Mismatch-Repair Protein Expression in High-Grade Gliomas: A Large Retrospective Multicenter Study

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
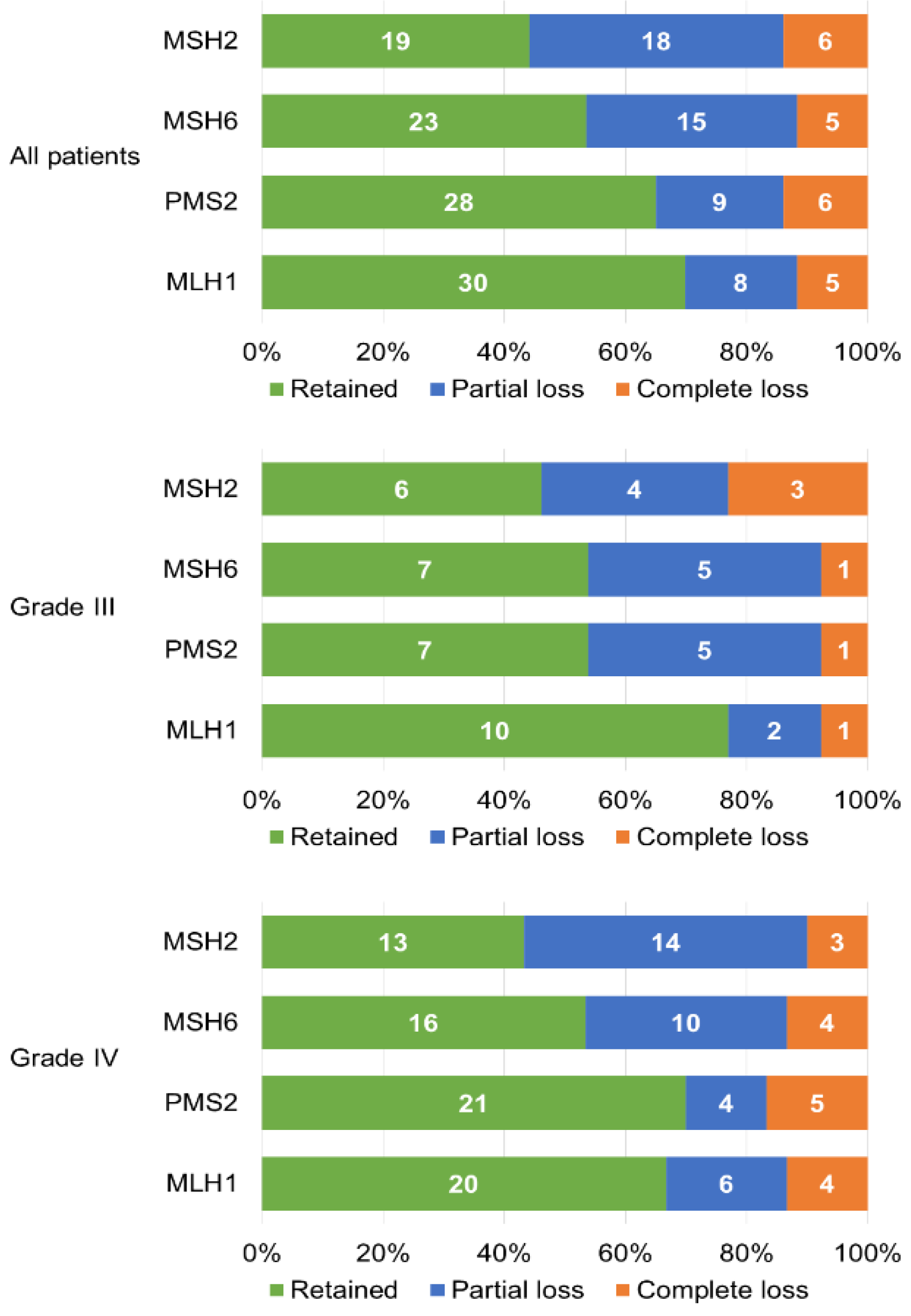
2.2. Mismatch Repair Status
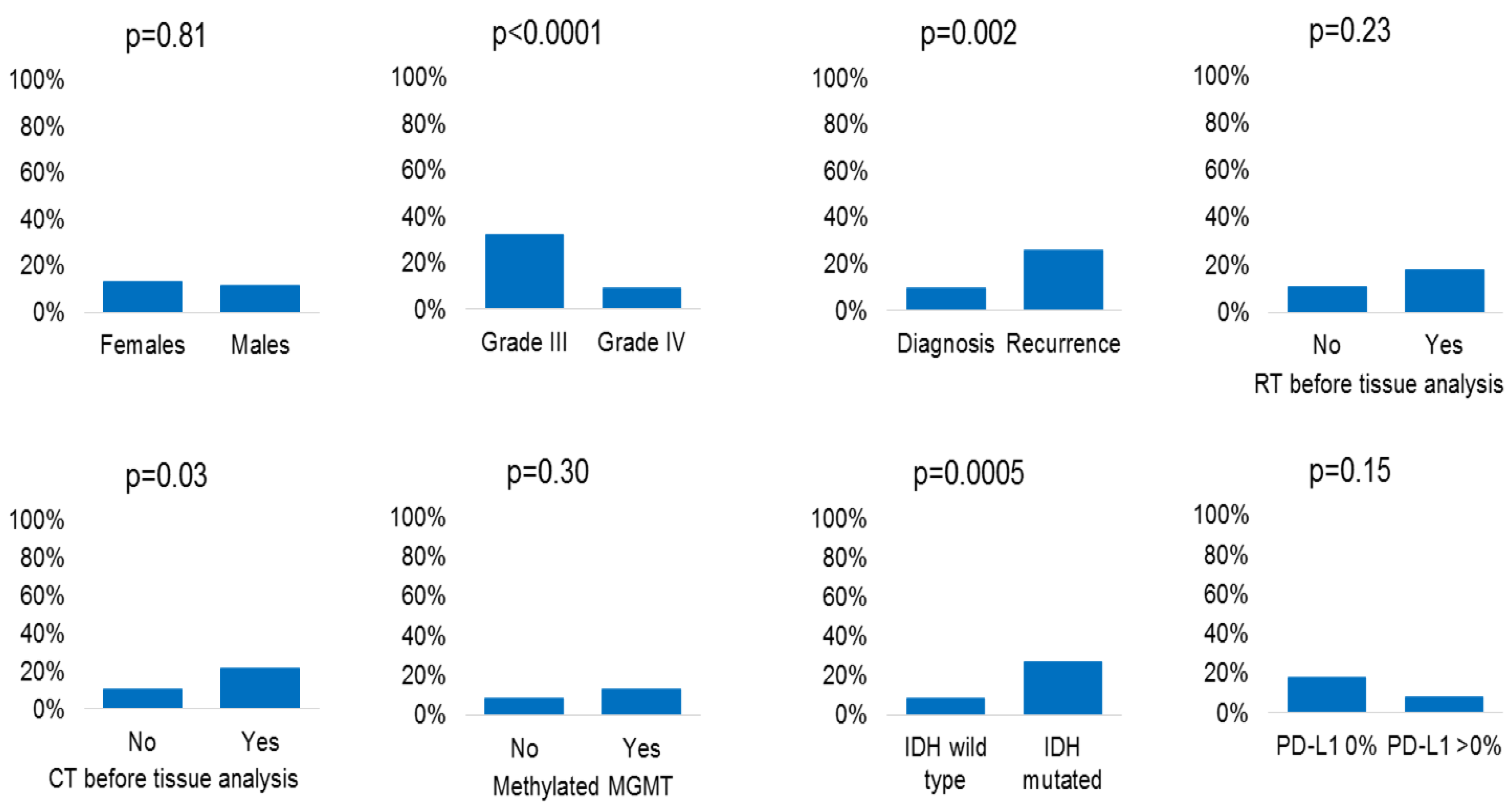
2.3. Mismatch Repair Deficiency and Clinical/Molecular Characteristics
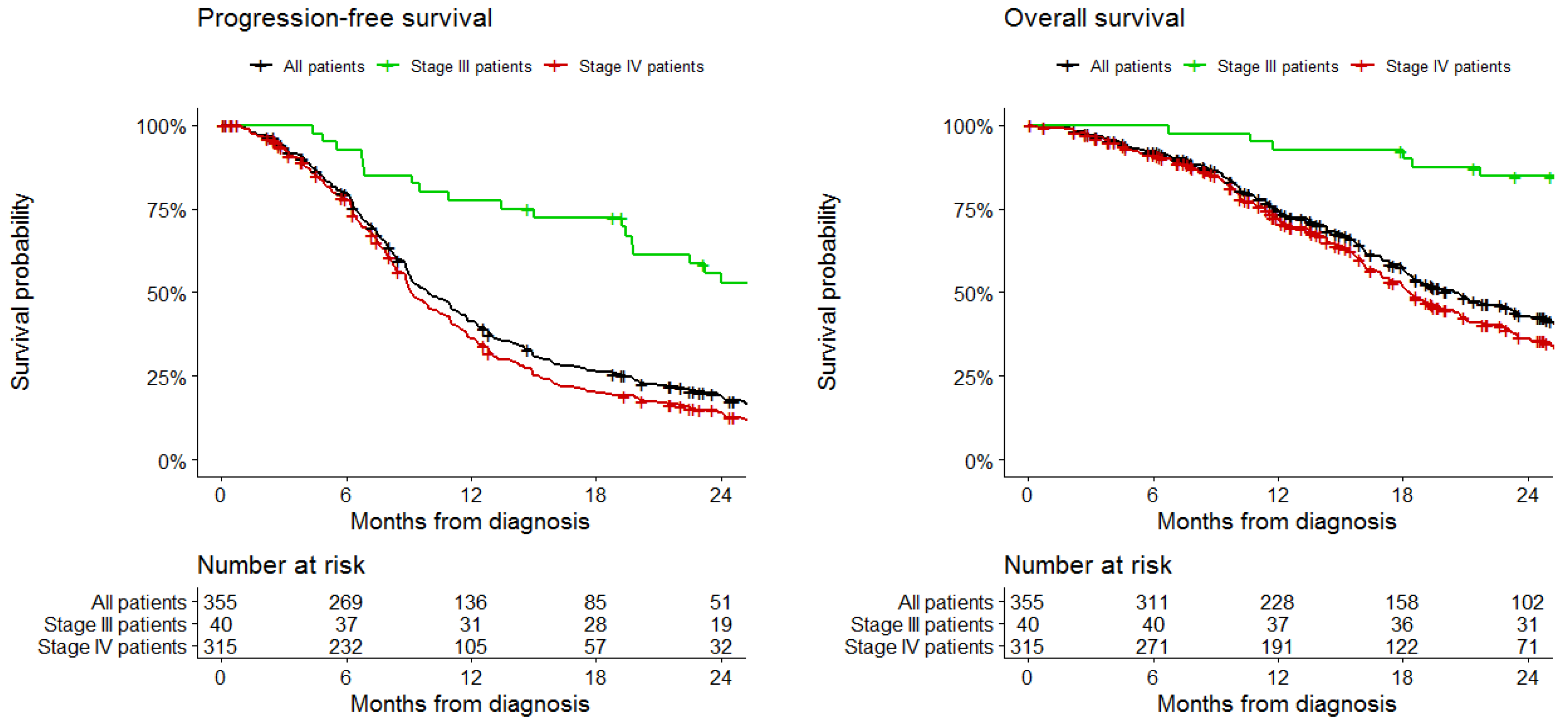
2.4. Loss of Mismatch Repair Proteins and Survival
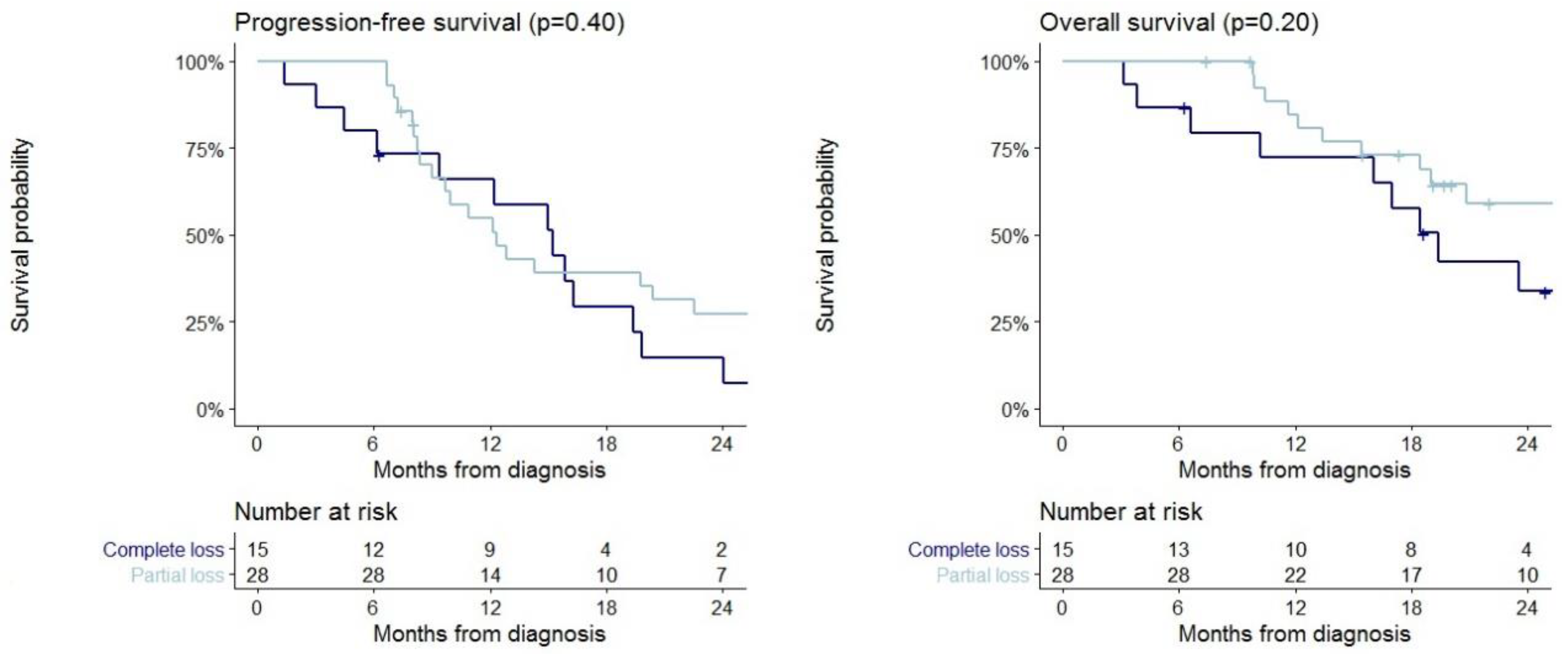
2.5. Survival in Patients with Immunohistochemical Loss of MMR Proteins Expression
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Patients
4.3. Procedures
4.4. Data Collection
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Louis, D.N.; Perry, A.; Reifenberger, G.; von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W.; et al. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dolcetti, R.; Viel, A.; Doglioni, C.; Russo, A.; Guidoboni, M.; Capozzi, E.; Vecchiato, N.; Macri, E.; Fornasarig, M.; Boiocchi, M.; et al. High prevalence of activated intraepithelial cytotoxic T lymphocytes and increased neoplastic cell apoptosis in colorectal carcinomas with microsatellite instability. Am. J. Pathol. 1999, 154, 1805–1813. [Google Scholar] [CrossRef] [Green Version]
- Hodges, T.R.; Ott, M.; Xiu, J.; Gatalica, Z.; Swensen, J.; Zhou, S.; Huse, J.T.; de Groot, J.; Li, S.; Overwijk, W.W.; et al. Mutational burden, immune checkpoint expression, and mismatch repair in glioma: Implications for immune checkpoint immunotherapy. Neuro-Oncology 2017, 19, 1047–1057. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Indraccolo, S.; Lombardi, G.; Fassan, M.; Pasqualini, L.; Giunco, S.; Marcato, R.; Gasparini, A.; Candiotto, C.; Nalio, S.; Fiduccia, P.; et al. Genetic, Epigenetic, and Immunologic Profiling of MMR-Deficient Relapsed Glioblastoma. Clin. Cancer Res. 2019, 25, 1828–1837. [Google Scholar] [CrossRef] [PubMed]
- Barresi, V.; Simbolo, M.; Mafficini, A.; Piredda, M.L.; Caffo, M.; Cardali, S.M.; Germanò, A.; Cingarlini, S.; Ghimenton, C.; Scarpa, A.; et al. Ultra-Mutation in IDH Wild-Type Glioblastomas of Patients Younger than 55 Years is Associated with Defective Mismatch Repair, Microsatellite Instability, and Giant Cell Enrichment. Cancers 2019, 11, 1279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCord, M.; Steffens, A.; Javier, R.; Kam, K.L.; McCortney, K.; Horbinski, C. The efficacy of DNA mismatch repair enzyme immunohistochemistry as a screening test for hypermutated gliomas. Acta Neuropathol. Commun. 2020, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Le, D.T.; Durham, J.N.; Smith, K.N.; Wang, H.; Bartlett, B.R.; Aulakh, L.K.; Lu, S.; Kemberling, H.; Wilt, C.; Luber, B.S.; et al. Mismatch repair deficiency predicts response of solid tumors to PD-1 blockade. Science 2017, 357, 409–413. [Google Scholar] [CrossRef] [Green Version]
- Azad, N.S.; Gray, R.J.; Overman, M.J.; Schoenfeld, J.D.; Mitchell, E.P.; Zwiebel, J.A.; Sharon, E.; Streicher, H.; Li, S.; McShane, L.M.; et al. Nivolumab Is Effective in Mismatch Repair–Deficient Noncolorectal Cancers: Results from Arm Z1D—A Subprotocol of the NCI-MATCH (EAY131) Study. J. Clin. Oncol. 2020, 38, 214–222. [Google Scholar] [CrossRef]
- Marabelle, A.; Le, D.T.; Ascierto, P.A.; di Giacomo, A.M.; de Jesus-Acosta, A.; Delord, J.; Geva, R.; Gottfried, M.; Penel, N.; Hansen, A.R.; et al. Efficacy of Pembrolizumab in Patients with Noncolorectal High Microsatellite Instability/Mismatch Repair-Deficient Cancer: Results from the Phase II KEYNOTE-158 Study. J. Clin. Oncol. 2020, 38, 1–10. [Google Scholar] [CrossRef]
- Le, D.T.; Uram, J.N.; Wang, H.; Bartlett, B.R.; Kemberling, H.; Eyring, A.D.; Skora, A.D.; Luber, B.S.; Azad, N.S.; Laheru, D.; et al. PD-1 Blockade in Tumors with Mismatch-Repair Deficiency. N. Engl. J. Med. 2015, 372, 2509–2520. [Google Scholar] [CrossRef]
- Overman, M.J.; Lonardi, S.; Wong, K.Y.M.; Lenz, H.; Gelsomino, F.; Aglietta, M.; Morse, M.A.; van Cutsem, E.; McDermott, R.; Hill, A.; et al. Durable Clinical Benefit with Nivolumab Plus Ipilimumab in DNA Mismatch Repair–Deficient/Microsatellite Instability–High Metastatic Colorectal Cancer. J. Clin. Oncol. 2018, 36, 773–779. [Google Scholar] [CrossRef] [PubMed]
- Andre, T.; Shiu, K.-K.; Kim, T.W.; Jensen, B.V.; Jensen, L.H.; Punt, C.J.A.; Smith, D.M.; Garcia-Carbonero, R.; Benavides, M.; Gibbs, P.; et al. Pembrolizumab versus chemotherapy for microsatellite instability-high/mismatch repair deficient metastatic colorectal cancer: The phase 3 KEYNOTE-177 Study. J. Clin. Oncol. 2020, 38 (Suppl. 18), LBA4. [Google Scholar] [CrossRef]
- Lemery, S.; Keegan, P.; Pazdur, R. First FDA Approval Agnostic of Cancer Site—When a Biomarker Defines the Indication. N. Engl. J. Med. 2017, 377, 1409–1412. [Google Scholar] [CrossRef] [PubMed]
- Reardon, D.A.; Brandes, A.A.; Omuro, A.; Mulholland, P.; Lim, M.; Wick, A.; Baehring, J.; Ahluwalia, M.S.; Roth, P.; Bähr, O.; et al. Effect of Nivolumab vs Bevacizumab in Patients with Recurrent Glioblastoma: The CheckMate 143 Phase 3 Randomized Clinical Trial. JAMA Oncol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Reardon, D.A.; Kim, T.M.; Frenel, J.S.; Santoro, A.; Lopez, J.; Subramaniam, D.S.; Siu, L.L.; Rodon, J.; Tamura, K.; Saraf, S.; et al. Results of the phase IB KEYNOTE-028 multi-cohort trial of pembrolizumab monotherapy in patients with recurrent PD-L1-positive glioblastoma multiforme (GBM). Neuro-Oncology 2016. [Google Scholar] [CrossRef]
- Stark, A.M.; Doukas, A.; Hugo, H.H.; Mehdorn, H.M. The expression of mismatch repair proteins MLH1, MSH2 and MSH6 correlates with the Ki67 proliferation index and survival in patients with recurrent glioblastoma. Neurol. Res. 2010, 32, 816–820. [Google Scholar] [CrossRef]
- Cahill, D.P.; Levine, K.K.; Betensky, R.A.; Codd, P.J.; Romany, C.A.; Reavie, L.B.; Batchelor, T.T.; Futreal, P.A.; Stratton, M.R.; Curry, W.T.; et al. Loss of the mismatch repair protein MSH6 in human glioblastomas is associated with tumor progression during temozolomide treatment. Clin. Cancer Res. 2007, 13, 2038–2045. [Google Scholar] [CrossRef] [Green Version]
- Yip, S.; Miao, J.; Cahill, D.P.; Iafrate, A.J.; Aldape, K.; Nutt, C.L.; Louis, D.N. MSH6 mutations arise in glioblastomas during temozolomide therapy and mediate temozolomide resistance. Clin. Cancer Res. 2009, 15, 4622–4629. [Google Scholar] [CrossRef] [Green Version]
- Yan, H.; Parsons, D.W.; Jin, G.; McLendon, R.; Rasheed, B.A.; Yuan, W.; Kos, I.; Batinic-Haberle, I.; Jones, S.; Riggins, G.J.; et al. IDH1 and IDH2 mutations in gliomas. N. Engl. J. Med. 2009, 360, 765–773. [Google Scholar] [CrossRef]
- Pinton, L.; Masetto, E.; Vettore, M.; Solito, S.; Magri, S.; D’Andolfi, M.; del Bianco, P.; Lollo, G.; Benoit, J.P.; Okada, H.; et al. The immune suppressive microenvironment of human gliomas depends on the accumulation of bone marrow-derived macrophages in the center of the lesion. J. Immunother. Cancer 2019, 7. [Google Scholar] [CrossRef]
- Felsberg, J.; Thon, N.; Eigenbrod, S.; Hentschel, B.; Sabel, M.C.; Westphal, M.; Schackert, G.; Kreth, F.W.; Pietsch, T.; Löffler, M.; et al. Promoter methylation and expression of MGMT and the DNA mismatch repair genes MLH1, MSH2, MSH6 and PMS2 in paired primary and recurrent glioblastomas. Int. J. Cancer 2011, 129, 659–670. [Google Scholar] [CrossRef] [PubMed]
- Lombardi, G.; Barresi, V.; Indraccolo, S.; Simbolo, M.; Fassan, M.; Mandruzzato, S.; Simonelli, M.; Caccese, M.; Pizzi, M.; Fassina, A.; et al. Pembrolizumab Activity in Recurrent High-Grade Gliomas with Partial or Complete Loss of Mismatch Repair Protein Expression: A Monocentric, Observational and Prospective Pilot Study. Cancers 2020, 12, 2283. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: https://www.R-project.org (accessed on 12 September 2020).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients | Patients with Grade III | Patients with Grade IV | |
|---|---|---|---|
| No. of patients | 355 | 40 | 315 |
| Age at diagnosis, years a | 56 (45–65) | 35 (31–46) | 58 (48–66) |
| Females | 114 (32.1) | 14 (35.0) | 100 (31.7) |
| Males | 241 (67.9) | 26 (65.0) | 215 (68.3) |
| Grade: b | 40 (11.3) | 315 (88.7) | |
| PS: | |||
| 0 | 190 (53.5) | 22 (55.0) | 168 (53.3) |
| 1 | 120 (33.8) | 13 (32.5) | 107 (34.0) |
| 2 | 39 (11.0) | 5 (12.5) | 34 (10.8) |
| 3 | 6 (1.7) | 0 (0.0) | 6 (1.9) |
| Surgery | |||
| Non-radical | 105 (29.6) | 10 (25.0) | 95 (30.2) |
| Radical | 250 (70.4) | 30 (75.0) | 220 (69.8) |
| Analyzed tissue: | |||
| Diagnosis | 301 (84.8) | 30 (75.0) | 271 (86.0) |
| Recurrence | 54 (15.2) | 10 (25.0) | 44 (14.0) |
| MGMT status: c | |||
| Unmethylated | 139 (46.3) | 2 (9.1) | 137 (493) |
| Methylated | 161 (53.7) | 20 (90.9) | 1412 (50.7) |
| IDH status: d | |||
| Wild type | 267 (84.8) | 9 (29.2) | 258 (91.2) |
| Mutated | 48 (15.2) | 23 (71.8) | 25 (8.8) |
| PD-L1 expression: e | |||
| 0% | 99 (66.0) | 19 (100.0) | 80 (61.1) |
| >0% | 51 (34.0) | 0 (0.0) | 51 (38.9) |
| MMR protein expression: | |||
| Retained | 312 (87.9) | 27 (67.5) | 285 (90.5) |
| Partial loss | 28 (7.9) | 9 (22.5) | 19 (6.0) |
| Complete loss | 15 (4.2) | 4 (10.0) | 11 (3.5) |
| All Patients | Patients with Grade III | Patients with Grade IV | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Alteration of MMR Protein Expression: n/N (%) | p-value | Partial:Complete Loss of MMR Protein Expression: n:n | Alteration of MMR Protein Expression: n/N (%) | p-Value | Partial:Complete Loss of MMR Protein Expression: n:n | Alteration of MMR Protein Expression: n/N (%) | p-Value | Partial:Complete Loss of MMR Protein Expression: n:n | |
| No. | 43/355 (12.1) | - | 28:15 | 13/40 (32.5) | - | 9:4 | 30/315 (9.5) | - | 19:11 |
| Females | 15/114 (13.2) | 0.81 | 12:3 | 7/14 (50.0) | 0.17 | 6.1 | 8/100 (8.0) | 0.67 | 6:2 |
| Males | 28/241 (11.6) | 16:12 | 6/26 (23.1) | 3:3 | 22/215 (10.2) | 13:9 | |||
| Grade: | <0.0001 | - | - | - | - | - | - | ||
| III | 13/40 (32.5) | 9:4 | |||||||
| IV | 30/315 (9.5) | 19.11 | |||||||
| Analyzed tissue at: | 0.002 | 0.70 | 0.003 | ||||||
| Diagnosis | 29/301 (9.6) | 20:9 | 9/30 (30.0) | 7:2 | 20/271 (7.4) | 13:7 | |||
| Recurrence | 14/54 (25.9) | 8:6 | 4/10 (40.0) | 2.2 | 10/44 (22.7) | 6:4 | |||
| RT before tissue analysis: | 0.23 | 0.99 | 0.25 | ||||||
| No | 33/299 (11.0) | 24:9 | 10/30 (33.3) | 9:1 | 23/269 (8.6) | 15:8 | |||
| Yes | 10/56 (17.9) | 4:6 | 3/10 (30.0) | 0:3 | 7/46 (15.2) | 4:3 | |||
| CT before tissue analysis: | 0.03 | 0.70 | 0.08 | ||||||
| No | 31/300 (10.3) | 23:8 | 9/30 (30.0) | 8:1 | 22/270 (8.1) | 15:7 | |||
| Yes | 12/55 (21.8) | 5:7 | 4/10 (40.0) | 1:3 | 8/45 (17.8) | 4.4 | |||
| MGMT status: | 0.30 | 0.99 | 0.90 | ||||||
| Unmethylated | 12/139 (8.6) | 5:7 | 0/2 (0.0) | 0:0 | 12/137 (8.8) | 5:7 | |||
| Methylated | 21/161 (13.0) | 15:6 | 7/20 (35.0) | 5.2 | 14/141 (9.9) | 10:4 | |||
| IDH status: | 0.0005 | 0.99 | 0.09 | ||||||
| Wild type | 23/267 (8.6) | 13:10 | 3/9 (33.3) | 2.1 | 20/258 (7.8) | 11:9 | |||
| Mutated | 13/48 (27.1) | 8:5 | 8/23 (34.8) | 5:3 | 5/25 (20.0) | 3:2 | |||
| PD-L1 expression: | 0.15 | NA | 0.77 | ||||||
| 0% | 18/99 (18.2) | 12:6 | 9/19 (47.7) | 7:2 | 9/80 (11.3) | 5:4 | |||
| >0% | 4/51 (7.8) | 3.1 | 0/0 | 2:2 | 4/51 (7.8) | 3:1 | |||
| Progression-Free Survival | Overall Survival | |||
|---|---|---|---|---|
| Hazard Ratio (95% CI) | p-Value | Hazard Ratio (95% CI) | p-Value | |
| Immunohistochemical loss of MMR protein expression: | 0.89 | 0.50 | ||
| No | Reference | Reference | ||
| Yes | 1.05 (0.55 to 2.01) | 0.72 (0.28 to 1.86) | ||
| Age, years | 1.00 (0.98 to 1.02) | 0.71 | 1.01 (0.98 to 1.03) | 0.58 |
| Grade: | 0.22 | 0.09 | ||
| III | Reference | Reference | ||
| IV | 2.09 (0.64 to 6.79) | 4.95 (0.76 to 32.22) | ||
| Surgery: | 0.10 | 0.48 | ||
| Radical | Reference | Reference | ||
| Non-radical | 1.66 (0.90 to 3.05) | 1.34 (0.59 to 3.05) | ||
| PS: | ||||
| 0 | Reference | Reference | ||
| 1 | 1.38 (0.82 to 2.31) | 0.22 | 1.83 (0.85 to 3.92) | 0.12 |
| 2–3 | 1.61 (0.85 to 3.05) | 0.15 | 4.87 (1.86 to 12.79) | 0.001 |
| MGMT status: | 0.14 | 0.04 | ||
| Unmethylated | 1.41 (0.90 to 2.23) | 2.03 (1.01 to 4.08) | ||
| Methylated | Reference | Reference | ||
| IDH status: | 0.007 | 0.23 | ||
| Wild type | 4.73 (1.54 to 14.48) | 2.99 (0.51 to 17.51) | ||
| Mutated | Reference | Reference | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caccese, M.; Ius, T.; Simonelli, M.; Fassan, M.; Cesselli, D.; Dipasquale, A.; Cavallin, F.; Padovan, M.; Salvalaggio, A.; Gardiman, M.P.; et al. Mismatch-Repair Protein Expression in High-Grade Gliomas: A Large Retrospective Multicenter Study. Int. J. Mol. Sci. 2020, 21, 6716. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21186716
Caccese M, Ius T, Simonelli M, Fassan M, Cesselli D, Dipasquale A, Cavallin F, Padovan M, Salvalaggio A, Gardiman MP, et al. Mismatch-Repair Protein Expression in High-Grade Gliomas: A Large Retrospective Multicenter Study. International Journal of Molecular Sciences. 2020; 21(18):6716. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21186716
Chicago/Turabian StyleCaccese, Mario, Tamara Ius, Matteo Simonelli, Matteo Fassan, Daniela Cesselli, Angelo Dipasquale, Francesco Cavallin, Marta Padovan, Alessandro Salvalaggio, Marina Paola Gardiman, and et al. 2020. "Mismatch-Repair Protein Expression in High-Grade Gliomas: A Large Retrospective Multicenter Study" International Journal of Molecular Sciences 21, no. 18: 6716. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21186716