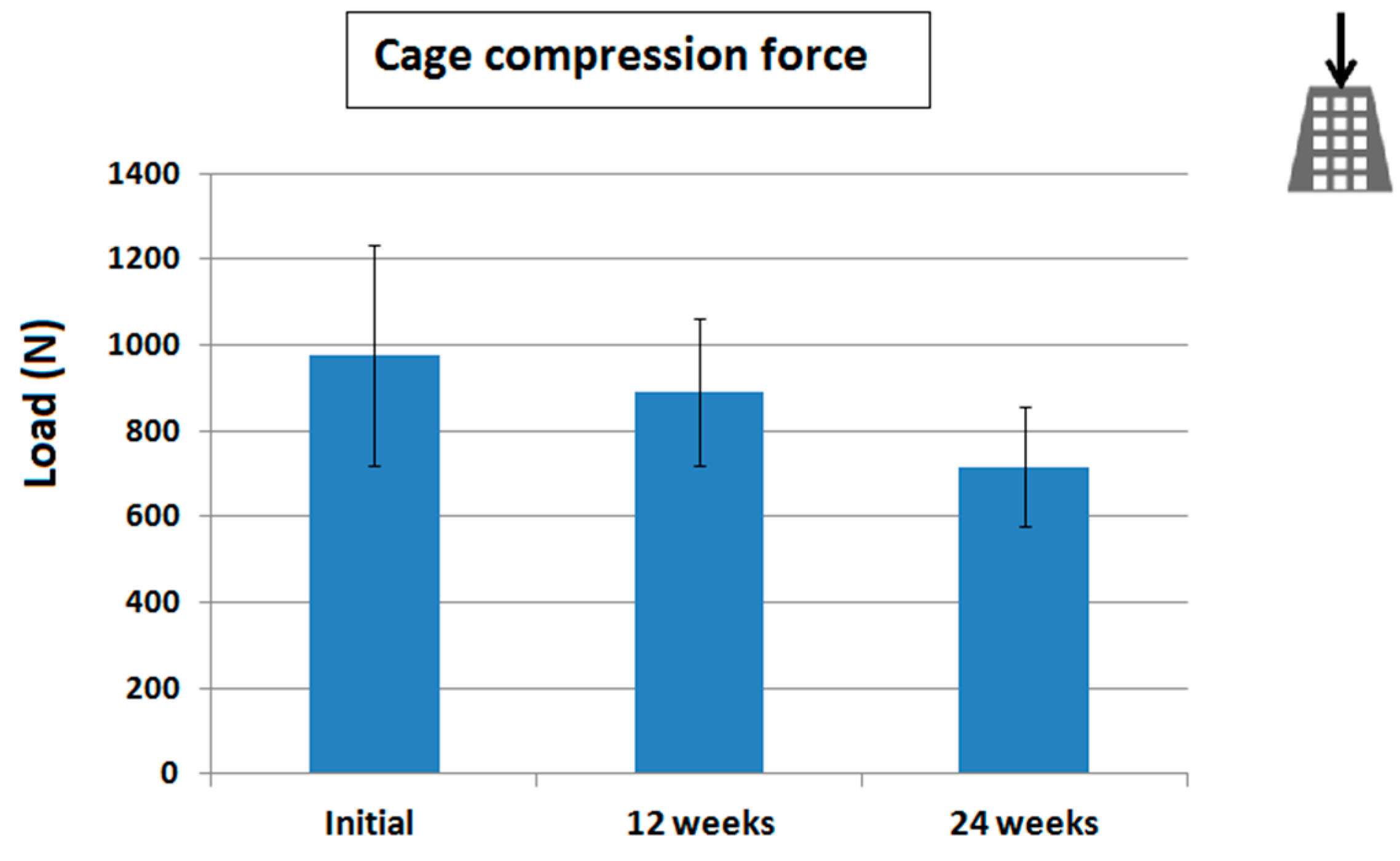
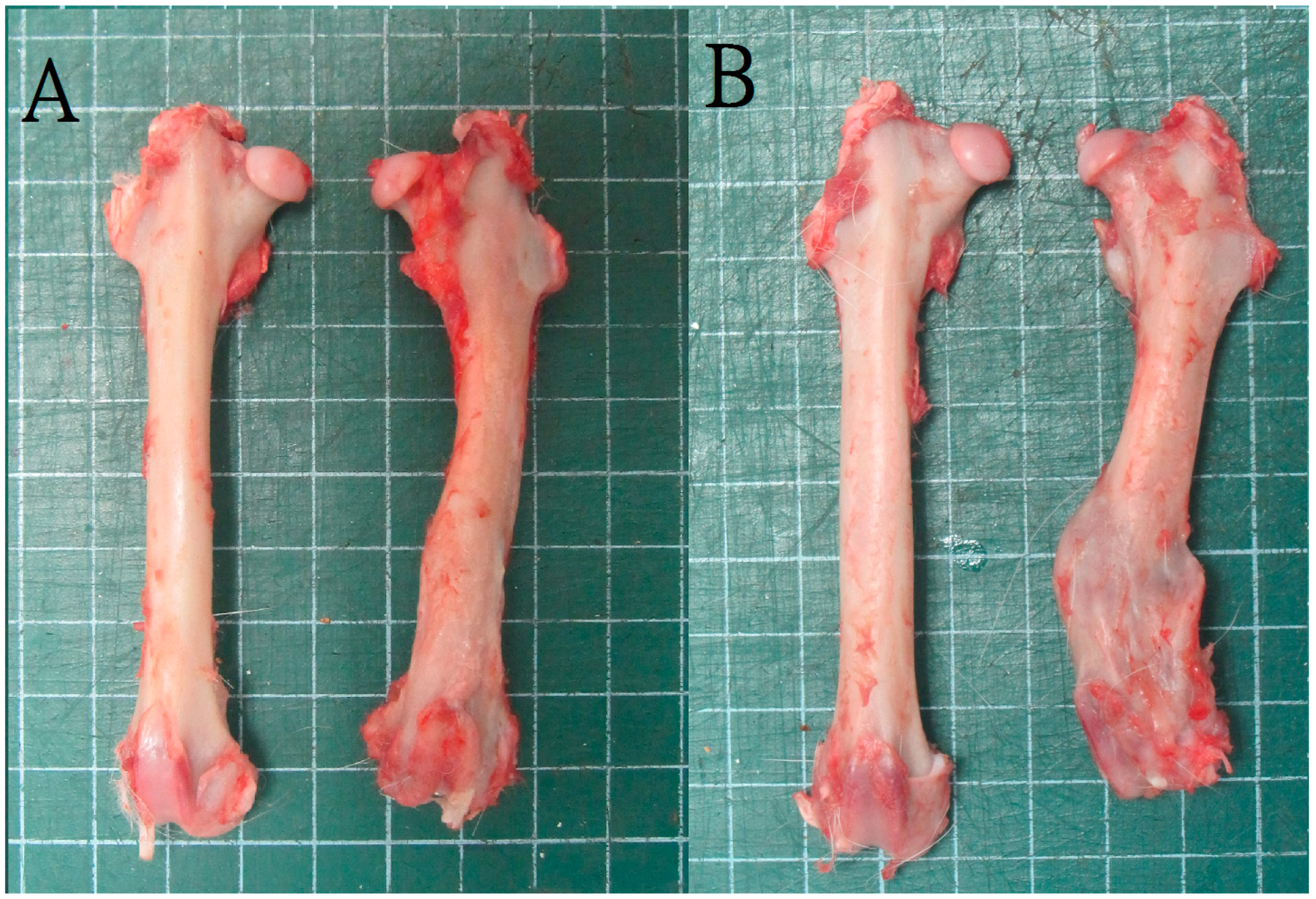
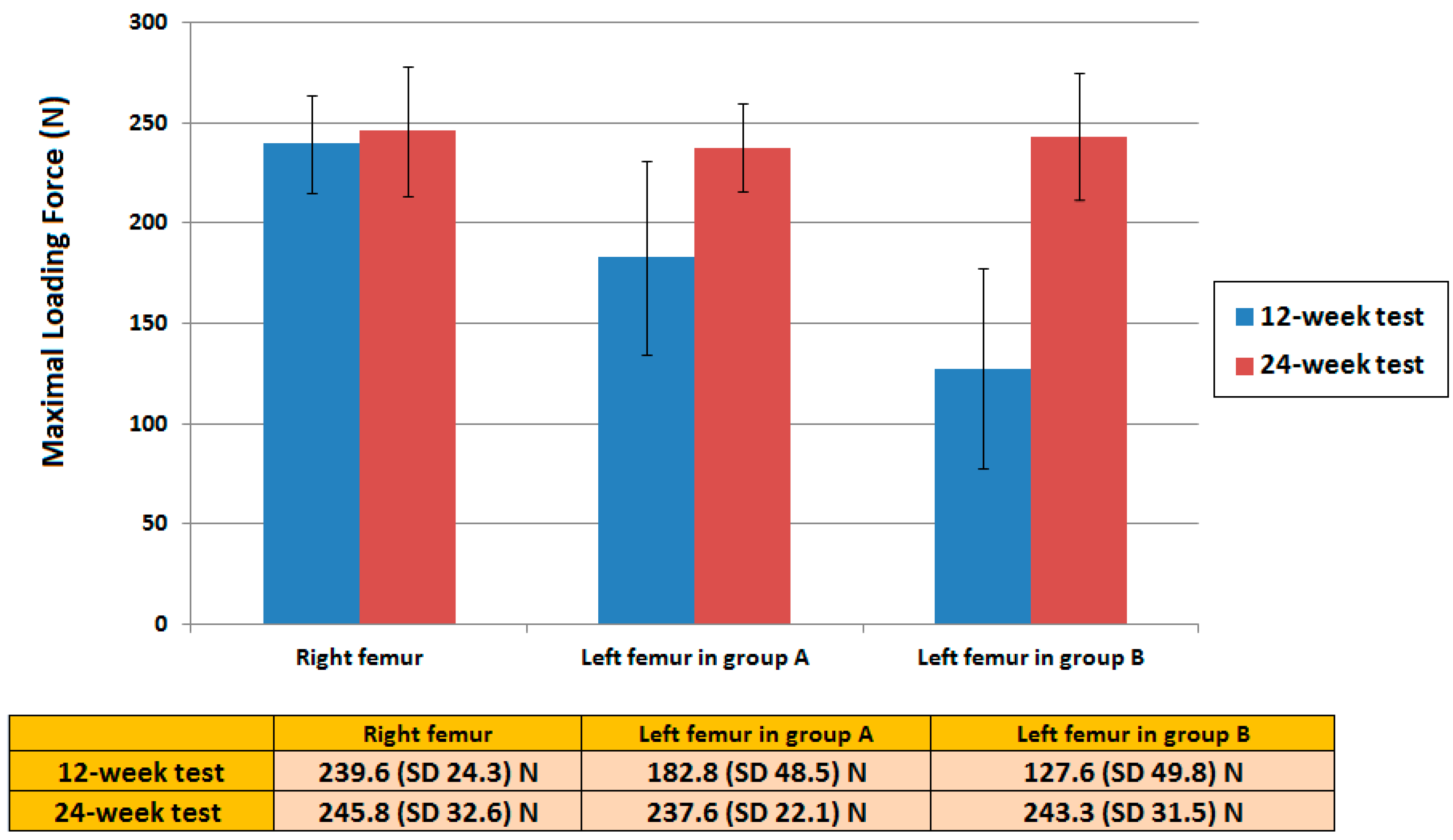
2.3. Leg Length and Mechanical Strength Test
3. Discussion
4. Experimental Section
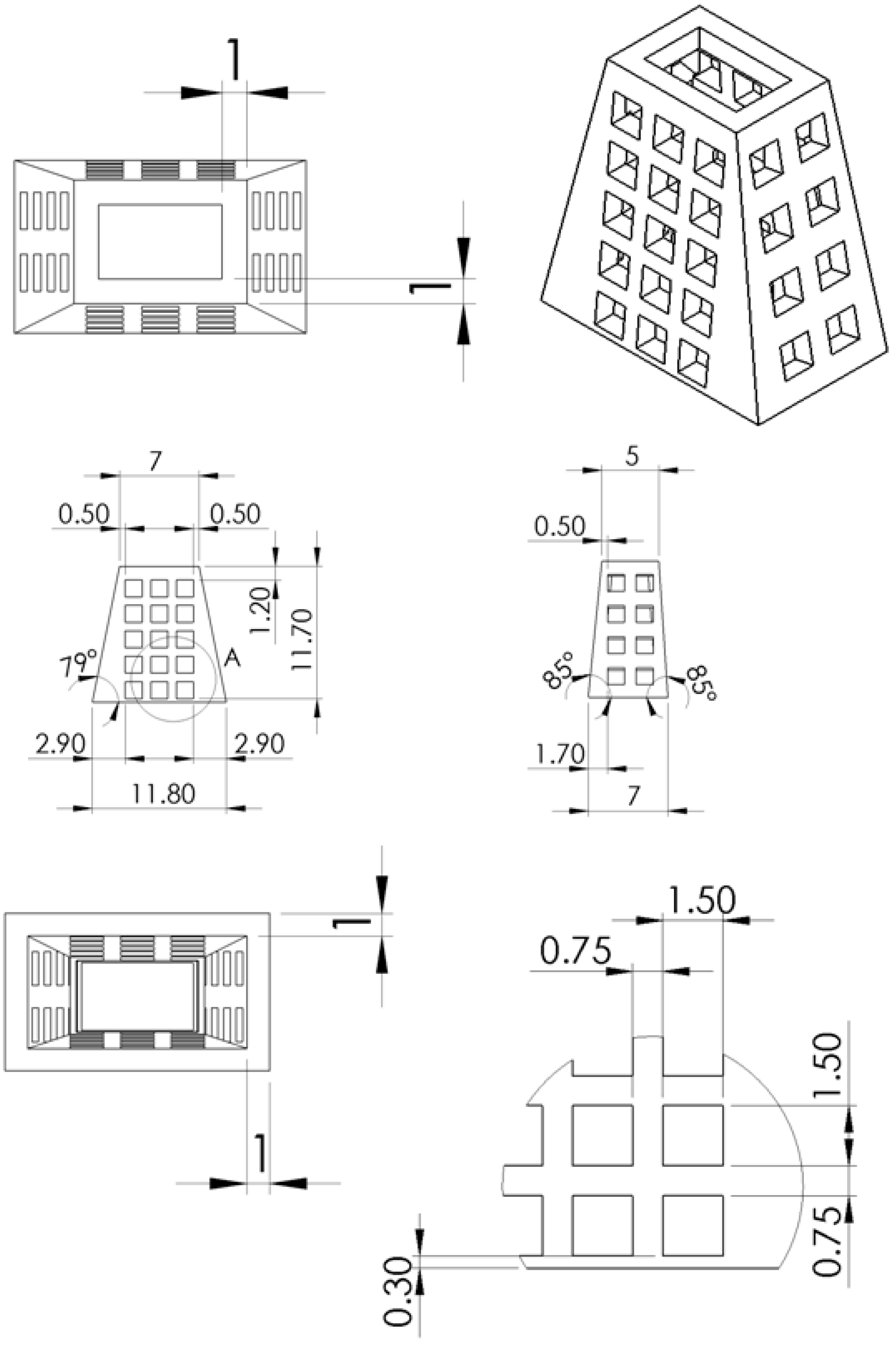
4.1. Biodegradable Bone Cages
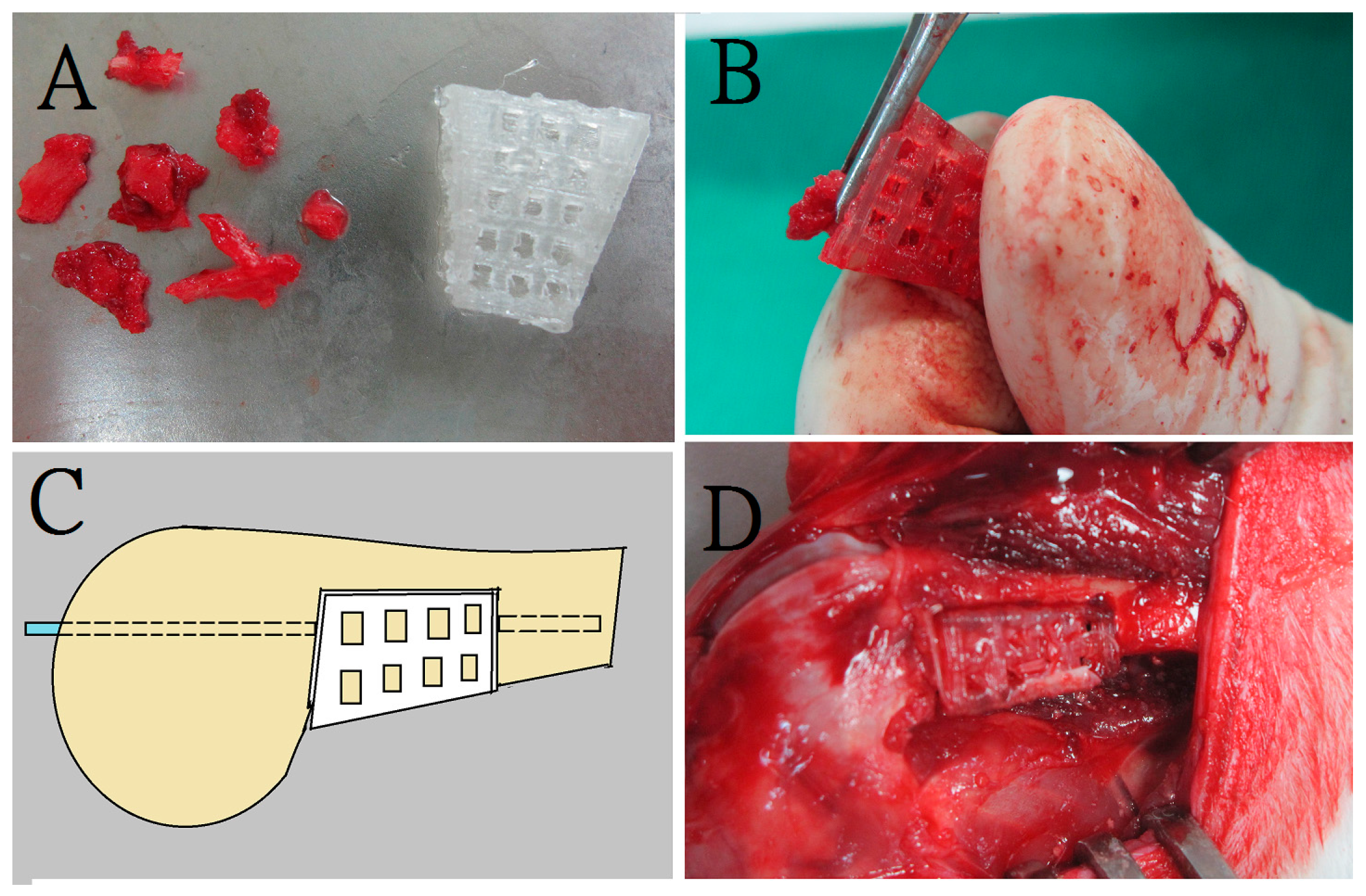
4.1.1. Fabrication of the Three-Dimensional (3D) Printed Bone Cage
4.1.2. Degradation and Mechanical Evaluation of the 3D Printed Cage
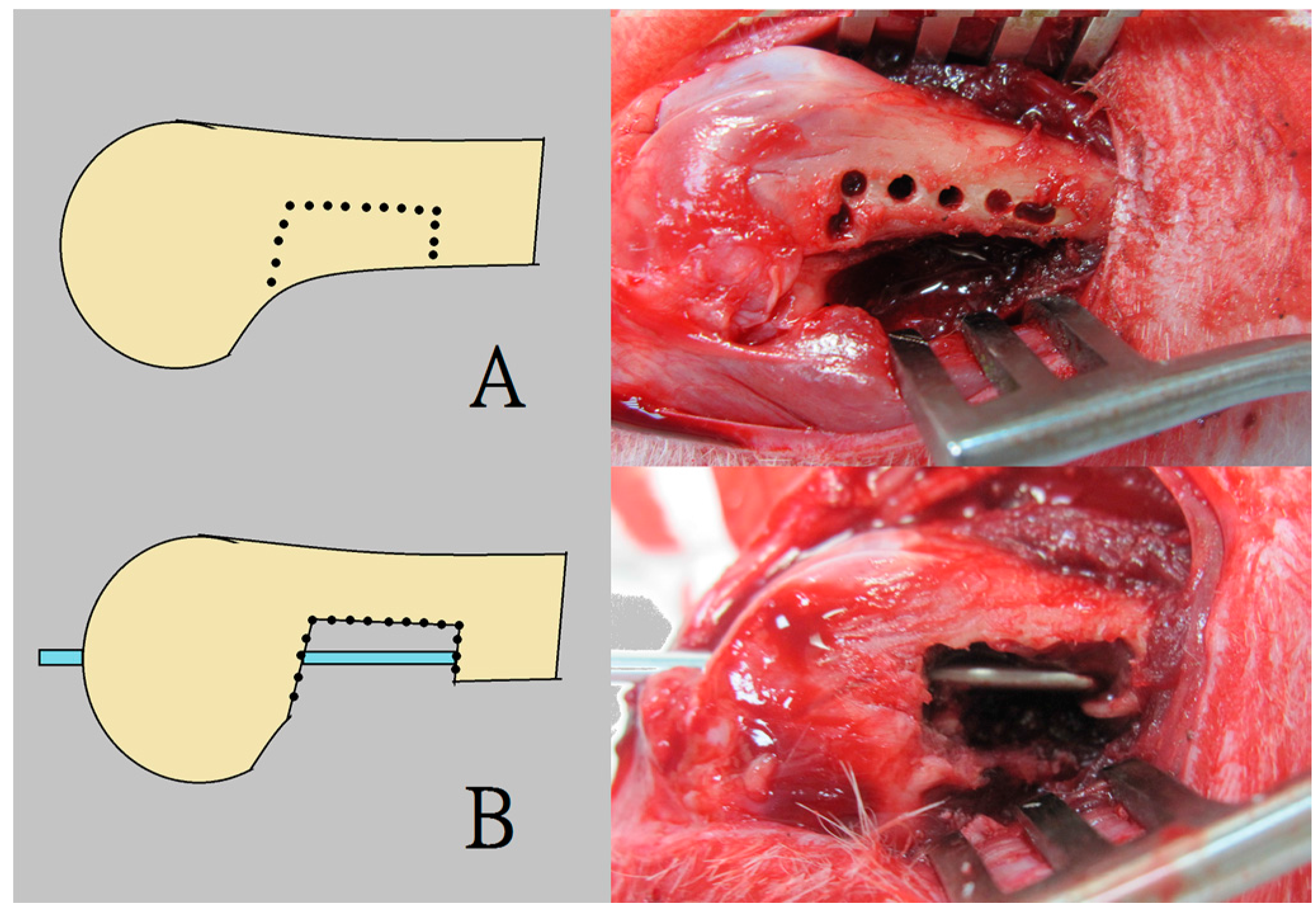
4.2. Surgical Procedure and Animal Care
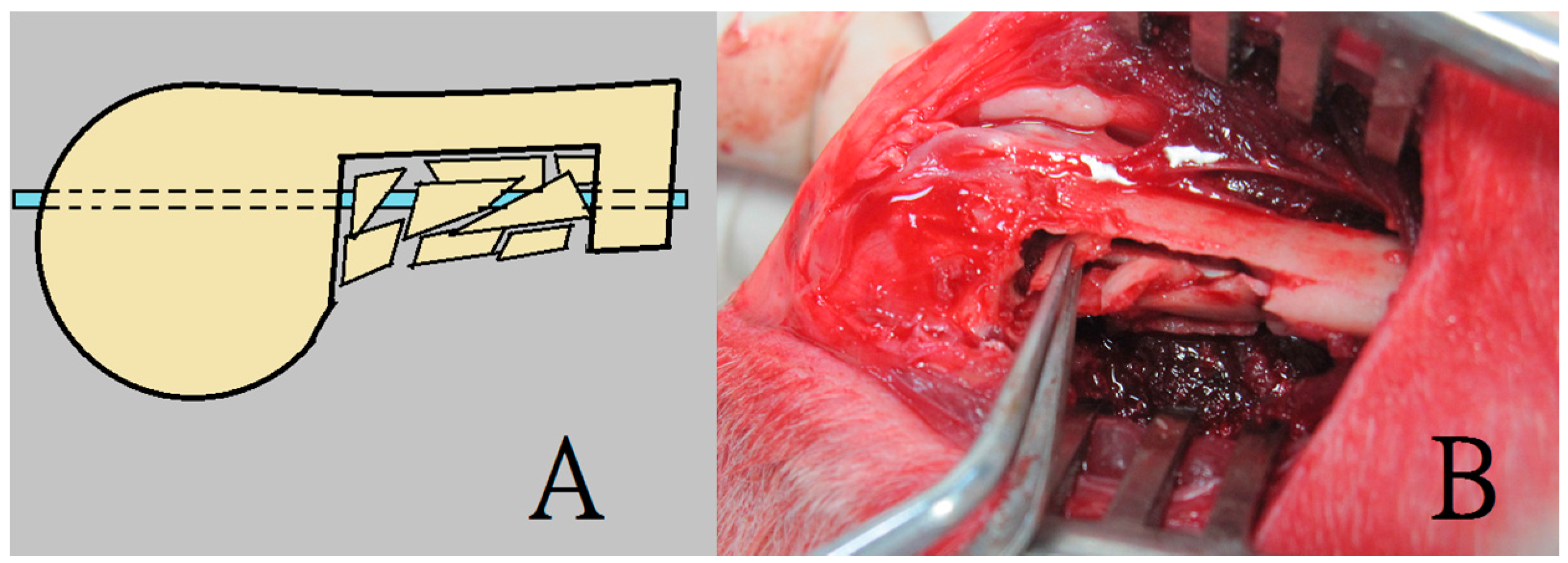
4.2.1. Surgical Procedure
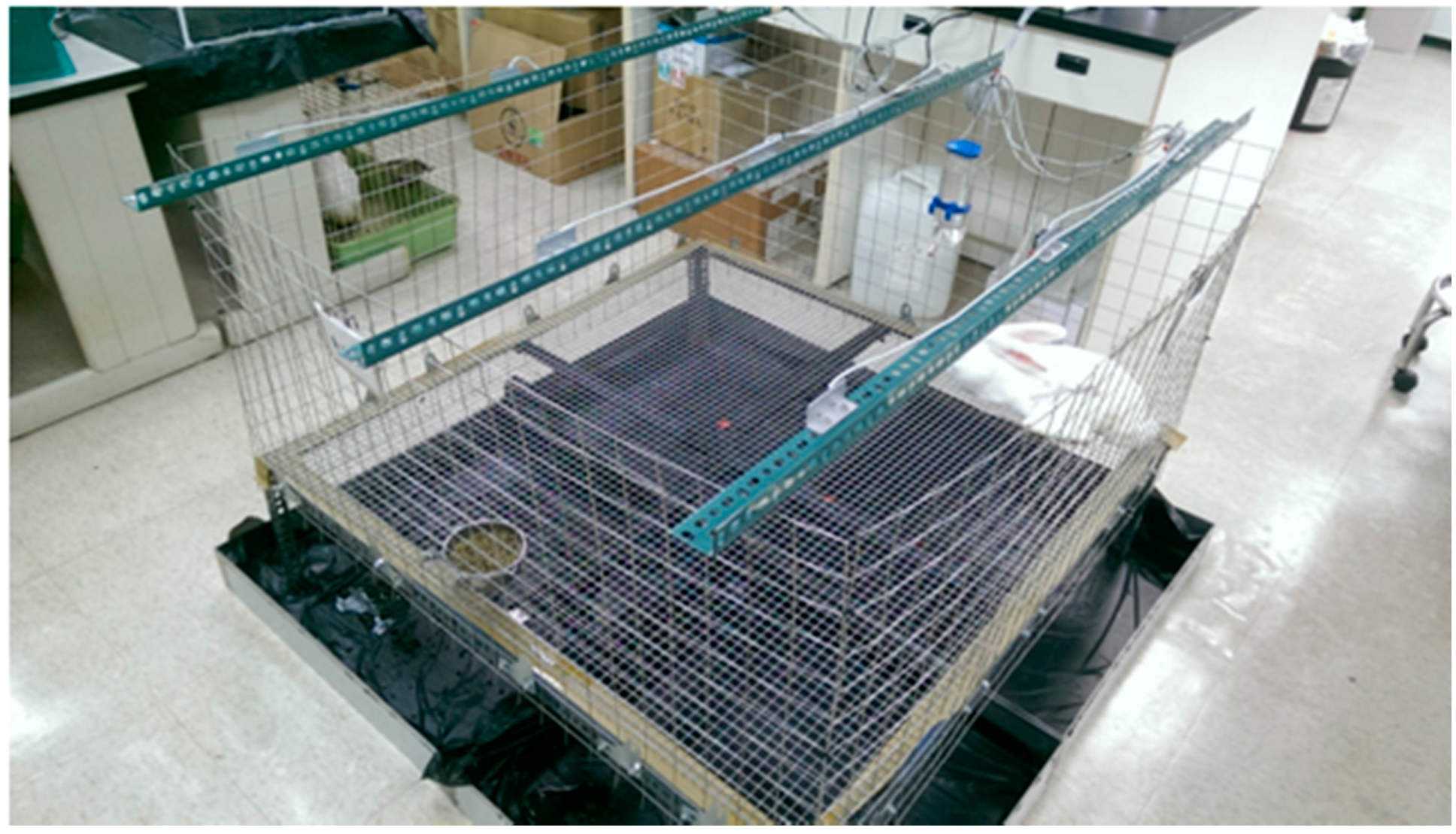
4.2.2. Postoperative Animal Care and Clinical Assessments
4.2.3. Animal Sacrifice and Mechanical Evaluation
4.3. Statistics and Data Analysis
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Koettstorfer, J.; Hofbauer, M.; Wozasek, G.E. Successful limb salvage using the two-staged technique with internal fixation after osteodistraction in an effort to treat large segmental bone defects in the lower extremity. Arch. Orthop. Trauma Surg. 2012, 132, 1399–1405. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Liu, G.H.; Wu, Q.; Yu, B. Repairing rabbit radial defects by combining bone marrow stroma stem cells with bone scaffold material comprising a core-cladding structure. Genet. Mol. Res. 2015, 14, 11933–11943. [Google Scholar] [CrossRef] [PubMed]
- Sporer, S.M.; O’Rourke, M.; Chong, P.; Paprosky, W.G. The use of structural distal femoral allografts for acetabular reconstruction. Surgical technique. J. Bone Jt. Surg. Am. 2006, 88, 92–99. [Google Scholar] [CrossRef] [PubMed]
- Glenn, R.E., Jr.; McCarty, E.C.; Potter, H.G.; Juliao, S.F.; Gordon, J.D.; Spindler, K.P. Comparison of fresh osteochondral autografts and allografts: A canine model. Am. J. Sports Med. 2006, 34, 1084–1093. [Google Scholar] [CrossRef] [PubMed]
- Tompkins, M.; Paller, D.J.; Moore, D.C.; Crisco, J.J.; Terek, R.M. Locking buttons increase fatigue life of locking plates in a segmental bone defect model. Clin. Orthop. Relat. Res. 2013, 471, 1039–1044. [Google Scholar] [CrossRef] [PubMed]
- Montijo, H.E.; Kellam, J.F.; Gettys, F.K.; Starman, J.S.; Nelson, M.K.; Bayoumi, E.M.; Bosse, M.J.; Gruber, H.E. Utilization of the AO LockingRatNail in a novel rat femur critical defect model. J. Investig. Surg. 2012, 25, 381–386. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Yang, K.H. Indications and outcomes of augmentation plating with decortication and autogenous bone grafting for femoral shaft nonunions. Injury 2013, 44, 1820–1825. [Google Scholar] [CrossRef] [PubMed]
- Ahearn, N.; Oppy, A.; Halliday, R.; Rowett-Harris, J.; Morris, S.A.; Chesser, T.J.; Livingstone, J.A. The outcome following fixation of bicondylar tibial plateau fractures. Bone Jt. J. 2014, 96, 956–962. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.R.; Halliday, R.; Aquilina, A.L.; Morrison, R.J.; Yip, G.C.; McArthur, J.; Hull, P.; Gray, A.; Kelly, M.B. Collaborative-Orthopaedic Trauma Society (OTS). Distal femoral fractures: The need to review the standard of care. Injury 2015, 46, 1084–1088. [Google Scholar] [CrossRef] [PubMed]
- Olerud, P.; Ahrengart, L.; Ponzer, S.; Saving, J.; Tidermark, J. Internal fixation versus nonoperative treatment of displaced 3-part proximal humeral fractures in elderly patients: A randomized controlled trial. J. Shoulder Elbow Surg. 2011, 20, 747–755. [Google Scholar] [CrossRef] [PubMed]
- Qu, H.; Guo, W.; Yang, R.; Tang, X.; Yan, T.; Li, D.; Yang, Y.; Zang, J. Cortical strut bone grafting and long-stem endoprosthetic reconstruction following massive bone tumor resection in the lower limb. Bone Jt. J. 2015, 97, 544–549. [Google Scholar] [CrossRef] [PubMed]
- Woiciechowsky, C.; Abbushi, A.; Zenclussen, M.L.; Casalis, P.; Krüger, J.P.; Freymann, U.; Endres, M.; Kaps, C. Regeneration of nucleus pulposus tissue in an ovine intervertebral disc degeneration model by cell-free resorbable polymer scaffolds. J. Tissue Eng. Regen. Med. 2014, 8, 811–820. [Google Scholar] [CrossRef] [PubMed]
- Kim, I.G.; Hwang, M.P.; Du, P.; Ko, J.; Ha, C.W.; Do, S.H.; Park, K. Bioactive cell-derived matrices combined with polymer mesh scaffold for osteogenesis and bone healing. Biomaterials 2015, 50, 75–86. [Google Scholar] [CrossRef] [PubMed]
- Zhou, R.; Xu, W.; Chen, F.; Qi, C.; Lu, B.Q.; Zhang, H.; Wu, J.; Qian, Q.R.; Zhu, Y.J. Amorphous calcium phosphate nanospheres/polylactide composite coated tantalum scaffold: Facile preparation, fast biomineralization, and subchondral bone defect repair application. Colloids Surf. B Biointerfaces 2014, 123, 236–245. [Google Scholar] [CrossRef] [PubMed]
- Naito, Y.; Terukina, T.; Galli, S.; Kozai, Y.; Vandeweghe, S.; Tagami, T.; Ozeki, T.; Ichikawa, T.; Coelho, P.G.; Jimbo, R. The effect of simvastatin-loaded polymeric microspheres in a critical size bone defect in the rabbit calvaria. Int. J. Pharm. 2014, 461, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Serra, T.; Ortiz-Hernandez, M.; Engel, E.; Planell, J.A.; Navarro, M. Relevance of PEG in PLA-based blends for tissue engineering 3D-printed scaffolds. Mater. Sci. Eng. C Mater. Biol. Appl. 2014, 38, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Mohanty, S.; Larsen, L.B.; Trifol, J.; Szabo, P.; Burri, H.V.; Canali, C.; Dufva, M.; Emnéus, J.; Wolff, A. Fabrication of scalable and structured tissue engineering scaffolds using water dissolvable sacrificial 3D printed moulds. Mater. Sci. Eng. C Mater. Biol. Appl. 2015, 55, 569–578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castro, N.J.; Patel, R.; Zhang, L.G. Design of a novel 3D printed bioactive nanocomposite scaffold for improved osteochondral regeneration. Cell. Mol. Bioeng. 2015, 8, 416–432. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Yang, M.; Zhu, Y.; Wang, L.; Tomsia, A.P.; Mao, C. Phage nanofibers induce vascularized osteogenesis in 3D printed bone scaffolds. Adv. Mater. 2014, 26, 4961–4966. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.S.; Lee, H.K.; Jeong, H.S.; Shin, H.W. Decreased postoperative pain after reduction of fractured nasal bones using a nerve block of the anterior ethmoidal nerve. Int. J. Oral Maxillofac. Surg. 2013, 42, 727–731. [Google Scholar] [CrossRef] [PubMed]
- Bateman, E.; Donald, S.M. Reconstruction of massive uncontained glenoid defects using a combined autograft-allograft construct with reverse shoulder arthroplasty: Preliminary results. J. Shoulder Elbow Surg. 2012, 21, 925–934. [Google Scholar] [CrossRef] [PubMed]
- Clements, J.R. Use of allograft cellular bone matrix in multistage talectomy with tibiocalcaneal arthrodesis: A case report. J. Foot Ankle Surg. 2012, 51, 83–86. [Google Scholar] [CrossRef] [PubMed]
- Angthong, C.; Chernchujit, B.; Apivatgaroon, A.; Chaijenkit, K.; Nualon, P.; Suchao-in, K. The anterior cligament reconstruction with the peroneus longus tendon: A biomechanical and clinical evaluation of the donor ankle morbidity. J. Med. Assoc. Thai. 2015, 98, 555–560. [Google Scholar] [PubMed]
- McDonald, E.; Chu, T.; Tufaga, M.; Marmor, M.; Singh, R.; Yetkinler, D.; Matityahu, A.; Buckley, J.M.; McClellan, R.T. Tibial plateau fracture repairs augmented with calcium phosphate cement have higher in situ fatigue strength than those with autograft. J. Orthop. Trauma 2011, 25, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Berkes, M.B.; Little, M.T.; Lazaro, L.E.; Cymerman, R.M.; Pardee, N.C.; Helfet, D.L.; Dines, J.S.; Lorich, D.G. Intramedullary allograft fibula as a reduction and fixation tool for treatment of complex proximal humerus fractures with diaphyseal extension. J. Orthop. Trauma 2014, 28, e56–e64. [Google Scholar] [CrossRef] [PubMed]
- Tan, E.; Lie, D.; Wong, M.K. Early outcomes of proximal humerus fracture fixation with locking plate and intramedullary fibular strut graft. Orthopedics 2014, 37, e822–e827. [Google Scholar] [CrossRef] [PubMed]
- Khashan, M.; Amar, E.; Drexler, M.; Chechik, O.; Cohen, Z.; Steinberg, E.L. Superior outcome of strut allograft-augmented plate fixation for the treatment of periprosthetic fractures around a stable femoral stem. Injury 2013, 44, 1556–1560. [Google Scholar] [CrossRef] [PubMed]
- Gras, M.; Mathoulin, C. Vascularized bone graft pedicled on the volar carpal artery from the volar distal radius as primary procedure for scaphoid non-union. Orthop. Traumatol. Surg. Res. 2011, 97, 800–806. [Google Scholar] [CrossRef] [PubMed]
- Takahata, M.; Schwarz, E.M.; Chen, T.; O’Keefe, R.J.; Awad, H.A. Delayed short-course treatment with teriparatide (PTH(1-34)) improves femoral allograft healing by enhancing intramembranous bone formation at the graft-host junction. J. Bone Miner. Res. 2012, 27, 26–37. [Google Scholar] [CrossRef] [PubMed]
- De Santis, R.; Russo, A.; Gloria, A.; D’Amora, U.; Russo, T.; Panseri, S.; Sandri, M.; Tampieri, A.; Marcacci, M.; Dediu, V.A.; et al. Towards the design of 3D fiber-deposited poly(ε-caprolactone)/iron-doped hydroxyapatite nanocomposite magnetic scaffolds for bone regeneration. J. Biomed. Nanotechnol. 2015, 11, 1236–1246. [Google Scholar] [CrossRef] [PubMed]
- Goffin, A.L.; Raquez, J.M.; Duquesne, E.; Siqueira, G.; Habibi, Y.; Dufresne, A.; Dubois, P. From interfacial ring-opening polymerization to melt processing of cellulose nanowhisker-filled polylactide-based nanocomposites. Biomacromolecules 2011, 12, 2456–2465. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Yang, F.; He, F.; Tian, X.; Tang, S.; Chen, X. A tubular gelatin scaffold capable of the time-dependent controlled release of epidermal growth factor and mitomycin C. Colloids Surf. B Biointerfaces 2015, 135, 416–424. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Li, J.; Liu, F.; Feng, L.; Yu, D.; Zhang, N. Theranostic polymeric micelles for the diagnosis and treatment of hepatocellular carcinoma. J. Biomed. Nanotechnol. 2015, 11, 613–622. [Google Scholar] [CrossRef] [PubMed]
- Tsiolis, P.; Giamarellos-Bourboulis, E.J.; Mavrogenis, A.F.; Savvidou, O.; Lallos, S.N.; Frangia, K.; Lazarettos, I.; Nikolaou, V.; Efstathopoulos, N.E. Experimental osteomyelitis caused by methicillin-resistant Staphylococcus aureus treated with a polylactide carrier releasing linezolid. Surg. Infect. (Larchmt). 2011, 12, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Pinczewski, L.A.; Lyman, J.; Salmon, L.J.; Russell, V.J.; Roe, J.; Linklater, J. A 10-year comparison of anterior cruciate ligament reconstructions with hamstring tendon and patellar tendon autograft: A controlled, prospective trial. Am. J. Sports Med. 2007, 35, 564–574. [Google Scholar] [CrossRef] [PubMed]












© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chou, Y.-C.; Lee, D.; Chang, T.-M.; Hsu, Y.-H.; Yu, Y.-H.; Liu, S.-J.; Ueng, S.W.-N. Development of a Three-Dimensional (3D) Printed Biodegradable Cage to Convert Morselized Corticocancellous Bone Chips into a Structured Cortical Bone Graft. Int. J. Mol. Sci. 2016, 17, 595. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms17040595
Chou Y-C, Lee D, Chang T-M, Hsu Y-H, Yu Y-H, Liu S-J, Ueng SW-N. Development of a Three-Dimensional (3D) Printed Biodegradable Cage to Convert Morselized Corticocancellous Bone Chips into a Structured Cortical Bone Graft. International Journal of Molecular Sciences. 2016; 17(4):595. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms17040595
Chicago/Turabian StyleChou, Ying-Chao, Demei Lee, Tzu-Min Chang, Yung-Heng Hsu, Yi-Hsun Yu, Shih-Jung Liu, and Steve Wen-Neng Ueng. 2016. "Development of a Three-Dimensional (3D) Printed Biodegradable Cage to Convert Morselized Corticocancellous Bone Chips into a Structured Cortical Bone Graft" International Journal of Molecular Sciences 17, no. 4: 595. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms17040595